
Abstract
Objectives:
The extension of healthy life expectancy is an important policy issue in Japan. This study aimed to clarify the association between subjective health and healthy life expectancy and identify the factors that improve subjective health of child-rearing-aged adults in Japan.
Methods:
A cross-sectional study was conducted. We used data from 2718 participants of the Japanese General Social Survey 2009 Life Course Study. The mean age was 35.5 ± 4.10 years, and 56% were female. Multivariate logistic regression analysis was performed on subjective health, which was treated as a binary variable when calculating healthy life expectancy as an objective variable. The predictors were gender, age, marital status, number of family members living in the home, household income, mental health score, age of youngest child, and the person from whom one seeks help. The prefecture where the participants resided was treated as a control variable.
Results:
There was no association between individual subjective health and healthy life expectancy. Mental health score (measured by the Mental Health Inventory-5, MHI-5) was significantly associated with subjective health. With a MHI-5 score of ⩽ 10 points as the reference criterion, as the score increased, the odds ratio of subjective health increased, and for MHI-5 scores ⩾ 16 points, odds ratio was 14.14 (confidence interval: 7.57–26.38).
Conclusion:
Among the child-rearing-aged adults, prefectural healthy life expectancy was not associated with individual subjective health. Mental health was significantly associated with subjective health and may be underestimated in calculating healthy life expectancy.
Introduction
In Japan, a country with high life expectancy, it is considered important not only to live long, but also to have a healthy life. In addition, the extension of healthy life expectancy (HLE) is a national policy goal. 1 There are three measures of HLE that are used as policy targets in Japan: (1) disability-free life expectancy without activity limitation, (2) life expectancy with self-perceived health, and (3) disability-free life expectancy without need for care. HLE is calculated using the Sullivan method, 2 and the variables used in this calculation include the population, number of deaths, life table for Japan, and variables that define health conditions. The health condition variables are crucial because they are combined with other variables in calculating HLE to categorize life expectancy into healthy and unhealthy periods. There are two types of variables that define health conditions: subjective criteria, in which the health condition is assessed using a self-administered questionnaire, and objective criteria, in which the health condition is determined by a third party’s confirmation. However, since the objective criteria are based on Japan’s long-term care insurance system, the statistics are generally only available for people aged 65 years or above. Moreover, the national guidelines 1 provide HLE statistics using subjective criteria. Among them, high disability-free life expectancy without activity limitation, which indicates a typical HLE, is associated with a high proportion of residents with a high perception of subjective health in the target area. 3 It has been pointed out since the 1950s that the results of regional and individual analyses are inconsistent; this is referred to as an ecological fallacy. 4 Furthermore, as HLE can only be calculated at the regional level, prior studies are limited in that the factors contributing to the extension of HLE at the individual level have not been discussed. It is important to clarify the factors related to health at the individual level because policy decisions for extending HLE based on analyses at the regional level may not adequately translate into individuals’ health promotion. Thus, the purpose of this study was to clarify the relationship between regional HLE and individuals’ subjective health, which is the most important health-defining variable for calculating HLE. Therefore, subjective health, instead of HLE, was used as the outcome variable, and the analysis was carried out at the individual level, considering the effect of regional HLE. Exploring factors that aid the improvement of individual subjective health, considering the method used to calculate HLE, will help to examine the policy measures of local governments for extending HLE.
