
Abstract
Introduction:
Different interventions have been done to reduce the burden of soil-transmitted helminths (STH). The available evidences in Ethiopia in either school or community-based school-aged children (SAC) have limitation in wetland areas. This study assessed the prevalence and associated factors of STH infection among SAC in wetland and non-wetland areas of Blue Nile Basins, Amhara Region, Northwest Ethiopia.
Method:
A community-based comparative study was conducted from October to November, 2019. Multistage stratified random sampling technique used to select 716 SAC. Data were collected using structured questionnaire and observational checklist. Stool samples were collected from children using tight-fitting plastic cups following the standard procedures. Data were coded and entered into Epi data version 4.6 and exported to SPSS version 20 software. Bivariate and multivariable logistic regression analysis was employed to identify factors associated with STH.
Results:
The overall prevalence of STH was 30.30% (95% CI: 26.90, 33.90) and did not show significant variation between wetland (33.60% (95% CI: 28.80, 39.60%)) and non-wetland (27.0% (95% CI: (21.90, 31.60)) areas. Presence of human feces near the house and certain habits such as nail trimming and playing with mud/soil was not different between wetland and non-wetlands. Nonetheless, the presence of human feces near the house of respondents was found to be significantly associated with STH infection (p value < 0.001). Moreover, other factors significantly associated with STH infection were lack of nail trimming (p value < 0.001) and playing with mud/soil (p value < 0.01).
Conclusions:
The prevalence of STH was high and did not show significant variation between the two areas. Emphasis needs to be given for hygiene and lifestyle-related factors.
Introduction
Soil transmitted helminths (STHs) such as Ascaris lumbricoides, Trichuris trichiura and hookworms (Nectar americanus and Ancylostoma duodenal) are the common species that infect people in low-income countries.1–3 These helminths usually occur in rural areas where poor hygiene and sanitation practices are common since these favor their transmission.4,5 Women of the reproductive age, pre-school age children (PSAC) and school-age children (SAC) are categorized as at-risk groups for STH by World Health Organization (WHO). 6 The morbidity and intensity of STH infection is the highest among SAC (5–14 years).7–9
The global (2020), latest estimates indicate that more than 2 billion people are infected with STH. The highest prevalence also occurs in areas where sanitation is inadequate and safe water supplies are not available. 6 Similarly, 568 million SAC are living in intensively transmitted areas, of which, 280 million (30.0% of the global) children live in 42 African countries. Greater than 40% are from three populous countries (Democratic Republic of the Congo, Ethiopia and Nigeria).6,10 In Ethiopia (2016), 25.30 million SAC are living in STH endemic areas. 11 The prevalence of STH varies within Ethiopia and is higher in Amhara region where more than 36.40% SAC were found to be infected with STH. 12 In general, different studies conducted in different settings of the country did show that the prevalence of STH infection in SAC ranged from 13.0%–69.20%.13–18
A previous study has shown that the burden of STH in the wetland area is high due to suitable conditions for the survival of helminths. 19 Warm and humid climates or aquatic environments are also the most preferable for the survival or proliferation of helminths.19,20 Unhygienic practices of children on playgrounds, poor sanitation, walking barefoot, lack of hand washing practice, eating of improperly washed raw vegetables, inappropriate waste disposal systems, unimproved water sources and densely populated areas were previously found to be predictors of STH infection.2,4,21,22 Lack of basic sanitation promotes the contamination of common areas, including children’s playgrounds since the feces contain the infective eggs which can then contaminate the water sources and the food they are washed with.23–25
The WHO set a roadmap for prevention, control, elimination and eradication of neglected tropical diseases (NTDs), including STH by the year 2020. 26 While substantial progress has been made since 2012, not all of the 2020 targets were met and the new road map that demonstrates critical gaps and the actions required to reach the 2030 targets has been recently launched since 2021. Experience from the past decade shows that further multisectoral action is required for all 20 diseases and disease groups to achieve the Sustainable Development Goals (SDGs) and accelerate control and elimination. In addition to multisectoral actions, the road map recommends the prevention of STH through preventive chemotherapy or deworming, as well as improved sanitation and hygiene.26–28 Similarly, Ethiopia launched the first and the second national NTD strategic plan for the control, elimination and eradication of NTDs including STH. But, only 13 million (51.40%) SAC were dewormed by the national deworming program. 