
Abstract
Objectives:
Fever control has been shown to reduce short-term mortality in patients with septic shock. This study aimed to explore the feasibility of early intensive fever control in patients with septic shock and to assess the immunomodulatory effects of this intervention.
Methods:
In this single-center, randomized, open-label trial, febrile patients with septic shock presenting to the emergency department were assigned to either a standard fever control or therapeutic normothermia group. Therapeutic normothermia involved intensive fever control in maintaining normothermia below 37°C. The primary outcome was the feasibility of fever control for 24 h. Secondary outcomes included changes in immunomodulatory biomarkers and adverse events.
Results:
Fifteen patients were enrolled and analyzed. Fever control was comparable in both groups, but significantly more patients in the therapeutic normothermia group experienced shivering (p = 0.007). Both groups demonstrated increased C-reactive protein and unchanged neutrophil chemotaxis and CD11b expression. The therapeutic normothermia group revealed significant decreased IL-6 and IL-10. The standard fever control group significantly expressed increased monocytic human leukocyte antigen. There were no significant differences between the groups in terms of immunomodulation.
Conclusions:
Therapeutic normothermia was feasible in patients with febrile septic shock but was not superior to standard fever control in terms of average body temperature and host defense function. Shivering was more frequent in the therapeutic normothermia group.
Trial registration:
Thai Clinical Trials Registry number: TCTR20160321001
Introduction
Septic shock has potentially devastating outcomes, including organ failure and death. Despite recent improvements in our understanding of sepsis, mortality due to septic shock remains high, even in clinical trial settings.1–3 There is thus an urgent need for effective interventions to help improve the clinical outcome of patients with septic shock.
A few clinical trials have reported a benefit of controlling fever in patients with septic shock. Applying an external cooling device to patients with septic shock to maintain normothermia for 48 h in an intensive care setting decreased vasopressor requirements and early mortality. 4 In the largest clinical trial to date assessing fever control in critically ill patients, acetaminophen administration tended to decrease early mortality compared with placebo, 5 although the exact mechanism responsible for this superior outcome has not yet been elucidated. One plausible explanation is that it might be due to changes in the immune response, given that temperature regulation has demonstrated a strong association with immunity. 6 Indeed, the immune system is considered to be core pathophysiology in sepsis.7,8
Fever can be relieved using pharmacological or nonpharmacological methods, of which the latter includes administration of a cool intravenous fluid or external cooling device. However, aggressive fever control involving the use of an external cooling device has mostly been initiated in an intensive care setting, and the feasibility of administering early intensive fever control to decrease the temperature of patients with early septic shock in the emergency department and its effect on immunomodulation remain unknown.
This research therefore aimed to determine the feasibility of early intensive fever control compared with standard fever control (SFC) in patients with septic shock and to examine the immunomodulatory effects and clinical outcomes of this treatment.
Materials and methods
Trial design
We conducted an open-label, randomized controlled trial in an urban emergency department with high acuity (Emergency severity index of 1–3) with a census of 40,000 visits per year in a 1400-bed tertiary care center at King Chulalongkorn Memorial Hospital, Bangkok, Thailand. The trial was registered in the Thai Clinical Trials Registry (TCTR20160321001). The research was approved by the Institutional Review Board, Faculty of Medicine, Chulalongkorn University (IRB No. 580/58). This trial is reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.
Patients
All adult patients (aged ⩾ 18 years) who presented to the emergency department between May 2016 and May 2017 were screened in the triage area. The screening was limited to patients presenting during business hours (Monday to Friday, 8 a.m. to 4 p.m.) because of laboratory availability. We included patients who were diagnosed with sepsis and fever, and with evidence of hypoperfusion or refractory hypotension. During the recruitment period, sepsis was defined as probable or documented infection with systemic manifestations of infection. 9 Hypoperfusion was defined as a serum lactate level >4 mmol/L. Refractory hypotension was defined as systolic blood pressure (SBP) < 90 mmHg after administration of 1 L of fluid, or a need for vasopressors to maintain SBP of >90 mmHg. Fever was defined as a screening axillary or oral temperature >37.8 or 38.3°C, respectively. We excluded patients who were moribund, terminally ill with a Do-Not-Attempt-Resuscitation (DNAR) order, had suspected sepsis due to microorganisms other than bacteria, were immunosuppressed, transferred from another hospital, diagnosed with sepsis for >12 h, or had suspected concomitant acute brain injury.
