
Abstract
Objectives:
This report summarizes a collaborative effort between the American Society of Reconstructive Transplantation and the International Society of Vascularized Composite Allotransplantation to establish what is known about chronic rejection in recipients of vascularized composite allografts, with an emphasis on upper extremity and face transplants. As a picture of chronic rejection in hand and face vascularized composite allografts emerges, the results will be applied to other types of vascularized composite allografts, such as uterine transplantation.
Methods:
The overall goal is to develop a definition of chronic rejection in vascularized composite allografts so that we can establish longitudinal correlates of factors such as acute rejection, immunosuppressive therapy, de novo donor-specific antibody and trauma/infection and other external factors on the development of chronic rejection. As Dr Kanitakis eloquently stated at the 2017 International Society of Vascularized Composite Allotransplantation meeting in Salzburg, “Before we can correlate causative factors of chronic rejection, we have to define what chronic rejection in VCA is.”
Results:
The first meeting report was presented at the sixth Biennial meeting of the American Society of Reconstructive Transplantation in November 2018. Based on collaborative efforts and descriptions of clinical cases of chronic rejection in vascularized composite allograft recipients, a working definition of chronic rejection in vascularized composite allografts with respect to overt functional decline, subclinical functional decline, histologic evidence without functional decline, and normal allograft function in the absence of histologic evidence of chronic rejection is proposed.
Conclusions:
It is the intent of this collaborative working group that these working definitions will help to focus ongoing research to define the incidence, risk factors and treatment regimens that will identify mechanisms of chronic rejection in vascularized composite allografts. As with all good research, our initial efforts have generated more questions than answers. We hope that this is the first of many updates.
Purpose
This report summarizes a collaborative effort between the American Society for Reconstructive Transplantation (ASRT) and the International Society of Vascularized Composite Allotransplantation (ISVCA) to establish what is known about chronic rejection (CR) in recipients of vascularized composite allografts (VCA), with an emphasis on upper extremity and face transplants. As a picture of CR in hand and face VCA emerges, the results will be applied to other types of VCA, such as abdominal wall and urogenital transplantation. As uterine transplants are not intended for long-term engraftment, this type of graft will not be a focus of this working group. The first meeting report of this working group was presented at the sixth biennial meeting of the ASRT in November 2018. Based on preliminary collaborative efforts and descriptions of clinical cases of CR in VCA recipients, the working group has proposed a working definition of CR in VCA with respect to overt functional decline, subclinical functional decline, histologic evidence without functional decline, and normal allograft function in the absence of histologic evidence of CR.
In this report the following details will be addressed: (1) the background and rationale for establishing the working group and a summary of how CR is defined for solid organ transplantation (SOT); (2) an overview of the current observations of CR-like symptoms in clinical VCA recipients; (3) a working definition of CR based on clinical observations and a draft classification system based on preliminary data from the centers collaborating in this working group. Finally, the report reviews some of the unanswered questions and the initial areas that will be the focus of the working group as we refine our definitions and classifications.
Defining the problem
Over the past several years, accumulating new clinical observations by VCA programs have resulted in a call for updates to the 2007 Banff pathologic criteria.1–7 In 2016, an international workshop on VCA histology entitled “Grades and Stages of Rejection: Towards Clinical Correlation” was organized through the ISVCA and held at Duke University Medical Center in Durham, North Carolina. At the 2017 ISVCA meeting in Salzburg during a discussion of how CR developed in VCA, Dr Jean Kanitakis eloquently stated, “Before we can correlate causative factors of chronic rejection, we have to define what chronic rejection in VCA is.” These meetings as well as ongoing discussions between VCA centers and at meetings of the ASRT and ISVCA have fueled the formation of this working group, with a mission to establish a working definition of CR in VCA that can be tested and applied to future research in VCA. The Chauvet Working Group—an international collaborative effort to address unique psychosocial issues in VCA—provided a template for discussions between then ASRT president Sue McDiarmid, MD, and ISVCA president Emmanuel Morelon, MD, to establish collaborative working groups between the two societies and others to address issues critical to the advancement of the field. The ASRT/ISVCA Chronic Rejection Working Group (CRWG) was one of the groups that resulted from these discussions.
