
Abstract
Introduction/Objectives:
Male involvement in family planning refers to all organizational actions focused on men as a distinct group to increase the acceptability and uptake of family planning among either sex. Despite the growing evidence of male involvement in increasing family planning uptake among couples, a little success has been achieved in Ethiopia, especially in rural areas. Hence, this study aimed to assess male involvement in family planning and its associated factors among currently married men in selected rural areas of Eastern Ethiopia.
Methods:
A community-based cross-sectional survey was conducted among 577 randomly selected currently married men, using a simple random sampling method in randomly selected rural districts of Eastern Ethiopia. Data were collected using a pretested interviewer-administered questionnaire. The collected data were entered into a computer using Epi-Data Version 3.1. The analysis was performed using the Statistical Package for the social sciences software version 21. Logistic regression analysis was used to analyze the association between the dependent and independent variables. Finally, adjusted odds ratio with 95% confidence intervals at P-value < 0.05 was considered to be significantly associated with the outcome variable.
Results:
Out of 577, a total of, 555 married men were included in the study, resulting in a response rate of 96.2%. The magnitude of male involvement in family planning use was 59.3% (95% confidence interval: 47.1, 68. 2). Ever use of family planning by a spouse (adjusted odds ratio: 2.37; 95% confidence interval: 1.59, 3.52), ever discussion of spouse on sexual and reproductive health/family planning issues (adjusted odds ratio: 2.05; 95% confidence interval: 1.40, 3.02), and the husband’s approval of family planning (adjusted odds ratio: 2.45; 95% confidence interval: 1.34, 4.96) were significantly associated with higher odds of male involvement in family planning use than their counterparts.
Conclusion:
The number of men involved in the family planning was low. Ever use of family planning methods by a spouse, ever discussion of spouse on sexual and reproductive health/family planning issues, and husband approval on family planning use were found to be important predictors of male involvement in family planning use. To improve modern family planning uptake among men and women, it is imperative to include men in family planning programs, such as family planning messaging, sensitizations, and services.
Introduction
Male involvement in family planning (FP) refers to all organizational actions focused on men as a distinct group to increase the acceptability and uptake of FP among either sex. It encompasses men being involved either in decision making, approving it, or supporting their spouse to use FP. 1 FP, which is the conscious effort by an individual or couple to limit or space the number of children they have through the use of contraceptive methods has many benefits including economic development, maternal and child health improvement, educational advances, and women’s empowerment through career aspirations with control over their fertility desires.2–5 The Sustainable Development Goal (SDG) 3 considers reproductive, maternal and child health as priority agenda, which will not be attained without FP. Involving men in FP is one of a crucial public policy intervention to achieve national and SDGs.6,7
Women face many obstacles, including lack of access to information and healthcare services, opposition from their husbands, communities, and misperceptions about side effects. Oppositions to FP from their husbands or noninvolvement of men in FP are the major reasons for the women not to use contraception despite their desire to do so.8,9 In traditional societies, family limitation and negotiation over sexual matters may not be considered respectable subjects, and it is not uncommon for husbands and wives to avoid the discussion of contraception or sexual matters. 10
Advancement has been seen since the 1994 International Conference on Population Development (ICPD) involving men in FP services worldwide. Interest in men’s involvement in reproductive health has increased among countries. Special efforts were made to focus on men’s shared accountability to promote their active involvement in sexual and reproductive health (SRH) issues including decision making in FP.4,5
Despite the growing evidence of involving men in reproductive health decision making, fertility rates, and unmet need for FP remain high in many sub-Saharan African countries.8,9
Evidence suggested that involving men in FP improves spousal communication, increase acceptance, and continuation of FP methods through pathways of increased knowledge or decreased male opposition.8,11–13
The matters of FP have not been left only for women. Husband is the most important decision maker in developing countries predicting future women’s fertility desires to limit or space birth. Apart from the role of decision makers in the family, their actions in terms of abuse or neglect have a direct impact on the health of their partners and children.14–16
The Ethiopian Federal Minister of Health also emphasized on men engagement in FP as a strategy to improve contraceptive rate. 17 Although Ethiopia has adopted the approach in line with the agenda of ICPD in 1994, a little success has been achieved in engaging men in fertility issues, especially in rural areas. Despite contraceptive utilization increase internationally, Ethiopia’s current contraceptive prevalence rate (CPR) remains 36% and 22% of currently married women have an unmet need for FP services. 2
In countries like Ethiopia, where the majority of the population are living in rural, with high women illiteracy rate, limited reproductive negotiation, and dominated by the patriarchal system using an innovative approach of communication strategies to increase FP utilization is very crucial. Understanding the role of male involvement in FP could contribute to efforts aimed at increasing the uptake of FP in the region. Therefore, this study aimed to assess the level of husband’s involvement in FP use among currently married men in selected rural areas of Eastern Ethiopia.
