
Abstract
Objectives:
Iron–folic acid non-compliance is a major problem in the study area. Therefore, this study aimed to assess the level of iron–folic acid supplementation compliance and associated factors among pregnant women.
Methods:
A community-based cross-sectional study design was conducted among pregnant women from 1 to 30 November 2018 in Dangila, Northern Ethiopia. A multi-stage sampling technique was used to select the participants. The data were collected using a structured questionnaire. For data entry and analysis, Epi Info 7 and Statistical Package for Social Science (SPSS) 23.0 were used, respectively. Bivariable and multivariable logistic regression analyses were done. Descriptive statistics like mean and standard deviation, and odds ratios with their respective confidence intervals were calculated. Statistically significant was declared at a p value of less than 0.05. The results were presented using text, tables, and figures.
Results:
A total of 589 pregnant women were involved, yielding a response rate of 91.2%. The average age of the participants in the study was 30.90 ± 5.93 years. The average weekly iron–folic acid pill intake was 5.3. The iron-folic acid compliance rate was 76.9% (95% confidence interval: 73.5–80.6). Women who had four or fewer alive children (adjusted odds ratio = 2.68, 95% confidence interval: 1.37–5.23), took less than 30 min to get to the health facility (adjusted odds ratio = 1.90, 95% confidence interval: 1.16–3.10), being a government employee (adjusted odds ratio = 0.16, 95% confidence interval: 0.03–0.81), attended antenatal care conferences (odds ratio = 2,95% confidence interval: 1.16–3.42), and started iron–folic acid tablets in the first trimester (odds ratio = 2.3, 95% confidence interval: 1.39–3.87) were associated with iron–folic acid compliance.
Conclusion:
The level of iron–folic acid supplementation compliance was low. Attending antenatal care training and starting to take iron-folic acid pills early in the first trimester were both factors associated with iron–folic acid supplementation compliance. Health care and health extension workers should emphasize and monitor the iron pill–taking habits of pregnant women in home-to-home visits.
Introduction
Anemia is a condition that occurs when the number of red blood cells (RBCs) or the hemoglobin concentration within them is lower than normal. The cut-off point of hemoglobin is determined by the age, gender, physiological status, smoking habits, and altitude at which the population being assessed resides. For example, anemia is defined as a hemophon concentration of less than 110 g/L at sea level in children under the age of 5 and pregnant women. There are different types of anemia including iron-deficiency anemia, sickle cell anemia, aplastic anemia, vitamin-deficiency anemia, and anemia associated with chronic conditions. 1 Iron-deficiency anemia accounts for around half of all anemia cases worldwide. 2
Anemia is a worldwide public health problem affecting over 2 billion people. Pregnant women, in particular, bear a disproportionate share of the burden. 2 Globally, anemia affects 30.2% of non-pregnant women and 41.8% of pregnant women.3,4 In wealthy countries, the prevalence of anemia among pregnant women was 18%, which is much lower than in low-income countries (56.0%).5,6 Maternal anemia was responsible for 12% of low birth weight, 19% of preterm births, and 18% of perinatal deaths in South Asia and the Sub-Saharan region. At 28 days, maternal death was the primary maternal outcome, stillbirth was the primary fetal outcome, and neonatal mortality was the primary neonatal outcome. 7
The World Health Organization 8 defines compliance as the degree to which a person’s behavior in taking medication, adhering to a diet, and/or implementing lifestyle changes corresponds with agreed recommendations from a health care provider. Several studies suggested that formal education, single-family size, early antenatal care (ANC) registration, increased antenatal visits, and the doses of iron pills were associated with iron-folic acid (IFA) compliance.9-12
IFA supplementation is the major approach for treating and preventing anemia in Ethiopia. Pregnant women who began ANC visits in the first trimester were more likely to comply with them than those who began in the third trimester. Anemia was common in the Dangila district, with 23% of the population suffering from it. Early ANC registration, four or more ANC visits, anemia on the initial visit, and IFA supplement advice were all associated with higher compliance.13-21 In 2016, the Ethiopian Demographic Health Survey (EDHS) found that a higher percentage of pregnant women (29%) were anemic. Women who had a malarial episode during their current pregnancy were more likely to take IFA supplements. 22
All pregnant women should take a standard dose of 60 mg of iron and 400 mg of folic acid for 6 months, with supplementation beginning during the early months of pregnancy or at the first antenatal visit. However, only a few countries have experienced considerable progress in IFA supplementation and anemia prevention and treatment.2,4
Anemia during pregnancy is a severe health problem in many impoverished countries, despite the fact that it affects everyone. Routine IFA supplementation is the main strategy for prevention and control of iron-deficiency anemia and neural tube defects during pregnancy. Nonetheless, its compliance and associated factors during pregnancy were not well investigated in the study area. In the current study area, little is known about the factors associated with compliance with IFA. Therefore, this study aimed to determine the level of IFA compliance and the factors that influence it among pregnant women in Dangila, Ethiopia, in 2018.
