
Abstract
Objectives:
Half of all drugs are used irrationally around the world, and about half of patients take their medications correctly. Inappropriate use of drugs leads to antibiotic resistance, medication therapy problems, and an increase in drug costs. This study aimed to assess irrational drug use and its associated factors at the outpatient pharmacy of Debre Markos Referral Hospital.
Methods:
A hospital-based cross-sectional study was used. Systematic random sampling was used as a sampling technique. The data were collected with a structured checklist. The data were entered into EPI Data Version 3.1 and analyzed using SPSS version 20. Descriptive statistics and logistic regression analysis were used for data analysis.
Results:
The average number of drugs per patient encounter was 2.14. The prevalence of antibiotics use per encounter was 39.3%. Polypharmacy was detected in 62.2% of prescriptions, and injections were prescribed in 13% of prescriptions. The percentage of drugs prescribed with a generic name was 95.5%. In multivariable logistic regression, comorbidities, professionals’ training, and prescribers’ experience were significantly associated with polypharmacy. Patient age, comorbidity, presence of chronic disease, professionals training, and type of diseases were significantly associated with antibiotic prescribing.
Conclusion:
Our findings revealed there were practices of polypharmacy and antibiotics overuse. Continuous seminars and training on rational prescribing and periodic prescription surveys are recommended to prevent irrational drug use.
Introduction
The study of medication utilization patterns involves gathering prescription data to recognize drug-related problems and resolve the problem and hence contributes to rational drug use (RDU). 1 Irrational drug use remains a serious and widespread public health problem in developing countries due to a shortage of trained personnel, knowledge gaps, and economic constraints.2–4 Resistance to antibiotics, inappropriate prescribing, inappropriate dispensing, and inappropriate use of drugs by patients in the diagnosis, prevention, and treatment of diseases are the leading public health challenges globally.5,6
According to the World Health Organization (WHO), “irrational use of medicines implies that patients get medications inappropriate to their clinical conditions, doses not that meet their requirements for the desired period.” 7 Worldwide, over half of all medicines are prescribed, dispensed, or sold inappropriately and only half of all patients take their medicine correctly. Irrational use occurs when WHO drug use indicators are not met.8–11
The use of wrong or unnecessary drug seriously affects public health worldwide. This leads to decreased treatment outcomes, drug resistance, increased treatment costs, and death.12,13 There are different methods to decrease and avoid these medication errors, including the institution of committees to develop policies on RDU, appropriate implementation, and enforced regulation of clinical guidelines, continuous monitoring, and evaluation of drug use utilization.14–16
WHO developed drug use indicators for the evaluation of drug use patterns in developing countries’ healthcare institutions.14,17 The core drug use indicators enlightening, feasible, less likely to fluctuate over time and place and are easier to measure drug use.18,19
Irrational drug use is a global problem. The problem includes prescribing using brand names, polypharmacy, overprescription of antibiotics, and overuse of injections among other practices. 20 Studies on medication use in India showed a higher prevalence of prescribing through brand names.21,22
Polypharmacy is associated with an increased risk of drug–drug interactions which may lead to adverse drug reactions (ADRs), decreased adherence of patients due to pill burden, and unnecessary high drug costs. Overprescription of antibiotics increases the risk of drug resistance and drug costs, while overuse of injections increases the risk of tissue injury and transmission of blood-borne diseases, such as HIV/AIDS and Hepatitis B. Moreover, injections are relatively more expensive than oral medications.8,20 Analysis of prescriptions and drug utilization studies can identify the problems and provide feedback to prescribers to curb the problem.8,17,20
Annually, multi-drug resistant bacteria are estimated to claim the lives of more than 20,000 patients in North America, 25,000 patients in Europe, and more than 90,000 patients in Southern Asia. 23 Deaths from drug-resistant infections are expected to increase from the current 700,000 to 10 million annually, and cost estimates are expected to be as high as US$100 trillion worldwide by 2050. 24
