
Abstract
Objectives:
To evaluate vibrotactile sense in an older group of people with normal glucose tolerance and type 2 diabetes relative to other sensory tests.
Methods:
Vibration perception thresholds on the sole of the foot (Multifrequency vibrametry and Biothesiometer) were compared to the results from evaluation of touch (monofilament), electrophysiology (sural nerve) and thermal sensation (Thermotest®).
Results:
Vibration perception and temperature thresholds, as well as sural nerve function, differed between normal glucose tolerance and type 2 diabetes. Measuring vibration perception thresholds at lower frequencies with multifrequency vibrametry versus biothesiometer provided correlations similar to sural nerve amplitude. Temperature thresholds correlated with vibration perception thresholds and sural nerve function. Monofilaments revealed pathology in only a few participants with type 2 diabetes.
Conclusions:
In an older group of people, vibration perception thresholds show a correlation similar to sural nerve amplitude on tactile and non-tactile surfaces. Measuring a vibration perception threshold on a tactile surface in type 2 diabetes provides no clear advantage over measuring it on the medial malleolus. In older type 2 diabetes subjects, both large and small diameter nerve fibers are affected.
Keywords
Introduction
Vibrotactile perception on tactile surfaces on the feet is important for somatic function1,2 and may be affected early on in various neuropathies. 3 Peripheral neuropathy is a well-known long-term complication, occurring in up to 50% of people with type 2 diabetes (T2DM).4,5 Symptoms of neuropathy are often already present at the time of diagnosis.4,6–9 Combined with reduced blood flow, neuropathy in the feet promotes risk of foot ulcers, infection, and at times even the need for limb amputation.10,11 Loss of sensation and reduced balance can lead to an increased risk of falls and tissue injury. 10 More than a third of those with T2DM and diabetic sensory-motor polyneuropathy develop neuropathic pain, which significantly impairs their quality of life. 4 In Sweden, annual screening is recommended to detect retinopathy and neuropathy in people with T2DM 12 and is efficient in terms of the health economy.13–16 Neuropathy is examined using monofilaments and a vibrating tuning fork. However, the sensitivity of the screening examination is low and will only screen out those with a manifest, painful neuropathy. 17 At an early stage, neuropathy may be reversible and with a more sensitive instrument for screening early detection18–20 could reduce the risk of complications. Invasive methods, such as electrophysiological assessment, can detect neuropathy even in the pre-diabetic stage, for example., when glucose tolerance is impaired.18,21 A simple and non-invasive method for a more sensitive everyday clinical diagnosis of peripheral neuropathy is called for.
Vibrotactile perception depends on the function of Pacinian corpuscles, responding to frequencies >80 Hz (in particular at 250 Hz) 22 and on Meissner’s corpuscles, which are most sensitive at 30 Hz.23,24 Evaluation of vibration perception thresholds (VPTs) at different frequencies, reflecting dysfunction in subsets of receptors and their connected axons, may be a useful tool for detecting early signs of peripheral neuropathy. In clinical practice, vibrotactile perception to detect neuropathy25,26 is traditionally investigated by means of bone contact through the skin, at the pre-tibia, at the medial malleolus, and at the big toe at an arbitrarily pragmatic frequency of 128 Hz. However, it may be more appropriate to examine tactile surfaces with respect to function.26–28 For example, disturbed vibrotactile perception in finger pulps has been reported in vibration-induced neuropathy and in carpal tunnel syndrome.3,29 Vibrotactile perception in the foot at different frequencies in a population with T2DM had not previously been examined and compared to normative data in people with normal glucose tolerance (NGT), 28 but recently it has been reported in children with type 1 diabetes, showing early signs of neuropathy. 30 Thus, our aim was, in an older group of people with NGT and T2DM, to evaluate VPTs on tactile surfaces on the sole of the foot bilaterally and to compare them with techniques previously used to evaluate sensory nerve function.