Subjective health, as an outcome variable in this study, is a simple and useful indicator of overall health conditions. A typical question of subjective health scale asks, “What is your current state of health care?” and responses are measured on a Likert-type scale with four or five options (e.g. “not good” to “very good”).5–7 Many studies have shown that subjective health predicts morbidity of cardiovascular and cerebrovascular diseases 8 and mortality.5,9,10 Furthermore, it has been reported that a person’s subjective health is more predictive of future decline in physical function than a doctor’s measure of health status based on objective health data. 11
Past studies that have explored the epidemiological characteristics of subjective health by age have shown the following: although mental and physical health both contribute significantly to adolescent self-rated health, mental health appears to make a greater contribution, which is opposite to what has been observed among adults; 12 the dissemination of information related to health promotion and positive health habits are important determinants of self-assessed health among the middle-aged and older adults; 13 older adults value positive subjective health factors, such as energy and happiness, more than negative factors, such as fatigue and sadness;14,15 and young people value the aspect of “health behavior” while older adults value the aspect of “health problem” as a referent of subjective health. 6
Since subjective health scales 16 were originally developed for the field of geriatrics, many previous studies have focused on older adults. However, a survey conducted by Healthy Life Expectancy Promotion Section, Health Care and Welfare Department, Shiga Prefecture, Japan, to clarify the factors contributing to the extension of HLE reported that the subjective health of child-rearing-aged adults in their 30s and 40s tends to be poor. 17 Child-rearing-aged adults experience many stressful life events, such as marriage, pregnancy, and childbirth, the effects of which may have a strong influence on their subjective health.
Therefore, in this study, we investigated the following two questions: (1) Is there an association between the subjective health of child-rearing-aged adults and the HLE of their region of residence? and (2) What are the factors related to the subjective health of child-rearing-aged adults in Japan, considering the effect of HLE? The results of this study will provide a basis for measures to promote the health of the child-rearing-aged adults and extend their HLE.
Methods
Study design and dataset
This study used a cross-sectional observational design. Secondary data from the Japanese General Social Survey 2009 Life Course Study (JGSS-2009LCS) were used. 18 The JGSS was launched in 2000 with the aim of continuously conducting comprehensive social surveys in Japan and creating open data that can be analyzed by researchers who lack the opportunity and resources to conduct a nationwide survey. The JGSS was developed by the JGSS Research Center of Osaka University of Commerce and conducted by Central Research Services, Inc. The survey is certified by the Ministry of Education, Culture, Sports, Science and Technology; categorized as an official survey; and reviewed by the Japan Information Processing Development Corporation (JIPDEC); thus, it is conducted with appropriate privacy protection measures. This survey was conducted in a non-medical research area, and although there is no requirement for an ethics review in this research area, the basic policy for the protection of personal information was formulated and observed. 19
The JGSS-2009LCS is a survey of adults aged 28–42 years (as of 31 December 2008), which focused on diverse ways of working and living. Sampling of the JGSS secondary data was based on a stratified two-step sampling method in which Japan was geographically divided into six blocks, and each block was stratified into four survey sites on a population scale. The participants at all 394 survey sites were extracted from the voter registry (or basic resident registry, if voter registry was not available) using the equal interval extraction method. The selection criteria applied to people born between 1966 and 1980. There were no exclusion criteria, but if two or more people from the same household were likely to be selected, they were disqualified. This sampling method used the same survey areas as those used in the 2006 Census, and it was set such that approximately 15 people were selected from each area. The total number of targets was 6000, and even with a response rate as low as 50%, detailed analysis could be made by gender at 5-year intervals. Since this study involves the secondary use of open data, it was not possible to clearly specify a desired sample size. However, applying the formula given below with a reliability coefficient (k) = 1.96 (95%) and response ratio (P) = 50%, the required sample size (N) is 400 cases when the allowable sampling error (E) is 5%, and it is 1111 cases, if E is 3%. Therefore, it is considered that the sample size of 2718 cases in this study is appropriate for ensuring representativeness and conducting robust statistical analyses.
The calculation formula for sample size is as follows:

where k is the sampling error, E is the reliability coefficient, and P is the response ratio.
A hybrid survey of interviews (Supplementary File 1) 20 and questionnaires (Supplementary File 2) 21 was conducted with the participants. The pre-test was conducted with 30 individuals using these questionnaires. The items related to work experience were partially revised, but it was confirmed that there were no problems with the survey items and survey time.