11 Even though there is progress in the improvement of improved water supply, sanitation and hygiene in the country since 2003, ensuring these basic needs still remains a challenge, particularly in Amhara Region. 29 Moreover, a study in Kenya showed that provision of sustainable water supply, sanitation, and hygiene services and regular preventive chemotherapy in wetland areas still remains a challenging. 20 The effect of such interventions on health outcomes should be done to generate evidence to devise or sustain and strengthen prevention and control strategies of STH. However, there is still not enough studies that assessed the factors associated to their presence in wetlands areas of the Blue Nile basin of Amhara region. Therefore, the current study aims to assess and compare the prevalence of STH and its associated factors among SAC in wetland and non-wetland areas of the Blue Nile basin of Amhara region, Northwest Ethiopia.
Methods and materials
Study area
The study was conducted in wetland and non-wetland areas of Fogera district which is located in South Gondar Zone, Amhara National Regional State. The district is found in the Blue Nile basin areas of the country in the eastern part of Lake Tana. It is located at 625 km away from Addis Ababa, to northwest Ethiopia. The district has 35 kebeles (the smallest administrative unit of the government), of which 6 kebeles are in the wetland areas (Figure 1). The projected population of the district for 2020 based on the 2007 national population census is 270,000. In the district, there are 62,795 households and 23,247 school-age children, of which 4527 reside in wetlands.

Map of the study area.
Study design, population and period
A community-based comparative cross-sectional study design was conducted from October to November, 2019 to assess the prevalence of STH and its associated factors in school-aged children. All school-age children and their mothers or care givers in the district were the source population and all SAC in randomly selected kebeles of wetland and non-wetland areas were the study population. School-age children (5–14 years) who were lived in the last 6 months in the district with their family were included in the study. Children who had taken deworming drugs within 3 months prior to the data collection period were excluded from the study.
Study variables
The outcome variable was having at least one STH (Ascaris lumbricoides, and/or Trichuris trichiura and/or the hookworm). Independent variables were age and sex of the child, residence, educational status of father and mother, wealth index, having a latrine facility, latrine utilization, drinking water source, solid waste disposal methods, habit of shoe wearing, washing hands before eating, washing hands after any waste contact, hand washing after toilet visit, using soap for washing hand, habit of playing with mud/soil, nail trimming, raw vegetable eating habit, and knowledge on prevention methods for STH.
Operational definitions
Soil transmitted helminths: Four main species of nematodes are collectively referred to as soil-transmitted helminths: the roundworm, Ascaris lumbricoides; the whipworm, Trichuris trichiura; and the hookworms, Necator americanus and Ancylostoma duodenale. 9
Soil transmitted helminth infection: the presence of Ascaris lumbricoides and/or Trichuris trichiura and/or the hookworms at school-age children stool.2,6
Wetland: areas that are swamps or marshes which are temporary or permanently settling of water during any season of the year. Mostly the land is covered by water and suitable for rice and some aquatic vegetable production due to muddy soil. 30
Non-wetland: areas that are not swamps or marshes and also which are not permanently or temporarily with water during any season of the year.
School-age children (SAC): children aged between 5 and 14 years who may or may not be enrolled in school. 6
Knowledge of respondent was assessed by developing 19 questions about STHs transmission, prevention and control measures. If a respondent scored between 80%–100% from knowledge measuring STHs questions, she or he was classified as knowledgeable, 50%–79% was classified as moderately knowledgeable and <50% was classified as less-knowledgeable. 31
Sample size determination
The sample size was determined using a double population proportion formula considering the following assumptions: 95% confidence level, 80% power of the study, two comparison groups population ratio 1:1, prevalence of STHs in previous study in the non-wetland area was 30.9% (P1 = 0.309) 32 assumed 16% difference from non-wetland area, 33 46.9% (P2 = 0.469), design effect 2% and 10% non-response rate. The calculated sample size was 716.