A study done in Australia indicated that 69% of people reported a history of injury related to injectable drug use. 24 Irrational use of medicines also include inadequate dosages, use of antimicrobials even for non-bacterial infections, excessive use of injections when oral forms are available, and inappropriate drug use. 25 Poor availability of practice guidelines, such as standard treatment guidelines (STGs), formularies, and essential drug lists (EDLs) in a health facility, can affect RDU in the facility. Inadequate continuous training for health professionals, lack of essential drugs, and workloads also can cause irrational drug use in the facility. 18
In Ghana, a study on drug use evaluation showed a high prevalence of polypharmacy, overuse of antibiotics, and underuse of drugs prescribed by their generic names. 25 Similarly, a study in Hawassa, Ethiopia, showed a high prevalence of inappropriate drug use. 8
Many studies done on drug use patterns indicated that irrational drugs use is the most challenging problem in Ethiopia. Irrational prescribing of drugs leads to misuse, overdose, underdose, toxicity, ADR, cost, and shortage of drugs at health facilities.26,27 Besides, injections were reported to be unsafe for the health care workers and patients. 28
In a study done at Jimma University Hospital, from a total of 2072 medications ordered, 58 ADRs were identified, and 47% of ADRs were due to errors in the administration of medication; 91% caused temporary harms and 9% resulted in permanent harm/death. 29
In studies done in Kenya and Zambia, age and sex of the patient, disease status of the patient, and prescriber-related factors (qualification, age, sex, years of experience, training) were the factors associated with irrational use of drugs.20,30
Despite the presence of many studies on different parts of Ethiopian irrational prescribing of drugs, studies assessing factors for irrational use of drugs are scarce. 20 Thus, the objective of this study was to determine the irrational use of drugs and associated factors at Debre Markos Referral Hospital (DMRH).
Methodology
Study area and study periods
The study was conducted at DMRH. It is located in Amhara Regional State, Northwestern Ethiopia. It is found 300 km away from Addis Ababa. The study period was from 1 September 2018 to 31 August 2019.
Study design and sample size
A hospital-based cross-sectional study design was employed to determine irrational use of drugs and its associated factors based on WHO core drug use indicators. In this study, we included 600 prescription papers for the analysis. We did not calculate the sample size, but we have used WHO recommendations for conducting drug utilization studies.8,17,20,31
Sampling technique and procedure
The study population comprised all those for whom prescriptions were dispensed from 1 September 2018 to 31 August 2019. All prescriptions were arranged based on the prescribing date and month. Prescriptions were selected using systematic random sampling at the outpatient department (OPD) pharmacy, and facility indicators were observed at each unit.
Eligibility criteria
Inclusion criteria
All prescriptions which were dispensed from 1 September 2018 to 31 August 2019 and that contain medicine were included in the study.
Exclusion criteria
Prescriptions with incomplete data and contain only medical equipment and supplies were excluded from the study.
Variables
Dependent variables
Polypharmacy, antibiotic use, and injection use were dependent variables.
Independent variables
Patient’s sex, patient’s age, prescribers’ sex and age, prescriber’s qualification, prescribers’ experience, prescribers’ training on RDU, presence of comorbidities, and chronic conditions were the independent variables.
Data collection procedures
WHO drug use indicator data compilation form was used as a tool. The data were collected with a structured checklist for prescribing and health facility indicators.30,32,33 Data regarding prescribing indicators were taken from prescription records and filled in a structured checklist. Facility indicators were collected by observation at all OPD units. Prescriber’s information was collected from their file at the human resource department.
Data processing and data analysis
The data were entered into EPI Data Version 3.1 and analyzed using SSPS version 20. The data were evaluated as per the WHO guidelines. Multivariable logistic regression was used to determine the associations of dependent variables and independent of the other. On the bivariable analysis, a p-value of each variable less than 0.25 was considered in multivariable logistic regression analysis. The cut-off point for statistical significance was set at 5% (0.05). The results were edited and presented in graphs and tables.
