
Abstract
Objective:
To determine the prevalence of drug-related problems and the factors influencing them among adult psychiatric inpatients.
Methods:
A multi-centre cross-sectional observational study was conducted from April to July 2021 at five randomly selected hospitals in Northwest Ethiopia. A total of 325 consecutively sampled patients participated in the study. Clinical pharmacists assessed the drug-related problems based on clinical judgement supported by updated evidence-based disease guidelines. We used the Medscape drug-interactions checker to check drug-to-drug interactions. The results were summarised using descriptive statistics, including frequency, mean, and standard deviation. For each variable, an odds ratio with a 95% confidence interval was calculated, as well as the related p-value. The value of p ⩽ 0.05 was considered statistically significant.
Results:
From the total number of 325 study participants, more than half of them (52.9%) were females, and the mean age ± (standard deviation) was 30.8 ± 11.3 years. At least one drug-related problem was recorded by 60.9% to 95% confidence interval (55.7–65.8) of study participants, with a mean of 0.6 ± 0.49 per patient. Additional drug therapy was the most common drug-related problem (22.8%) followed by non-adherence to medicine (20.6%) and adverse drug reactions (11%), respectively. Factors independent associated with drug-related problems were rural residence (adjusted odds ratio = 1.96, 95% confidence interval: 1.01–2.84, p-value = 0.046), self-employed (adjusted odds ratio = 6.0, 95% confidence interval: 1.0–36.9, p-value = 0.035) and alcohol drinkers (adjusted odds ratio = 6.40, 95% confidence interval: 1.12–37.5, p-value = 0.034).
Conclusion:
The prevalence of drug-related problems among adult psychiatric patients admitted to psychiatric wards was high. Healthcare providers give more attention to tackling these problems. Being a rural resident, self-employed, and alcohol drinkers were associated with drug-related problems.
Introduction
The World Health Organization (WHO) defines mental health as ‘a state of well-being in which a person understands his or her capacity, can cope with normal stresses of life, can work productively and fruitfully, and can contribute to his or her community’. According to a WHO survey, 450 million people worldwide suffer from mental or behavioural illness. 1 Whereas in most regions of Africa, mental illness is considered as a silent epidemic and has been neglected and is increasingly affecting all segments of the population due to inadequate health care, infrastructure, an insufficient number of mental health specialists, and inadequate access to all levels of care.2,3 While, in Ethiopia, mental illness is the most common non-communicable disease and it accounts for 11% of the overall disease burden in a largely rural region of the country. 4
A drug-related problem (DRP) is defined as an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes, and DRPs are classified as unnecessary drug therapy, needs additional drug therapy, dosage too low, dosage too high, ineffective drug therapy, adverse drug reaction (ADR) and non-compliance. 5 DRPs are the most common in patients with a psychiatric disorder due to the pharmacokinetic and pharmacodynamic characteristics of medicine in psychiatric therapies. 6 Antipsychotics, benzodiazepines, and mood stabilisers are among other drugs used to treat mental illness. They are effective, although they may have significant side effects. 7
In today’s clinical practice, prescribers often use more drugs to treat each of their patients’ comorbid conditions. The situation becomes much more complicated as patients see healthcare providers of different specialties, potentially resulting in DRPs. 8 Psychiatric patients are becoming more vulnerable to drug-to-drug interactions (DDI). 9 Since DRPs are a vital issue and a significant number of them are preventable, the specific hazard factors that encourage the event of DRPs are of extensive interest. However, there is no data which has published about the prevalence of and extents of DRPs in the Northwest Ethiopia. Therefore, this study was aimed to determine the prevalence of drug related problems and the factors influencing them among adult psychiatric inpatients in the selected hospitals in Northwest Ethiopia.
Method and materials
Study area and period
The study was conducted at five comprehensive and specialised hospitals in Northwest Ethiopia from April to July 2021. The hospitals were University of Gondar Comprehensive and Specialized Hospital (UoGCSH), Felege Hiwot Comprehensive and Specialized Hospital (FHCSH), Tibebe Ghion Comprehensive and Specialized Hospital (TGCSH), Debre-Markos Comprehensive and Specialized Hospital (DMCSH) and Debre-Tabor Comprehensive and Specialized Hospital (DTCSH).