Materials and methods
Study area and period
East Hararghe is one of the zones of the Oromia regional state, located in the Eastern part of Ethiopia, 526 km from Addis Ababa. This zone has a total population of 2,723,850, of whom 1,383,198 are men and 1,340,652 women; East Hararge has a population density of 151.87. While 216,943 or 8.27% are urban inhabitants, a further 30,215 or 1.11% are pastoralists. Approximately, a total of 580,735 households were residents of this zone which results in an average of 4.69 persons to a household, and 560,223 housing units. 13 The study was conducted in January 1–30, 2020.
Study design and population
A community-based cross-sectional study was conducted among currently married men living in selected kebeles (a small administrative unit in Ethiopia) in the rural parts of the Eastern Hararghe Zone. All currently married men living in selected kebeles and available during the data collection period were included in the study, while men with mental and serious health problems, those who reported infertility, and those who were not available at home during the data collection period after three visits were excluded from the study.
Sample size determination and sampling procedure
The sample size was calculated using single population proportion formula with the assumption of proportion (p) for male involvement in FP to be 65.5% (i.e. p = 0.655) from previous study, 8 95% confidence interval (CI) with 5% tolerable error and design effect of 1.5 and a 10% nonresponse rate, which gave the final sample size of 577 participants.
Multi-stage sampling techniques were used in this study. Among the woredas (an administrative division of Ethiopia) in the study area, three were selected using lottery methods. Then one kebele from each woreda was selected by simple random sampling. Proportional allocation for each kebele was used to provide an equal chance. All eligible households in each selected kebele were selected using systematic random sampling. From the eligible households, study participants (currently married men) were selected using simple random sampling.
Data collection procedure and quality control
Data were collected using a structured and interviewer-administered questionnaire adapted from a national study and modified to the study setting after the pretest, which consisted of men’s sociodemographic information, knowledge about contraception, reproductive history, contraceptive use, fertility desire, couple’s communication, and decision making on FP.1,2,18,19 Three health extension workers and two supervisors have participated in data collection.
Data were collected by the local language version of the tool and every participant was interviewed in a private area where they were comfortable answering the question freely. To control the data quality, supervisors and data collectors were trained for 2 days. The tools were pretested on 5% (29 participants) of the total sample size and modifications were made to our setup based on the pretest results. The collected data were checked daily and double data entries were performed.
Study variables
Independent/explanatory variables
Operational definitions
Statistical analysis
The collected data were entered into a computer using the Epi-Data Version 3.1. Data analysis was performed using the Statistical Package for the social sciences (SPSS) software version 21. Frequencies of variables were generated; and tabulation and percentages were used to illustrate the study findings. Bivariate and multivariate logistic regression analyses were used to analyze the association between the dependent and independent variables. The outcome variable (male involvement in FP use) was coded as a yes/no response and each explanatory variable was tested for association in bivariate analyses. Covariates with a P-value < 0.25 were retained and entered into the multivariable logistic regression analysis using a forward selection and backward elimination approach. Hosmer and Lemeshow’s goodness-of-fit test was used to assess whether the necessary assumptions were fulfilled. Adjusted odds ratio (AOR) with 95% confidence intervals using a P-value < 0.05 was considered as statistically significant association with the outcome variable.