Measures
Subjective health was used as the outcome variable and was assessed by asking the participants, “What is your current state of health care?” The response was measured on a 5-point visual analog scale, ranging from 1 (good) to 5 (bad). For calculating HLE, subjective health was converted to a binary variable, where a score of 1–3 was defined as “healthy” and a score of 4–5 as “unhealthy.” 3
Predictive variables were gender, age, marital status, number of family members living in the home, household income, mental health score, age of youngest child, and the person from whom one seeks help. Mental health was a dependent variable, and it was assessed using the Mental Health Inventory-5 (MHI-5) developed by Berwick et al. 22 The MHI-5 was developed as a scale to measure the mental health of workers, but it was an appropriate scale for this study because of its efficiency, as child-rearing-aged adults have a high employment ratio and generally lead very busy lives. This scale asks how often one has had the following five experiences in the past month: (1) a state of being very nervous, (2) a state of feeling hopelessly depressed, (3) a state of being calm, (4) a state of having fallen into a melancholy mood, and (5) a state of being happy. Answers were measured on a 5-point Likert-type scale, ranging from “always” to “not at all.” The scores of questions (1) and (2) were inverted, and the total score ranged from 5 to 25 points. Several cut-off values for the MHI-5 have been suggested for categorizing respondents into high-risk and low-risk groups,22–25 and the most used cut-off point is 13 (if converting to 100 points, it is 52).22,23
Household annual income and mental health scores were divided into four categories by quartiles. The age of the youngest child was classified as ⩽ 5 years (preschoolers), 6–11 years (elementary school students), 12–14 years (junior high-school students), and ⩾ 15 years (high-school students and above); those with no children indicated that they had none. The variable regarding the person from whom one seeks help was assessed through the following question: “When you were suffering from a large number of personal worries or stress to whom did you ask for help?” The responses obtained were classified as parents/siblings (family of orientation), spouse/lover/children (family of procreation), friends/neighbors (non-expert third party), and professional/others. Family of orientation refers to the family an individual is born into or grows up in, and family of procreation refers to the family that one creates through marriage, childbirth, or adoption.
The prefecture where the participant resided was used as a control variable to analyze the association between their subjective health and HLE. The values for healthy life expectancies were those calculated and published by the national research team; 26 most Japanese local governments quote these HLE values. The prefectures where the participants resided were divided into the following four categories, according to the length of HLE by quartiles: high, somewhat high, somewhat low, and low. For these four categories, the average HLE of each category was compared by a one-way analysis of variance and significant differences were confirmed (Table 1). Although the data used in this study were collected in 2009, HLE as a policy target by Japanese local governments is only calculated every 3 years and was not calculated in 2009; the figures that have been published are for 2010, 2013, and 2016. Although HLE was not calculated for 2009, we confirmed that there was no significant change in HLE by analyzing the trend over the three time-points of 2010, 2013, and 2019; thus, we decided to use the average of the 3 years.
Grouping by average healthy life expectancy in 2010, 2013, and 2016 by prefecture in Japan.

ANOVA: analysis of variance.
p < 0.05; **p < 0.01.
Statistical analyses
The participants’ basic attributes and predictive variables were cross tabulated with subjective health, and a chi-square test was performed to analyze these associations. The variance inflation factor between participants’ characteristics was calculated to verify whether multicollinearity problems occurred between the predictive variables and control variables. Univariate logistic regression analysis was performed using subjective health as an outcome variable and each one of the following variables as a predictor: gender, age, marital status, number of family members living together, household income, mental health score, age of youngest child, the person from whom one seeks help, and prefecture classification by HLE. Multivariate logistic regression analysis was performed using participants’ demographic variables and the variables that were significantly associated with subjective health in the univariate analysis as predictors. In addition, to analyze the association between subjective health and HLE, we used the prefecture classification by HLE as a control variable. In all analyses, missing values were excluded pairwise. All statistical analyses were conducted using SPSS Statistics version 27 (IBM, Chicago, USA) and R (The R Foundation for Statistical Computing, Vienna, Austria).
