
Abstract
Introduction:
Controversies exist regarding the relationship between body fat and disease activity in patients with rheumatoid arthritis. The evaluation of the disease is critical for establishing treatment and prognosis. Fat mass could be a predictive factor for poor prognosis in rheumatoid arthritis because of its association with low- and high-grade inflammation.
Objective:
To evaluate the correlation between fat mass values and disease activity in patients with rheumatoid arthritis.
Materials and methods:
This was a cross-sectional study. Eighty female patients diagnosed with rheumatoid arthritis (American College of Rheumatology of 1987) were evaluated. For each one, the evaluation determined fat mass using bioelectrical impedance analysis and disease activity using the Disease Activity Score on 28 joints (DAS28).
Results:
The mean age was 59.11 ± 9.92 years, with an average disease duration of 14.13 ± 10.13 years; 85% of patients showed a high body fat percentage. Pearson’s correlation between DAS28 values and fat mass was r = 0.035 (p = 0.76).
Conclusion:
The levels of DAS28 showed no correlation with fat mass percentage. Further studies are required to clarify the factors that can modify these levels.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease. In addition to symptoms in the joints, the disease can be related to changes in body composition, such as obesity and rheumatoid cachexia, especially when the disease is active.1,2 RA is one of the most frequent autoimmune diseases with a prevalence of 1.3% worldwide; in Latin America, it ranges from 0.4% to 1.6%, and, in Mexico, 1.6% of the population is affected.3 –5
Body weight and body mass index (BMI) may contribute to the high disability risk associated with RA.6,7 Regulation of body weight in RA patients is a complex issue 8 because overweight and obesity are states of low-grade chronic inflammation associated with a diminution in physical capacities, increased pain, comorbidities, and increased inflammation markers.2,9 Therefore, it is important to assess body composition to achieve a greater understanding of the physiology of these changes and the general clinical conditions of these patients by means of a combination of anthropometric measurements (including height, weight, BMI, waist circumference, percentage of fat mass (FM), hip circumference (HC), and waist-to-hip index), dual X-ray absorptiometry (DXA), and bioelectrical impedance analysis (BIA).10,11
A high BMI is associated with radiographic joint damage that is less severe in the early stages of the disease as well as decreased mortality related to cardiovascular disease. Hence, a high BMI is considered a protective factor. 8 In contrast, body composition alterations, such as obesity and FM, are associated with worse results.9,12,13 However, a lower BMI is associated with lower survival, 8 which indicates a bidirectional relationship between changes in body weight and disease activity in RA patients.
Nevertheless, BMI is only an approximate measurement of body fat, and it does not detect all individuals with increased body fat. 2 Adipose tissue is considered an active organ that sends and responds to a wide range of biological signals. 14 Likewise, systemic inflammation starts with excess adiposity along with other factors such as smoking. 15 However, high-degree inflammation in RA coexists with a higher accumulation of FM and a reduced lean mass (LM). 15
In RA, the main objectives of the existing diverse therapeutic strategies are to attain disease remission (a state in which neither inflammatory activity nor progression of the structural damage exists) or a low level of clinical activity. The evaluation of disease activity is of fundamental importance for therapeutic decision-making and the establishment of a prognosis for patients with this disease. 16 Every patient’s necessary goal is to control their disease activity in order to improve their symptoms, diminish their joint damage, prevent functional limitations, and improve their quality of life. 17
It is desirable to count individualized predictors of the course of a disease. In addition to the determination of the autoantibodies of a disease, the rheumatoid factors, and the antibodies against cyclic citrullinated peptides, other diverse factors can predict the development of more severe diseases. These include advanced age at the onset of disease, female sex, smoking, genetics, degree of physical disability, and early erosive disease. 2 Hence, predicting future clinical results based on these factors could help optimize disease management.2,18
The association of factors such as body fat and BMI with the clinical course of RA is still a debated issue, and the clinical applications of the currently available data are not entirely clear. Consequently, little is known about adiposity in rheumatic disease.2,8 Our objective was to evaluate the specific correlation between body fat percentage and RA disease activity.
Material and methods
Study design
This is a cross-sectional study.
Study population
Eighty incident and prevalent female patients aged ⩾18 years diagnosed with RA according to the criteria of the American College of Rheumatology of 1987 (ACR87) 19 were studied. The inclusion period was 18 months. Patients were cared for in the Unidad de Investigación Biomédica 02 in the Unidad Médica de Alta Especialidad, Hospital de Especialidades Centro Medico Nacional de Occidente IMSS. Patients excluded were those with chronic infections, cancer, thyroid disease, psychiatric diseases, and pregnancy.