As a first step in defining CR in VCA the working group examined the processes involved in defining the CR criteria for other organs such as the heart and lung. 8 For SOT in 1997, a definition of CR was proposed as follows: “A process which induces late terminal graft failure, following a progressive decrease in organ function.” 9
This initial definition for CR in SOT does describe some processes that have occurred in VCA recipients, but does not cover the diversity of presentations, some of which resulted in VCA failure at less than 1 year. Of note, this initial definition has evolved extensively over the years for SOT, and we expect the definition of CR in VCA to undergo the same transitions. It is the intent of this collaborative working group to propose working definitions for CR in VCA to focus ongoing research to define the incidence, risk factors and treatment regimens that will identify mechanisms of CR in VCA. An underlying objective of the working group is to use these definitions of CR in VCA to establish longitudinal correlates of causative factors on the development of CR. The long-term goal of this collaborative working group is to define an “if/then” algorithm that will identify CR in VCA patients at the very earliest phases, ideally in a timeframe to permit effective intervention.
In the initial meetings of the working group, discussion centered on first reviewing what is established regarding CR of the components of VCA as defined in SOT. Focus was given to presentations of CR in SOT which might be similar to what has been observed in VCA recipients. A major limitation in defining both acute rejection (AR) and CR in VCA recipients is the lack of a laboratory marker of rejection such as serum creatinine that is available in renal transplantation. Vasculopathy, with involvement of both arteries and veins, although the former are affected more severely, appears to be a manifestation or feature of CR in VCA recipients. The primary target of CR in cardiac transplantation is also the vessels, and in 2010, the International Society for Heart and Lung Transplantation (ISHLT) developed a working formulation to describe cardiac allograft vasculopathy (CAV). 8 CAV is characterized by the proliferation of the intima, in a diffuse and concentric pattern that can be very aggressive and result in graft ischemia and failure. As experience incorporated angiography and the use of intravascular ultrasound as diagnostic markers in addition to immunohistologic and circulating biomarkers, progress was limited by a lack of standards in the nomenclature of CAV. The approach used was to define cardiac function in the complete absence of disease (vasculopathy) followed by histologic evidence in the absence of symptoms, and then as patients became symptomatic and showed significant changes as evidenced by angiography and ultrasound. Then, as today, CAV is one of the major causes of morbidity and graft loss late after transplantation. 10 As humoral immunity has been associated with the development of CAV in both experimental 11 and clinical studies, 12 a logical approach was to treat heart-transplant recipients with the B-cell depleting agents rituximab. Interestingly, depleting B-cells early post-transplant resulted in a marked and significant increase in CAV in the first year. 13 While CAV was increased, the rate of rejection, infection, or mortality at 1 year was not affected. Overall, the development of DSA did not differ between the groups, although there was a trend for less anti-human leukocyte antigen-Class I (anti-HLA-CI) and more anti-HLA-Class II (CII) in the rituximab-treated heart-transplant recipients. A primary objective of establishing a working definition of CR in VCA is the potential to predict outcomes, in time to intervene. Based on definitions of CAV developed by the ISHLT, a retrospective analysis showed subjects with CAV grades of 0 and 1 at year 1 had significantly fewer major adverse cardiac events at 10 years post-transplant than those subjects with a CAV grade of 2 or 3. 14 This type of information would be of great value in managing VCA recipients. This is especially critical in the case of hand transplantation, with a practical exit strategy in response to complications related to immunosuppression.
While many VCA programs use immunosuppressive regimens based on renal transplant protocols, the correlation and nomenclature of CR between VCA and renal transplantation is not as direct. More than 50% of kidney allografts are lost by 10 years, 15 and death censored attrition rates beyond the first year of transplant have remained unchanged for the past 25 years. 16 The history of CR nomenclature in renal transplantation is complex. CR, chronic allograft nephropathy, transplant glomerulopathy, and chronic allograft injury are just some of the terms that have been used to describe a syndrome of chronic changes culminating in renal graft dysfunction. Most recently, during the 2017 Banff meeting, a category of chronic active T-cell-mediated rejection (TCMR) with Grade 1A, 1B, and II was added to designate the severity of the tubulitis involved, and the presence of chronic allograft arteriopathy was added. 17 In this respect, chronic changes in renal transplant are similar to VCA grafts in that there is more than one major target for chronic changes, namely, the vessels and glomeruli. Experience in liver transplantation may be less informative to the definition of CR in VCA. Overall, the incidence of CR is lower in liver transplants than other types of SOT with reports as low as 2% for graft failure due to chronic rejection. 18
In contrast to liver allografts, lung transplantation mirrors VCA in that rates of AR are high. Incidence rates of up to 90% have been reported, 19 but a more recent report for the Registry of the ISHLT describes an active cellular rejection (ACR) incidence of 28% in the first year post-transplant. 20 In addition, like VCA, although ACR is common in lung transplants, it responds well to treatment. Another commonality between the two types of transplant is continuous exposure of the allograft to the environment. Lung transplants are especially sensitive to a type of CR, bronchiolitis obliterans syndrome (BOS), which is the primary cause of lung graft failure, resulting in one of the shortest transplant graft half-lives, with a median patient survival of 5.8 years. 21 Risk factors for BOS include nonimmune influences such as primary graft dysfunction, gastroesophageal reflux, and viral, fungal and bacterial infection.21,22 The nomenclature of lung allograft dysfunction has evolved over the years, and BOS grade or staging is defined based on lung function, with 0 grade meaning normal function (forced expiratory volume (FEV1) > 90%) and grades 0-p, 1, 2 and 3 with lower functional readouts, culminating in FEV1 as less than or equal to 50% for BOS stage 3. 21 In addition, a new classification system for chronic lung allograft dysfunction (CLAD) was proposed to include restrictive form of CR which did not fit the criteria of BOS. 23 The term CLAD was proposed to cover all forms of graft dysfunction, despite the fact that CLAD was, and remains, not well defined. The authors proposed a flowchart of lung allograft dysfunction based on functional parameters as well as known specific causes. The working group considered this approach to be a good one for developing classification criteria for VCA CR.
