
Abstract
Objective:
Despite the concerted effort to improve skilled delivery service utilization in Ethiopia, a considerable proportion of births still occur at home by traditional birth attendants, notably in a rural setting. Hence, the aim of this study was to investigate whether mother’s perceived service quality and physical accessibility affect skilled delivery service utilization.
Methods:
A community-based cross-sectional study was conducted from 1 July 2019 to 30 August 2019, among mothers who gave birth in the last 12 months before the study, in selected five districts of Kaffa Zone, Ethiopia.
Result:
In this study, 262 (70.1%) of mothers utilized skilled delivery service in their recent childbirth. Mothers regarding the nearby health facility’s physical environment as “Good” (adjusted odds ratio = 2.48, 95% confidence interval = 1.44, 4.25), mothers mentioning time to reach to the nearby health facility “<1 h” (adjusted odds ratio = 1.92, 95% confidence interval = 1.11, 3.34), and mothers regarding prompt transport service from home to the nearby health facility “Available” (adjusted odds ratio = 2.01, 95% confidence interval = 1.11, 3.63) were positively associated with skilled delivery services’ utilization. Furthermore, completing secondary education and above, attending three and more antenatal care visits, and having good knowledge of danger signs during pregnancy showed a significant association.
Conclusion:
Although the study evidenced statistically significant association between perceived physical accessibility and perceived service quality, further study is recommended to investigate the relationship between actual physical accessibility and actual service quality. Targeted health education program intended to improve skilled delivery service utilization should give due emphasis on enhancing antenatal care service uptake, and raising mothers’ awareness on danger signs during pregnancy, with particular focus on those mothers with low schooling.
Introduction
Maternal health is still one of the core agendas of the international community as it was asserted by Sustainable Development Goals (SDGs), that demand significant reduction in maternal mortality ratio (MMR) by 2030, it set different targets depending on countries’ baseline level of MMR. 1 Although significant improvement has been made in the past two decades, about 295,000 mothers died during and following pregnancy and childbirth in 2017. This figure is unacceptably high. The overwhelming majority of this mortality (94%) happened in a low-resource setting, and most could have been avoided. Sub-Saharan Africa and southern Asia contributed to approximately 86% of the estimated global maternal mortality in 2017. 2
There has been a considerable decline in the magnitude of MMR in Ethiopia. According to 2016 EDHS (Ethiopia Demographic and Health Survey), Ethiopia has made remarkable progress in mitigating maternal mortality from 871 deaths in 2000 to 412 deaths per 100,000 live births in 2016. 3 However, the decline rate is still less than 6.4% which is needed to attain the SDGs of 70 maternal deaths per 100,000 live births. 1
Enhancement in the coverage of the proportion of births attended by a skilled attendant and their provision of care may have attributed to the decline in maternal mortality and morbidity. 4 Nevertheless, the estimated coverage of birth attended by skilled attendants revealed inequality between World Health Organization (WHO) regions as 59% of the births in sub-Saharan Africa region, where maternal mortality is the highest, are attended by skilled attendant while other WHO regions over 68%–99% of all births are attended by skilled birth attendants. 5
Facility-based childbirth can decrease maternal mortality and morbidity through skilled birth attendance.5,6 Skilled birth attendance is where a pregnant woman is attended by a qualified healthcare provider in a setting that has required resources during childbirth. 7 Proper medical attention and hygienic condition during childbirth decrease the risk of complication, infection, or deaths of the mother and the newborn. 8
Despite the various efforts made by the Ethiopian government to ensure skilled attendants at birth, a considerable proportion of births are attended by unskilled birth attendants at home or in other informal institutions.9–12 The proportion of home delivery is even much higher in rural settings, where pregnant mothers have to travel a long distance to get the service.13–16 Several individual, social, and cultural determinates have been suggested for poor skilled delivery service utilization by different studies conducted in various parts of the country.10,12,13 However, mothers’ perception of quality and physical accessibility as determinants of skilled delivery service utilization in a rural setting has not been sufficiently addressed. Hence, this study investigated whether mothers’ perception to quality of care and physical accessibility affects skilled delivery service utilization in rural Kaffa zone, Ethiopia.
