
Abstract
Introduction:
Drug use evaluation is a method of obtaining information to identify problems related to drug use and if properly developed, a means of correcting the problems. Ceftriaxone is among the most commonly utilized cephalosporins. Owing to a broad spectrum of activity and being used empirically, ceftriaxone has been used inappropriately posing a risk for development of antimicrobial resistance. This study is, therefore, designed to evaluate the appropriateness of ceftriaxone utilization in government hospitals in Harar town.
Methods:
A retrospective cross-sectional study was conducted in four government hospitals of Harar town by reviewing the medical records of 271 patients who received ceftriaxone from 1 January to 31 December 2016. Systematic random sampling was utilized to capture the medical records. Data were entered and analyzed using SPSS version 22.
Results:
From the 271 medical records reviewed majority of patients were from surgical ward (n = 85, 31.4%) followed by gynecology and obstetrics ward (n = 67, 24.7%). Demographically, the majority of the patients were female (n = 142, 52.4%). Patients in the age group of 20–29 years were dominant (n = 98, 36.2%). A total of 71 drugs were co-administered with ceftriaxone, the most common being metronidazole followed by tramadol. Among the co-administered drugs, unfractionated heparin (n = 6), warfarin (n = 5), and enoxaparin (n = 1) were found to have a moderate drug interaction with ceftriaxone. Ceftriaxone was commonly used for post-operative prophylaxis (n = 80, 27.5%) followed by for the management of pneumonia (n = 62, 21.3%). The result of ceftriaxone use evaluation showed that majority (n = 190, 70.1%) were found to be inappropriate. The inappropriate utilization was primarily due to wrong indication (indications for which ceftriaxone was not the primary option) (n = 114, 60.0%) followed by wrong duration (n = 54, 28.4%).
Conclusion:
Ceftriaxone was used inappropriately in more than two-thirds of the patients, with wrong indication and wrong duration contributing the majority. Inappropriate use of antibiotics may potentially lead to the emergence and spread of drug-resistant microorganisms and also ultimately exposes the patient to treatment failure, prolonged hospital stay, and higher cost of therapy.
Introduction
The use of antimicrobial agents is showing a dramatic change globally, with a recorded increase by 65% between 2000 and 2015, from 21.1 to 34.8 billion defined daily doses. 1 Increased use of antibiotics is linked with the development of resistant bacteria. 2 Antibiotic resistance, in turn, would increase the risk of morbidity and mortality as well as the cost of therapy.3,4 Inappropriate antibiotic use is a huge problem in Ethiopia, as many microorganisms were resistant to commonly used antibiotics and multidrug-resistant bacterial strains such as Escherichia coli and Staphylococcus aureus are becoming highly prevalent. 5 To reduce the burden associated with antimicrobial resistance, evaluation of antimicrobial use should be conducted to take corrective measures. 6 Drug use evaluation is a system of continuous, systematic, criteria-based evaluation that ensures the appropriate use of drugs. It is a method of obtaining information to identify problems related to drug use. If it is properly developed, it will also provide a means of correcting the problem, and thereby contributes to rational drug therapy. 7
Broad-spectrum antibiotics, such as third-generation cephalosporins, are categorized as “Watch” antibiotics that should be used with caution because of their high potential to cause antimicrobial resistance and/or their side effects.8,9 Ceftriaxone is among the most commonly utilized cephalosporin owing to its high potency, broad spectrum of activity, and low-risk of toxicity. 10 Ceftriaxone, like the other cephalosporin antibiotics exert its action by inhibiting the final stages of peptidoglycan assembly, which is a major component of the cell wall of all bacteria giving the layer its strength and rigidity. 11 As an empiric therapy, ceftriaxone can be used for a wide range of infections due to its broad spectrum of activity against several pathogenic bacteria. For specific therapy, it can be used against meningitis, Lyme disease, Gram-negative sepsis, streptococcal endocarditis, melioidosis, penicillinase-producing Neisseria gonorrhoeae, chancroid, and osteomyelitis.12,13 Resistance to ceftriaxone arises when the penicillin-binding proteins (PBPs) are modified, or when they are protected by beta-lactamases. Target-mediated cephalosporin resistance can involve either reduced affinity of an existing PBP component or the acquisition of a supplementary beta-lactam insensitive PBP. 11 Because of a broad spectrum of activity and empirical use, ceftriaxone can be subjected to inappropriate utilization, and hence posing a risk for development of antimicrobial resistance.14,15 Thus, this study is designed to evaluate the appropriateness of ceftriaxone utilization and to assess major areas of inappropriate use in government hospitals in Harar town.