Methods
Study design and study setting
A community-based cross-sectional study design was conducted to determine compliance and factors associated with the utilization of iron supplementation from 1 to 30 November 2018 in Dangila, Ethiopia. According to the Ethiopian national population and housing census of 2007, the population of Dangila district is estimated to be around 158,223 people, with 5325 of them being pregnant women. For administrative purposes, the district is divided into four urban kebeles and 31 rural kebeles. Six health centers, five private for-profit clinics, 35 health posts, and 3 drug vendors serve the district. Based on the national guidelines for IFA supplementation, all health centers and health posts now provide IFA supplementation services.
Population
Pregnant women who had ANC visits in Dangila district in the selected sites were the source population, and those women who were taking IFA supplementation during the study period in the selected sites were the study population.
Inclusion and exclusion criteria
All pregnant women who had used IFA tablets for at least 3 months were included in the study. Pregnant women who were unable to hear or speak, extremely ill, or refused to participate in the study were not included in the study.
Sample size determination
The sample size was determined using Epi Info version 7 with the following assumptions: The level of confidence was 95%, the proportion of IFA supplement compliance was 55.3%, and substantial factors for compliance (IFA compliance among women with family size ⩾ 4 = 60.6% and those with family size < 4 = 46.5%). 16 The calculated sample size was 392. The total sample size was 646 after adding a 10% non-response rate and multiplying by 1.5 design effects.
Sampling procedures
A multi-stage sampling technique was used. Two kebeles from four urban kebeles and 15 kebeles from 31 rural kebeles were selected using a simple random sampling method. Then, the samples were proportionally allocated to each kebele and the study participants were selected from the health extension registry book using a simple random sampling method in the respective kebeles (Figure 1).

Sampling procedures were used to determine the level of iron–folic acid compliance among pregnant women.
Operational definitions
Data collection procedures and quality control
The data were collected using an interviewer-administered questionnaire. The questionnaire was adapted from previous literatures.1,22 To ensure uniformity, the questionnaire was first written in English, and then translated into Amharic, and then back to English. Interviewers from the district’s health extension workers and one health officer as a supervisor were recruited. The data collectors and supervisor were trained for 3 days on the questionnaire, interviewing techniques, the study’s goal, and maintaining the privacy of the participants prior to the actual data gathering period. Throughout the data collection period, the principal investigator and supervisor conducted daily on-site supervision. At the end of each day, the questionnaire was checked for completeness, accuracy, and consistency. Data quality was maintained through training and close supervision. The questionnaire was pretested on 5% of the randomly selected pregnant women.
Statistical analysis
After data collection was completed, the data were entered into Epi Info version 7 and exported to SPSS version 23 for analysis. For each of the variables, descriptive statistics were done. To select candidate variables for multivariable logistic regression analyses, bivariate logistic regression analysis was performed for the independent variables with the outcome variable. To determine their independent effects, all variables with a p value less than or equal to 0.20 in the bivariate logistic analysis were put into a multivariable logistic regression model. Finally, characteristics associated with an independent relationship with IFA supplementation compliance were discovered. A statistically significant result was reported when the p value was less than 0.05 at 95% confidence. The findings were presented using texts and tables.
Results
Socio-demographic characteristics
This study comprised a total of 589 pregnant women, yielding a response rate of 91.2%. The average age of the participants in the study was 30.90 ± 5.93 years. In all, 503 (99.0%) of the women were married, 580 (98.5%) were Amhara, 589 (100.0%) were Orthodox believers, 535 (90.8%) were housewives, 504 (85.6%) had no formal education; and 454 (77.1%) had a family size of four or more (Table 1).
Socio-demographic characteristic of compliance to IFA supplementation among women in Dangila, Northern Ethiopia, 2018.

