
Abstract
Introduction:
Healthcare workers play a vital role in assessing and appropriately responding to family violence. Discipline-specific differences in the readiness to respond have been indicated in the literature but no studies have directly compared multiple disciplines using the same measure. Given the imperative need for a hospital-wide, multidisciplinary approach to managing family violence, this study aimed to compare and contrast clinician perceived levels of knowledge, confidence and clinical readiness to manage disclosures of family violence across major professional groups in a tier 1, tertiary adult trauma hospital in Australia.
Methods:
This prospective cross-sectional study implemented a brief questionnaire to explore self-reported knowledge, confidence and clinical skills in managing family violence. Data were analysed using non-parametric analyses. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for observational research were followed in the reporting of this study.
Results:
Significantly greater self-reported clinical skills, knowledge and confidence were found among social work clinicians relative to all other disciplines. By contrast, allied health clinicians reported the lowest levels of clinical knowledge, confidence and skills relative to other discipline areas. No significant differences were seen between nursing and medicine.
Conclusion:
There are significant differences across clinical professional groupings in knowledge and confidence levels, and clinical skills in assisting patients experiencing family violence. The findings have implications for facilitating a hospital-wide, multidisciplinary response to assisting clients experiencing family violence.
Keywords
Introduction
Family violence (FV) is recognised as a significant health problem with serious long-term impacts at both an individual and a societal level. 1 The Family Violence Protection Act (2008) in Victoria, Australia, defines FV as behaviour by a family member that is physically, sexually, emotionally or psychologically abusive, or behaviour that is threatening or coercive or in any way controls or dominates or induces fear for safety. 2 It also includes behaviour in which a child hears or witnesses or is exposed to the effects of this behaviour. In Australia, 2.2 million adults reported being subjected to physical and/or sexual violence from a partner since the age of 15 equating to 1 in 6 women and 1 in 16 men. 3 Globally, FV is a major cause of gender-based violence against women, defined by the World Health Organization as behaviour that results in, or is likely to result in, physical, sexual or mental harm or suffering to women. 4 Also, encompassed under this definition are threats of such acts, coercion or deprivation of liberty occurring in public or private settings. A recent global systematic review found that one-third of women worldwide have experienced either physical and/or sexual abuse perpetrated by an intimate partner. 5 In addition, as many as 38% of all murders in woman were found to have been committed by an intimate partner. 5
Available evidence indicates that women and children are most commonly the victims of FV, resulting in chronic physical and mental health problems and high levels of morbidity and mortality.3,6 Survivors have been found to have higher rates of hospital admissions and medical usage relative to their non-survivor counterparts. 7 Bonomi et al. 8 found women who were physically abused made more use of mental health, emergency department, outpatient, primary care and specialty related services. Recent Australian data indicate that between 2016 and 2017, 29% of all assault presentations in Australian hospitals were due to FV; a figure which has shown a steady increase over the last decade. 3 Similar findings have been documented internationally.8,9 The multidisciplinary nature of the healthcare sector is pivotal in the response to violence against women through its ability to provide a trusted and safe environment for disclosure and to assist to disrupt the cycle of violence.1,10,11 This includes the need to recognise medical co-morbidities occurring in those affected by FV and for more time and attention to be provided to integrate medical and FV intervention. 1
In 2015, the Victorian government launched a Royal Commission into Family Violence. The resulting comprehensive report emphasised the need for services to respond to survivors’ needs in a timely and appropriate manner and called for a ‘whole-of-hospital’ model for responding to violence. 12 The Commission found many victim-survivors continue to interact with healthcare professionals in seeking treatment for injuries sustained from violence, despite not contemplating engagement with specialist FV services. As such, frontline hospital staff need to be ready to facilitate a unified approach to the acute management of FV.