CR in tissues specific to VCA
The skin is a defining feature of hand and face VCA allografts, and a major target of alloreactivity. In experimental models, a skin graft is commonly used to induce both cellular and humoral reactivity in naïve recipients, as well to test for the presence of donor-specific tolerance. 24 Multiple reports have focused on the immunobiology of skin in VCA,25–33 as well as normal subjects.34–42 Publications and experience prior to 2007 formed the basis of the Banff criteria for grading histologic rejection of the skin. 43 These criteria do discuss anticipated presentation of CR in skin of VCA recipients based on characteristics of skin graft versus host disease (GvHD) and scleroderma patients, but in 2007, CR in VCA had not been reported. In the last 12 years, there have been numerous observations and reports that now allow better definition of what changes in the skin would be good markers for a working definition of CR. These include potential predictors of AR and CR observed in VCA skin allografts that may be applicable to SOT. One example is the appearance of capillary thrombosis (CT) in VCA skin biopsies with moderate AR. 44 Another distinct feature of VCA grafts is that CR appears to target both skin and vessels, 7 with the development of tertiary lymphoid-like organs in the skin. 45
Because SOT is de-nervated, there is limited knowledge on the effect of CR on nerve tissue. In general, nerve tissue appears to be less antigenic than skin. 46 In a rat sciatic nerve model, triple drug immunosuppression with tacrolimus, mycophenolate Mofetil and prednisolone resulted in the best prevention of skin rejection compared to tacrolimus monotherapy at various doses. 47 However, motor recovery (and thereby nerve rejection) was not enhanced compared to tacrolimus alone. No immunosuppression in this model did result in reduced axonal regeneration, confirming nerve tissue is susceptible to alloimmune responses. 47 Histologic analysis of hand transplant recipients has not demonstrated significant cellular or humoral immunity directed against nerve tissue, although cellular infiltrates are seen occasionally or in very severe rejection or ischemia. Graft function in hand transplantation does not seem to be affected by AR, with the exception of edema which may physically impede function.48,49 Of note, while reconstructive surgeons take advantage of as much recipient nerve length as possible in the transplant, the majority of nerve tissue in the allograft is of donor origin. There is a clear demarcation both macro- and microscopically in vessels and nerves showing a lack of alloreactivity to recipient tissues. In a hand transplant recipient with severe vasculopathy resulting in ischemic graft loss at 9 months post-transplant, the donor nerves were relatively spared from histologic rejection, although pain was a major component of the symptoms leading to graft loss. 50 More recently, a hand recipient from the Louisville VCA Program lost his graft 8 years post-transplant after multiple episodes of AR, multiple surgeries (rotator cuff repair and carpal tunnel release) and infection. The patient had also shown evidence of skin changes and atrophy of the hand consistent with CR, and increased thickness of arterial vessel walls on ultrasound, although with patent vessels on ultrasound and magnetic resonance angiogram. Histology of nerve biopsies taken at the time of carpal tunnel release and after explant of the hand revealed significant cellular infiltrates of both the ulnar and the median nerves. 51 At the time of explantation, three digits had been lost to ischemia, and severe ischemic vasculopathy was present. Pain was the major complaint of the recipient in the months leading up to the graft loss, suggesting the nerves may have also been a target of alloimmunity. Alternatively, the pain may be a consequence of nerve infiltration by lymphocytes or associated with the inflammatory response in the context of ischemia. To date, there does not seem to be evidence of chronic nerve allograft rejection. The expected clinical or pathologic symptoms of chronic nerve rejection are likely to be chronic pain and decline in sensory or motor function. An additional complicating issue in upper extremity (UE) transplantation is the possibility of nerve compressions in native nerves outside the transplant which can result in numbness and pain in the graft.