Materials and methods
Examinations were performed as part of a 10-year follow-up of a cohort originally from the population-based Västerbotten Intervention Program (VIP), 31 with participants recruited between November 2004 and April 2007; the original study population has been described elsewhere. 32 The study is defined as a case-control study, although it is a part of a long-term follow-up of a specific cohort (i.e. part of a cohort study or prospective observational study). All participants provided written informed consent and the Regional Ethical Review Board of Umeå University, Umeå, Sweden approved the study (ethical application no. Dnr 2013-21-31M). The original study was based on a certain number of participants who were recruited consecutively from the intervention program, that is, the VIP, comprising subjects with normal (n = 39), impaired (n = 29), and diabetic (n = 51) glucose tolerance, respectively, matched for age and sex. The intention was to study large and small nerve fiber function (i.e. electrophysiology and intraepidermal nerve fiber density). 32 That number of patients was considered sufficient to study such nerve functions in the original study. At the 2014 follow-up, 6 of the original 119 participants were deceased, and 26 declined further participation. The remaining 87 participants with 36, 9, and 42 participants in the NGT, IGT, and T2DM categories, respectively, underwent an examination of vibratory perception thresholds (VPTs). This was considered appropriate although no conventional power analysis was performed. The impaired glucose tolerance group was excluded from further analyses because of the small sample size. Thus, 78 participants were analyzed (Table 1). The glycemic status of individuals with NGT and IGT was verified by means of two standardized oral glucose tolerance tests (OGTT).33,34 NGT was defined as a capillary fasting plasma glucose <6.1 mmol/L and a 2-h plasma glucose <7.8 mmol/L; IGT as fasting plasma glucose <7.0 mmol/L and a 2-h plasma glucose ⩾7.8 and <11.1 mmol/L. Finally, T2DM was defined as a fasting plasma glucose level of ⩾7.0 mmol/L and/or a 2-h plasma glucose ⩾11.1 mmol/L as defined by the 1999 WHO criteria.33,34 The glomerular filtration rate was calculated according to the Cockroft-Gault formula where creatinine clearance = (((140 − age) × mass (kg) × constant) / serum creatinine (in µmol/L)). The constant is 1.23 for men and 1.04 for women.
Baseline characteristics of the study population. Participants with normal glucose tolerance (NGT) and type 2 diabetes (T2DM).
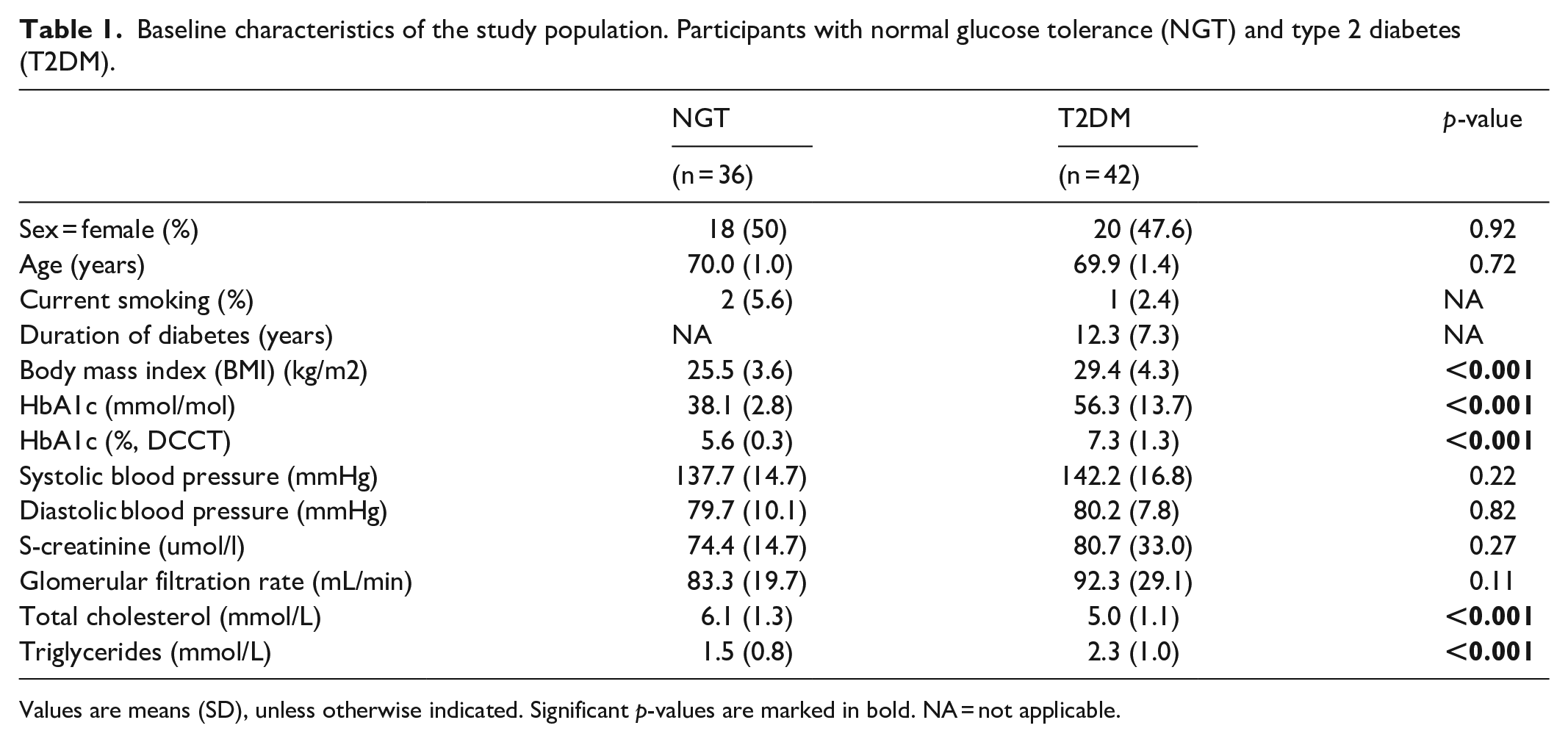