Ethical considerations
Ethical approval was obtained from the Haramaya University College of health and medical sciences institutional health research ethics review committee. Formal letters were written to all concerned authorities and permission was secured at all levels. Informed, voluntary, written, and signed consent was obtained from each respondent after explaining the purpose and procedure of the study. All the basic principles of human research ethics (respect for persons, beneficence, voluntary participation, confidentiality, and justice) were respected. The study was conducted in accordance with the principle of the Declaration of Helsinki.
Results
Sociodemographic characteristics of respondents
Out of 577, a total of 555 married men participated in the study which gave a response rate of 96.2%. The mean age of participants was 26.6 (±standard deviation = 4.62). A total of, 459 (82.7%) participants were from the Oromo ethnic group. A total of, 471 (84.9%) were Muslim. Concerning educational status 307 (55.3%) participants had no formal education (Table 1).
Demographic characteristics of currently married men in the study area (n = 555), 2020.

USD: United States Dollar; ETB-Ethiopian Birr.
Others: Guraghe, Tigre, Somali; **others: Catholic, Adventists, Pagans; ***others: Laborers, merchants, and gov’t employees.
Knowledge toward modern contraceptive methods
Most of the study participants 521 (93.9%) had heard about modern FP methods. Regarding the knowledge of study participants toward modern FP methods, 507 (91.4%) knew at least one type of modern FP method. The most popular method was the injection 491 (94.2%), implants 447 (85.8%), pills 367 (70.4%), intra uterine contraceptive device (IUCD) 79 (15.2%), condom 24 (4.6%), and permanent FP methods 4 (0.8%), respectively.
Contraceptive use among study participants