Results
General characteristics of study participants
A total of 600 prescriptions were included in the study. The average age of patients attended at OPD pharmacy during the study period was 35 years. Of the total participants, 323 (53.8%) were females. A total of 67 prescribers participated in the study. Regarding the prescriber’s profession, 27(40.3%) were nurses. The average age of prescribers was 34.5 years. Regarding disease-related factors, 144 (24%) patients had comorbidity and 220 (36.7%) patients had a chronic disease (Table 1).
Baseline characteristics of study participants at DMRH, 2019, N = 600.

RDU: rational drug use; GP: general practitioners.
WHO prescribing indicators
Of the 600 surveyed prescriptions, 225(37.5%) prescriptions had only one drug. The overall prevalence of polypharmacy was 62.2% (n = 373) (Figure 1).

Number of drugs prescribed per prescription at DMRH, from 1 September 2018 to 31 August 2019.
The mean number of drugs prescribed per patient encounter was 2.14 (SD ± 1.24). The percentage of patients with an antibiotic was 39.3%. The overall usage of injections was 13% (Table 2).
Core drug use indicators at DMRH, 2019, N = 600.

DMRH: Debre Markos Referral Hospital; EDL: essential drug list; WHO: World Health Organization.
Common antibiotics prescribed at the outpatient pharmacy
From total prescribed antibiotics, Amoxicillin and Ciprofloxacin were prescribed frequently; the least prescribed antibiotics were Clarithromycin and Ceftriaxone (Table 3).
Commonly prescribed antibiotics at DMRH, 2019.

DMRH: Debre Markos Referral Hospital.
Factors associated with drug use patterns
Factors associated with polypharmacy
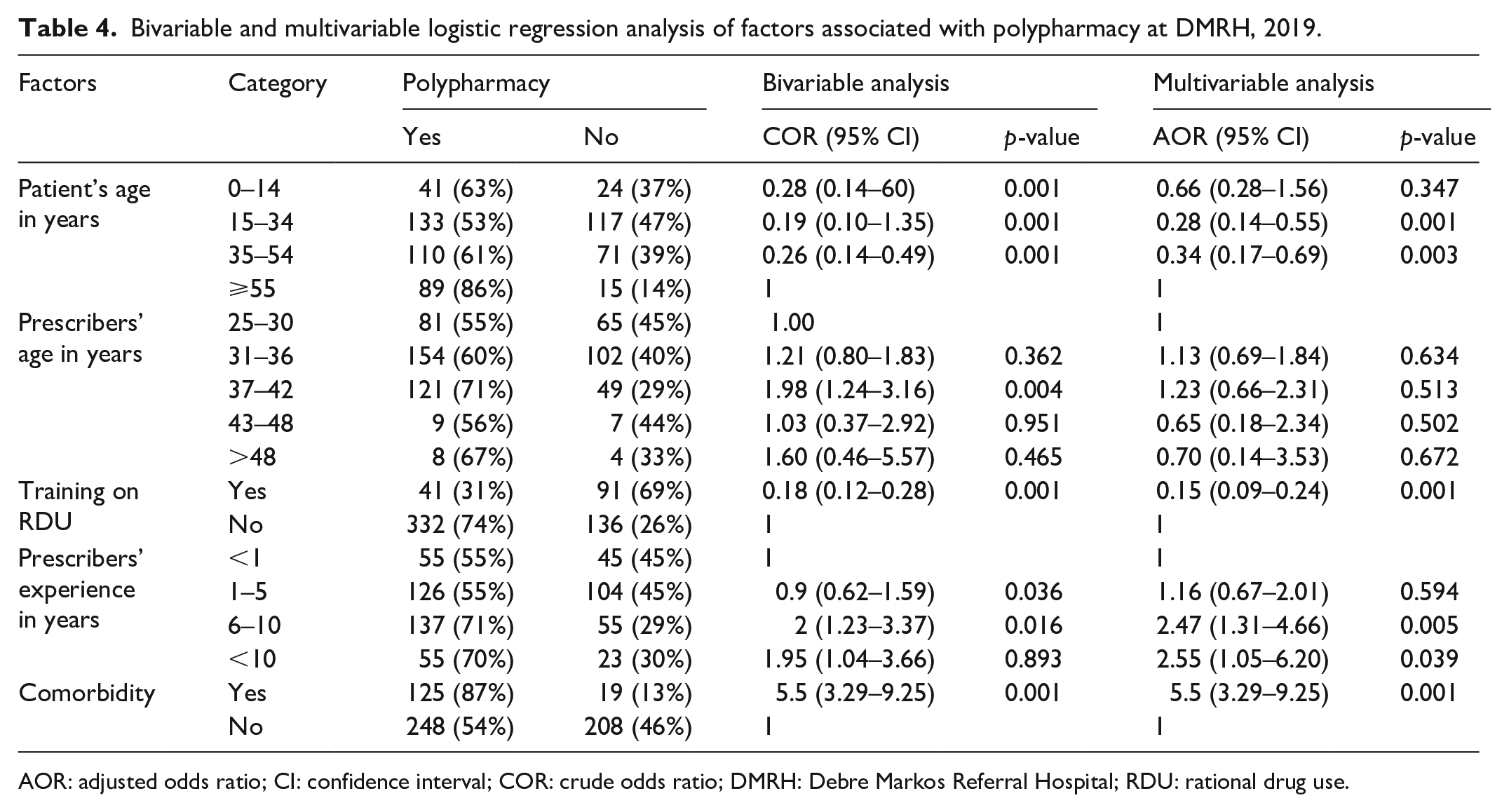