Values are means (SD), unless otherwise indicated. Significant p-values are marked in bold. NA = not applicable.
Examination methods
Electrophysiological assessment
An experienced neurophysiologist, blinded to group identity for all participants, performed a standardized nerve conduction assessment at the clinical neurophysiology laboratory at Umeå University, Sweden. All measurements were conducted on the right leg and included the amplitude and conduction velocity of the sural nerve. 17 The conduction velocity of the peroneal nerve was also measured but was not analyzed further as it contains a larger proportion of motor neurons than the sural nerve, which was thus deemed the most appropriate target for evaluation of sensory nerve function.
Vibration perception thresholds
VPTs were measured using two different methods: (1) VibroSense Meter and (2) biothesiometer.
Using a VibroSense Meter, VPTs were measured bilaterally on the sole of the foot at two different locations, that is., the pulp of the first and fifth metatarsal heads. 30 The sites were selected to mirror the function of the median plantar branch of the tibial (first metatarsal head) and the lateral plantar branch of the tibial (fifth metatarsal head) nerve. Measurements were performed using a modified VibroSense Meter adapted for measurements taken on the feet. 35 The thresholds were measured at four frequencies (8, 16, 32, and 125 Hz) on each site. The foot VibroSense Meter comprised a modified hand device with an extended vibrating probe and a special footplate with a hole, which was placed over the modified device as described elsewhere (for details, see Ising et al. 30 and Dahlin et al. 35 ) The measuring procedure for the foot was identical to the previously reported examination of the fingers; that is., according to ISO13091–1. 35 The examination sequence on the sole of the foot was (1) first metatarsal head and (2) fifth metatarsal head. The examination time was approximately 3 min/site; that is., in total 6 min/foot. Prior to the examination, the temperature at each investigated extremity was measured with the internal temperature probe on the VibroSense Meter. This is standard procedure to ensure that the VibroSense Meter device secures an appropriate interval of 27°–35° Celsius according to ISO 13091–1.36–38 The room temperature was between 20°–22°C (requirement according to ISO 13091–1).
Using a hand-held biothesiometer (Bio-Medical Instrument Co, ROVA Company Inc, Newbury, OH), VPT was tested according to a previously described procedure. 17 The VPTs, using the biothesiometer, were measured bilaterally at the medial malleolus and at the distal dorsal bony surface of both big toes.