Materials and methods
Study area, design, and period
The study was conducted in Harar town located 526 km away from the capital of Ethiopia, to the East with a total population of 203,438. In Harar town, there are four governmental hospitals, two private hospitals, and eight health centers. 16 The study was conducted in four governmental hospitals, namely: Hiwot Fana Specialized University Hospital (HFSUH), Jugel Hospital (JH), Federal Harar Police Hospital (FHPH), and South-East command III Hospital (SECIIIH). HFSUH is a tertiary care teaching hospital, JH is a regional hospital of Harari regional state while FHPH and SECIIIH are government hospitals that provide medical services for the military base in the area and their families. Medical records of patients who received ceftriaxone from 1 January to 31 December 2016 were reviewed during the period of 1 May to 30 June 2018.
Study design
A hospital-based retrospective cross-sectional study was conducted in government hospitals of Harar town.
Sample size and sampling techniques
The sample size was determined using single population proportion formula,
Data collection procedure
The data were collected by reviewing medical records of patients to whom ceftriaxone was prescribed. A data abstraction format was employed to extract data regarding indication for ceftriaxone use, dose, frequency of administration, and duration of therapy, co-morbid condition/s, duration of hospital stay, and co-administered drugs from patient’s medical record (Supplementary file). To ensure the collection of meaningful data, pre-test was conducted on 5% of the total sample size (n = 14) before commencing the actual data collection at Haramaya Hospital. Then, amendments were made into the final version of the data abstraction format. In addition, training of data collectors and supervision of data collection were undertaken. The data were collected with one pharmacist at each hospital.
Data processing and analysis
The data were analyzed using Statistical Package for Social Sciences (SPSS) version 22.0. Univariate analysis was used to describe the frequency and percentage distribution of each variable. The appropriateness of ceftriaxone utilization was evaluated using indication, dose, frequency, and duration of drug administration as a focus area of the criteria. The protocol for use evaluation was developed by reviewing Standard Treatment Guideline (STG) of Ethiopia and standard textbooks.18,19 The utilization of ceftriaxone was evaluated against the standards in the protocol by the research team. Accordingly, the utilization was declared appropriate when the use was in line with guideline recommendation with respect to the four parameters (indication for use, dose, frequency of administration, and duration of therapy), otherwise it was deemed inappropriate. The utilization of ceftriaxone was declared indeterminate when there was missed/unrecorded information in one of the four parameters (indication, dose, frequency of administration, and duration of therapy) in the patient’s medical record.
Results
From a total of 271 medical records of patients to whom ceftriaxone use was evaluated, majority of them (n = 85, 31.4%) were from the surgical ward followed by gynecology and obstetrics ward (n = 67, 24.7%). The majority of the medical records were from HFSUH (n = 167, 61.6%) followed by JH (n = 89, 32.8%) (Figure 1).

Distribution of drug use evaluation of ceftriaxone in government hospitals of Harar town, 2016.
The demographic characteristic of the patients for whom the use of ceftriaxone was evaluated showed that the majority were female (n = 142, 52.4%). Patients in the age group of 20–29 years were dominant (n = 98, 36.2%) followed by 30–39 years (n = 46, 17.0%) with a mean of 30.49 years (standard deviation (SD) = 17.9) (Figure 2). From anthropometric characteristics, height and waist circumference were not recorded at all in medical records while weight was recorded only in four of the medical records. Pregnancy and lactation status was recorded in only 30 (21.1%) and two medical records of female patients, respectively.