Methods
Study setting
The study was conducted in Kaffa Zone, Southwest Ethiopia, from 1 July 2019 to 30 August 2019. Kaffa Zone is located in the Southwest direction of Ethiopia in between 60 24’ to 70 70’ North and 350 69’ to 360 78’ East, and it is 460 km away from the capital city, Addis Ababa. Based on the 2007 census of the central statistical agency (CSA) of Ethiopia, the total population of the zone for the year 2017 was estimated to be 1,171,133, of whom 578,151 (49.4%) were males and 592,982 (50.6%) were females. Despite several interventions, still home delivery is prevalent in the area, and this study was driven by the report of the zone. The zone has one general public hospital, one primary hospital, and 43 public health centers; they provide preventive, curative, and rehabilitative care. Administratively, the zone is found under the SNNPR regional state and divided into ten districts and one city administration.17,18 Among the 10 districts, mothers residing in the rural Kebeles of Chena, Decha, Gimbo, Gewata, Menjiwob, and Tello districts were considered in this study.
Study design and population
A community-based cross-sectional study design was employed. The source population were all women of childbearing age (15–49 years) in Kaffa Zone who had experienced at least one birth, whereas the actual study population were randomly selected mothers who had given birth in the past 12 months prior to the survey and who lived at least 1 year in the zone prior to the study. Mothers who were mentally or physically ill and not able to be interviewed were excluded from the study.
Sample size and sampling procedure
The sample size was calculated using a single population proportion formula, taking the following assumptions: marginal error of 5%, confidence level 95%, and expected prevalence of skilled delivery service utilization in the area 38.2% (taken from a similar study conducted in Northwest Ethiopia). 19 After adding a 10% non-response rate, the final sample size became 399. When recruiting study participants, a multi-stage sampling procedure was used. First, at zone level, six districts (Chena, Decha, Gimbo, Gewata, Menjiwob, and Tello) were selected by employing a lottery method. Again, with a similar approach, 15 rural Kebeles were selected from the above five districts, three Kebeles from each district. For the purpose of allocating a proportionate sample to each Kebele, a list of all mothers who gave birth in the past 12 months before the commencement of the study was obtained from respective Kebele administration. Then, the total calculated sample size was proportionally allocated to each Kebele, based on the number of mothers residing in each Kebele. At community/household level, study participants were selected by a systematic random sampling technique, using a list of mothers residing at particular Kebele as a sampling frame.
Data collection tools and procedure
An interviewer-administered structured tool was used to collect data. The tool was developed after reviewing similar studies conducted in a different part of the country.12,19,20 It has five sections: the first section was about mothers’ socio-demographic characteristics, the second section was about mothers’ obstetric characteristics, the third was about mothers’ knowledge of danger signs during pregnancy, the fourth section contains items related with mother’s perception to physical accessibility and quality related with skilled delivery service of the nearby health facility, and the final section enquires about skilled delivery service utilization in their recent childbirth. Data were collected by eight health extension workers having previous experience on survey data collection technique and the overall data collection procedure was supervised by three BSc health professionals. Attempt was made not to assign health extension workers (data collectors) in the catchment area of the health facility they are currently working in. Before data collection, 3 days of training on data collection techniques and the procedure was given both for data collectors and supervisors. The interview was taken place at each participant’s home after assuring their privacy. The tool used to collect data is available as Supplementary Material.
Inclusion and exclusion criteria
Pregnant women within the age group ⩾18 and residing for more than 6 months in the area were included in this study. Whereas, pregnant women who were unable to respond due to illness or other physical impairment were excluded from the study.