The UoGCSH is one of Ethiopia’s oldest academic institutions. For more than half a century, it has produced a number of health professionals. It is situated in the centre of Gondar, in Ethiopia’s Amhara Region, in the northwest.
The city is located 738 km away from Addis Ababa, the capital city of Ethiopia. It has more than 1000 beds for inpatient service at six different wards. It provides primary and referral health care services for nearly 5 million people living in Gondar town and neighbourhood woredas and zones. The annual admission last year in the psychiatric ward was 264 patients.
The FHCSH is also one of the largest hospitals in the region, located in Bahir-Dar, the regional state’s headquarters, 565 km Northwest Ethiopia’s capital, Addis Ababa. It serves as a comprehensive hospital for the residents of Bahir-Dar, West Gojjam, Awi, and South Gondar zones, which have a combined population of about 7 million people. 10 It contains 492 inpatient beds spread across six units. In the previous year, 192 people were admitted to the psychiatric ward.
The TGCSH is also one of the largest teaching hospitals situated in Bahir-Dar. It has 498 beds for inpatient service in five wards. Bahir-Dar University uses it as a teaching hospital as well. It provides primary and referral health care services to more than 5.5 million people living in Bahir-Dar town and neighbourhood woreda as and zones. The annual admission in the last year in the psychiatric ward was 180 patients per year.
The DTCSHis 295 km from Ethiopia’s capital, Addis Ababa, and 265 km from Bahir Dar, the capital of the Amhara regional state. In its catchment area, it is expected to serve almost 5 million people. It has 458 beds for inpatient service at five wards. Among this, psychiatric ward is one of the inpatient services areas. 10 The annual admission in the last year in the psychiatric ward was 192 patients per year.
Similarly, DTCSH is located in the Debre-Tabor town: South Gondar zone, Amhara regional state, Northwest Ethiopia, located 666 km from Addis Ababa. It provides services to nearly 4 million people in its catchment area. It has 458 beds for inpatient service at five wards among this psychiatric ward is one of the inpatient services areas. 1 The annual admission in the last year in the psychiatric ward was 156 patients per year.
Study design and period
Hospital-based cross-sectional observational multicentre study was conducted.
Population
Source population
All adult patients with a psychiatric disorder who were admitted to the psychiatric wards of hospitals in Northwest Ethiopia.
Study population
All adult patients with psychiatric disorders who fulfilled the inclusion criteria and were admitted to the psychiatric wards of the selected hospitals during the study period.
Eligibility criteria
Inclusion criteria
All patients whose age was ⩾ 18 years of old, diagnosed with any psychiatric disorder and admitted for treatment.
Exclusion criteria
Critically ill patients with no caretaker during the study period and patients who were readmitted during the study period.
Sample size determination and sampling techniques
Sample size determination
The single population proportion formula was used to calculate the required sample size by considering the following assumptions: Proportion of DRPs 74.1%, 11 95% confidence level, and 5% margin of error (absolute level of precision). n = the minimum sample size, Z = reliability coefficient for desired interval (CI) for 95% = 1.96, p is an estimate of the prevalence rate of drug related problems among admitted psychiatric patients, since the prevalence is DRPS 74.1% (p = .741), q = 1-p = .259, d = desired interval (degree of precision) = 5% (0.05).

After adding a 10% (contingency) non-response was added, so the sample size was 295 + 29. 5 = 325. Therefore, a sample size of 325 was considered. Based on a proportional allocation formula;
Sampling procedure and techniques
There are seven comprehensive and specialised hospitals in the Amhara region. Five comprehensive specialised hospitals in Northwest Ethiopia were included in the study by lottery method. The overall sample size was then proportionally allocated to each selected comprehensive hospital based on the number of patients admitted to the psychiatric ward in the previous year.

where n = required sample size
Ni = total population of each hospital
N = total population each selected hospital
Study participants recruited from UoGCSH = 264/yr = 22/ month = n = 325×264 /984 = 87
Study participants recruited from FHCSH = 192/yr = 16/month = n = 325×192 /984 = 63
Study participants recruited from TGCSH = 180/yr = 15/month = n = 325×180 /984 = 60
Study participants recruited from DMCSH = 192/yr.= 16/month = n = 325×192 /984 = 63
Study subjects recruited from DTCSH = 156/yr. = 13/month = n = 325×156 /984 = 63 = 52.