Sampling procedures
Multistage stratified sampling followed by simple random sampling technique was used to select kebeles and households. Stratification of the kebeles was done based on the geographical location of the kebeles as being wetland and non-wetland areas. Of all kebeles in the district, 34% (6 kebeles in wetland and 6 kebeles in non-wetlands) were selected randomly. Proportion to population size allocation was made to determine the required sample size of each selected kebele. Finally, 716 households were selected using systematic random sampling technique (every other household). When there were two or more school-age children in a single household, one child was selected using lottery method.
Data collection tools and procedures
Data were collected using a structured and pretested questionnaire, observational checklist and stool examination procedures. The questionnaire was developed after reviewing available literature.21,34–37 It had five parts which included sociodemographic variables, environmental-related variables, children hygiene practice behaviors, intervention or prevention and knowledge-related variables. First, the questionnaire was developed in English then translated in to Amharic (local language) and then back to English to check for consistency. The questionnaire was pretested using 5% of the total sample in another kebele which was not included in the study and the necessary amendments were done after the pretest.
Household data were collected by two trained public health officers who have previous experiences on data collection works. Stool samples from each child were collected by two laboratory technicians using tight-fitting plastic cups that used to collect and transported the samples to the examination laboratory following the standardized procedures.
Parasitological examination
The collected stool samples were emulsified and preserved in 8% formalin and transported to the health center (Wereta Health Center and Quar Health Center) laboratories for microscopic examination. At the laboratory slides were prepared by dropping normal saline for stool examination. Then, some portion of preserved stool samples were added on the slide and mixed by applicator stick and covered with cover slide. Finally, direct microscopic examination was performed using (10× with 0.25 magnification power) Olympus microscope. 38 The result was recorded carefully on well prepared format for this purpose. Two laboratory technicians analyzed the stool samples at the health centers independently.
Data management and analysis
Four data collectors and two supervisors recruited and trained on how to conduct the interviews, on the questionnaire contents, on the ethical aspect for approaching the care givers which was in a polite and respectful manner and how to collect stool samples from a child. Data collectors were selected based on their previous experience on data collection. In order to assure its validity, double stool samples were taken from 18 SAC and analyzed by direct microscopy during pretest. Both of them detected the parasites (STH) equally on positive children in the same manner. After the data collection, the information was reviewed and incomplete questionnaires were returned to the data collectors to revisited the respondent and complete it. Data were coded and entered in Epi data version 4.6 and exported to SPSS version 20 for analysis. Descriptive statistics were used to describe data. Principal Component Analysis (PCA) was done to construct the household wealth index. The sampling adequacy for PCA was assessed using Kaiser–Meyer–Olkin (KMO) statistics. The KMO measures the adequacy of sampling thoroughly and the sampling adequacy for each variable that indicates the proportion of variance the variables might be caused. Sampling adequacy set at communality value >0.5 with p value >0.05 and complex structure factor (Eugene value) greater than 1 was considered. 39 Bivariate and multivariable logistic regression analyses were done to identify variables significantly associated with STH. Results reported using adjusted odds ratio (AOR) with 95% confidence interval (95% CI). Model fitness was checked using Hosmer–Lemeshow test with p value <0.05. During the bivariate analysis, variables with p value <0.25 were considered as candidate for multivariable logistic regression analysis.40,41 Statistically significant association of independent variable with dependent variable was declared at p value <0.05.