Measurements
The primary variable of interest for this study were: skilled delivery service utilization, mothers’ perception to the nearby health facility’s physical environment, mother’s perception to service providers’ technical ability, time to reach to the nearby health facility (on foot), mother’s perception to availability of prompt transport service from home to the nearby health facility, and mother’s perception of delivery service charge. The tool was adopted from a similar study. 20 Furthermore, mothers’ socio-demographic characteristics, mothers’ obstetric characteristics, and mothers’ knowledge of danger signs during pregnancy were also considered in the analysis.
Skilled delivery service utilization
Skilled delivery service utilization is the use of delivery services provided at health facilities and attended by skilled attendants in clinics, health centers, public and private hospitals among mothers who gave birth in the last 12 months for their last delivery.
Mothers’ perception to the nearby health facility’s physical environment
This was assessed using five items inquiring about the presence of waiting area, maternity ward’s toilets, hand washing and shower, infrastructures like electricity, water, and easiness of getting maternity ward starting from the gate. Each item had 5-point Likert-type scale from strongly disagree (1) to strongly agree (5). The total sum was dichotomized into “Good” and “Poor” depending on the mean score. This dimension had an internal consistency or reliability score of 0.81.
Mother’s perception to service providers’ technical ability
This construct was intended to measure how mothers perceive the professional ability of the care provider in terms of handling labor and complication. This was assessed using three items inquiring about support given during, labor and delivery, care given to newborn, and pain management. Each item had 5-point Likert-type scale from strongly disagree (1) to strongly agree (5). The total sum was dichotomized into “Good” and “Poor” depending on the mean score. This dimension had an internal consistency or reliability score of 0.76.
Time to reach to the nearby health facility (on foot)
This was assessed by asking mothers, what time it takes from home to the nearby health facility, on foot. Their responses were dichotomized into “<1 h” and “⩾1 h.”
Mother’s perception of the availability of prompt transport service from home to health facility
This was assessed from mothers’ self-report; mothers responding “Yes” to the statement “prompt transport service (an ambulance) from home to the nearby health facility is available” were code 1; otherwise, 0.
Mother’s perception of service charge
This was assessed from mothers’ self-report; by asking mothers how they perceive the delivery service charge in the nearby health facility, and three options were provided “High,” “Moderate,” and “Low.”
Mother’s knowledge of danger signs during pregnancy
Mother’s knowledge of danger signs during pregnancy was measured by a list of nine danger signs stated by WHO guide for essential practice (Childbirth, postpartum, and Newborn). 21 Mothers were regarded to have “Good knowledge,” if they were able to spontaneously mention at least four of the nine danger signs, otherwise, “Poor knowledge.”
Data processing and analysis
Data were checked for completeness, edited, cleaned, coded, and entered into Epi Data version 3.1 and then exported to SPSS version 20 for analysis. Descriptive statistics were computed to assess the prevalence of skilled delivery service utilization and other relevant variables. In the descriptive statistic, frequencies, proportion, and mean were calculated and the results of the analysis were presented in text, tables, and graphs. An unadjusted logistic regression model was fitted to detect whether there was any association between the outcome variable (skilled delivery services’ utilization) and mother’s socio-demographic characteristics, obstetrics characteristics, knowledge of danger signs during pregnancy, and perceptions to quality and physical accessibility-related with skilled delivery service. Then, variables demonstrating p < 0.25 on the unadjusted logistic regression model were considered candidates for the multivariate logistic regression. The final, multivariate logistic regression model was fitted to investigate the independent effect of each explanatory variable on the likelihood skilled delivery service utilization; odds ratio and their 95% confidence intervals (CIs) were computed and variables with p-value less than 0.05 were considered as significantly significant.
Data quality assurance
The tool which was prepared in English was translated into Amharic, and then back-translated into English to ensure its consistency. Before actual data collection commenced, the tool was pre-tested on 5% of the actual sample size in Sheko district, which is out of the selected area; then, amendments were made accordingly. There was a supervision on a daily basis and checking on 10% of the collected questionnaire. Finally, error reports were checked after entry to Epi data using each case code.