The study findings showed that 243 (43.8%) of the study participants’ spouses ever used modern contraceptive methods. The current utilization of modern contraceptive methods among spouses was 102 (18.4%). Concerning the types of modern contraceptive methods, 50 (49%) used injectable, 45 (44.1%) implants, 5 (4.9%) pills, and 2 (2%) used IUCD. However, none of the participants reported the use of condoms or permanent methods. More than two-fifths (43.7%) of the spouses used contraceptive methods for spacing birth while 27% used contraceptive method to limit birth. The remaining participants used it for health benefits or treatment. Reason for not using FP among spouse were, inconvenience for use, want to have a child, husband disapproval, fear of side effect, and some others.
Male involvement in FP
Three hundred and twenty-nine (59.3% (95% CI: 47.1, 68. 2)) of the participants were involved in the FP use. Concerning decision-making of FP method use, 202 (69.4%) replied that they made decisions jointly while only 70 (24.1%) replied that spouses made decisions by themselves alone (Table 2).
Communication, involvement in decision making and approval of FP use among currently married men (n = 555), 2020.
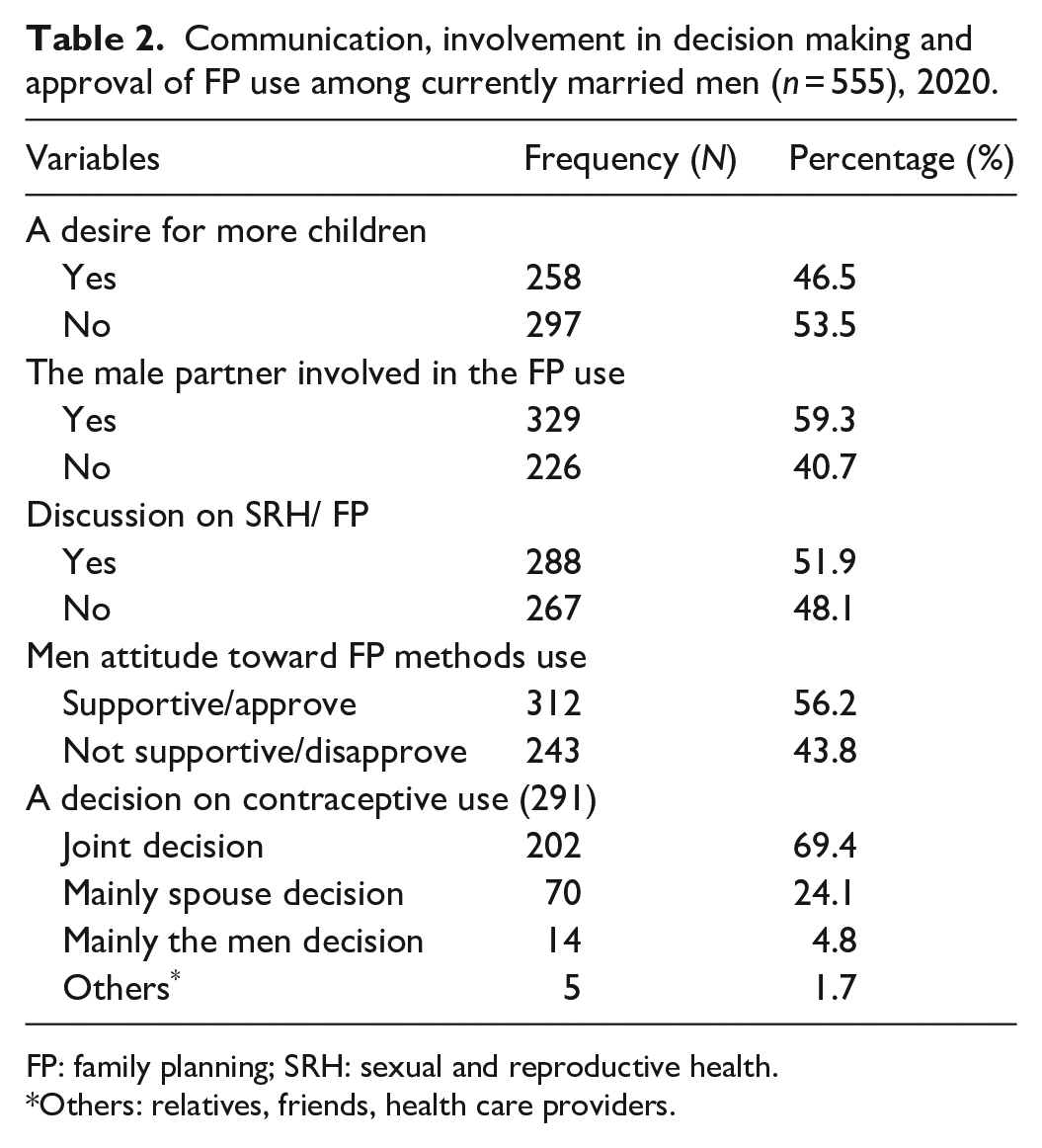
FP: family planning; SRH: sexual and reproductive health.
Others: relatives, friends, health care providers.
Factors associated with male involvement in FP use
A binary logistic regression analysis of some independent variables with the dependent variable was performed. Men whose spouses ever used FP methods were 2.37 times more likely (AOR = 2.37 95%, CI: 1.59, 3.52) to be involved in FP use than those men whose spouses had never used FP methods.
Men who discussed about SRH/FP with their spouse were 2 times more likely (AOR = 2.053, 95% CI: 1.40, 3.02) to be involved in FP use than those who did not discussed with their spouse. Men who approved/supported FP use were 2.5 times more likely (AOR = 2.45, 95% CI: 1.34, 4.96) to be involved in FP use than men who did not approve (Tables 3 and 4).
Bi-variable analysis of factors associated with male involvement in modern FP use (n = 555), 2020.