The unit of measurement is decibels (dB).
Monofilament
The pressure/touch sensation was examined bilaterally on the sole of the foot using a Semmes-Weinstein 10 g monofilament (Gertab AB, Stockholm, Sweden) at three standard sites; that is., the plantar surface of the distal hallux and the 1st and 5th metatarsal heads. 39 A pathological monofilament test result was defined as the absence of sensation at one or more sites on either foot.17,40
Thermal testing
Thermal sensory testing was performed according to the method of limits using Thermotest® equipment (Somedic AB, Hörby, Sweden) as previously described. 17 The limb temperature was kept above 31 °C.
Statistical analysis
Participant characteristics in the NGT group and the T2DM group were described in terms of counts and proportions for categorical variables and means and standard deviations for quantitative variables. Chi-square tests and Student’s t-tests were used to test for statistically significant differences in characteristics between the NGT and T2D groups.
All measurements of sensory perception were summarized using means and standard deviations. Statistical differences between the left and the right side of the body regarding sensory perception were explored by studying standardized differences in means, that is., t-values from paired Student’s t-tests samples. Differences in means between the NGT and T2D groups were studied using t-values from independent Student’s t-tests samples. Standardized differences allow for comparisons of the different methods for studying sensory perception. All tests were two-sided and the significance level was set to 5% for all the analyses, that is., a t-value of approximately 2. Spearman’s correlations were calculated between all sensory measurements stratified by NGT and T2D groups. The statistical analyses were performed using R 3.4.3 (R Core Team 41 ) and the package “corrplot.” 42
Results
Demographics of participants
The characteristics of the participants are presented in Table 1. Out of the 78 participants in the study, 77 completed vibrametry, 78 biothesiometer, 74 electrophysiological assessments (amplitude and conduction velocity of sural nerve), 78 monofilament testing, and 73 thermal testing. For the VibroSense Meter, data were missing for the left MT1, 16 Hz, and left MT5, 125 Hz in one (though not the same) subject. The mean duration of diabetes was 12.3 years in the T2DM group (Table 1). As expected, participants with diabetes had a higher BMI than those with normal glucose tolerance as well as higher HbA1c levels. Serum cholesterol was lower and serum triglycerides were higher among participants with diabetes (Table 1). Monofilament testing was pathological in 4 participants with T2DM but in none of those with normal glucose tolerance.
Vibration perception and thermal thresholds
Vibration perception thresholds were higher with both methods (VibroSense Meter and biothesiometer) on the soles of the feet in participants with T2DM compared to participants with normal glucose tolerance (Table 2, Figure 1). There were no clear within-group differences between the right and left sides of the feet (Table 2, Figure 1). In a similar way, temperature thresholds for both heat and cold were higher among participants with T2DM than participants with normal glucose tolerance. There were no within-group differences between the right and left sides of the feet regarding temperature thresholds (Table 2, Figure 1).
Means and standard deviations for different methods of measuring nerve function in the foot, stratified by group and extremity.

NGT: normal glucose tolerance; T2DM: type 2 diabetes.
N.B. Standardized differences between means of groups and extremities are indicated in Figure 1.
Values are mean and standard deviations. ND = not determined.
MT1 = at first metatarsal head at sole of the foot.
MT5 = at fifth metatarsal head at sole of the foot.

Standardized differences between means of groups and extremities.
Correlations between methods of nerve assessment
Correlations between the vibration perception thresholds and amplitude of sural nerve were generally higher in the participants with diabetes than in those with normal glucose tolerance, who had correlations close to zero (Figure 2). There were similar correlations between the amplitude of the sural nerve and vibration perception thresholds, at all frequencies.

Correlations (Spearman) between different methods for the examination of peripheral nerve function in the foot. The units of measurement for the methods displayed are the same as in Table 2.
In the present study, in participants with T2DM there was a tendency for the biothesiometer to have a slightly higher correlation to the sural nerve amplitude than the multifrequency vibrametry, but in the normal glucose tolerance group, the correlations were close to zero. Using a biothesiometer, there were similar correlations between the amplitude and vibration perception at both locations of testing, that is., the medial malleolus and big toe. Multifrequency vibrametry had a tendency to correlate more strongly to the amplitude of the sural nerve at the medial plantar examination site (MT1 > MT5).