After adjusting for confounders, patients age from 15 to 34 years (AOR = 0.28; 95% CI: 0.14–0.55; p < 0.001) and age 35–54 years (AOR = 0.34; 95% CI: 0.17–0.69; p < 0.001) were significantly associated with polypharmacy. Presence of comorbidity (AOR = 5; 95% CI: 2.81–8.88; p < 0.001) and prescribers having training on RDU (AOR = 0.15; 95% CI: 0.09–0.24; p < 0.001) were also significantly associated with polypharmacy. Similarly, prescribers having the experience of 6–10 years (AOR = 2.47; 95% CI: 1.31–4.66; p < 0.005) and having experience of more than 10 years (AOR = 2.55; 95% CI: 1.05–6.20; p < 0.039) were significantly associated with polypharmacy (Table 4).
Bivariable and multivariable logistic regression analysis of factors associated with polypharmacy at DMRH, 2019.
AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; DMRH: Debre Markos Referral Hospital; RDU: rational drug use.
Factors associated with antibiotic prescribing
Patient age, presence of comorbidities, presence of chronic conditions, and having training were all significantly associated with antibiotic prescribing. Patient age from 35 to 54 years (AOR = 0.31; 95% CI: 0.16–0.61; p < 0.001) and ⩾ 55 years (AOR = 0.24; 95% CI: 0.11–0.53; p < 0.001) were significantly associated with antibiotic. Presence of comorbidities (AOR = 3.48; 95% CI: 2.07–5.85; p < 0.001) and presence of chronic conditions (AOR = 0.09; 95% CI: 0.05–0.15; p < 0.003) were significantly associated with antibiotics drug use. Similarly, having training on RDU (AOR = 0.49; 95% CI: 0.29–0.83; p < 0.008) was significantly associated with antibiotic prescribing (Table 5).
Bivariable and multivariable logistic regression analysis of factors associated with antibiotic prescribing at DMRH, 2019.

AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; DMRH: Debre Markos Referral Hospital; GP: general practitioners; RDU: rational drug use.