Results
Response rate and analysis targets
Of the 6000 targeted respondents, 664 were unable to take part due to reasons including unknown moving residence/address, long absence, and sick/hospitalization. The questionnaire was distributed to 5336 participants and 2727 responses were received (recovery rate: 51.1%). Excluding 9 cases with missing answers for subjective health, 2718 cases were included in the analysis (Figure 1). When the results were compared with the national census and the population by gender and by 3-year age groups, the residual was −2.24 ± 0.70 for men and 2.24 ± 2.48 for women, thereby indicating that there was no significant bias, although there was a slight tendency for women aged 40–42 years to be overrepresented. The sampling bias was judged to be small because the recovery rate achieved the target and the residual was small. The most common reason for the lack of responses was “reject” at 50.2%, followed by “temporary absence” at 28.6% and “relocation” at 10.1%. In addition, the proportion of “temporary absence” and “relocation” was higher among the younger participants.
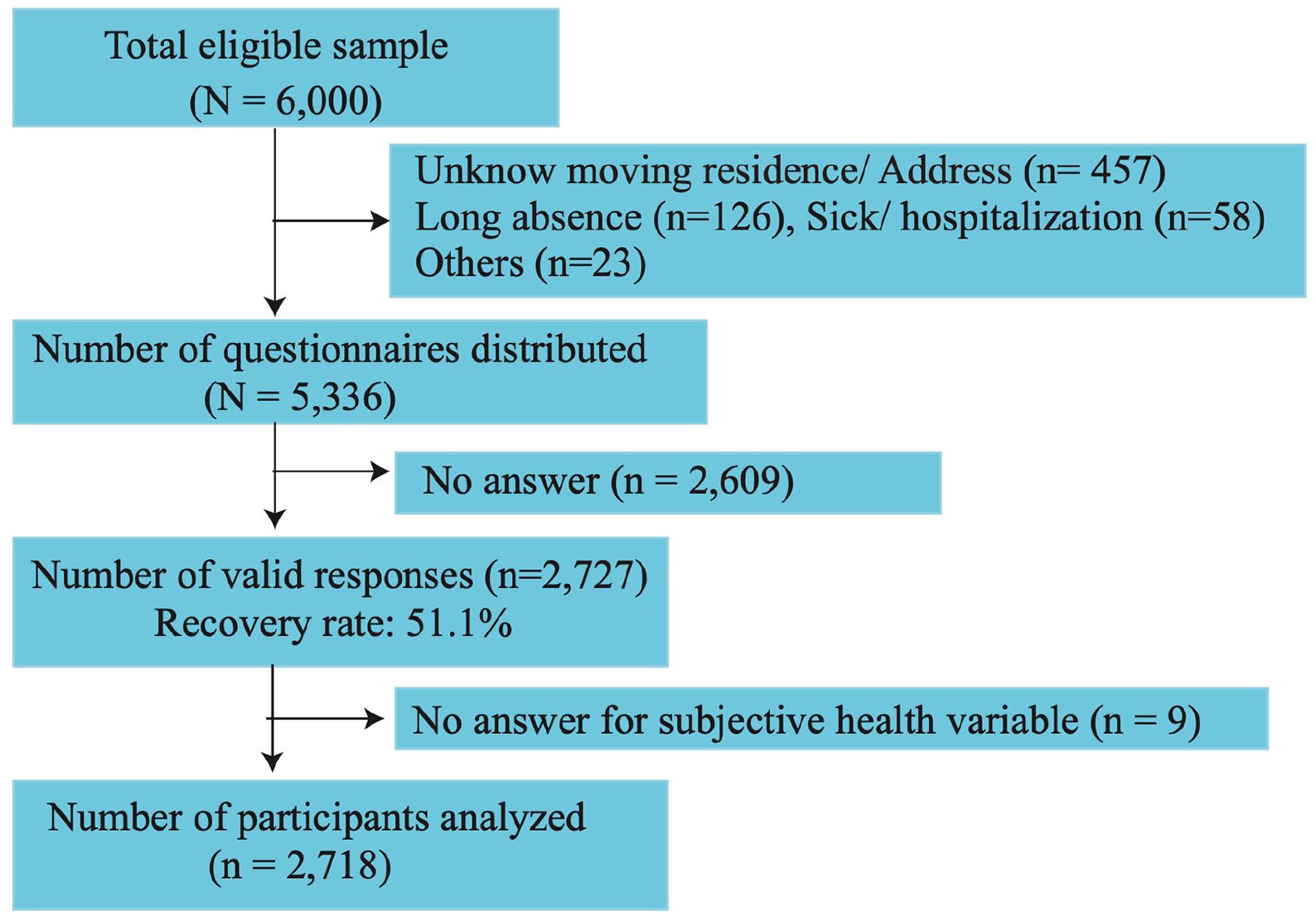
Study flow chart.