Disease characteristics
A rheumatologist examined the patients. Information was recorded according to clinical and demographic characteristics, board-certified time of disease duration (years), and disease activity defined by the Disease Activity Score on 28 joints (DAS28) 2 (permission was requested online at https://www.das-score.nl/en/useful-links and https://eprovide.mapi-trust.org/, which allow for direct use of the instrument for academic purposes). In addition, DAS28 scores were classified as follows: disease remission (<2.6), low disease activity (⩽2.6–<3.2), moderate activity (⩽3.2–⩽5.1), and high activity (>5.1). 20 The use of disease-modifying antirheumatic drugs (DMARDs), glucocorticoids, non-steroidal anti-inflammatory drugs (NSAIDs), and biological agents was recorded as pharmacological therapies.
Anthropometric measurements
A trained nutritionist performed the anthropometric measurements. Evaluations included height in centimeters (cm) and weight in kilograms (kg). These were measured using a wall stadiometer graded in centimeters with a 0.5-cm accuracy (SECA 206, Hamburg, Germany) and a digital precision scale with a 0.1-kg accuracy and a scale with a range of 0–150 kg with an induction frequency of 50 kHz 21 (TANITA BC-533 Inner Scan Body Composition Monitor, IL, USA), respectively. This scale also provided FM percentages. FM was measured as a percentage and dichotomized as <30% (healthy FM) and ⩾30% (high FM). 22 Body weight was measured in kg, with patients wearing light clothing and no shoes, and the patients relaxed their arms next to their trunk for the foot-foot measurements (metatarsus-calcaneus). 23 The patients attended the scale measurements and were instructed to: not ingest liquids in the 4 h before the test, to urinate 30 min before the test, not to perform strenuous exercise 12 h before the test, not to consume alcoholic beverages 48 h prior, not to take diuretics 7 days before the test, and not to wear metallic elements on or in their body (watches, rings, bracelets, earrings, etc.). 21
From the height and weight measurements, BMI values were classified according to the definition provided by the World Health Organization: low weight (<18.5 kg/m2), healthy weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obesity (⩾30 kg/m2). 24 Abdominal circumference and HC were measured (cm) using a flexible fiberglass metric tape (GULICK) with a 1-mm accuracy, as established by the International Society for the Advancement of Kinanthropometry (ISAK). 25
Statistical analysis
Quantitative variables were described as mean value ± standard deviation, and qualitative variables were described as frequencies and percentages. Quantitative variable comparisons among groups were performed using Student’s t-test, and qualitative variables were analyzed using the chi-square test. Pearson’s correlation was used to correlate the percentages of FM with the DAS28 scores. Statistical significance was set at p ⩽ 0.05. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) for Windows version 18.
Ethical considerations
The study protocol was approved by the Ethics Committee (CLIES R-2014-1301-79). All patients signed an informed consent form.
Results
The study included 80 female patients. The average age of the patients was 59.11 ± 9.92 years, the mean weight was 66.93 ± 10.87 kg, and the mean height was 1.54 ± 0.06 m. The mean BMI of the patients was 28.17 ± 3.94 kg/m2, and 58 patients were overweight or obese (72.6%). The mean percentage of FM was 36.96 ± 6.17, and 85% of the population presented a high FM percentage (⩾30%). Among the disease’s clinical characteristics, we found a duration time of 14.13 ± 10.13 years, with DAS28 values of 3.08 ± 1.08; 49 patients (61.3%) were classified as having active disease. Of these active patients, 24 were in the low disease activity group, 20 were in the moderate activity group, and only 5 were in the high activity group. Regarding the treatment established at the time of evaluation, 62 patients (76.3%) received glucocorticoids and 65 (81.3%) received some NSAIDs. Seventy-five patients (93.8%) were on DMARDs, and only eight patients (10%) received biological agent therapy. Complementary general characteristics are described in Table 1.
Clinical-demographic characteristics of 80 women with rheumatoid arthritis (RA) at the time of inclusion in the study.

RA: rheumatoid arthritis; BMI: body mass index; DAS28: Disease Activity Score in 28 joints; NSAIDs: non-steroidal anti-inflammatory drugs; DISMD: disease-modifying drug.
Qualitative variables are expressed as frequencies (%); quantitative variables are expressed as mean values and standard deviation.
The correlation analysis between FM percentages and the examined variables showed a correlation with body composition parameters, such as BMI (r = 0.835, p < 0.001), and with the waist-to-hip index (WHI) (r = 0.281, p = 0.01). Table 2 shows that there was no correlation with disease characteristics.
Correlation of FM percentage and body composition parameters with disease characteristics in 80 AR patients.

FM: fat mass; BMI: body mass index; AR: rheumatoid arthritis; DAS28: Disease Activity Score in 28 joints.