Results
Sociodemographic characteristics of the respondents
Seven hundred respondents (with a response rate of 97.80%) gave complete responses. Nearly, 50-50% of the respondents were from wetlands and non-wetland areas: 49.70% and 50.30%, respectively. More than two-third of school-age children (79.0%) in wetlands and 65.30% in non-wetland areas were enrolled or attending school. The mean (±SD) age of children was 8.01(±2.33) and 7.93 (±2.65) years old in wetland and non-wetland areas, respectively. The majority of mothers or care givers in both settings did not have any formal education (93.0% for wetland and 94.60% for non-wetland).
The availability of latrine facilities for the households in the study areas were found to be 12.90% for wet lands and 30.0% for non-wet land, respectively. However, latrine utilization rates of the household members of the respondents were 33.0% for wetland and 40.0% non-wetland area.
Neither of the household located in wetland nor non-wetland areas use any household water treatment methods. A substantial number of children in both wetland and non-wetland areas did not wash their hands after defecation, 89.10% and 90.70%, respectively. Only few children reported using soap during their hand washing in all cases: 12.0% in wetland and 16.0% non-wetland (Table 1).
Socioeconomic and demographic characteristics of the respondents from wetland and non-wetland areas of Fogera district, north-west Ethiopia, 2019 (n = 700).

NCH: number of children; HHs: households.
Washing hands with water and ash, other plants like endode.
Wearing shoe at holiday, market day.
Prevalence of soil-transmitted helminths
Seven hundred stool specimens were obtained from the children and examined for its parasitic status. From the specimens examined, 212 were positive for at least for one parasite. The overall prevalence of STH in the district was 30.30% (95.0% CI: 26.90%, 33.90%). The prevalence was found to be 33.60% (95% CI: 28.80%, 39.60%) in the wetland area and 27.0% (95% CI: 21.90%, 31.60%) in the non-wetland area. According to this finding, there is no statistically significance difference in the presence of STH infection between wetland and non-wetland areas of the district. The most prevalent parasite was Ascaris lumbricoides (20.40%). In this study, there was no Trichuris trichiura infection among school-age children. From the total infected students, 21 were affected by double infection (Ascariasis and Hookworms; Figure 2).