The existing literature has highlighted gaps in clinician perceived knowledge and readiness across professions. Studies in various healthcare settings and fields such as obstetrics and gynaecology, primary care specialties, psychiatrists, and trainees and community mental health practitioners have found that basic knowledge in the identification and management of abuse is lacking.10,13–16 Despite overarching similarities in findings across studies, a number of differences have been identified across professional groups. For instance, relatively high rates of knowledge and confidence were identified at a government maternal health service 17 but not in the overall combined responses for all clinical professions in an adult hospital for the current study. 18 To date, no studies have robustly compared and contrasted clinician readiness across professional groups within a large tertiary public hospital in Australia. Given the complex nature of FV and government recommendation for a unified, whole of hospital response, there is a need to understand relative areas of strength and weakness in clinician self-rated knowledge and confidence in FV clinical skills, by discipline. Doing so represents an essential first step in tailoring training to match the baseline skill sets of clinicians across disciplines. This study further analyses the overall data presented by Fisher et al., 18 by comparing clinician perceived levels of knowledge, confidence and clinical readiness to manage disclosure of FV across major professional groups in a tier 1, tertiary adult trauma hospital in Australia. It was hypothesised that differences would be seen across professional groupings, and that social workers were likely to report higher levels of knowledge and confidence working in their area, relative to other discipline colleagues. The basis for this was FV being part of required curricular content for social work accreditation standards and that clients experiencing FV are routinely referred to social workers in hospital settings.19,20
Method
Design and materials
This study aimed to prospectively explore clinician reported knowledge, confidence, clinical abilities and barriers in managing FV across professional clinician groupings in a large metropolitan hospital. The overall combined total results for this dataset have already been reported, along with the details of the brief, but targeted, online survey designed to collect these data. 14 The questionnaire was newly developed as no tools available at the time had the properties required to meet the needs of the research project. 14 This article presents the results of the study separated and compared by clinical professional groupings. Data from this study were collected using the online questionnaire, administered on the Survey Monkey platform (see Supplementary File 2), over a 6-week administration period in November–December 2017. Cronbach’s alpha from the current data was 0.83, which represents satisfactory internal consistency. Informed consent was presumed on submission of the anonymous questionnaire. The study was conducted as part of ‘baseline’ research into FV response skill levels in clinicians, prior to the roll out of a hospital-wide FV transformational change project. The local hospital environment at the time of the study was one in which no dedicated FV procedure or guideline existed to guide screening or practice for staff, and no regular or routine training in FV clinical response was available.
This article sought to specifically compare and contrast nursing, allied health, medicine and social work knowledge, confidence and clinical skills in responding to FV. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines for observational research 21 were followed in the reporting of this study (Supplementary File 1).
Participants and setting
Clinicians from a large government tertiary trauma hospital in Melbourne, Australia, were approached to participate. The hospital encompasses multiple divisions across both acute and subacute settings including emergency medicine, trauma and community rehabilitation. All available email addresses of nursing (N = 1541), medical (N = 1067) and allied health (N = 422) staff were sent an email inviting them to participate online. Existing organisational email distribution lists for medical and allied health staff were utilised. A distribution list for nursing staff was developed by collating the organisation email addresses of all staff in the email directory with a role description that aligned to nursing (e.g. Nurse Unit Manager, Assistant Nurse Unit Manager, Registered Nurse, Enrolled Nurse, Nurse Educator and Nurse). The sample size was not predetermined, as the survey was open to all clinical staff with email addresses available to the research team, and the actual response rate could not be conclusively determined. The response rate percentage was estimated to likely fall between 10% and 20% based on two other online-only surveys in large samples of healthcare workers.22,23 Although in another recently published FV survey conducted in healthcare workers, across services, a response rate of just 6.7% was obtained, and thus a lower response rate was possible given the nature of the subject matter. 10
Approval for this study was granted by the Melbourne Health Human Research and Ethics Committee (HREC/17/MH/283). Data were collected anonymously, with informed consent assumed upon submission of survey responses, as approved by the ethics committee.
Data analysis
All data were analysed using SPSS (version 26). A two-sided alpha value of less than 0.05 was considered statistically significant for all analyses. Differences in self-reported rates of knowledge, confidence, screening and frequency of working with clients who disclose between professional groups were analysed using Kruskal–Wallis test. Post hoc analysis using pairwise comparison was undertaken to explore significant effects, with Bonferroni’s correction applied. Effect sizes were calculated using Cohen’s f coefficients, 24 with magnitude interpreted according to Cohen (1988) (0.1 = small, 0.3 = medium and 0.5 = large). This non-parametric analysis was chosen due to the ordinal nature of data. Nominal data relating to demographics, understanding of indicators, knowledge of how to manage disclosures and ability to inquire about violence were compared using chi-square analyses. Post hoc analysis using Bonferroni’s correction was applied.