Table 3 presents a comparison between patients with healthy body fat (<30%) and those with high body fat (⩾30%). Among the variables of interest, a significant difference was observed in weight (p = 0.001) and BMI (p < 0.001).
Comparison of anthropometric and clinical characteristics of 80 RA patients, categorized by percentage of body fat.
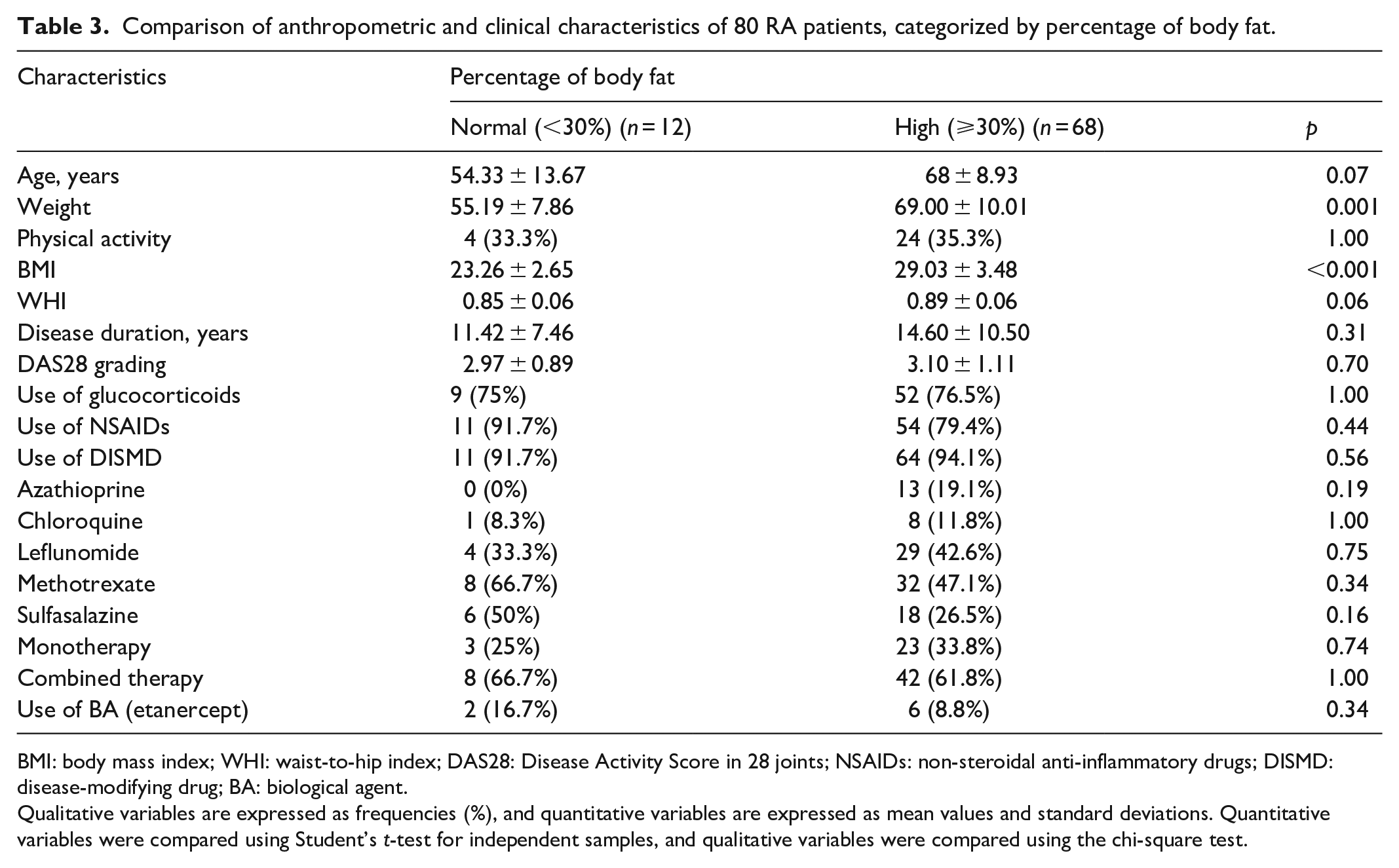
BMI: body mass index; WHI: waist-to-hip index; DAS28: Disease Activity Score in 28 joints; NSAIDs: non-steroidal anti-inflammatory drugs; DISMD: disease-modifying drug; BA: biological agent.
Qualitative variables are expressed as frequencies (%), and quantitative variables are expressed as mean values and standard deviations. Quantitative variables were compared using Student’s t-test for independent samples, and qualitative variables were compared using the chi-square test.
Table 4 depicts the comparison of RA characteristics according to disease activity or remission of the disease measured using the DAS28. An association was observed in patients in remission with more physical activity (p = 0.05).