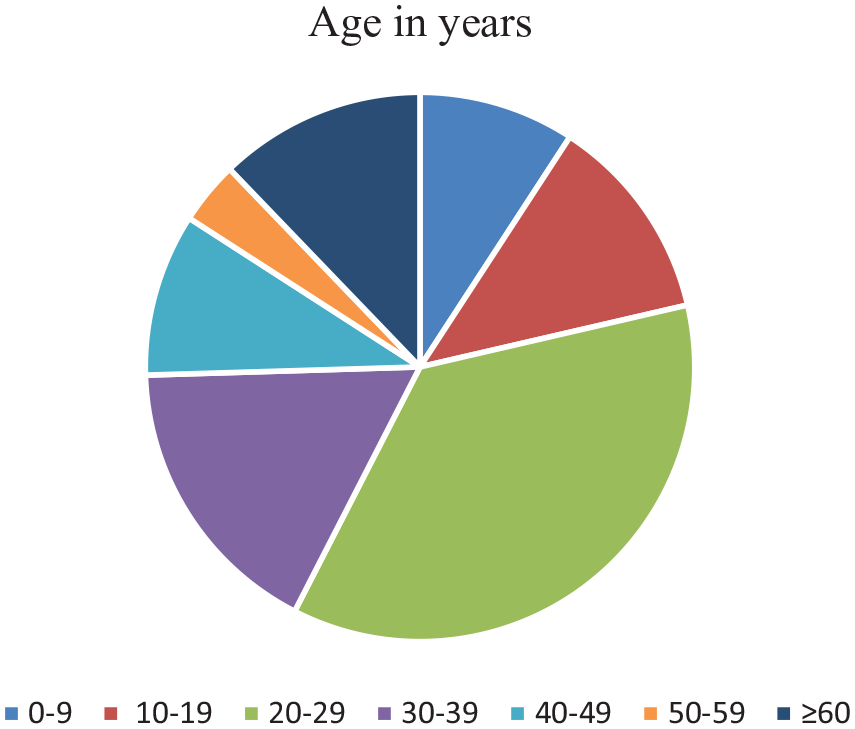
Age distribution of patients treated with ceftriaxone in government hospitals of Harar town, 2016.
The mean duration of treatment with ceftriaxone was 3.43 days (SD = 3.7 days). The duration of hospital stay for the patients who were treated with ceftriaxone showed that the majority of the patients stayed for 6–10 days (n = 91, 33.6%) followed by 1–5 days (n = 62, 22.9%) and 11–15 days (n = 55, 20.3%). The mean hospital stay was 6.57 days (SD = 7.67 days).
A total of 71 drugs with a frequency of 674 were co-administered with ceftriaxone. The most commonly co-administered drug with ceftriaxone was metronidazole (n = 128, 18.9%) followed by tramadol (n = 112, 16.6%) (Table 1). Among the co-administered drugs unfractionated heparin (n = 6), warfarin (n = 5), and enoxaparin (n = 1) were found to have moderate drug interaction with ceftriaxone.
Top 10 co-administered drugs with ceftriaxone in government hospitals of Harar town, 2016 (n = 674).

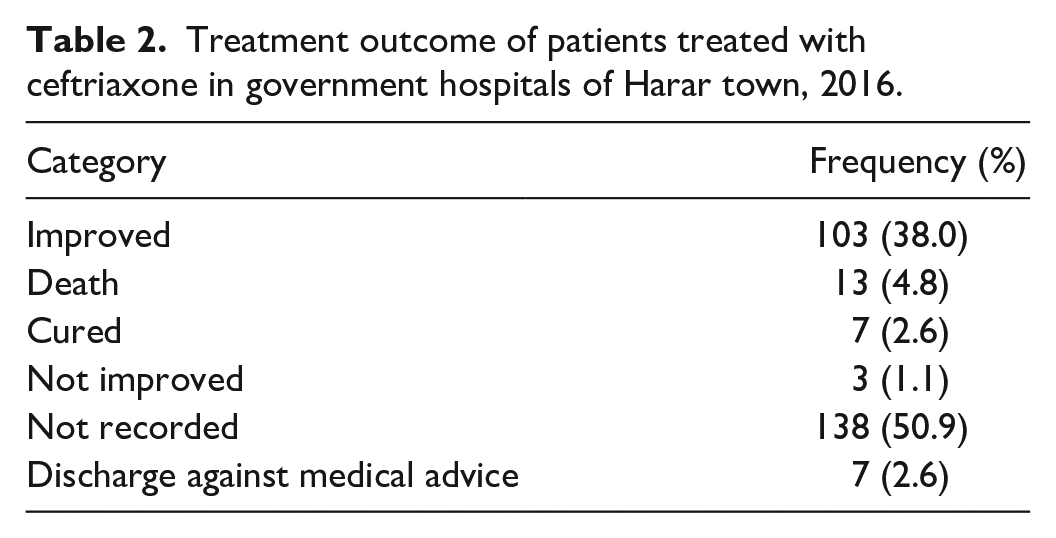
As shown in Table 2, 103 patients (38.0%) who were on ceftriaxone therapy had been improved while death was recorded for 13 (4.8%) patients (Table 2).
Treatment outcome of patients treated with ceftriaxone in government hospitals of Harar town, 2016.
The top three indications for ceftriaxone use were post-operative prophylaxis (n = 80, 27.5%) followed by pneumonia (n = 62, 21.3%) and pre-operative prophylaxis (n = 25, 8.6%) (Table 3).