Convenient sampling technique was employed to extract data from medical records and to interview the study participants
Variables of the study
Dependent variable: drug-related problems (DRPs)
Independent variables: patient-related factors.
Age, gender, bodyweight, height, income, body mass index (BMI), marital status, smoking, alcohol drinking, khat chewing, substance use, educational level, residency, history of allergy, breastfeeding, pregnancy, occupation, living status, and religion.
Factors related to medicines.
The type of medicine, the number of medicines, and the length of treatment, disease-related factors and the number of hospitalisations.
Definition of terms
Drug-Related Problem: is an occasion or situation involving drug treatment that really or conceivably obstructs health outcomes outcomes. 2
Polypharmacy: The concurrent use of five or more number of medicines in a patient. 12
Adherence: Is defined as the extent to which the patient’s action matches the agreed recommendations. 13
Comorbidity: is the presence of one or more additional conditions often co-occurring with the primary condition.
Intervention: When pharmaceutical care plan designed, communicated and the identified problems suggested to be solved.
Adverse drug reactions (ADRs): Is an unwanted or harmful reaction experiencing following the administration of a drug or combination of drugs under normal conditions of use and is suspected to be related to the drug. 14
Drug-Drug Interactions: is defined as the pharmacological or clinical response to the administration or co-exposure of a drug with another drug that modifies the patient’s response to the drug index. 15
Social support: Is the perception and actuality that one is cared for, has assistance available from other people, and most popularly, that one is part of a supportive social network.
Number of hospitalisations: The number of hospitalisations in the previous one year excluding the current hospitalisation.
Psychiatric disorder: According to DSM-5 definition ‘syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behaviour that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental function’.
Data collection procedures and instrument
Data were collected using structured questionnaire in English language and which was developed after reviewing different literature.8,16–23 The data collected by both interviewing the patients and patient medical records were also used for primary and secondary data, respectively. Primary data such as socio-demographic and clinical characteristics were collected by interviewing patients or their caregivers using a structured questionnaire. Data were collected by five trained clinical pharmacists and five trained psychiatry nurses supervised by two assistant lecturers of clinical pharmacy.
Trained clinical pharmacists about the evidences and their scientific judgmental assessed the DRPs supported by updated evidence-based disease guideline.24–26 DRPs were classified according to Cipolle et al and adherence was assessed according to the medication measurement rating scale (MARS).27.We used Dipiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM,2014, Adock BJ. Kaplan & Sadock’s Synopsis of Psychiatry, 2007, Jacobs G, Cohen AJBJoCP, 2008 guideline, which is an international guideline and all five centres used it. The medscape drug-interactions checker was used to check drug-drug interactions.
Data quality control
To ensure the quality of the data, the collectors were trained for two days, and orientation was also given by the principal investigator. The principal investigator (PI) closely supervised the data collection process, and the collected data were checked daily for completeness during the data collection period. The data collection tool was pretested on 17 (5% of the calculated sample size) patients admitted to the psychiatric ward of Dessie comprehensive specialised hospital to check the acceptability and consistency of the data collection tool two weeks before the actual data collection. The data from the pre-test was not included in the analysis. The questionnaire was sent to senior clinical pharmacists and senior physicians who were academicians and researchers for face validity and approval.
Statistical analysis
The collected data were coded, cleared, checked for completeness, and entered into EPI-data version 4.6.02 and exported to statistical software package for social sciences (SPSS) version 26 for analysis. The chart numbers were entered into Microsoft Office Excel 2016 and checked for duplication. Then, data were inspected and cleaned manually for its appropriateness and consistency.
The results were summarised using descriptive statistics including frequency, mean, and standard deviation for continuous and categorical. Independent variables having a p-value < 0.25 in the bivariate logistic regression analysis were entered into the multivariable logistic regression analysis in order to control for confounding effects. The odds ratio (OR) with a 95% confidence interval (CI) were also computed for each variable for the corresponding p-value. The value of p < 0.05 was considered statistically significant.