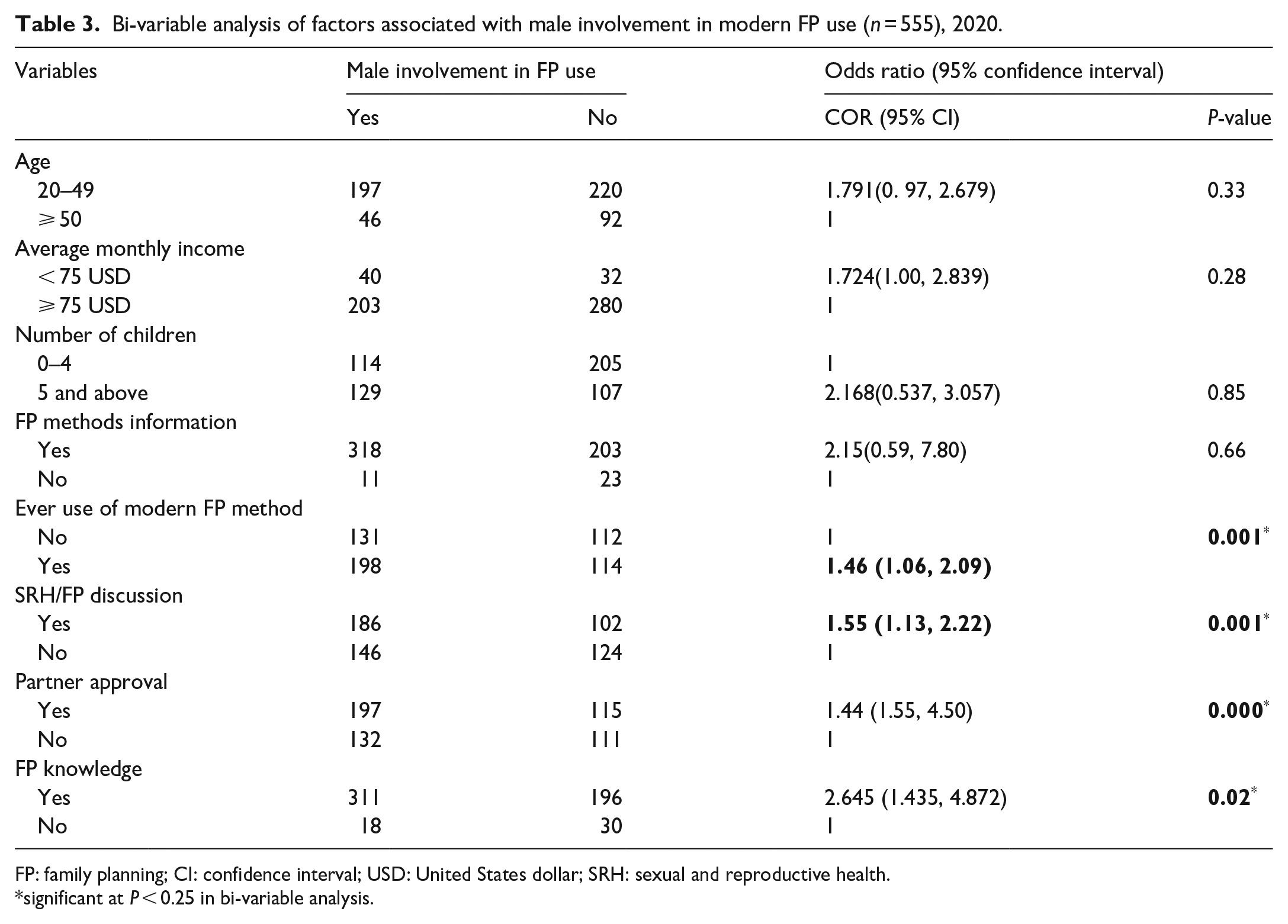
FP: family planning; CI: confidence interval; USD: United States dollar; SRH: sexual and reproductive health.
significant at P < 0.25 in bi-variable analysis.
Multivariate analysis of factors associated with male involvement in modern FP use (n = 555), 2020.