Ethical consideration
Before data collection, ethical clearance was obtained from the College of Health Science, Mizan-Tepi University, and an official permission letter was also obtained from Kaffa Zone administration and Kaffa Zonal health office. Written informed consent was sought from all participants, after explaining the study’s purpose, risks, and benefits. Moreover, participants were assured that their participation was voluntary and personal information will never be disclosed.
Result
Socio-demographic characteristics
In this study, 374 mothers willingly responded to the interviewer-administered structured questionnaire making a response rate of 93.7%. The mean age of the respondents’ was 24.6 (±4.2) years. The majority of the respondents, 330 (88.2%) were currently married women. Regarding their educational attainments, more than half of the respondents, 242 (64.7%) had no formal education, while 87 (23%) attended primary education, and the remaining 45 (12%) completed secondary education and above. One hundred and ninety-eight (52.9%) and 115 (30.7%) were Orthodox Christian and Protestant faith followers, respectively (Table 1).
Socio-demographic characteristics of study participants, Ethiopia, August 2019.

Obstetric and related characteristics
Regarding age at first pregnancy, 219 (58.6%) were pregnant at the age of 19–25 years and 64 (17.1%) were pregnant before they turned 19 years. The majority of respondents made at least one antenatal care (ANC) visit, during pregnancy, of which only 98 (26.2%) of the respondents attended all the WHO recommended ANC visits, 7 while 113 (30.2%) attended two ANC visits, and the rest 103 (27.5%) made a single visit. The majority of the respondents were multigravida and multipara, and 97 (25.9%) of the respondents reported that their pregnancy was unwanted (Table 2).
Obstetrics and related characteristics of study participants, Ethiopia, August 2019.

ANC: antenatal care.
Mothers’ knowledge of danger signs during pregnancy
About 126 (33.7%) of the respondents were able to mention more than three signs of danger sign during pregnancy and were regarded as having “Good knowledge.” Vaginal bleeding (63.9%), headache (49.7%), and reduced fetal movement (45.5%) were the most frequently mentioned danger signs by the respondents (Figure 1).

Mothers’ knowledge of danger signs during pregnancy in Kaffa Zone, Ethiopia, August 2019 (N = 374).
Mothers’ perception of quality and accessibility of skilled delivery service
Mothers’ were asked how they perceive the quality, accessibility, and affordability of the skilled delivery service, in the nearby healthcare facility. Accordingly, 231 (61.8%) of the respondents perceived the physical environment of the nearby health facility as “Good,” and the service providers’ technical ability was designated as “Good” by 258 (69.0%) of the respondents. Regarding time to reach the nearby health facility (on foot), about 215 (57.5%) respondents mention that it will take less than 1 h from home to the nearby health facility and 131 (35%) respondents claimed that prompt transport service is unavailable when needed (Table 3).
Mothers’ perception of quality and accessibility of skilled delivery service, Ethiopia, August 2019.

Skilled delivery services’ utilization
In this study, 262 (70.1%) of the recent births (occurred in the past 12 months) were attended by skilled birth attendants, of those 148 (56.5%) births were attended at health centers, and 114 (43.5%) births were attended at hospitals. Mothers were asked why they used skilled delivery service and 107 (41%) mothers mentioned that they were advised by health extension workers, 81 (31%) mentioned that they were informed during ANC visit, and 74 (28.24%) thought that it would be safe both for the newborn and for the mother.
Factors associated with skilled delivery service utilization
To select candidate variables for the final multivariate logistic regression, binary logistic regression was carried out. Accordingly, mothers’ socio-demographic characteristics, obstetrics characteristics, mothers’ knowledge on danger signs during pregnancy, and mothers’ perception of quality and accessibility were discretely entered into the bivariate logistic regression, and eventually, 10 variables became candidate yielding a p-value ⩽ 0.25. After adjusting for the mother’s age, monthly income, pregnancy status, and mother’s perception of the service provider’s technical ability, six variables demonstrated a significant association with the likelihood of utilizing skilled delivery service utilization.