Prevalence of soil-transmitted helminthiasis among school-age children from wetland and non-wetland areas in Fogera district, Northwest Ethiopia, 2019.
Factors associated with soil transmitted helminthiasis
Pooled and separate analyses were done to see the association of factors with STHs. In the first place, the association of each independent variable with STHs was assessed by using bivariate logistic regression and those variables with a p value <0.25 in this analysis identified for multivariable analysis.
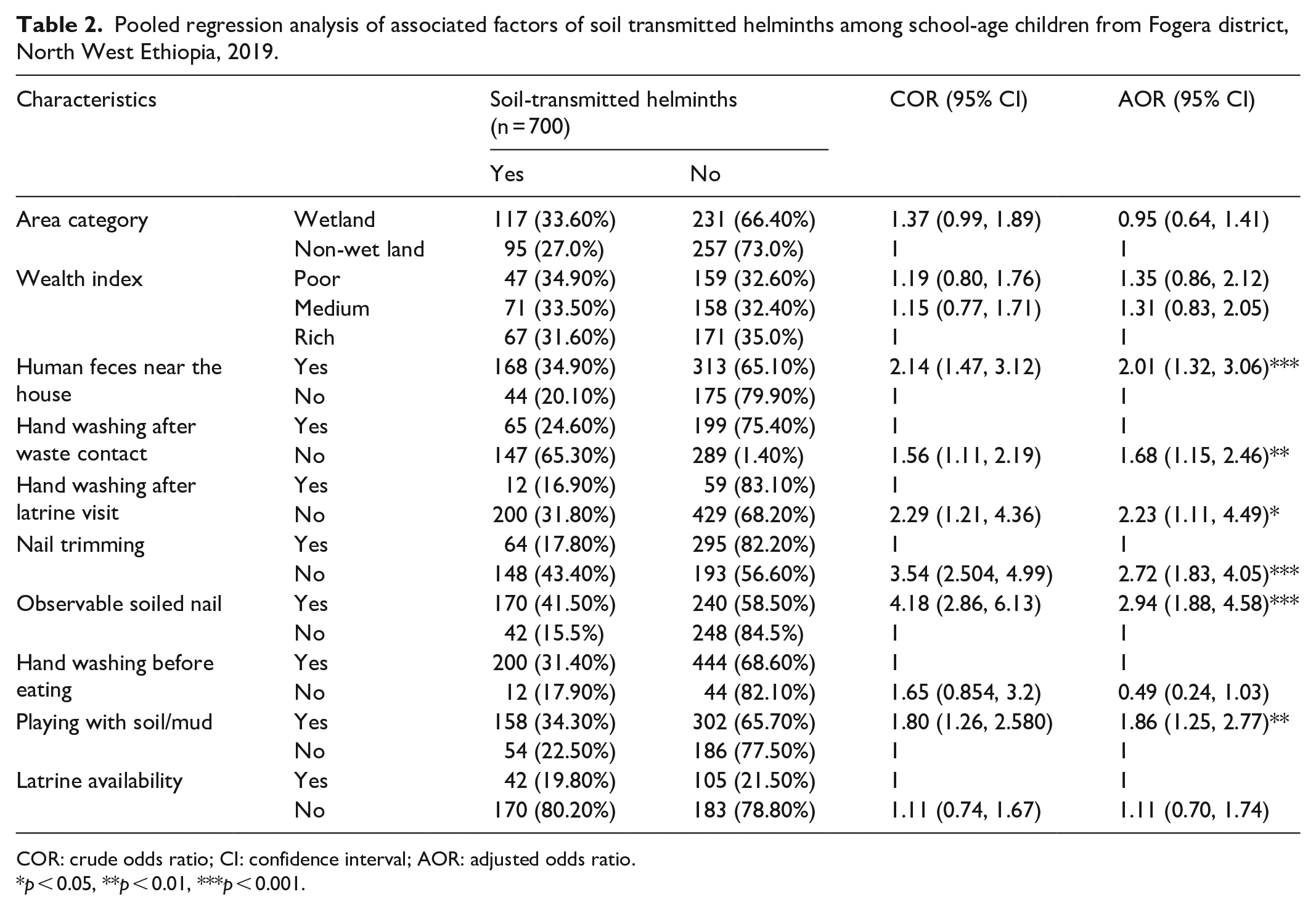
During the multivariable logistic regression analysis variables like presence of human feces near the house, washing hands after any waste contact, washing hands after defecation or toilet visit, nail trimming, soiled or dirty nails and children played with soil or/and mud are found to be significantly associated with the outcome variable in pooled analysis. In the separate analysis, presence of human feces near the house, nail trimming and children played with soil or/and mud were the only variables found to be significantly associated in the wetland areas. In the non-wetland areas similar to the pooled analysis, except washing hands after defecation or toilet visit all the variables that were significantly associated found to be significantly associated with STH.
During the pooled estimate regression analysis, the odds of children in the households where human feces are present near to the house was 2.01 times higher to be infected with STH than their counterparts (AOR = 2.01, 95% CI: 1.32, 3.06; Table 2). In the same manner, presence of human feces near the house was found to be significantly associated with STH infection in both wetland and non-wetland areas during separate analyses (AOR = 2.58, 95% CI: 1.38, 4.83, AOR = 1.90, 95% CI: 1.02, 3.53), respectively (Tables 3 and 4). The odds of children who did not wash their hands after latrine visit or defecation was 2.23 times higher than children who washed their hands to be infected with STHs (AOR = 2.23, 95% CI: 1.11, 4.49; Table 2). This variable lost its significant association during separate analyses in both wetland and non-wetland areas (Table 3 and 4).
Pooled regression analysis of associated factors of soil transmitted helminths among school-age children from Fogera district, North West Ethiopia, 2019.
COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.05, **p < 0.01, ***p < 0.001.
Logistic regression analysis of associated factors of soil transmitted helminths among school-age children for wetland areas of Fogera district, North West Ethiopia, 2019.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.05, **p < 0.01, ***p < 0.001.
Logistic regression analysis of associated factors of soil-transmitted helminths among school-age children for non-wetland areas of Fogera district, North West Ethiopia, 2019.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio.
p < 0.05, **p < 0.01, ***p < 0.001.
Discussion
The government of Ethiopia in collaboration with different partners has implemented different types of interventions to alleviate infection with STH. Periodic evaluation of the status of health problems when there is an intervention program to control that problem is important public health actions. It is with this assumption that the current study is conducted to determine the status of STH infection. According to the findings of the current study, the overall prevalence of STH infection among school-age children is still high. The study also tried to compare the prevalence of STH infection among school-age children between the two areas (wetland and non-wetland) and it was found that there is no statistically significant difference although there was lower prevalence in the non-wetland areas.
The possible explanation for the absence of significant difference might be due similar household sanitation conditions in both areas. This is to mean that the available sanitation services like latrine utilization in both cases was found to be low or below 40%. Even the available latrines are traditional pit latrines which may have limitations to prevent STH infection. The limitations of these pit latrines to prevent STH infection may be associated with its viability for fly breading. Moreover, greater than two-third of households in both settings practiced open defecation which in turn can be considered as a risk factor to drinking water source and environmental contamination. In both wetland and non-wetland areas, children who played on soil or mud playgrounds were more likely to be infected than those who did not. Besides, study findings from Tanzania revealed that traditional pit latrines had limitation to prevent STH infection. 42 The other possible explanation for the absence of significance variation between the two areas might be due to the fact that the government implemented deworming as an intervention that may have significant effect on both study areas.
The finding of the study was also compared with other studies done in different parts of the country and abroad. The finding found to be comparable with the study conducted in the same region (Bahir Dar zuria district) Arbaminch town and Chencha district.4,15,43 However, the finding was lower than studies done in other areas of the Amhara region (Bahir Dar city administration, Zegie Peninsula, Durbete town) and other parts of the country like Jimma and Yirgacheffee.16–18,21,37 The difference could be the parasitological examination technique the researchers used. For example, the authors in Yirgacheffee used Kato-Katz technique which is more sensitive and increase the prevalence. The other possible reason for this difference might be time variation. Two researches (Durbete town and Jimma) were conducted before 3 years. This is to mean that currently, the government of Ethiopia now is implementing mass deworming activities as an intervention which may have a significant impact on the prevalence of STH.
In the same way, the prevalence of STH infection in this study is lower than the studies conducted in Nigeria, Kenya and Rwanda.19,44,45 This variation can be explained in many ways like environmental health facility provision, health service access, life style of students in the study area and the likes. The finding is also higher than the study findings in other parts of Amhara region, Gurage zone and Ambo town specifically and other parts of Ethiopia13,14,46,47 with in the country and Victoria basin of Tanzania 48 in African country.