Results
Participants
A total of 534 staff participated in the online survey, representing 18% of all clinical staff invited to participate via email. Greatest levels of participation were seen for social work (100% response rate) and the remainder of (non-social work) allied health (48%), followed by nursing (16%) with comparatively low rates evident in medical staff (6%) (see Table 1 for sample demographics and further information on specific disciplines/clinical areas within the professional groups). Significant disparities were evident between social work clinicians and all other disciplines in allied health, with greater self-reported clinical skills observed in the former. This supported the pre-planned approach to separate social work from remaining allied health disciplines in all analyses.
Participant demographics.
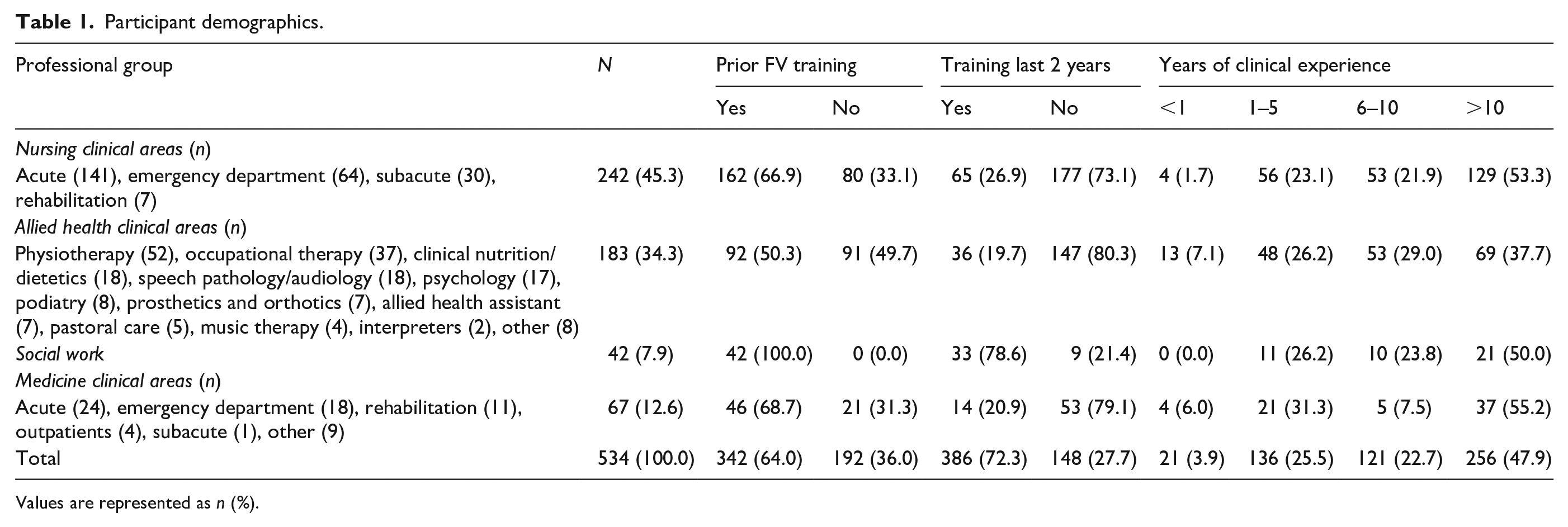
Values are represented as n (%).
As seen in Table 1, while most clinicians described some prior FV training experience, the majority had not received training within the last 2 years. The one notable exception to this was in social work, where most clinicians had received recent training.
Chi-square analysis indicated a significant difference in training rates in the clinicians who had completed prior FV training across professional groups (χ2 = 40.15, p < 0.001). Post hoc analysis indicated that non-social work allied health clinicians were significantly less likely to have undertaken prior training, while social work clinicians were significantly more likely to have undertaken FV training (p < 0.001 for both). A significant difference was also seen in clinicians who had completed training in the last 2 years across professional groups (χ2 = 61.77, p < 0.001). Post hoc analysis again indicated that social work clinicians were more likely to have undertaken training (p < 0.001) and allied health significantly less likely to have undertaken training in the last 2 years (p = 0.03). Finally, while there was a significant difference in years of experience between professions (χ2 = 28.06, p < 0.001) at an overall level (with allied health having a lower proportion of clinicians with more than 10 years of experience), this association was not seen in any between-group comparisons on post hoc analysis.
Knowledge, confidence and screening
In order to explore differences in self-reported knowledge, confidence, screening rates and frequency of working with those who disclosed violence, a series of Kruskal–Wallis analyses were conducted (see Table 2 for associated mean ranks).