Results
Socio-demographic characteristic of the study participants
A total of 325 study participants were approached and more than half of them, 172 (52.9%) were females. The mean (± SD) age of the study participants was 30.8 ± 11.3 years. Among the participants, 154 (47.4%) were single and nearly two-thirds (66.2%) lived in a rural area. More than one-third (33.9%) of the study participants had no formal education. Nearly half (49.2%) of the participants were unemployed. Almost all (98.2%) of the study subjects never smoked and chewed khat. The majority of the study subjects 287 (88.3%) were living with their families (Table 1).
Socio-demographic characteristic of the patients with psychiatric disease admitted to Psychiatric wards of selected hospitals in Northwest Ethiopia from 1 April–30 July 2021.

BMI: body mass index.
Clinical characteristics of the study participants
Most of the patients had 14 days of hospital stay which accounted for 290 (89.2%) with the average (± SD) length of hospital stay was 13.8 ± 9.8 days. The mean (± SD) duration of treatment was 2.4 ± 2.8 years and more than half (59.4%) of the study participants had treatment duration of 1 year or less. Most (84%) of the study participants had a history of hospitalisation in the last one year. Of the total study participants, 21.2% had comorbid conditions. The most common psychiatric disorder was schizophrenia. The most common co morbid diseases were anxiety (3.07%), epilepsy, 9 (2.8%), dyspepsia, 6 (1.8%), urinary tract infections, 5 (1.5%) and substance use disorder, 4 (1.2%). Near to all (99.7%) of the patients reported that they didn’t experience documented allergy (Table 2).
Clinical characteristics of psychiatric patients admitted to psychiatric wards of selected hospitals in Northwest Ethiopia from 1 April–30 July 2021.

post-traumatic stress disorder and attention deficit hyperactivity disorders.
cardiovascular disorders, neurological disorders and diabetes mellitus.
Ohers*, Post-traumatic stress disorder; attention deficit-hyperactivity disorder, others**, cardiovascular disorders; neurological disorders, diabetes.
Prescribed medicines in admitted to psychiatric patients
In the current study, on average, 2.9 ± 1.23 medicines were prescribed for each studied participant. Benzodiazepines were the most commonly used medicine class (31.1%). Diazepam and Risperidone were the most frequently prescribed medicines from the benzodiazepine group (28.9%), followed by second-generation antipsychotics SGA (22.1%) (Table 3).
Prescribed medicines for patients admitted to psychiatric wards of selected hospitals in Northwest Ethiopia from April–July, 2021. Total number of medicines (N = 752).

Anticholinergics, anti-infective, anti-diabetics, anti-retroviral, calcium channel blockers.
Prevalence of drug-related problems (DRPs)
The current study indicated the prevalence of DRP to be 60.9% (95% CI: 55.7–65.8). As indicated in Figure 1, the most common DRPs were ‘need additional drug therapy (22.8%)’, followed by ‘non- adherence to medicine (20.6%)’, and ‘adverse drug reactions (11%)’.
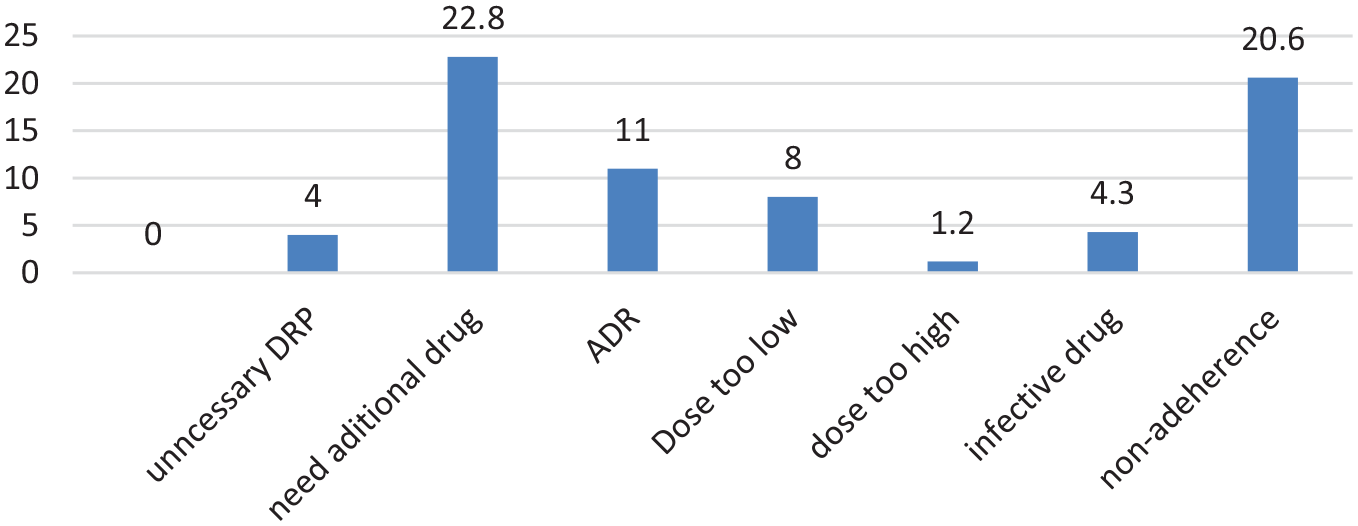
Prevalence of DRPs among psychiatric patients admitted to psychiatric wards of selected hospitals in Northwest Ethiopia from 1 April to 30 July 2021.