The health extension program which has been implemented for the last decade in Ethiopia is supposed to bring about changes on different risk factors of STH infection. In this study analyses, different factors that have linkage with this program were considered and checked for their association with STH in both pooled and separate analyses approaches. The presence of human feces near the houses of the study participants, nail trimming and children who played with mud or soil playground were variables found to be significantly associated with STH in both cases for both areas consistently. Hand washing after any waste contact and presence of observable dirt on the nail of students were variables found to be significantly associated with STHs in pooled analysis and in the non-wetland areas during separate analysis. Similar with the current study, another finding supported that better sanitation practice has significant reduction effect on STH infection, especially for Ascaris lumbricoides and hookworm. 13
Habits of playing with soil or mud is one of the predictors of STH infections. The finding of the current study is consistent with other studies done in Ethiopia and Indonesia15,31,49 in that the probability to be infected with STH is high for SAC who played with soil and mud. This might be due to the fact that children who played on the contaminated soil may get the chance to ingest eggs of the parasite or the infective stages (eggs and larva) of helminths penetrated children who play in the contaminated soil. The probability of being infected might be high where open defecation practice is prevalent.15,50
This study also revealed that children who had dirty nails were associated with high prevalence of STH. The finding is also consistent with previous studies done in Bahir Dar city. 51 Similarly, children who had untrimmed finger nails were more likely to be infected by soil transmitted helminths infection than children those who had a habit of trimming their nail. This result agrees with previous studies from Ethiopia and Nigeria.46,51,52 The possible explanation for this greater risk of infection among children who did not trim their finger nails than their counterparts might be due to the fact that children with untrimmed fingernails are at higher risk of collecting dirty under their nails. This dirt under the finger nails may harbor infective agents of STH and this in turn helps to easily acquire the ova of helminths through fecal-oral route. Not washing hands after latrine visiting and after any waste contact can be considered as an indicator for hygienic behavior of children. These findings are supported by other studies carried out in Ethiopia, Africa and India.35,37,53
Conclusion
The prevalence of STH among school-age children was high and did not show significance difference between wetland and non-wetland areas. The presence of human feces near the house, not washing hands after defecation, children playing with soil/mud, not washing hands after any waste contact, untrimmed fingernails and the presence of dirt under fingernails were identified as significant predictors of STHs infections among school-age children in the study area. Therefore, improving personal hygiene-related activities such as thorough hand washing of children, removing dirt from nails by trimming the fingernails, regular practice of hand washing after defecation and after contact waste, avoiding playing with soil or muddy play grounds need to be the intervention areas. Important emphasis on the use of sanitation services and especially on latrine construction and use also needed to eliminate the practice of open defecation.
Limitation of the study
This study was trying to investigate one of the vulnerable groups (school-age children). But this study had its own limitation including social desirability bias and potential recall bias. Another limitation of this study is that the hygiene practices of the mother at critical times were not explored. It is also the limitation of the study in that the microscopic examination used only direct observation of the fecal samples and therefore the sensitivity is quite low, adding a sedimentation technique and Kato-Katz for quantification would improve the probability of finding an STH and the prevalence would probably be higher than what is reported. In future studies, PSAC and those on the deworming programs need to be included in the prevalence study.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211063354 – Supplemental material for Prevalence and associated factors of soil transmitted helminthiasis among school-age children in wetland and non-wetland areas of Blue Nile Basins, northwest Ethiopia: A community-based comparative study
Supplemental material, sj-docx-1-smo-10.1177_20503121211063354 for Prevalence and associated factors of soil transmitted helminthiasis among school-age children in wetland and non-wetland areas of Blue Nile Basins, northwest Ethiopia: A community-based comparative study by Almaw Genet, Achenef Motbainor, Tsion Samuel and Muluken Azage in SAGE Open Medicine
Footnotes
Author contributions
A.G. conceived and designed the study, collected data and analyzed. A.M. designed the study, analyzed, interpreted and wrote. T.S. designed, interpreted and wrote. M.A. conceived the study, reviewed and wrote.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval and consent to participate
Ethical approval was obtained from the Institutional Review Board (IRB) of Bahir Dar University, College of Medicine and Health Sciences. Formal support letter was also obtained from Amhara Public Health Institute and given to North Gonder Zonal Health Office and Fogera Woreda health office. Informed consent was waived by the Institutional Review Board with protocol No. 02084/18.09 and all participants were asked to give a verbal informed consent. Before starting the interview, the data collector explained the purpose of the study for the participants. The confidentiality of the study participants related to data was maintained by avoiding possible identifiers such as name of the study participants. Only identification number was used as a reference. Helminths infected children were transferred to the nearest health center for treatment
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There is no fund received from any organization to conduct this study. However, expense for data collection was covered by principal investigator.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.