Level of compliance toward IFA
The average weekly pill intake was 5.3 tablets. A total of 403 respondents (76.9%) took four or more IFA tablets per week, while 136 (23.1%) took fewer than four IFA tablets per week (Table 2).
Reproductive and service-related factors of compliance to IFA supplementation among women in Dangila, Northern Ethiopia, 2018.

Reproductive history and service-related characteristics of the respondent
A total of 507 (86.1%) of the 589 respondents had one or more pregnancies. Of those, 506 (85.9%) were multi gravid, only 52 (8.8%) had experienced complications in a previous pregnancy, and 53 (9.0%) had undergone an abortion. The respondents’ average number of living children was five. Only 34 people (5.5%) had a known medical issue (Table 2).
In terms of current ANC follow-up locations, the majority of women (421, 71.6%) went to the health center. More than half of the respondents (331, 56.1%) started their ANC follow-up in the first trimester of pregnancy, and 484 (82.2%) reported they were satisfied with the care provided during the ANC follow-up. The majority of the respondents (557, 94.6%) had received nutritional counseling, and 458 (77.8%) had attended an ANC conference.
Women’s knowledge about IFA tablets
The majority of the respondents (509, or 86.4%) have heard about anemia in their lifetime. Health practitioners were the sources of information for 478 (81.2%) of individuals who had heard about anemia in their lifetime. Pregnant women are more likely to be affected by anemia than non-pregnant women, 482 (81.8%), 507 (86.1%) respectively. Overall, the study found that over half of the mothers (276, or 46.9%) had strong awareness of anemia, while the remaining 313 (53.1%) had poor understanding of anemia (Table 3).
Women’s knowledge about anemia among women in Dangila, Northern Ethiopia, 2018.

Associated factors toward IFA supplementation
Age, maternal occupation, time to reach the health facility, number of living children, history of abortion, gestational age of current pregnancy, gestational age at the time of initiation, attendance at ANC conferences, number of IFA tablets collected in one ANC visit, counseling during IFA tablet collection, knowledge about anemia, and knowledge about IFA tablets were all found to have a significant relationship with IFA supplementation compliance in the bivariate analysis.
However, after controlling for other variables in the final model, time to reach the health facility, maternal occupation, number of alive children, participation in the ANC conference, gestational age at initiation, number of IFA tablets collected in one ANC visit, and counseling during IFA tablet collection were all significantly associated with IFA supplementation compliance in the multivariable analysis.
Access to IFA tablets was 1.9 (95% CI: 1.16–3.10) times more likely among women who lived within 30 min walking distance of the health facility than among mothers who lived more than 30 min walking distance. Women with four or fewer children were shown to be 2.68 (95% CI: 1.37–5.23) times more compliant than women with more than four children (Table 4).