Participants’ attributes and the association with subjective health
The mean age of the participants was 35.47 ± 4.09 years, and 56.0% were female. Of these, 69.8% were married and four family members was the most common number of people living in the home (31.2%), followed by three (24.4%), and five (14.9%). Although 35.6% of the participants had no children, among the families with children, the youngest child in most families was ⩽ 5 years old (32.4%), followed by 6–11 years (23.9%). When faced with personal concerns or stress, 10.4% had no one to consult, whereas among those who consulted someone, family of procreation (spouse/lover/children) was the most common source of personal counseling (46.0%), followed by friends/neighbors (25.2%; Table 2).
Basic attributes including participants’ categorization into healthy/unhealthy and results of chi-square tests (N = 2718).

MHI-5: Mental Health Inventory-5; HLE: healthy life expectancy.
In the chi-square test, variables such as gender (p = 0.019), marital status (p = 0.000), number of family members living together (p = 0.009), the MHI-5 score (p = 0.000), age of the youngest child (p = 0.000), and the person from whom one seeks help were each significantly associated with subjective health. Men (13.6%) were more likely to be unhealthy compared to women (10.7%). In terms of marital status, compared with married individuals (9.6%), bereaved/divorced (19.8%) and unmarried (17.1%) individuals had a higher percentage of those who were unhealthy. As for family composition, those living alone (16.7%) or with one other person (16.8%) tended to be unhealthy, and in terms of the youngest child’s age, families with the youngest child aged 12–14 years (16.4%) or ⩾ 15 years (16.1%) tended to be unhealthy. The proportion of unhealthy persons tended to increase as the score on MHI-5 increased, with the proportion being 27.8% for MHI-5 scores of 16 points and higher. Participants who sought help from parents/siblings (9.2%) had the lowest percentage of unhealthy people and those who sought help from professionals/others (36.2%) had the highest percentage. In addition, the prefecture classification by HLE did not yield a significant association with subjective health.
Association between subjective health and predictive variables in the univariate analysis
The MHI-5 score was significantly associated with subjective health (Table 3). The odds ratios (ORs) of being unhealthy increased with higher MHI-5 scores. Participants with a score of 16 points or higher may have had a problem with mental health because the OR was remarkably higher than the other criteria. In addition, those who sought help from parents/siblings (OR = 0.53, CI = 0.35–0.82) or spouse/lover/children (OR = 0.45, CI = 0.32–0.65) had a low OR of poor subjective health, while those who sought help from professionals/others (OR = 2.54, CI = 1.37–4.71) had a high OR.
The results of univariate and multivariate logistic regression analyses with subjective health as the outcome variable.

OR: odds ratio; CI: confidence interval; MHI-5: Mental Health Inventory-5; HLE: healthy life expectancy.
p < 0.05; **p < 0.01;・p < 0.10.