Types of drug related problems and possible causes
A total of 228 DRPs from 325 patients screened with a mean (± SD) of 2.9 ± 1.23 DRPs per patient. The most common cause of the need for additional drug therapy was the need for preventive therapy (11.7%), whereas the most common cause of non-adherence to medication was no willingness to take the drug (14.5%). The most possible cause for adverse drug reactions was drug interactions causes’ undesirable reactions not related to dose (8.9%). Details of the types of DRPs and possible causes are given in Table 4.
Types of drug related problems and causes among psychiatric patients admitted to psychiatric wards of selected hospitals in Northwest Ethiopia from 1 April to 30 July 2021.

DRP: drug-related problem.
Factors associated with the occurrence of DRPs
The findings from multivariate logistic regression showed the presence of a significant association between DRPs and three independent variables (residency, occupation, and alcohol drinkers). Accordingly, patients who live in rural residences were 1.96 times more likely to have DRPs than those in urban residence area. Meanwhile, those who were self-employees were 6 times more likely to experience DRPs than those who were government or private organisation employees (AOR = 6.0, 95% CI: 1.0–36.9, p = 0.035). On the other hand, alcohol drinkers are 6.4 times more likely to have DRPs than those who never drink (AOR = 6.40, 95% CI: 1.12–37.5, p = 0.034) (Table 5).
Bivariate and multivariate analysis of factors associated with drug- related problems among psychiatric patients admitted at hospitals in North-west Ethiopia from 1 April to July 2021.

DRP: drug-related problem; CI: confidence interval; AOR: adjusted odds ratio; ETB: Ethiopia birr; COR: crude odd ratio.
p < .05.
Discussion
This is a multi-centred cross-sectional observational study to identify the prevalence of DRPs and associated factors among adult psychiatric patients in hospitals in Northwest Ethiopia. Findings of this study revealed that 60.9% of the study participants had at least one DRP per patient. The average numbers of DRP per patient was 1.2 ± 0.4. Residence, occupation, and alcohol drinker were statically significant variables with the occurrence of DRPs.
The current study revealed that the overall prevalence of DRPs in the study subjects was 60.9%, which is low compared to similar studies in Jimma, 11 which was (74.1%) but higher than the finding from India, 28 which was 15.8%. The possible reasons for such discrepancies might be the difference in clinic setup, the guidelines’ variation, study design and professionals working in the area. In addition, the difference in inclusion and exclusion criteria might also be the reason for the difference in the prevalence of DRPs.
The result of the ADR category of DRPs was less prevalent compared to previous studies conducted in Jimma (22.2%). 11 The possible reason for this difference might be methods of assessing ADR (Naranjo scale). In addition, the current finding also showed that lesser prevalence of ADR than studies done in India and Japan, 43.5% and 63%, respectively.3,29 The possible reason is due to the setting difference (outpatient versus inpatients), difference in sociodemographic characteristics of the patients and method of assessment of ADR (severity was done using the modified Hartwig and Siegel scale), but in this study, severity was not determined.