Common diagnosis for the use of ceftriaxone in government hospitals of Harar town, 2016.

From a total of 271 medical records evaluated, the use of ceftriaxone was found to be inappropriate for 190 (70.1%) patients while 18 records (6.6%) were treated as indeterminate. The distribution of the use evaluation of ceftriaxone among the four government hospitals has shown the inappropriate use to be high in HFSUH (n = 121, 72.5%) followed by JH (n = 63, 70.8%) (Table 4).
Distribution of use evaluation of ceftriaxone among government hospitals of Harar town, 2016 (n = 271).

HFSUH: Hiwot Fana Specialized University Hospital; JH: Jugel Hospital; FHPH: Federal Harar Police Hospital; SECIIIH: South-East command III Hospital.
From the areas of the inappropriate use of ceftriaxone, incorrect indication was the commonest (n = 114, 60.0%) followed by incorrect duration (n = 54, 28.4%) (Table 5).
Reason for inappropriate use of ceftriaxone in government hospitals of Harar town, 2016 (n = 190).

Combination of either of incorrect indication, incorrect duration, incorrect dose, or incorrect frequency.
Discussion
Judicious and appropriate use of antibiotics is important to contain the development of multidrug-resistant microorganisms, to minimize the overall healthcare costs and to maximize patient outcomes. 20 In this study, the appropriateness of ceftriaxone utilization was evaluated against STGs. In this study, the inappropriate use of ceftriaxone was noted in more than two-thirds (70.1%) of patients. This finding is similar with the result from Felege Hiwot Referral Hospital (70.1%) 21 but lower than Gondar University Referral Hospital (80.2%) 22 and Dil Chora Referral Hospital (80.46%). 17 On the other hand, the overall inappropriate use was higher than studies conducted at Ayder Referral Hospital (64.2%), 23 Dessie Referral Hospital (46.2%), 24 Zewditu Memorial Hospital (51.1%) and Hayat General Hospital (55.4%), 25 Veteran Hospital in the United States (53%), 26 Korean Hospital (34.5%) 10 and Mizan Aman General Hospital (60.8%). 27 The inappropriate use of ceftriaxone in hospitals of Harar town was high and might be considered as a driving factor for the development and spread of resistant bacteria harboring in such settings. 28 This will impose severe financial and service burden in the hospitals and negates the therapeutic outcome.29,30
Considering criteria and standards while prescribing as well as initiating antimicrobial stewardship programs will potentially preserve antimicrobials like ceftriaxone from becoming ineffective. 31 The inappropriate use of ceftriaxone was found to be higher in HFSUH when compared to the other hospitals included in the study. This might be because HFSUH is the only tertiary hospital in the area, which could cause a higher patient load that in turn might contribute to inappropriate use. In addition, the complexity of cases presented to the hospital might have contributed to the high inappropriate use.
Poor adherence to standard treatment guidelines and irrational use of antibiotics is alarmingly increasing in different parts of the world.32–35 Wrong indication (60.0%) (indications for which ceftriaxone was not the primary option) followed by wrong duration (28.4%) was the common areas of inappropriate use of ceftriaxone in our setting. This finding is similar to the results from Korea, 10 Zewditu Memorial Hospital and Hayat General Hospital, 25 Veteran Hospital from the United States, 26 and Felege Hiwot Referral Hospital. 21 This might be partly due to the pharmacokinetic profile of ceftriaxone, which makes it an appealing option for quick use in the management of patient’s conditions.36,37 The majority of ceftriaxone users in this study were from the surgical ward followed by gynecology/obstetrics ward. This might have occurred as a result of frequent use of ceftriaxone for surgical prophylaxis in hospitals of eastern Ethiopia despite the fact that it is not the first-line option. 38
The duration of antibiotic therapy plays a pivotal role to optimize antibiotic use and reduce resistance. An appropriate antibiotic use together with a treatment course as short as possible can positively affect patient care and the health system by reducing the frequency of adverse events and development of resistance and associated healthcare costs. 39 We found that the mean duration of treatment with ceftriaxone was 3.43 days (SD = 3.7 days). This is an important indicator as the duration of antibiotic treatment correlates with the emergence of antimicrobial-resistant organisms and treatment failure.40,41 However, patients treated with ceftriaxone were hospitalized for a mean period of 6.57 days (SD = 7.67 days). This might expose the patients to hospital-acquired infections, which might require an expensive drug for treatment that further increase hospital stay and cost of therapy for the patients. 42