Factors associated with injection drug use
On multiple logistic regression, prescriber sex (female) (AOR = 0.42; 95% CI: 0.25–0.72; p < 0.002) and presence of chronic conditions (AOR = 5.11; 95% CI: 2.94–8.87; p < 0.001) showed significant association with injectable drug use (Table 6).
Bivariable and multivariable logistic regression analysis of factors associated with injection drug prescribing at DMRH, 2019.

AOR: adjusted odds ratio; CI: confidence interval; COR: crude odds ratio; DMRH: Debre Markos Referral Hospital; GP: general practitioners, RDU: rational drug use.
Discussion
The average number of drugs prescribed per patient encounter was 2.14 (SD ± 1.24). The result was higher than WHO recommendation (1.6–1.8), a study done at Tigray region, Hiwot Fana Harar, Asmara, and Northwest Amhara, but lower compared to the findings of studies done in Saudi Publican, Zambia, Kenya, Ghana, and Tikur Anbessa.17,20,25,30,34–38
Patient age was associated with polypharmacy. Patients who were 15–34 years and 35–54 years were 72% and 64% less likely to have polypharmacy compared with those aged ⩾ 55 years, respectively. This could be the prevalence of several diseases that may occur in older patients who need treatment with many drugs. This finding is similar to the studies done in Kenya and Spain.20,33 The Ethiopian government should give special attention since these segments of the population are at higher risk for polypharmacy which may result in drug–drug interactions, ADRs, noncompliance, and increased cost of treatment.
Prescribers having 6–10 years and more than 10 years of experience were 2.45 and 2.55 times more likely to prescribe multiple drugs, respectively, compared with those having less experience. The finding is supported by a study done in Kenya, Spain, and Lagos.6,20,33 Prescribers having training about RDU were 85% less likely to prescribe polypharmacy as supported by a similar study done in Malaysia. 39 Continuous trainings should be given to prescribers and other health care professionals on how to decrease polypharmacy, injectables, and overuse of antibiotics. Prescriptions for comorbid conditions were five times more likely to have polypharmacy compared to prescriptions having no comorbidities. This was expected since comorbidities involve several diseases that may require different drugs to manage, hence leading to polypharmacy. There was a similar study in Kenya and Swedish.20,40
In total, 39.3% of prescriptions had at least one antibiotic prescribed, which shows a high prevalence of antibiotic prescribing in the Hospital. The prevalence of antibiotic prescribing is very high compared to WHO standards.24,25,41 This percentage was lower compared to that reported in Saudi Publican Zambia, South India, Kenya, Asmara, Tigray region Hawassa, Hiwot Fana Harar, Northwest Amhara, higher compared to that reported in Madurai, Ghana, and Tikur Anbessa.2,8,17,30,31,34–38,42 Patient age was associated with antibiotic drug prescribing. Patients aged from 35 to 54 years and age ⩾ 55 years were 69% and 76% less likely to have antibiotics compared to younger patients as supported by the study in Kenya and Addis Ababa.20,41 This could be due to the prevalence of more infectious diseases than chronic diseases at a younger age.
A prescriber who has training was 51% less likely to prescribe antibiotics compared to a prescriber without training. This is similar to a study done in London. 43 Presence of comorbid conditions was strongly associated with a higher prevalence of antibiotics use. Prescriptions for comorbid conditions were 3.48 times more likely to have an antibiotic compared to the ones with no comorbidities. This result was similar to Kenya, Asmara, and Korea.20,35,42 Prescriptions for chronic conditions were 91% less likely to have an antibiotic prescribed compared to prescriptions for non-chronic conditions. This is similar to the studies done in Kenya, Zambia, and Ghana.20,30,42 This may be explained by the observation that most of the chronic conditions were cardiorenal disorders, neuropsychiatric, and hormonal disorders, which did not necessarily require antibiotics for management.