Observations of CR in human VCA recipients
As proposed by Demetris et al. 9 in 1997, CR in SOT can be broadly defined as an indolent but progressive form of allograft injury characterized primarily by fibro-intimal hyperplasia of arteries, interstitial fibrosis (IF) and atrophy of parenchymal elements. For the most part this condition is irreversible, and often progresses to graft loss. As defined above, different solid organs are affected by CR at different levels, different rates, and in general at different parenchymal targets. Common features to liver, kidney, heart and lung transplantation are patchy organized interstitial inflammation, patchy IF and associated parenchymal atrophy, graft vascular disease, destruction of epithelial-lined conduits, and destruction and atrophy of organ-associated lymphoid tissue. 52 In general, graft loss as a result of CR occurs years after transplant, but loss can occur much sooner if vasculopathy is a major component. All of these presentations have been observed in recipients of VCA, but there are some significant differences between SOT and VCA.
In VCA, isolated graft vasculopathy was first noted in vascularized knee joint transplants 53 and then obliterative vasculopathy in a hand transplant recipient at only 9 months post-transplant. 50 The former presentation was remarkable for a lack of infiltrate and relative sparing of all other tissues at the time of graft loss. Subsequently it became obvious that CR could target more than one tissue, even in the early stages in VCA grafts. The Lyon team has published multiple reports of CR in VCA, including hand and face transplant,6,7,27,44,54,55 which presented with graft vasculopathy. A recent literature review found that graft vasculopathy has occurred in 6% of all human VCA recipients. 56 This review highlights the need for prospective and collaborative analysis of vasculopathy and CR in VCA. Review of previous publications is likely to miss unreported cases and key follow-up that is critical to correct conclusions. For example, some patients were initially reported to be DSA-positive, but subsequently it was determined that the DSA found were non-specific reactions. 57 The focal vasculopathy detected in one artery by histology did not evolve into clinically significant vasculopathy, and this subject continues to have minimal vasculopathy at more than 18 years post-transplant, although chronic skin changes are apparent. Assignment of a subject who did not present with DSA prior to (non-HLA antibodies were also tested and were negative, and IgG and IgM deposition on the amputated graft was also negative), but only after, amputation may not help to characterize the role of DSA by artificially skewing the small population. In addition, with more follow-up, the presentation of graft vasculopathy may be of a focal slowly progressing or aggressive confluent type. Further analysis of the types of long-term presentation is critical and is one of the focus areas of this working group.
Kanitakis and colleagues7,55 reviewed their own cases and those reported in the literature and established a list of clinical and pathologic findings of CR in VCA. These are summarized in Table 1 with additional observations from their publication on CT 44 and additional findings by Krezdorn et al. 58
Documented characteristics of chronic rejection in VCA recipients.

Another observation in VCA that may be different from SOT is the diversity of presentation of CR. In hand and face transplants, patients have presented with clear vasculopathy in the presence of skin lesions (Figure 1A) as well as chronic skin changes in the absence of significant vasculopathy in a hand (Figure 1B.A) and face transplant recipient (Figure 1B.B). Vasculopathy in the absence of acute or chronic skin changes has also been observed (Figure 1C). The observation that skin and vessels seem to be independent targets could be linked to different pathophysiological mechanisms: skin may be target of cellular immune response, whereas vessels may be more susceptible to chronic changes induced by humoral mechanisms. The type, duration and specificity of cellular or humoral response are also likely to play a role in these diverse outcomes.