In a situation where two or more drugs are used, drug interaction should be suspected. Increased vigilance by clinicians at the time of changing drugs improves the chance of identifying unwanted drug interactions before they cause significant harm. 43 The most common co-administered drug with ceftriaxone in this study was metronidazole followed by tramadol and then diclofenac. This finding is in concordance with the study conducted in Tikur Anbessa Specialized Hospital 44 and Dil Chora Referral Hospital 17 in which metronidazole, tramadol, and azithromycin were the top three drugs administered with ceftriaxone. However, when compared to this study, moderate drug interaction with heparin and warfarin was found to be high in the study done at Tikur Anbessa Specialized Hospital. 44 However, studies from different parts of the country showed maintenance fluids to be the most common co-administered drug with ceftriaxone.22–25 This might have resulted as these studies were conducted in in-patient settings where the use of maintenance fluids is high. 45
In this study, ceftriaxone was most commonly used as a post-operative prophylaxis followed by for the management of pneumonia. This finding is more or less consistent with findings from Ayder Referral Hospital (pre-operative prophylaxis followed by pneumonia) 23 and Tikur Anbessa specialized hospital (respiratory tract infections followed by prophylactic indications). 44 However, the use of ceftriaxone as a prophylactic agent is higher in this study when compared to studies from Dessie Referral Hospital, 24 Zewditu Memorial Hospital and Hayat General Hospital, 25 Veteran hospital in the United States, 26 Gondar University Referral Hospital, 22 Felege Hiwot Referral Hospital, 21 and Mizan Aman General Hospital. 27 This might be because of the easy access to the drug and lack of other first-line options in surgical prophylaxis. 38
Conclusion
Ceftriaxone was used inappropriately in more than two-third of the patients in government hospitals of Harar town, a ringing bell for preserving the available antibiotics and timely containing the emergence and spread of bacterial resistance. This also ultimately exposes the patient to treatment failure and higher cost of therapy. A wrong indication and wrong duration of treatment were the major contributors to the inappropriate use of the drug. The common indication for the use of the drug was for post operation prophylaxis followed by pneumonia. Having strict antibiotic use policy and guidelines, establishing antimicrobial stewardship programs and adhering to national and international treatment guidelines may mitigate the problem.
Strength and limitation
The drug use evaluation of ceftriaxone was conducted in four government hospitals of Harar town, making it a multicenter study, which helps us show the overall use of ceftriaxone in the Harar town. Even though, it is a comprehensive drug use evaluation, the retrospective nature of the design was a bottleneck in extracting the required data from medical records. In addition, since the data were extracted from patients’ medical record, missing or incomplete data were another limitation of the study.
Recommendation
Based on the result of the study, we recommend the government hospitals of Harar town to adhere to national guidelines (STGs) in prescribing ceftriaxone and monitor the presence of drug–drug interaction. In addition, the hospitals need to strengthen the record keeping on patients’ medical records. Moreover, establishing an antimicrobial stewardship program in the hospitals, strengthening the antimicrobial resistance sub-committee under the drug and therapeutic committee and periodical evaluation of ceftriaxone use should be undertaken in the hospitals.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211051525 – Supplemental material for The appropriateness of ceftriaxone utilization in government hospitals of Eastern Ethiopia: A retrospective evaluation of clinical practice
Supplemental material, sj-docx-1-smo-10.1177_20503121211051525 for The appropriateness of ceftriaxone utilization in government hospitals of Eastern Ethiopia: A retrospective evaluation of clinical practice by Firehiwot Amare, Tigist Gashaw, Mekonnen Sisay, Yohannes Baye and Tewodros Tesfa in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank data collectors and staff of all hospitals, without them, this research would not have been realized.
Author contributions
All authors had substantial contributions to the study design and development of the data collection tools. All authors were also involved in data acquisition, analysis, interpretation, and write up. F.A. drafted the manuscript and prepared the final version for publication. All authors read and approved the final version of the manuscript.
Availability of data and materials
All the data used for the study is contained within the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Health Research Ethical Review Committee (IHRERC) of College of Health and Medical Sciences, Haramaya University with reference no. IHRERC/078/2017.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported from the Haramaya University for conducting this research work.
Informed consent
Informed consent was not sought for this study because data were collected by reviewing medical records of patients, retrospectively. The requirement for written informed consent from the subjects or the legally authorized representative of the subjects (in case of minor subjects) prior to study initiation was waived by IHRERC of College of Health and Medical Sciences, Haramaya University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.