The correlations between the amplitude of the sural nerve and temperature thresholds were similar to the correlations between sural nerve amplitude and vibration perception thresholds. There were similar correlations between the amplitude of the sural nerve and laterality (i.e. the right and left extremity) concerning both vibration perception thresholds and thermal thresholds. The correlation was generally weak between the conduction velocity of the sural nerve and both vibration perception and thermal thresholds (Figure 2).
Discussion
The present study shows that vibration perception and temperature thresholds on the sole of the foot are different in this older group of people with NGT and long-standing T2DM. Measuring vibration perception thresholds at lower frequencies, compared to the current standard of 128 Hz, provided correlations similar to the amplitude of the sural nerve. Evaluating vibration sense on a tactile area provided a similar correlation to the amplitude of the sural nerve, as compared to a non-tactile area, such as the medial malleolus.
Peripheral neuropathy is one of many potential multi-factorial complications in T2DM. 43 In combination with reduced blood flow, neuropathy in the feet increases the risk of foot ulcers, infection, and sometimes even the need for limb amputation. 11 Early detection of disturbed sensory perception in T2DM is important for the avoidance of further complications.19,20,44 During the early stages of T2DM, the plasticity of the nervous system remains, and metabolic corrections have the potential to reverse the symptoms.20,45 In the present study, with a case-control design and long follow-up of the participants, we used a variety of methods to detect neuropathy. Vibration sense, detected by two different methods, was evaluated in an age-matched sample of older individuals with NGT and T2DM. Most previous studies used the biothesiometer, applied at a single frequency (128 Hz) to non-tactile surfaces, to detect vibrotactile perception. 17 This may seem a strange site at which to assess peripheral sensory perception, as a tactile sensation on the sole of the foot or on the glabrous skin in the hand, which may even differ with respect to firing characteristics in response to vibration stimuli, 46 is considered to be more relevant for the functioning of the lower extremity and the hand, respectively. Together with poorer balance at higher ages, a reduced tactile sensation increases the risk of falls. 10 This is also relevant in view of the fact of the interaction described between vibrotactile sense and proprioception at the ankle joint 47 since the sole of the foot is considered a sensory structure. 46 This suggests that measuring peripheral sensory perception on a tactile surface may be more relevant than measuring it on a non-tactile surface area. However, the present study indicates that measuring the vibration sense using the two techniques on a tactile or non-tactile area produced a correlation similar to the amplitude of the sural nerve and thus a correlation similar to a gold standard method for revealing neuropathy. Measuring vibration perception thresholds at lower frequencies than the current standard of 128 Hz provides no clear advantage, judging by the correlation to the amplitude of the sural nerve in the present study in older people with long-standing and well-controlled T2DM. The current practice of measuring vibration perception on the bony surface of the medial malleolus seems to be as fair an approximation to the amplitude of the sural nerve as measuring vibration perception on the tactile surface of the foot, indicating a loss of myelinated nerve fibers. Furthermore, temperature thresholds had similar correlations to sural nerve amplitude as vibration perception thresholds, indicating involvement to a similar degree of both myelinated and non-myelinated nerve fibers. Thus, in older people with long-standing and well-controlled T2DM, large and small diameter nerve fibers seem to be affected equally. In contrast, the correlation was generally weak between the conduction velocity of the sural nerve and both vibration perception and thermal thresholds. This is probably due to the fact that demyelination of nerves is less apparent than the loss of nerve fibers in the early stages of neuropathy. 18 Previous results suggest an association between blood glucose level and the severity of peripheral neuropathy, measured as amplitude of the sural nerve. 18 Thus, finding and evaluating sensitive methods for detecting a reduced function of various nerve fibers in peripheral nerves is an important task. As expected, there were differences between participants with NGT and those with T2DM. VPTs in men and women are affected differently by diabetes with males with diabetes 48 having a higher risk of neuropathy. No analysis of gender differences was possible in the present study due to the limited number of participants.