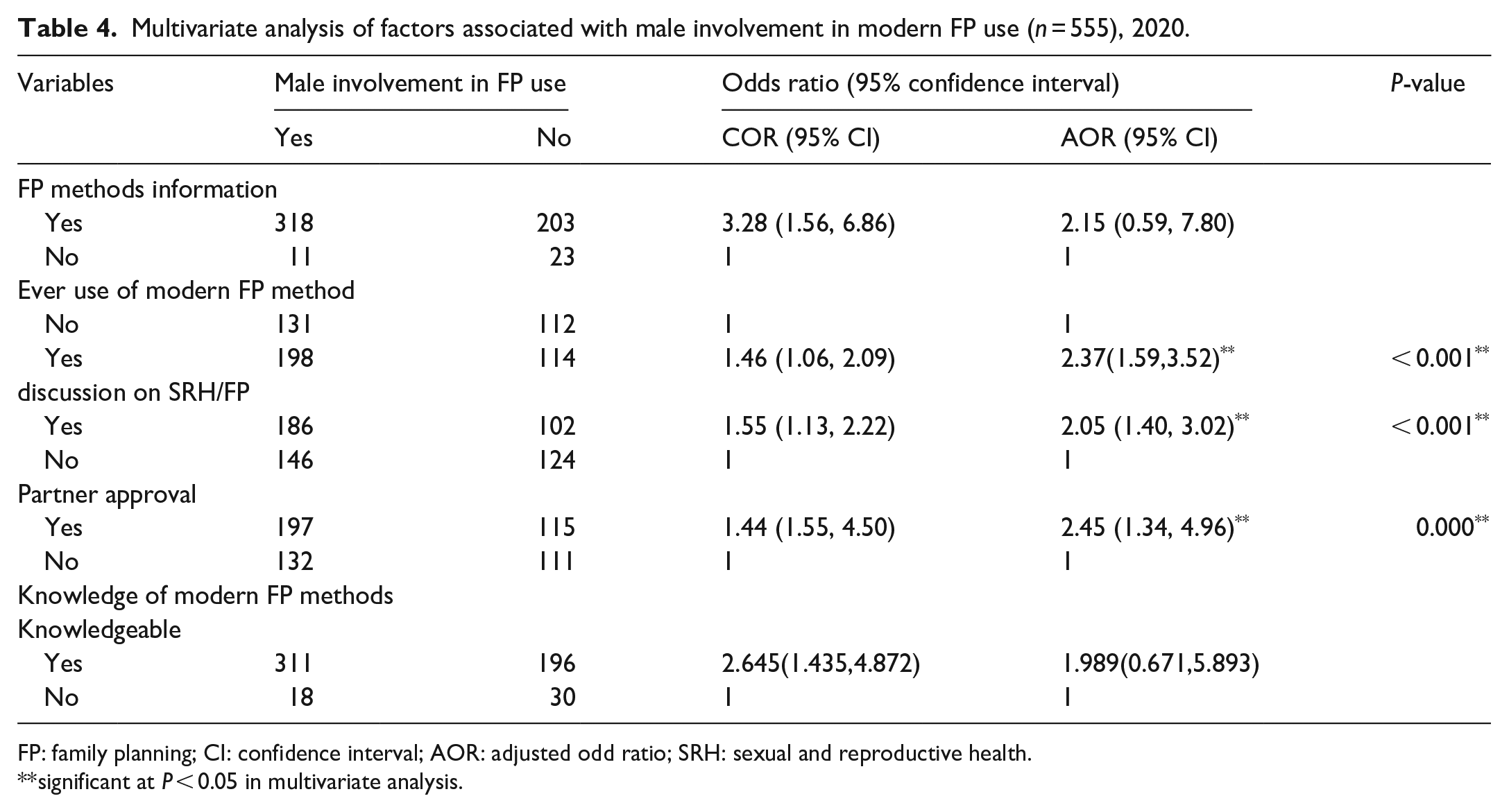
FP: family planning; CI: confidence interval; AOR: adjusted odd ratio; SRH: sexual and reproductive health.
significant at P < 0.05 in multivariate analysis.