The OR for females was significant at 0.76 (CI = 0.60–0.96) with males as a reference group. Regarding family environments (reference = married participants), those who were separated/bereaved (OR = 2.33, CI = 1.45–3.74) or unmarried (OR = 1.95, CI = 1.52–2.50) had significantly higher OR. In addition, participants living together with a total of three (OR = 0.56, CI = 0.35–0.89) or four (OR = 0.50, CI = 0.30–0.86) people had a lower OR. With having no children as the reference group, the OR was lower for participants with children ⩽ 5 years (OR = 0.44, CI = 0.32–0.59) or 6–11 years (OR = 0.69, CI = 0.52–0.93). Prefecture classification by HLE had no significant OR.
Association between subjective health and predictive variables in the multivariate analysis
The variance inflation factor between the predictive and control variables was 1.33 ± 0.42 (maximum = 2.18, minimum = 1.03), which indicated that there was no problem with multicollinearity. Age, gender, and household income variables have been frequently used as predictors in prior studies, and other predictors were significantly associated with subjective health in the chi-square test and univariate analysis. Prefectural classification by HLE was the main control variable in this study. Therefore, a multivariate logistic regression analysis was performed using all predictors and control variables used in the univariate analysis.
The MHI-5 score significantly contributed to the “unhealthy” rate in subjective health. The risk of poor subjective health increased with the mental health scores as follows: 11–13 points (OR = 3.55, 95% CI: 1.80–7.00), 14–15 points (OR = 4.86, 95% CI: 2.48–9.51), and 16 points or higher (OR: 14.14, 95% CI: 7.57–26.38). In addition, compared with the person from whom one seeks help, the professionals/others group had a significantly higher OR of poor subjective health (OR = 3.81, 95% CI: 1.63–8.90). The variables of gender, marital status, number of people living together, and age of the youngest child, which were significant in the univariate analysis, were not significant in the multivariate analysis. Moreover, prefecture classification by HLE had no significant OR in the multivariate analysis.
Discussion
There was no association between individual subjective health and HLE among the child-rearing-aged adults. However, the calculation of HLE reflects the subjective health of younger people, and these rates are not negligible compared with those of older adults. Based on the proportion of healthy and unhealthy people in the National Basic Survey of Living Conditions, which measures subjective health, and the stationary population in the life table in 2016, it can be confirmed that, although the rate of unhealthy people slightly increases among the older adults, approximately 10% of people in all age groups are unhealthy, starting from the age of 30 years. 17 The Sullivan method, which is a widely used method for calculating HLE, excludes unhealthy periods from life expectancy. 2 Tokudome et al. 27 reported that although HLE in Japan has been extending linearly with life expectancy, the increase in life expectancy has been greater and unhealthy life expectancy has also been increasing. In addition, previous studies on HLE have focused on older adults, 28 and reports describing trends in Japan27,29 and overseas30,31 have not discussed younger age groups. Therefore, life expectancy has a greater impact than health conditions, and the health status of young people, including the child-rearing-aged adults, may be underestimated compared to older people.
The results of this study show that mental health has a strong influence on the subjective health of child-rearing-aged adults, which is similar to the results of studies with adolescents. 12 Adolescence is the life period when identity is established, 32 and adolescents have both developmental/behavioral problems and age-specific risks, such as family, peer, or school problems; substance misuse; early sexual activity; and risk-taking behavior. 33 As a result, adolescents tend to have mental health problems, but different types of problems arise when people reach child-rearing age. The child-rearing age is a period in which life events such as marriage, pregnancy, childbirth, and separation are likely to occur. Holmes et al.34,35 identified life events as stressors and developed a scoring scale (Social Readjustment Rating Scale) on which higher scores are associated with higher rates of illness. In other words, the simultaneous occurrence of multiple stressful life events is a major risk to health, which is likely to occur during child-rearing years.