Mean ranks for self-reported knowledge, confidence and screening for family violence between clinical groups.

There was a large, statistically significant difference between self-reported knowledge among professional groups, H = 122.27, df = 3, p < 0.001, Cohen’s f = 0.55. Post hoc analysis using pairwise comparisons indicated that allied health clinicians reported significantly lower levels of knowledge than nursing (p = 0.003) and social work (p < 0.001) colleagues. By contrast, social workers reported significantly greater levels of knowledge than all other professional groups (p < 0.001 for all comparisons). No significant difference was seen between medical staff and nursing staff (p = 1.00) nor between medical and allied health counterparts (p = 0.08).
Regarding clinical confidence, there was a large, statistically significant difference between self-reported confidence among professional groups, H = 116.22, df = 3, p < 0.001, Cohen’s f = 0.53. Pairwise comparison with Bonferroni’s correction again revealed significantly greater confidence among social work clinicians compared with all other disciplines (p < 0.001 for all comparisons). Allied health self-reported significantly lower levels of confidence than medicine and nursing staff (p < 0.001 for both). No further difference was observed between medical and nursing clinicians (p = 1.00).
A moderate, statistically significant difference was seen between professional groups on self-reported frequency of screening clients for FV, H = 99.30, df = 3, p < 0.001, Cohen’s f = 0.48. Social work clinicians reported significantly greater frequency of screening clients than all other disciplines (p ⩽ 0.001 for all comparisons). By contrast, allied health clinicians reported significantly lower rates of screening than medicine and nursing counterparts.
Finally, frequency of working with clients who disclose FV, Kruskal–Wallis analysis indicated significant difference between professional groups, H = 50.34, df = 3, p < 0.001, Cohen’s f = 0.32, of a medium magnitude. Social work again reported significantly greater frequency of working with clients who had disclosed, relative to nursing (p < 0.001), medicine (p = 0.05) and allied health (p < 0.001). Further difference was seen between allied health and medicine clinicians, with the latter reporting greater frequency of working with clients who had disclosed FV (p < 0.001). No further significant difference was seen.
Clinical skills
A series of chi-square analyses were used to investigate the differences in clinician knowledge of FV indicators, knowledge of how to ask about FV and capacity to manage FV disclosures (see Table 3). As noted in Table 3, all chi-square analyses indicated differences in clinical skills in these areas. Post hoc-analysis with Bonferroni’s correction indicated that allied health clinicians were significantly less likely to know, or somewhat know, how to ask about FV (p < 0.001 and 0.03, respectively). By contrast, social work clinicians were significantly more likely to know how to ask about FV (p < 0.001). The same pattern was seen in clinician knowledge of FV indicators, with allied health significantly less likely to know about indicators (p < 0.001) and correspondingly more likely to not know (p = 0.01). The opposite pattern was seen in social work with clinicians significantly more likely to report knowledge of FV indicators, than to report that they did not know (p < 0.001 for both). For FV disclosures, allied health were significantly less likely to know how to respond to disclosures, and more likely to not know how to respond (p < 0.001 for both) following disclosures of FV. The opposing finding was again seen in social work (p < 0.001 for both). No additional significant differences were seen between nursing and medical clinicians for knowledge of how to respond to FV disclosures.
Summary of clinical skills across professional groups.

FV: family violence. Values are represented as n (%).
Discussion
This study aimed to compare and contrast self-reported levels of knowledge, confidence and clinical readiness to respond to FV disclosures across major clinician professional groups in a tertiary trauma hospital in Australia. Findings indicated significantly greater perceived clinical skills, knowledge and confidence among social workers relative to all other disciplines. The results are consistent with the existing literature and highlight the unique and skilled role that social workers play in the acute hospital setting.25,26,27 These data are unsurprising given the course accreditation requirement for Australian social work clinicians to have a critical understanding of domestic and FV as part of curriculum content 19 : requirements not yet mirrored in other discipline groups. Consistent with this notion, all social work clinicians reported some prior FV training, compared with half of allied health, and just under two-thirds for nursing and medicine clinicians. Taken together, findings emphasise the importance of training and associated accreditation standards to support clinician readiness to respond to FV.