Comparison of anthropometric and clinical characteristics of the disease in 80 RA patients according to remission or activity measured by DAS28 scores.

BMI: body mass index; WHI: waist-to-hip index; DAS28: Disease Activity Score in 28 joints; NSAIDs: non-steroidal anti-inflammatory drugs; DISMD: disease-modifying drug; BA: biological agent; NA: not available.
Qualitative variables are expressed as frequencies (%), and quantitative variables are expressed as mean values and standard deviations. Quantitative variables were compared using Student’s t-test for independent samples, and qualitative variables were compared using the chi-square test.
Multivariate analysis was performed to assess the risk of developing a body FM >30% in terms of other plausible variables. No association was found with either the DAS28 score or with the other variables introduced in the model (Table 5).
Regression analysis assessing the association of independent variables with the development of increased body FM.

FM: fat mass; OR: odds ratio; IC95%: interval of confidence at 95%; DAS28: Disease Activity Score in 28 joints; DISMD: disease-modifying drug.
Covariants included in the analysis corresponded to those with biological feasibility for developing body FM percentage. The model was adjusted for age and disease duration.
Discussion
This study provides information on the specific correlation of disease activity, assessed using the DAS28, with percentage of FM. According to the literature review, we did not find studies in which the main objective was to determine the associations between variables capable of producing alterations in body fat. Moreover, the FM register was a descriptive variable reported among the related variables (BMI, adiposity index, waist, and WHI). In addition, the epidemiological designs were of the longitudinal type (clinical assays or cohorts).26 –32
Variables related to FM have been reported discrepantly among authors, which could be due to the fact that RA is more prevalent in women.29,33 This study provides information on these aspects in women. The data analyzed in this study agree with previous literature reports that reported patterns of low correlation values.27,29,32
Although being overweight significantly decreases the chance of achieving reasonable disease control,34,35 this pattern of low correlation values between FM percentage and DAS28 scores may be associated with the use of therapeutics (93.8% of this study population was being treated with the DMARDs regimen, whereas 10% used biological agents).29,32 Both treatment modalities have immunosuppressive effects that act by controlling the immune response; hence, they can regulate and diminish inflammation, leading to disease improvement and changing the natural history of the disease.14,36 These treatments also affect the regulation of FM and LM (an effect that has been studied scarcely in short-lasting treatments), which could be a factor that could explain the results of this study. 27 In addition, in this study, we describe and analyze the therapies used at the time of evaluation, including DMARDs and biological agents; these are characteristics not typically included in the analyses of most reported studies.26 –33,36,37
However, we found that 68/80 patients had a high percentage of FM (⩾30%); 22 however, we found no association between the clinical and anthropometric characteristics. No correlation was found between FM percentages and DAS28 scores. The multivariate analysis, which was adjusted for age and disease duration, of the biological feasibility variables yielded no risk association for these variables.
Among the limitations of this study, we found that the sample size and the power analysis were not calculated, resulting in a small final sample size that could miss low mean disease activity differences. Its cross-sectional nature impaired us from identifying variations between FM percentage and disease activity measurements in the follow-up; these factors could modify the decrease in inflammatory activity and increase FM. We planned the study with a dichotomized value for FM according to Frankenfield et al., 22 and unfortunately, we could not convert the DAS28 values to other scores.
In addition, body composition assessment via BIA is not the standard method of measurement; however, when tested against the reference measurement method of hydrostatic weighing, 22 BIA values were found to correlate with this standard measurement by 90%.
In addition, we decided to use the ACR 1987 RA criteria because of the long disease durations in several cases that were extending before the ACR 2010 RA criteria became available, thus leading to a lower sensitivity for early RA cases. Regarding disease activity and health assessment measurements, we did not include the SDAI (Simplified Disease Activity Index), CDAI (Clinical Disease Activity Index), and HAQ (Health Assessment Questionnaire).
The factors potentially contributing to the differences found in the literature-reported studies include physical activity 7 and its relationship with disease activity, resulting in less time spent performing physical activity, and thus the greater the disease activity. 38 Other factors include the time between the FM and LM measurements 33 as well as the presence of metabolic syndrome and even cardiovascular diseases.9,27 These factors, together with adipokines,14,32 could influence the distribution of FM percentage.
Conclusion
This article shows the lack of a relationship between disease activity as measured by DAS28 levels and FM percentage. As a significant issue, because the group of studied patients was composed of both incident and prevalent cases of rheumatoid arthritis, more longitudinal studies of incident cases are required to clarify the factors that could modify the relationship between DAS28 values and FM percentages.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review board from CLIES 1301 (R-2016-1301-94).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially financed by a research grant (FIS/IMSS/PROT/G16/1581).
Informed consent
Written informed consent was obtained from all subjects before the study.