Randomization and procedures
Information on eligible patients was provided by trained research associates, and written informed consent was obtained from the patients or their legal representatives. Participants were randomized into two groups in a 1:1 ratio by block randomization with varying block sizes (2, 4, or 6), generated by a web-based program and prepared by an investigator with no clinical involvement in the trial. The allocation sequences were placed in sequentially numbered, sealed, opaque envelopes. After obtaining informed consent, the research associate opened the appropriate numbered envelope and assigned the patient to either a therapeutic normothermia (TN) group or SFC group. All patients received standard treatment for septic shock, including early and aggressive fluid resuscitation, early appropriate antibiotic administration, source control, and a mean arterial pressure target of 65 mmHg. The temperature was measured rectally, monitored continuously, and recorded every 4 h in both groups.
Interventions
Body temperature in the TN group was controlled at around 36–37°C for 24 h using cool intravenous fluid and a cool blanket (Blanketrol II, Cincinnati Sub-Zero, OH, USA). The cool intravenous fluid was either 0.9% NaCl solution or lactated Ringer’s solution, maintained at 4°C and administered at a rate determined by the physician, according to the patient’s hemodynamics. Patients were monitored for shivering and treated according to the adapted three-step Columbia antishivering protocol as follows: 10 step 1, oral acetaminophen (500–1000 mg) every 4–6 h and intravenous magnesium sulfate (0.5–1 mg/h) for 4 h; step 2, mild sedation by intramuscular or intravenous meperidine (50–100 mg) or fentanyl (25 µg/h); and step 3, moderate sedation.
The intervention was initiated as soon as possible in the emergency department or the inpatient unit. If the intervention was started in the emergency department, the blanket was disconnected temporarily during transfer to the inpatient unit and reconnected when the patient arrived at the new unit. The TN protocol was continued for 24 h and then stopped.
SFC involved administration of acetaminophen 500–1000 mg every 6 h for 24 h when the patient’s temperature exceeded 39.5°C.
After the respective intervention, the decision on whether or not to control the patient’s temperature was made by the responsible clinicians.
Outcome measures
The primary outcome was the feasibility of fever control, defined as control of temperature at <37.5°C for more than 80% of the intervention period. This goal was chosen as the period during which the patient was without fever in the 24-h intervention period.
The secondary outcomes were the difference in temperature between the groups during the intervention period, and changes in levels of CD11b, neutrophil chemotaxis, interleukin (IL)-6, IL-10, C-reactive protein (CRP), and monocytic human leukocyte antigen (mHLA-DR) at 24 h after intervention. Adverse events during the intervention were defined as shivering, episodes of hypothermia (temperature < 36°C), new arrhythmia, and intractable hyperglycemia. We also recorded the number of protocol violations.
Biomarker assays
Blood samples were drawn and enriched for polymorphonuclear neutrophils (PMNs) and mononuclear cells in the laboratory within a 4-h time frame. The cells were extracted by one-step centrifugation with PolymorphPrep (Alere Technologies AS, Norway), containing sodium diatrizoate and an 8% (w/v) polysaccharide solution (AxisShield, Norway) for 30 min at 500×g (1700–1800 r/min). The monocyte and PMN layer were then removed and washed with RPMI 1640 by centrifugation at 800×g for 5 min to remove residual PolymorphPrep. The cell pellet was then resuspended in ammonium chloride lysis buffer (9:1 ratio) with RPMI 1640 for 3 min to remove contaminating red cells. The cells were pelleted at 800×g for 5 min and resuspended in RPMI 1640 supplemented with 5%–10% (v/v) human AB serum (or fetal bovine serum).
The proportions of CD11b- and mHLA-DR-positive PMNs were determined by flow cytometry. Monocytes and neutrophils were collected and incubated with allophycocyanin-conjugated CD11b (IgG1; Beckman Coulter, France) and with phycoerythrin-conjugated HLA-DR (IgG1; Beckman Coulter) for 30 min, respectively. The samples were then washed twice in phosphate-buffered saline without magnesium or calcium and fixed with 4% paraformaldehyde. All samples were applied to a flow cytometer (BD LSR II; BD Biosciences, CA, USA) using acquisition and analysis software (BD FACSDiva; BD Biosciences).