Logistic regression analysis results showed determinants of compliance of IFA supplementation among women in Dangila, Northern Ethiopia, 2018.
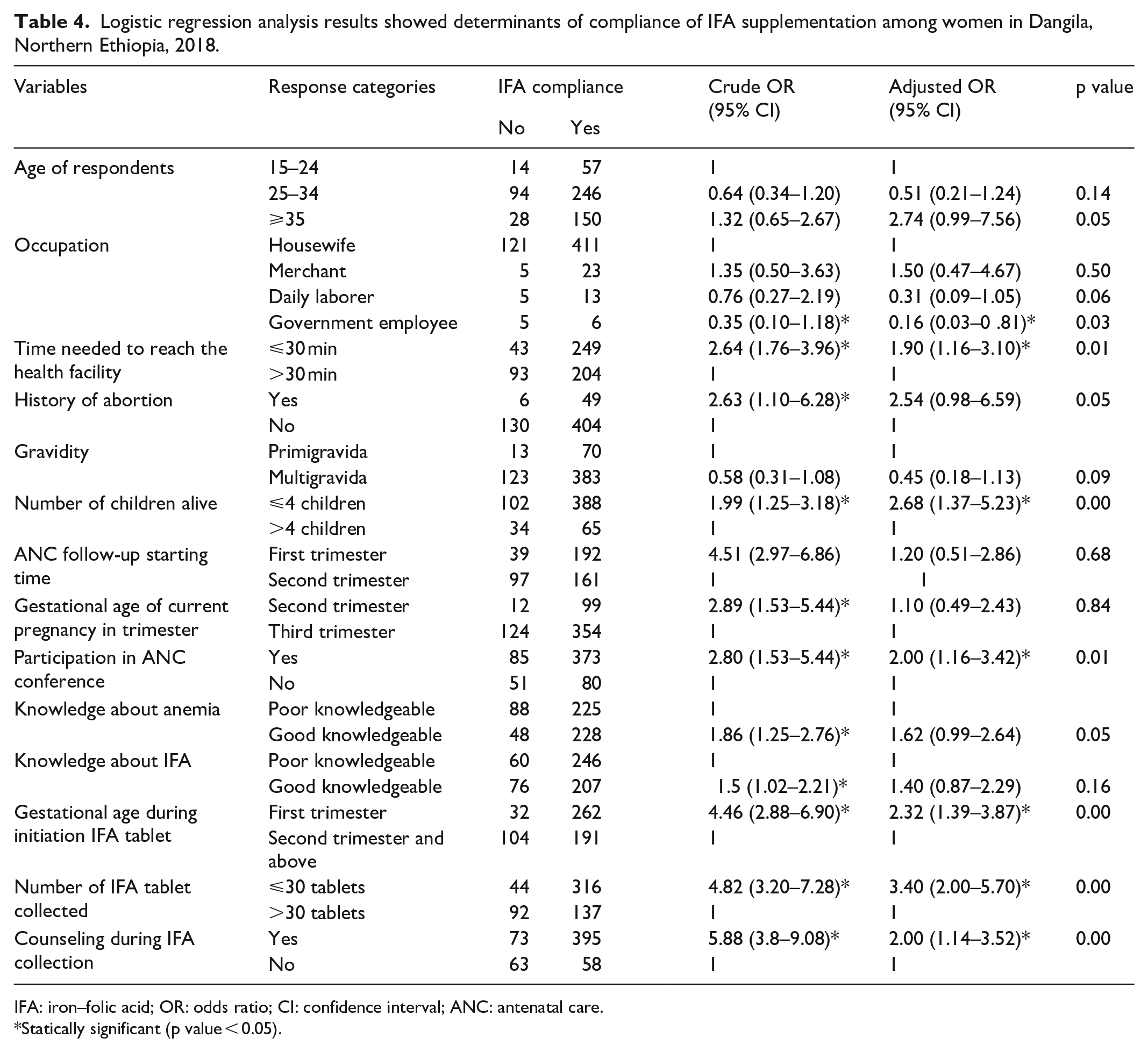
IFA: iron–folic acid; OR: odds ratio; CI: confidence interval; ANC: antenatal care.
Statically significant (p value < 0.05).
Discussion
The level of IFA compliance among pregnant women who took the tablets was found to be 79.6% in this study. This result is similar to a study conducted in four Ethiopian regions, which found 74.9%, 11 and greater than a study conducted in the Mecha district in the Amhara region of Ethiopia in 2013, which found 20.4%. In 2014, a study in Goba district, southeast Ethiopia, found that 18.0% of the population was illiterate.20,21 The variation in geographic locations and the time interval between studies could be the likely causes. During this time, the government is working to promote maternal health, including a strategy to supplement IFA. Furthermore, the discrepancy could be attributed to the study subjects; in this study, the study subjects were pregnant women, whereas in prior studies, the study subjects were 6 months to 1 year post-delivery, which could lead to trouble recalling the number of tablets taken in a given period. The results of this survey were lower than those of a study conducted in North Sudan, which came in at 91.2%. 23 This discrepancy could be attributable to the research area. The prior study was conducted in one of Sudan’s referral hospitals so that high-level specialists could provide proper counseling. It could also be attributable to the different educational levels of the study subjects. In this survey, 86% of the participants were illiterate, whereas in the previous study, 76.3% of the participants had completed secondary school. According to other studies, educated women were more obedient to IFA than illiterate women. 13
Among socio-demographic factors, time taken to reach the nearest health facility was significantly associated with compliance with IFA intake, indicating that mothers who lived within 30 min walking distance of a health facility with access to IFA tablets were about two times more likely to comply with IFA supplementation than mothers who lived more than 30 min walking distance. However, the variable was not significant in a similar study in Addis Ababa. 14 This disparity could be attributable to the prior study’s higher health insurance coverage and easier access to health care and transportation than the present study’s.
Maternal occupation is another crucial component that reveals a strong relationship. In comparison to mothers who are housewives, mothers who work for the government are 84.0% less likely to comply with IFA supplementation. This research is similar to one done in Ethiopia. 21 This could be because they believe that eating a well-balanced diet will suffice.