Mothers regarding the nearby health facility’s physical environment as “Good” (adjusted odds ratio (AOR) = 2.48, 95% CI = 1.44, 4.25), mothers mentioning time to reach to the nearby health facility “less than 1 h” (AOR = 1.92, 95% CI = 1.11, 3.34), and mothers regarding prompt transport service from home to the nearby health facility “Available” (AOR = 2.01, 95% CI = 1.11, 3.63) were positively associated with the likelihood of utilizing skilled delivery services. In addition to the physical accessibility, and mothers’ perception of service quality, the likelihood of utilizing skilled delivery service was significantly associated with completing secondary education and above (AOR = 3.52, 95% CI = 1.40, 8.84), attending three and more ANC visits (AOR = 4.41, 95% CI = 1.88, 10.31) and having good knowledge of danger signs during pregnancy (AOR = 2.29, 95% CI = 1.27, 4.12) (Table 4).
Factors associated with skilled delivery service utilization in multivariate logistic regression, Ethiopia, August.
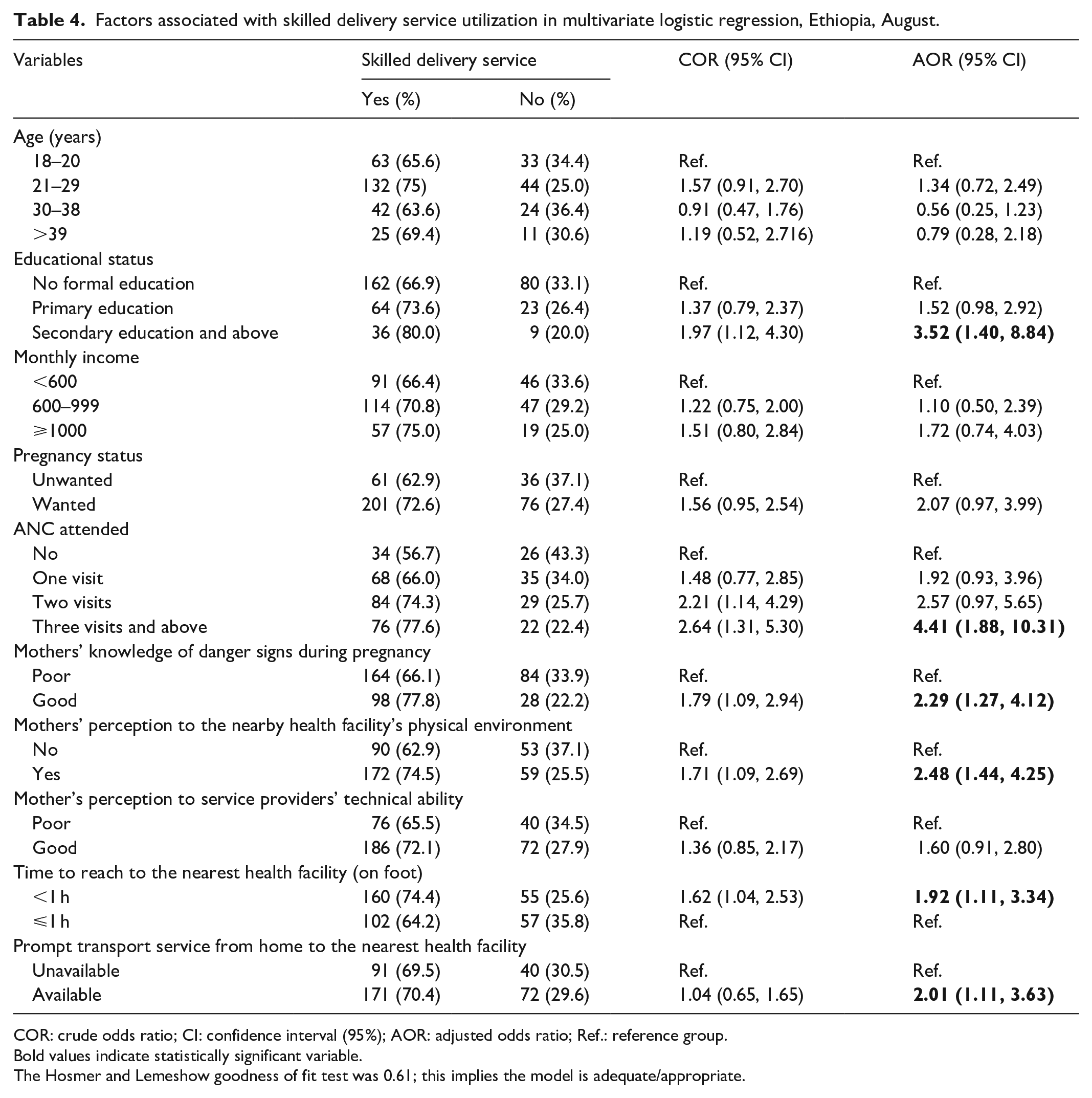
COR: crude odds ratio; CI: confidence interval (95%); AOR: adjusted odds ratio; Ref.: reference group.
Bold values indicate statistically significant variable.
The Hosmer and Lemeshow goodness of fit test was 0.61; this implies the model is adequate/appropriate.
Discussion
This study established that 70.1% of the childbirths that occurred in the past 12 months were attended by skilled health personnel. This prevalence is more or less comparable with studies conducted in Bahir Dar, Tigray, and Tanzania.22–24 However, the finding is much higher when compared with studies conducted in the different parts of the country: Munisa, Arsi, Dodota, rural Jimma, and Sekela District. This discrepancy in prevalence could be attributable to the time difference in which the studies are undertaken; in the past few years, the Ethiopian government has made significant efforts to ensure access to skilled delivery service mainly through the expansion of health facility to the wider rural areas, community mobilization by health developmental army, and widespread implementation community-focused program known as the health extension program. 25 These coordinated efforts along with socio-economic development might have positively impacted maternal health service utilization in a rural part of the country.