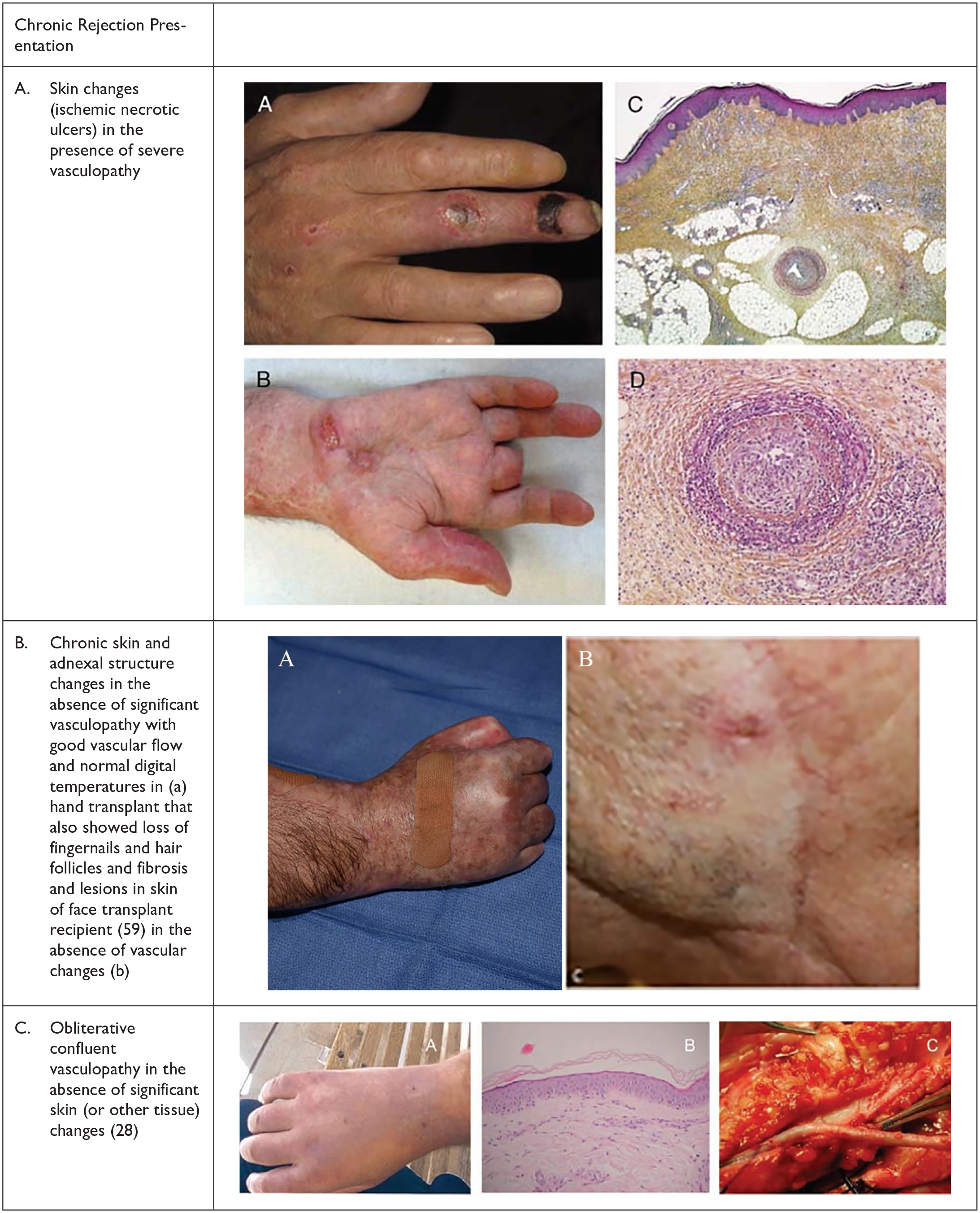
Diverse presentations of chronic rejection in hand and face transplant recipients.
In addition to the diverse presentations of what appears to be CR in VCA recipients, there are pathologic changes that could be predictive of CR in patients who are at risk. Kanitakis et al. 44 have reported an association of CT with severe rejection and CR in two of their VCA recipients. In this report the group also pointed out a number of new pathologic changes, not covered in the 2007 Banff Score, 43 including the deep vessel and medium cutaneous vasculopathy, dermal sclerosis and epidermal and adnexal atrophy. Two hand patients from the Lyon program were noted to have CT in the skin during AR, and one subject subsequently developed CR that led to graft loss. 44 This association was recently confirmed by the Louisville VCA Program at the 2017 meeting of the ISVCA in Salzburg, Austria. Two subjects who subsequently developed CR had CT in the first year post-transplant in association with Banff grade 2 or higher rejection episodes. By contrast, two other hand recipients who have not developed CR did not show evidence of CT in grade 2 or higher biopsies. In addition, CT was found after the development of CR, but only in the presence of significant AR. 59 Multicenter studies of digitalized skin biopsies are planned and will provide evidence for or against this potential marker for clinically relevant CR.