At present, monofilament testing, using the 10-gram monofilament, and vibration perception thresholds, measured with a 128 Hz tuning fork, is used in the routine clinical setting in Sweden. 40 Lack of sensation measured with monofilaments and vibration techniques has high specificity, but the sensitivity is quite low.40,49 Accordingly, the 10-gram monofilament test indicated very few of the pathological values in the present study. This is in accordance with a recent study by Rinkel et al. 50 in which loss of sensation in patients with diabetes could be graded. Interestingly, static and moving two-point discrimination tests (i.e. 2-PD) seem to be sensitive in detecting loss of sensation, followed by a test of vibration sense (i.e. Rydel-Seifer tuning fork at medial malleolus and dorsal on the interphalangeal joint of the big toe), the 10-g monofilament and the ability to feel the cold stimulus. 50 However, the authors included both somewhat younger (median age 64 years) male and female patients (but more males) with types 1 (22%) and 2 (78%) diabetes, who varied regarding previous foot ulcers and amputations as well as the duration of diabetes (median 16 years). This should be taken into consideration as being slightly different from our cohort (Table 1). Nevertheless, the analysis of the vibration sense was better than when the 10 g monofilament test was used to reveal dysfunction. We did not include 2-PD in our study since that method in evaluating the diabetic foot is not clinically routine in our country, despite the results presented by Rinkel et al.50,51 However, 2-PD is frequently used to measure nerve function in fingers after nerve injury and repair, even with its inherent extensive limitations and variability. 52 Electrophysiology, a more challenging method, does not reflect all types of nerve dysfunction and therefore a battery of tests is recommended for clinical detection of distal symmetrical diabetic neuropathy. 51
The strength of the present study is that both older people with T2DM and age- and gender-matched subjects were examined. This is relevant since vibration perception thresholds are age-dependent and appropriate cut-off values for judging and distinguishing between pathological and non-pathological values vary across age categories. 30 Sensory perception in the foot was measured using different methods and at different sites on the lower extremities and vibration perception thresholds were measured using two different methods. The temperature of the foot was carefully measured before the examination, as this influences vibrotactile perception. One limitation of the study is that the vibration threshold at each site was only measured once with each method in each participant. However, good test–retest reliability has been shown for VPTs, which reduces the need for repeated measurements. 53 It is also less likely that repeated measurements would influence results and conclusions because of the number of participants. A further limitation is that a conventional sample size calculation was not done in the present follow-up since we only were able to include available subjects. In the original examined cohort, 54 a rough estimation of the probability to find a sufficient number of subjects with neuropathy among T2DM subjects was made based on previous assumptions and studies.1,18,54
Conclusions
Vibration perception and temperature thresholds on the sole of the foot are different in an older group of people with NGT and long-standing well-controlled T2DM. Measuring vibration perception thresholds at lower frequencies compared to the current standard of 128 Hz, or evaluating vibration sense on a tactile area compared to a non-tactile area, provided correlations similar to the amplitude of the sural nerve. Thus, measuring vibration perception thresholds at a tactile surface did not, in the present study with an older population, seem to provide any clear advantage over the traditional way of measuring the vibration perception threshold at 128 Hz on the medial malleolus. In older people with neuropathy due to long-standing T2DM, large (myelinated) and small (non-myelinated) diameter nerve fibers seem to be equally affected.
Footnotes
Acknowledgements
Our sincerest gratitude to Dr. Sigbritt Rasmark, RN Karin Nilsson, and biomedical scientist Anette Broberg for their skillful assessment of the participants. We would like to thank Tony Speidel, Vibrosense Dynamics, for help with technical issues. We are indebted to the late Professor Göran Sundqvist, who was one of the initiators of the study. We would also like to thank all the participants who made this study possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the regional ethical review board of Umeå University, Umeå, Sweden (ethical approval no. Dnr 2013-21-31M).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grants from Västerbotten County Council, and Umeå University, Sweden (to O.R.), funds from Skåne University Hospital, Lund University, the Diabetes Association in Malmö and the Swedish Diabetes Foundation (to L.D.). The funders played no part in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Informed consent
Written informed consent was obtained from all subjects before the study.