Dose too low was a less common DRPs (8%) among the current study participants. This finding was similar to the result from the study at Jimma, Ethiopia, which was (9.9%), 11 but lower than the findings reported by Ilickovic et al. (13%). 30 This finding was closer with the result of the study conducted in Germany, 31 which reported that the least commonly encountered type of DRP in hospitalised patients with psychiatric disease was the dose-too-low category of DRPs, which accounted for 11.1% of the DRPs. Insufficient doses will result in failure to achieve the desired goal of treatment. Hence, there was a need to titrate/step up the dose of the medicines. In contrast, the dose too low in the current study is more prevalent than the findings from Brazil (2.2%). 32 This discrepancy was most likely due to a difference in socio-demographics of the study participants, a lack of institutional guidelines and professional experience working in the study area. Similarly, the dose too low category of DRPs identified by the current research was higher compared to the results from Denmark. 33 This difference might be due to the difference in the socio-demographics of the study participants, the professionals working in the area, the difference in monitoring of the laboratory (organ function test) and the availability of the medicines.
Through the assessment of different types of DRPs by trained clinical pharmacists through the helping of clinical practise guidelines, the pharmacist was also involved in the intervention recommendations according to the types and extent of the DRPs.
The results obtained from multivariate logistic regression indicated that rural residence, self-employment, and current alcohol drinkers were significantly associated with the occurrence of DRP. Patients who live in rural areas were about 1.96 times more likely to develop drug-related problems compared to patients who lived in urban areas. The highest risk of DRPs in rural areas might be due to the inadequate access to health information because of the long distances to reach the health facilities. The other possible reasons might be medicine information in rural areas is limited and has implications for rural people of low education attainment. Appropriate interventions should focus on providing outreach programmes and rigorous pharmacovigilance. Patients who were alcohol drinkers were found to be 6.4 times more likely to have DRPs than those who never drank alcohol. The interactions between alcohol and psychiatric medicines can lead to drug-related consequences. Individuals with psychiatric disorders are particularly vulnerable to drug related problems (DRPs) because of their psychotropic medicine, which are typically taken over long periods and which are known to have pharmacokinetics and pharmacodynamics interactions with alcohol. 34
Those who were self-employed were 6.0 times more likely to experience DRPs than those who were government or private organisation employees (AOR = 6.0, 95% CI: 1.0–36.9, p = 0.035). The possible reason for this might be; self-employed is poor understanding of the instruction of the medicine usage and fear of disbeliefs on the medicine effectiveness led to non-adherence to the medicine.
Generally, the extent and severity of DRPs might have different multidirectional reasons even though the practise guidelines used to determine the DRPs were similar across comparative studies; the way patients approach, differences in settings, practitioners’ experience and patient demographics may be different across different settings globally, which are also determinant factors for the extent and types of different DRPs. Therefore, any interventions towards resolving these problems could be individualised and address multidirectional contributing factors.
Strength and limitation of the study
One of the strengths of the current study is its multicentre nature, which increases the generalisability of the findings. Giving timely intervention to the identified DRPs is also a strength that resulted in the resolution of a majority of DRPs. The shorter duration of the study period is a limitation of the current study.
Conclusion
The prevalence of drug-related problems among adult psychiatric patients admitted to psychiatric wards was found to be high. The rural area residence, occupation of self-employed and Alcohol drinkers were independent predictors of DRPs. Health care providers could be focusing on counselling patients to avoid alcohol consumption while on anti-psychiatry medicines. Strengthening of clinical pharmacy services should be given due emphasis to prevent and resolve DRPs.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221112485 – Supplemental material for Drug-related problems and associated factors among adult psychiatric inpatients in Northwest Ethiopia: Multicenter cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221112485 for Drug-related problems and associated factors among adult psychiatric inpatients in Northwest Ethiopia: Multicenter cross-sectional study by Ephrem Mebratu Dagnew, Mohammed Biset Ayalew, Gizework Alemnew Mekonnen, Alehegn Bishaw Geremew and Ousman Abubeker Abdela in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank the University of Gondar for funding this research project. We are also very grateful to the study participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Ethical Review Committee of School of Pharmacy, University of Gondar with reference number (SOP/123/2021).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is a master’s thesis work financially supported by the University of Gondar.
Informed consent
Written informed consent from participants was waived by the Institutional Review Board/Ethics Committee since verbal informed consent was assumed to be enough prior to initiation of the study. Confidentiality was ensured since they were anonymous.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.