“Three Delays” A Model of the Constraints to Effective maternity Care suggest perceived quality of care as a determinant for poor maternal service utilization. This means mothers not only driven by proven actual quality of care but also by perceived quality of care, this implies information gained from relatives, or friends matters as actual service quality matters. For this, in this particular study, attempts were made to measure mothers’ perception of the physical environment, service providers’ ability, accessibility, affordability, and service charge.
In this study, mother’s perception of the nearby health facility’s physical environment significantly predicted mother’s utilization of skilled delivery service. Mothers regarding the nearby health facility’s physical environment as “Good” were two times more likely to use skill delivery service than those who did not regard so. A similar study conducted in Northern Ethiopia affirmed this claim. 20 This implies that the expansion of health facilities to the different corners of the country alone does not guarantee mothers’ utilization of skilled delivery service. In a rural setting with the presence of various cultural and social deterrents, it is when mothers’ perception of service quality outweighs that they prefer skilled delivery over home delivery by TBAs (traditional birth attendants).
Time to reach the nearby health facility was found to be a strong predictor of skilled delivery service utilization. This finding is line with others studies done in Western Ethiopia, Dembecha District Ethiopia, and Zambia,20,26,27 where mothers reaching health facility with a lesser time were more likely to use skilled delivery service than those mothers who had to walk more hours to reach the nearby health facility. Again, the likelihood of utilizing skilled delivery was predicted by the mothers’ perception of availability of prompt transport service from home to the nearby health facility. Similarly, a study conducted in Northern Ethiopia reported that less proportion of mother utilized skilled delivery service among who claimed unavailability of easy transport service from home to nearby health facility. 20 In Ethiopia, various attempts have been made to improve mothers’ physical access to health service; more importantly, through provision of free emergency ambulance services for pregnant mothers, particularly for rural areas, where transport service is not easily available. However, it is still difficult to for women living in some pocket rural area to use the government’s free ambulance service, given poor road construction and difficult weather condition they live in.