In the univariate analysis of this study, being married, having children, and being able to consult with one’s family about personal stress or concerns were factors significantly associated with reduced risk of poor subjective health. However, these significant variables were no longer significant in the multivariate analysis, suggesting that people who were able to adjust to life events had reduced stress, while those who were unable to adjust to life events had very high stress and became unhealthy. Marriage has been reported to improve mental health, which is consistent with the results of this study, which found that the proportion of unhealthy people was lower among the married people.36,37 Several studies have examined the effects of family composition on mental health in relation to parenting stress and postpartum depression38,39 or in children,40–42 but there has been no report of subjective health in child-rearing-aged adults. In Japan, support for parents with children up to 3 years of age is provided on a regular basis, including visits to all households with newborns, as well as infant and toddler checkups with a rate of nearly 100%. However, in this study, the proportion of unhealthy people with children older than 12 years is high, and their poor health may be overlooked. This may be because the education of children in junior high and high school is the most expensive 43 and some changes in the family environment may occur due to children going to school; however, further research is desired to clarify this issue in the future.
The limitations of this study are as follows. First, causality cannot be determined because this study used a cross-sectional design. In particular, regarding the variable “the person from whom one seeks help,” although only professionals/others have a significantly high OR, this result needs to be interpreted with caution because individuals with psychological disorders may have been more likely to give this response. Second, the survey data are somewhat dated. However, Japan has seen a rising divorce rate, an increase in single-parent households, and reduced support from grandparents due to the trend toward nuclear families since the survey year, 31 and it is unlikely that the child-rearing environment has become less stressful. Therefore, we believe that there are no significant differences between the results at the time of the survey and those at present. Finally, it may have been better to use variables related to physical health in the multivariate analysis, but the secondary data did not include the appropriate variables. However, we presume that these are not major problems due to the low rate of medical history of lifestyle-related diseases and physical function problems.17,31
New findings revealed in this study suggest that mental health is significantly associated with child-rearing-aged adults who are less likely to be subject to government health measures and research, and that parents of children aged ⩾ 12 years tend to have a higher proportion of those with unhealthy subjective health. Furthermore, in the calculation process of HLE, the health status of child-rearing-aged adults may be underestimated, and a more detailed investigation is desired.
Conclusion
Among child-rearing-aged adults, prefectural HLE was not associated with individual subjective health. Mental health had a strong influence on the subjective health of child-rearing-aged adults. In the future, more substantial research needs to be conducted on the subjective health of child-rearing-aged adults, especially parents with children ⩾ 12 years, including the physical aspects of health.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221074483 – Supplemental material for Factors affecting subjective health of child-rearing-aged Japanese adults, considering the effect of healthy life expectancy: A cross-sectional study
Supplemental material, sj-docx-1-smo-10.1177_20503121221074483 for Factors affecting subjective health of child-rearing-aged Japanese adults, considering the effect of healthy life expectancy: A cross-sectional study by Kazuya Taira in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221074483 – Supplemental material for Factors affecting subjective health of child-rearing-aged Japanese adults, considering the effect of healthy life expectancy: A cross-sectional study
Supplemental material, sj-docx-2-smo-10.1177_20503121221074483 for Factors affecting subjective health of child-rearing-aged Japanese adults, considering the effect of healthy life expectancy: A cross-sectional study by Kazuya Taira in SAGE Open Medicine
Footnotes
Acknowledgements
The Japanese General Social Survey 2009 Life Course Study (JGSS-2009LCS) was designed and carried out by the JGSS Research Center at Osaka University of Commerce (Joint Usage/Research Center for Japanese General Social Surveys accredited by the Ministry of Education, Culture, Sports, Science and Technology). It is financially assisted by the Japanese Ministry of Education, Culture, Sports, Science and Technology, and the Osaka University of Commerce. The author would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work and APC were funded by the Japan Society for the Promotion of Science KAKENHI (grant no. 18K17637).
Ethical approval
This study is the secondary use of open data, which is typically exempt from IRB approval. The secondary use of data in this study was conducted by researchers in the social sciences and humanities field, and ethical review in the field is still under discussion. In Japan, only medical research is subject to ethical review based on the “Ethical Guidelines for Medical and Health Research Involving Human Subjects.” For these reasons, this study has not been discussed or approved by the ethics review committee due to the differences in the research field.
Informed consent
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.