Many hypothesize that it is the magnitude and timing of the immune response that may drive outcome toward CR. After graft loss at 9 months in a hand transplant recipient due to vasculopathy, the Louisville VCA Program performed deep tissue biopsies and identified histologic evidence of vasculopathy in all patients tested. However, changes observed ranged from a mild focal vasculopathy that did not progress (or aging changes) to the confluent aggressive vasculopathy that affected all donor arteries resulting in ischemic graft loss. Subsequent analysis of arterial wall changes using very high-resolution biomicroscopy ultrasound have confirmed this diverse range of presentation in subsequent hand transplant recipients. In addition, changes in vessel wall thickness have been observed in the native vessels, underscoring the need to differentiate vasculopathy associated with aging, preexisting atherosclerosis and drug toxicity from alloimmune-mediated vasculopathy. In the Louisville program, a subject with chronic skin changes, ACR and antibody-mediated rejection (ABMR) rapidly developed vasculopathy after the development of infection in the transplanted arm, culminating in ischemic vasculopathy and graft loss. 51 Indeed, it is probable that multiple mechanisms resulting in vasculopathy are occurring at the same time. In Figure 2, Kolegraff et al. 2 picture the relationship of immune and nonimmune factors in VCA outcomes, including aging and recovery of sensation and function. In addition to the factors shown in Figure 2, the role of infection and environmental stimulators, such as vibration and trauma, may have led to the subject’s ischemic vasculopathy described above.

The natural history of a vascularized composite allograft includes reperfusion, wound healing, recovery of motor and sensory function and aging, as well as the alloimmune response.
A significant obstacle in defining CR in VCA is the paucity of clinical data. At well below 300 recipients, there simply are not enough cases to give a definitive definition. That said, there are enough cases to develop a working definition of CR, based on experience in SOT, and extrapolated to the data we have in VCA. Establishing that working definition is the primary current mission of the ASRT/ISVCA CRWG. We began the discussion by reviewing the literature and what strategies had been taken in defining CR in SOT, focusing on strategies for heart transplantation. Dr Mandeep Mehra 8 who was a key player in the development of a working formulation of a standardized nomenclature CAV for the ISHLT was invited to join the working group. Based on his input, reviews of the literature, the experience of Dr Kanitakis and Lyon group and others, as well as discussions held in conference calls/emails, and finally at the ASRT meeting in Chicago in November 2018, the following definition was proposed by the working group:
Objective—establish a working definition of CR based on the description of clinical VCA cases
The working group proposes that our definition characterize four different levels of CR as defined in Table 2.