Higher levels of clinical skill and knowledge in social workers may also reflect their role within multidisciplinary teams, which increases the likelihood they would have previously been required to assist clients with these issues. There is a high frequency of referrals to social work from nursing and medical staff when FV is suspected, 20 and existing research emphasises the need for social workers to have a presence in emergency departments to support this work. 28 This contributes to a high expectation and demand on social work clinicians to take a more active role in assessing and managing FV in the hospital context. While results in this professional group are encouraging, given that FV involves complex biopsychosocial interactions, 29 victim-survivors will likely benefit from a multidisciplinary approach to care from a variety of healthcare workers across disciplines who can provide a multifactorial approach to management. A recent study, in the same hospital, indicated that patients self-reported disclosing FV concerns to staff from a range of different professions (including social work, clinical psychology, neuropsychology, physiotherapy and nursing staff). 30 Hence, there remains a need for all clinical professions to be adequately skilled, knowledgeable and confident in this area to meet the requirement of a whole of hospital response. A whole of hospital response also aligns with the national strategy in Australia recommending that both first point of contact and mainstream services (i.e. those that are not FV specific) are skilled at identifying and responding to FV needs in clients. 31
Allied heath clinician respondents reported the lowest levels of clinical knowledge, confidence and skills relative to other discipline areas. The explanation for this finding is less clear and may relate to discrepancies in prior FV training. Compared with their medicine and nursing counterparts, allied health clinicians were significantly less likely to have received FV training (at all, and in the last 2 years). Fisher et al. 30 identified that a minimum of 7–9 h of training was needed to establish ‘moderate’ levels of knowledge, while 10–15 h was needed to build ‘moderate’ confidence. Hence, in the absence of prior training, allied health clinicians may be less likely to develop clinical skills needed to detect and manage FV. Another potential explanation for this finding is the low levels of normative beliefs and behavioural control identified among allied health clinicians in relation to adopting evidence-based practice, 32 which may be accounting for lower perceived confidence, knowledge and skills.
This study is not without limitation. Due to the anonymous nature of data collection, this study was unable to examine participant-level factors which may be affecting outcomes. Similarly, data are taken from a single tertiary trauma hospital and while we did achieve statistical significance in inferential analyses, no formal power analysis was undertaken. Consequently, findings may not be generalisable to all trauma services. There is also likely a degree of response bias in the sample, particularly self-selection bias, as participants were free to choose whether to participate. Participants may have had a higher level of interest in the subject matter than staff who did not participate, and may have had more time/access to a computer/email as part of their role than those who did not. Finally, the results are based on self-report and may not reflect actual clinical practice. Notwithstanding, this study provides an important snapshot of differences among clinical staff readiness to manage violence with clear implications for clinical practice.
Conclusion
This study has shown significant differences across clinical professional groupings in a tertiary hospital in knowledge and confidence levels, and clinical skills, in assisting patients experiencing FV. Consistent with their scope of practice, social workers had received the most training and self-reported higher FV knowledge, confidence and skill levels. For a whole of hospital response to be effective, improvements in FV skills are required in the remaining professional groupings of nursing, medicine and particularly, allied health. FV disclosures from patients can be provided to clinicians from any profession. All clinicians should have adequate capacity to respond and assist appropriately.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211000923 – Supplemental material for Responding to family violence: Variations in knowledge, confidence and skills across clinical professions in a large tertiary public hospital
Supplemental material, sj-docx-1-smo-10.1177_20503121211000923 for Responding to family violence: Variations in knowledge, confidence and skills across clinical professions in a large tertiary public hospital by Toni D Withiel, Helen Gill and Caroline A Fisher in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121211000923 – Supplemental material for Responding to family violence: Variations in knowledge, confidence and skills across clinical professions in a large tertiary public hospital
Supplemental material, sj-docx-2-smo-10.1177_20503121211000923 for Responding to family violence: Variations in knowledge, confidence and skills across clinical professions in a large tertiary public hospital by Toni D Withiel, Helen Gill and Caroline A Fisher in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all of the clinicians who supported the conduct of this study and invested their time and effort in making it possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Victorian state government as part of the Strengthening Hospital Responses to Family Violence (SHRFV) initiative.
Ethical approval
Ethical approval for this study was obtained from the Melbourne Health Human Research and Ethics Committee (No. HREC/17/MH/283).
Informed consent
As data were collected anonymously, informed consent was assumed upon submission of survey responses. This methodology was approved by the above listed committee.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.