In this study, women with four or fewer children were shown to be 2.68 times more compliant than women with more than four children. This outcome is consistent with research conducted in Uganda and Kenya.24,25 In a prior study in Kenya, the level of compliance decreased as the number of children increased. This outcome is due to the fact that they require more healthy youngsters who can appropriately follow the recommendations of health professionals.
In this study, the gestational age of pregnancy had a significant impact on IFA supplementation commencement and compliance. Women who began taking an IFA supplement in the first trimester of pregnancy were 2.3 times more likely to be compliant than those who began later in the pregnancy. This study was consistent with earlier Ethiopian investigations, with an adjusted odds ratio (AOR) of 3.80, which was greater than an Indian study with an AOR of 2.04.13,26 It is possible that this is due to repeated visits, with useful information acquired from each one early on.
Participation in ANC conferences was another factor that was linked to compliance. Women who had ever attended ANC conferences during their current pregnancy were twice as likely to take IFA supplements as those who had never attended ANC conferences. This conclusion is backed up by an Ethiopian study. 14 Since then, conferences have provided opportunities for mothers to talk with one another and with health care providers about anemia and its consequences, as well as the need for IFA supplementation and how and when to take the pills.
Another crucial element that influences supplement compliance is the amount of IFA obtained in one ANC visit. Women who took fewer than 30 tablets were 3.4 times more obedient than women who took more than 30 tablets. Participants who collected fewer tablets per visit had higher levels of compliance. This is consistent with a study conducted in Ethiopia. 16 According to evidence in India, when the quantity of tablets decreases, treatment compliance improves. 27 This is due to the fact that a higher pill count has a negative psychological influence on compliance.
Another variable associated with IFA supplementation compliance is counseling provided during the collection of IFA tablets. Women who received counseling during IFA tablet collection were two times more likely to be compliant than those who did not. A study conducted in Ethiopia, Cambodia, and Senegal backed this conclusion.15,28,29 This is because IFA supplement information is provided during counseling at the time of tablet collection.
The weakness of this study is that information on pregnant women’s compliance levels came from self-reported IFA intake, so there might be a chance that pregnant women who did not take the tablets were reported.
Conclusion
The level of compliance was low in the study area. Women who had less than or equal to four live children, traveled less than 30 min to get to the health facility, attended ANC conferences, started taking IFA tablets in the first trimester, had less than or equal to 30 IFA tablets collected in one ANC visit, and received counseling during IFA tablet collection were all positively associated factors in this study. Women who worked for the government, on the contrary, had a lower rate of IFA supplementation compliance. Health care and health extension workers should emphasize and monitor the iron pill–taking habits of pregnant women in home-to-home visits.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221118989 – Supplemental material for Compliance level and factors associated with iron–folic acid supplementation among pregnant women in Dangila, Northern Ethiopia: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221118989 for Compliance level and factors associated with iron–folic acid supplementation among pregnant women in Dangila, Northern Ethiopia: A cross-sectional study by Abiyot Wolie Asres, Woldeamilak Adamu Hunegnaw, Addisu Gasheneit Ferede and Tamene Wolie Azene in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the data collectors, supervisors, and women who participated in this study.
Author contributions
TWA and WAH conceived and designed the study, performed the analysis, and interpreted the data. AGF and AWA participated in the design, analysis, and interpretation of the data. AGF, AWA, TWA, and WAH participated in drafting the article. All authors read and approved the final submitted version of the article. All authors have agreed to both be personally accountable for the author’s contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The ethics approval letter was obtained and ethical clearance was obtained from the Institutional Review Board (IRB) of Bahir Dar University, College of Medicine and Health Science with ethics approval number CMHS/IRB 03-008. Permission was obtained from Amhara National Research Institute and Dangila district health office administration. The purposes and benefits of the study were discussed with each respondent. Written consent from the respondent was obtained first, before proceeding to the formal data collection.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study. The exceptions for consent to medical treatment for minors fall into two categories. The first is for situations where the minor is married or is the parent of a child. The second is for situations where a minor seeks particular types of treatment. These minor subjects did not require parental or guardian consent because they were married and lived independently. Furthermore, the study did not need medical treatment or did not have injury for individuals under the age of 18 years old. They gave their own written informed consent. These concerns were taken into account by the IRB when approving the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.