Overview of working chronic rejection categories proposed and defining characteristics.
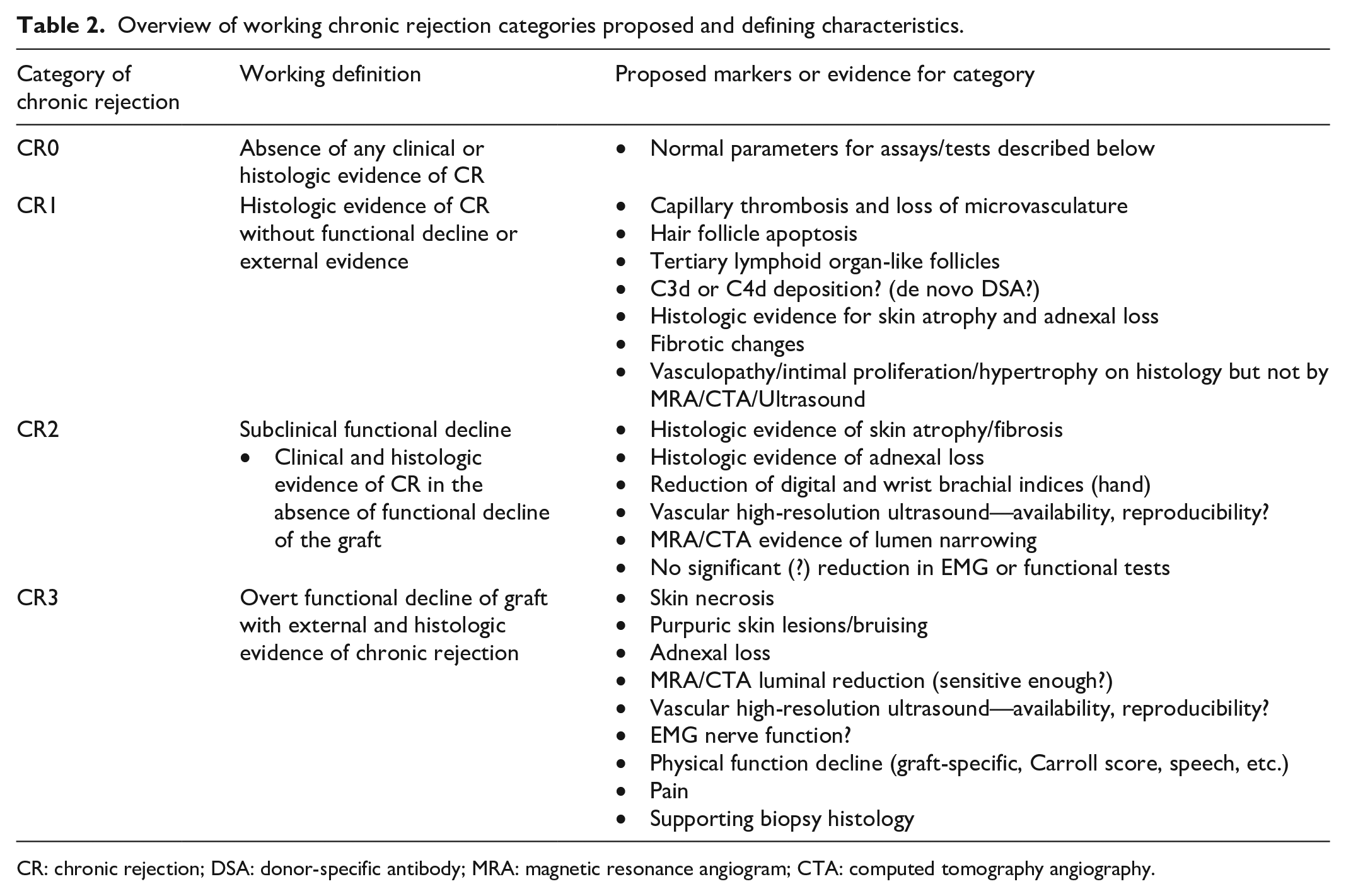
CR: chronic rejection; DSA: donor-specific antibody; MRA: magnetic resonance angiogram; CTA: computed tomography angiography.
Based on these working definitions, the working group asked active VCA programs to fill in a questionnaire on patients in their programs. The purpose of the pilot project was to obtain data that could be used to categorize de-identified patients in the proposed four groups with respect to CR. The questionnaire comprised of checkboxes in seven areas as well as limited demographics as shown in Table 3.
VCA patient questionnaire for pilot study.

VCA: vascularized composite allotransplantation; MRA: magnetic resonance angiogram; ACR: acute cellular rejection; DSA: donor-specific antibody; ABMR: antibody-mediated rejection; TLO: tertiary lymphoid organelle.
For the pilot study, two programs in Europe and five programs in the United States contributed de-identified patient information. There were a total of 37 patients. Based on the information provided, patients were assigned a category (CR0, CR1, CR2 or CR3). Figure 3 shows the data by number of transplants, with the average time posttransplant given in each category. Of the 37 subjects, 20 patients had no evidence of CR and 1 patient has only histologic evidence. However, 16 patients did have evidence, and 11 (30% of them) fell into the category or grade CR3 group. Five patients or 13.5% of them had histologic as well as radiologic or ultrasound evidence, putting them in the category or grade CR2 group. With the caveat that these data are preliminary and the working group is in the process of revising the questionnaire and including more centers, this first analysis does present a clear picture that hand and face VCA patients are at significant risk of vasculopathy and skin changes that are consistent with CR. Sixteen of the 37 patients (ca. 44%) had category CR2 or CR3 profiles. As seen in Figure 3, patients with a CR0 score had an average time post-transplant of 3.9 years, shorter than the average 7.5 years for CR3 patients. However, time post-transplant alone is not sufficient to induce CR as the time post-transplant was longest in patients in the CR2 and CR1 categories. Again, these data are preliminary, but it does provide data to guide future directions of the working group.

Time post-transplant versus CR category.
The data were further subdivided by the type of VCA graft, and this analysis is shown in Figure 4. The percentage of overall CR2/3 was about the same for face or UE recipients, but interestingly, face recipients appeared to have either no evidence of CR or significant CR (CR3) with external, functional and histologic evidence. Conversely, UE recipients have representation in all four categories.

VCA graft type versus CR category.
Again, these data are preliminary, but does suggest some differences between types of VCA, that might be important as the definitions for CR in VCA are refined.