Discussion
This study assessed men’s involvement in FP use and its associated factors in selected rural areas of Eastern Hararge, Eastern Ethiopia. The study showed that 59.3% of men were involved in FP use. This finding is in line with finding from Cameroon (57.2%). 21 However, it is higher than that of Afar, Ethiopia (42.2%), 1 and Kenya (46.24%). 22 This might be due to increased awareness and knowledge of the community about contraception with an increase in time, increased access to FP services, or increased involvement of NGOs, private, and religious organizations in the advocacy and provision of FP services. This is evidenced with some studies in Ethiopia that suggest awareness of FP in the general population are increasing substantially from time-to-time.1,18–20,23
The study finding is lower than other study findings from Agaro, 18 Ethiopia which showed that (70.3%) of couples approve the use of FP. This discrepancy might be due to differences in the study setting and the sociocultural difference between these communities. In our study area, there were higher number of Muslim religion followers as indicated in sociodemographic distribution on (Table 1), which commonly prohibits modern FP use, than other religions. This is evidenced by other studies conducted in different context that revealed the prevailing social and cultural practices of gender role, norms, and religion as the deep root of maternal health problems including male involvement in FP.19,24
The study showed that men whose spouse ever used FP methods were about 2.37 times more likely (AOR = 2.34 95%, CI: 1.59, 3.52) to be involved in FP use than those men whose spouse had never used FP methods. This can be due to the fact that ever users of modern FP methods were more familiar with the benefits of modern FP methods. Hence, they are more likely to use/continue the methods than their counterparts. This finding is in line with other study findings from Afar and Debremarkos, Ethiopia.1,19
This study revealed that men who discussed on SRH/FP with their spouse were 2 times more likely (AOR = 2.05, 95% CI: 1.40, 3.02) to be involved in FP use than those men who did not discuss with their spouse.
This finding is in agreement with finding from Agaro town, south-west Ethiopia. 18 This may be because joint decisions for FP are based on spousal communication implying that when couples communicate effectively they are more likely to jointly agree on what type of contraceptive method to use, how many children to have, and the space between their offspring. This study is supported by various studies demonstrated that women who discuss FP issues with their husbands are more likely to have their partner’s approval on FP and are more likely to use a modern method of contraception.17,19,25
This study also showed that men who approved/supported FP use were about 2.5 times more likely (AOR = 2.45, 95% CI: 1.34, 4.96) to be involved in FP services utilization than men who did not approve. This is in line with other studies conducted in Ethiopia and Ghana.19,25,26 This might be because women who have their partner’s approval on FP use are more likely to use a FP method without any fear of opposition.
Finally, the findings of this study might suffer from social desirability bias because it is based on men’s perceived role; their role may be inflated. Since the interview included only men it was also difficult to know if the women covertly use FP without their partner approval. With this limitation, the research can be interpreted and used in the local context and will serve as a component for planning a program.
Conclusion
The number of men involved in the FP was low. Ever use of FP methods by a spouse, a couple’s discussion on SRH/FP, and husband approval of FP use were found to be significant factors of male involvement in the FP use. To improve modern FP uptake among men and women, it is imperative to include men in all FP programs, including men in FP messaging, sensitizations, and services.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221094178 – Supplemental material for Male involvement in family planning use and associated factors among currently married men in rural Eastern Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121221094178 for Male involvement in family planning use and associated factors among currently married men in rural Eastern Ethiopia by Teshale Mulatu, Yitagesu Sintayehu, Yadeta Dessie and Merga Dheresa in SAGE Open Medicine
Footnotes
Acknowledgements
The authors express our deepest thanks to Haramaya University College of Health and Medical Science for their facilitation to conduct this study by their constructive comments and ethical review. They are also grateful to study participants, data collectors, and site supervisors for their contribution.
Author contributions
TM, MD, YS, and YD conceived the study and involved in the study design, reviewed the article, analysis, report writing, and drafted the manuscript. All authors have read and approved the final manuscript.
Availability of data and materials
All related data are presented fully within the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Institute of Health Research and Ethical Review Committee of Haramaya University College of Medical and Health Sciences with the reference number IHRERC/116/2018.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by CIRHT-Ethiopia (Center for International Reproductive Health Training) the affiliate of Michigan university. The funding organization has no role in designing the study, data collection, analysis, and its interpretation, protocol writing, and submission.
Informed consent
Written informed consent was obtained from study participants after explaining the purpose and procedure of the study. Formal letters were written to all concerned authorities and permission was secured at all levels. Informed, voluntary, written, and signed consent was obtained from each respondent after explaining the purpose and procedure of the study. All the basic principles of human research ethics (respect of persons, beneficence, voluntary participation, confidentiality, and justice) were respected.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.