The prevalence of injection drug use was 13%. This is similar to studies done in Northwest Amhara, Ghana, and Zambia.30,38,42 From the result of multivariable logistic regression, female prescribers were 58% less likely to prescribe injection drugs for patients compared to male prescriber, but studies done in Asmara and China showed females prescribed injections more injections than males.35,44 Presence of chronic conditions was 5.11 times more likely to have injected drugs than non-chronic condition patients.
Prescribing using generic names was widely practiced in the Hospital (95.5%) but it was low compared to WHO standard (100%), a study done at Tigray region, Hiwot Fana Harar, Kenya, and Ghana, but higher compared to a study done at Tikur Anbessa and Northwest Amhara region.17,20,25,36–38
However, 99.8% of the drugs were prescribed from the Hospital drug list; this indicated that there was high compliance with the EDL of the hospital during prescribing. This could be attributed to the availability of copies of EDL in the facility and probably hospital drug and therapeutic committees work strongly in continuous updated and distributed of copies of EDL for all Hospital unities (100%) and comparable to studies done in Hawassa, Tikur Anbessa, better than a study done Northwest Amhara.8,37,38
Irrational use of drugs leads to wastage of drugs and other healthcare resources. Our study has identified different factors which lead to irrational use of drugs. Based on our findings, we recommend the following strategies for policymakers to enhance rational use of medicines. An education program promoting RDU should be delivered through different ways. Special attention should be given on rational use of antibiotics since antimicrobial resistance is currently a major public health problem. The hospital should provide training on rational use of drugs for health care professionals. The EDL and formulary of the hospital should be updated periodically. In addition, the hospital’s drug and therapeutic committee should evaluate the hospitals drug use patterns on a regular basis.
Limitation of study
First, as this study involved a retrospective prescription review, we might have missed unrecorded data. Second, patient care indicators were not assessed in this study. Third, there was no sample size calculation for this study. We took 600 prescription papers as per WHO recommendations for drug utilization studies. The study may not be adequately powered.
Conclusion
Our study finding showed prescribing indicators deviate from the standard values recommended by WHO. There is polypharmacy, overuse of antibiotics, and the use of non-generic name drugs. Lack of continuous education, presence of comorbid diseases, and prescriber educational status were identified to have contributed to irrational drug use. As a result, an education program promoting RDU is recommended. The hospital must take note of this finding and implement a training program that will provide both medical and pharmacy personnel with up-to-date information on RDU and how to act on it. In addition, the hospital’s drug use should be evaluated on a regular basis.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211025146 – Supplemental material for Irrational drug use and its associated factors at Debre Markos Referral Hospital’s outpatient pharmacy in East Gojjam, Northwest Ethiopia
Supplemental material, sj-pdf-1-smo-10.1177_20503121211025146 for Irrational drug use and its associated factors at Debre Markos Referral Hospital’s outpatient pharmacy in East Gojjam, Northwest Ethiopia by Legese Melku, Muluken Wubetu and Bekalu Dessie in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank data collectors and Debre Markos Referral Hospital staffs.
Data availability statement
The data used for this study are available from the corresponding author upon request (Bekalu
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the research and ethics review committee of College of Health Sciences, Debre Markos University. The ethics approval number given was ጤሳኮ/1017/16/12.
Informed consent
In this study, consent could not be obtained for patient’s prescription review due to retrospective nature and it was difficult to contact patients since they live in remote rural areas, so an official permission letter was obtained from Debre Markos Referral Hospital to conduct the study. Confidentiality of patients’ data was assured. According to the Declaration Helsinki 64th WMA General Assembly, Fortaleza, Brazil in October 2013, verbal informed consent is acceptable. Informed verbal consent was prepared and approved by the research and ethics review committee of College of Health Sciences, Debre Markos University; therefore, informed verbal consent was obtained from health care professionals and hospital administrators before being involved in the study. Participants were informed that they could leave the study at any stage of the interview. Confidentiality of data was assured for participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.