These data were presented at the ASRT Meeting in Chicago in November 2018. In addition to the presentations of the working groups (in addition to the CRWG), there are also ASRT/ISVCA working groups addressing how to define function in UE and face transplant, as well as the long-term project of the Chauvet Working Group to define psychosocial issues unique to VCA and the ASRM/Uterus transplant working group.
Another unique aspect of the meeting was that the organizers saved time for a breakout session for the working groups to meet with any meeting attendees to discuss the presentation and potential future directions. In the CRWG, many interesting questions were raised, and despite the generous amount of time allocated to these meetings, the only consensus was that this project is a work in progress. Some of the questions raised by the working group as well as the attendees of the breakout session are listed below. The discussion also included a list of possible trigger factors, which have been summarized in Table 4:
Possible triggering factors for CR in VCA.

DSA: donor-specific antibody; ACR: acute cellular rejection.
How does time distinguish mechanism? Does ischemic vasculopathy at 9 months have the same causative factors as vasculopathy at 9 years?
How do we distinguish focal versus confluent involvement of the graft? Are these different mechanisms?
Non-uniformity of skin, that is, hand versus face, lips versus scalp, palm versus forearm, and so on.
Role of CT.
Role of lymph node (LN)/resident lymphocytes, Langerhans and other immune cells in donor skin
Role of composite proportion—that is, above the elbow allografts contain much more muscle and bone marrow than distal hand allografts
Role of mucosal epithelium
Role of direct interaction with environment
Role of vascularized bone (? marrow)
Potential of more than one primary target of CR in VCA (skin/vessels/muscle/nerve?)
Mild, focal slowly progressing CR versus aggressive, confluent catastrophic (perfect storm) CR? How do we define chronic “chronic” rejection versus acute “chronic” rejection?
In addition, the group discussed issues and caveats with the proposed working definition. The only category that did not raise concerns was that of CR0, with preserved function of the graft and no histologic evidence of CR. The subsequent categories or grades were more problematic. With respect to CR1, the issue of multiple targets of CR in the graft was raised. Is histologic evidence of vasculopathy in the small vessels equivalent to changes to the dermis or epidermis? There will be a hierarchy of histologic changes which may be more informative than just any histologic evidence of CR. Also, it may be that dropout of adnexal structures histologically may be more predictive of progression to CR2 and CR3 than epidermal or small vessel changes. With only four categories there is also concern that someone with minimal focal vasculopathy might be categorized the same as someone with confluent thickening of the vessels and evidence of dermal atrophy that is not yet apparent externally.
Some of the same issues, that is, importance of vascular versus tissue changes for CR2, were raised, but the diverse presentations and outcomes associated with CR in category CR3 was a focus of the discussion. There does not appear to be a typical presentation of CR in VCA recipients. There have been graft losses in the first year with almost exclusive involvement of the vessels. There have been multiple losses many years after transplantation with acute ischemia with and without significant skin changes. And there are patients with moderate to severe skin involvement with relative sparing of the vessels. Using a CR3 category for these diverse populations may not be informative or predictive of eventual outcomes.
Future directions include refining the questionnaire and accumulating more data that can be used to address the concerns raised by the CRWG and the attendees of the ASRT breakout session. The CRWG will continue to meet and progress made will be presented annually alternating between the ISVCA and the ASRT meetings as they both occur biennially. Some of the goals we hope to achieve are the inclusion of data from as many centers as possible and the ongoing refinement of the proposed working definition. Another major goal is to extend these criteria to other types of VCA, such as abdominal wall and urogenital transplants. In addition, while uterine transplants are not intended for long-term engraftment, chronic changes while the recipient is not in the relatively protected state of pregnancy may be clinically important and could also help us understand the mechanisms of CR in other types of VCA grafts.
In summary, it is clear that the vision of the presidents of the ASRT and ISVCA to create intersociety working groups to address key areas to advance the field of VCA has been realized. In order to move the field of VCA forward and take advantage of what can be learned from every single VCA recipient, we must work together and share our data. The field has matured to the point that a more complete definition may now be possible. The working group is pleased to present our progress and data collected as a genuine step toward that goal. The overall message is that this project is underway, and collaboration and input are welcome and encouraged. Plans for the further collaborative projects will be presented at future ASRT and ISVCA meetings.
Footnotes
Acknowledgements
The authors acknowledge and thank the following teams and centers that contributed VCA outcome data to this working group: the Lyon VCA Program, Brigham and Women’s Hospital, Johns Hopkins University, the University of Louisville VCA Program, the Innsbruck VCA Program, UCLA, and the Mayo Clinic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.