Other than the health facility-related factors (mothers’ perception of quality and physical accessibility of skilled delivery service), completing secondary education and above, attending three and more ANC visits, and mother’s knowledge of danger signs during pregnancy significantly predicted the likelihood of utilizing skilled delivery service. Mothers completing secondary education and above were three times more likely to utilize skilled delivery service than mothers attending no formal education. Different studies have substantiated this fact that more educated mothers are more likely to seek skilled delivery service than the less educated mothers.28–32 In a patriarchal community like Ethiopia, men are the principal decision-makers in all matters including whether their spouses should utilize healthcare services; however, through education, women could challenge this inequality and make a decision on their own health affairs. The other likely explanation for this is that more educated mothers better comprehend the information being disseminated on mainstream media and other written materials promoting the utilization of skilled delivery service.
Mothers who made three and more ANC visits in their recent pregnancy were four times more likely to utilize skilled delivery service than those with no ANC visits at all; this is substantiated by other studies.33–35 Maternal continuum care strategy suggests that provision adequate ANC service during pregnancy improves the uptake of subsequent maternal health services including delivery and postnatal care; this might be for the fact that ANC offers a discussion platform between pregnant mothers and healthcare providers during which pregnant women share their concerns on the matters that hinder them not to utilize the service.
Mother’s knowledge of danger signs during pregnancy was found to be another important predictor of skilled delivery service utilization; the positive influence of mother’s knowledge of danger signs on the utilization of skilled delivery service has been suggested by different studies.26,36,37 This could due to the fact that mothers who recognize the danger signs during pregnancy better understand the possible maternal and neonatal risks associated with home delivery and they are more likely to seek skilled delivery.
Conclusion
Generally, skilled delivery service utilization in rural Kaffa zone is still low when compared with previous studies conducted among urban dwellers. Physical accessibility of the nearby health facility and mother’s perception toward the physical environment of the nearby health facility strongly influenced the utilization of skilled delivery service in the area. Furthermore, completing secondary education and above, attending three and more ANC visits, and having good knowledge of danger signs during pregnancy were found to have a positive association with skilled delivery service utilization. Although the study evidenced statistically significant association between perceived physical accessibility and perceived service quality, further study is recommended to investigate the relationship between actual physical accessibility and actual service quality. Targeted health education program intended to improve skilled delivery service utilization should give due emphasis on enhancing ANC service uptake, and raising mothers’ awareness on danger signs during pregnancy, with particular focus on those mothers with low schooling.
Limitations
The finding of this study has to been seen in light of some limitations. There might be possibility of social desirability bias as data collectors were from health system the response may be biased toward more positive answers. Another important limitation is the cross-sectional nature of the study means that it is impossible to determine causality.
Supplemental Material
sj-pdf-1-smo-10.1177_20503121211036794 – Supplemental material for Perceived physical accessibility, mother’s perception of quality of care, and utilization of skilled delivery service in rural Ethiopia
Supplemental material, sj-pdf-1-smo-10.1177_20503121211036794 for Perceived physical accessibility, mother’s perception of quality of care, and utilization of skilled delivery service in rural Ethiopia by Shewangizaw Hailemariam, Lidya Gutema, Molla Asnake, Wubetu Agegnehu, Biruk Endalkachew and Wondwosen Molla in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the Mizan-Tepi University for technical support and ethical approval, study participants, and data collectors.
Availability of data and materials
The data sets collected and analyzed for this study is available from the corresponding author and can be obtained upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the College of Health Science, Mizan-Tepi University (reference no. HSE/00429/2012).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.