PMN chemotaxis was assayed using Hanging Millicell inserts (Merck Millipore, Germany). Tissue culture plates with 24 wells were coated with poly(2-hydroxyethyl methacrylate) to prevent cell adhesion following transmigration and 800 μL RPMI 1640 with chemoattractant (10− 9 mol/L formyl methionyl-phenylalanine) was then added to each well. Hanging inserts with a 3-μm pore-size filter at their base and 1 × 106 neutrophils in 200 μL of culture medium were then added into the hanging inserts and incubated in a 5% CO2 incubator for 90 min at 37°C. The hanging inserts were then removed and the migrated neutrophils in each well were counted. The number of migrated neutrophils was calculated as a percentage of the total number of cells initially added.
Plasma IL-6 and IL-10 levels were measured using commercial enzyme-linked immunosorbent assay kits (R&D Systems, MN, USA), and serum CRP concentration was measured by nephelometry.
Sample size determination
According to the feasibility outcome, a total sample size of at least 46 patients was needed to detect a 40% difference between the groups in the ability to control fever for > 80% of the time, considering a two-sided alpha level of 0.05 and a power of 80%.
Statistical analysis
Numerical data with a normal distribution are reported as the mean ± 1 standard deviation (SD), and non-normally distributed data are reported as the median and interquartile range (IQR). All analyses were conducted on an intention-to-treat basis. The primary outcome was compared between groups using Fisher’s exact test. Differences in temperature and changes in immunomodulation markers between the groups were compared using an independent sample t-test. Changes in markers within each group were assessed using a dependent sample t-test. Adverse events were compared using Fisher’s exact test. Statistical significance was accepted at the p < 0.05 level. The analysis was performed using Stata 14.0 software. The statistician was blinded to the group allocation and the hypothesis of the study.
Results
Baseline characteristics
A total of 65 patients were screened for eligibility from May 2016 to May 2017. Forty-six patients met the exclusion criteria, and one did not provide consent. Eighteen patients were therefore randomized equally between the TN and SFC groups. Three patients were excluded from the analysis, including one with neutropenia and one who was transferred to another hospital in the TN group, and one patient in the SFC group who developed cardiac arrest and acute brain injury after randomization but before the beginning of the intervention (Figure 1). Regarding the baseline characteristics, patients in the SFC group were generally older and had more underlying diseases, higher severity scores, and a shorter time from the start of the intervention until the administration of antibiotics (Table 1). Recruitment was stopped after 1 year due to the slow recruitment rate and the presence of significant adverse effects in the intervention group.

Screening and enrollment of study participants. DNAR: Do-not-attempt-resuscitation.
Baseline patient characteristics.

APACHE: acute physiology and chronic health evaluation; Cr: creatinine; ESI: emergency severity index; SFC: standard fever control;OFA: sequential organ failure assessment;; TN: therapeutic normothermia; WBC: white blood cell.
Data are presented as amean ± 1 SD, bnumber, or cmedian (IQR).
Fever control protocol
During the 24-h intervention, two participants in the SFC group received acetaminophen to control fever >39.5 C, compared with all participants in the TN group. There were no protocol violations in the SFC group but two violations (28.6%) in the TN group, with early termination of the protocol. One protocol violation was at the physician’s request after the patient developed shivering and new, rapid atrial fibrillation, and the other at the patient’s request because they felt cold.
Primary outcome
During the 24-h intervention period, 71.4% of subjects in the TN group maintained their temperature at <37.5°C for >80% at the time, compared with only 50% in the SFC group. However, this difference was not significant (p = 0.61).
Secondary outcomes
Patients in the TN group could decrease and maintain their average body temperature at 37°C, while those in the SFC group had an average temperature of 37.2°C; however, there was no significant difference in temperature between the two groups (p = 0.56) (Figure 2).

Average body temperature during the 24-h intervention period. Data are presented as the mean, and one-sided error bars represent the SD.
There were no significant differences between the groups regarding immunomodulation effects during the 24-h period (Figure 3). Both groups revealed increased CRP over time (TN group: +105.6 ± 93.37 mg/L, p = 0.02; SFC group: +64.66 ± 74.99, p = 0.04). The TN group exhibited significantly decreased level of IL-6 and IL-10 (−429.65 ± 373.89 pg/ml, p = 0.02; −174.92 ± 125.59, p = 0.01, respectively), while the SFC group demonstrated increased monocytic human leukocyte antigen expression (+9.99 ± 9.13, p = 0.02). There were no significant changes in neutrophil chemotaxis and CD11b expression in both the groups.
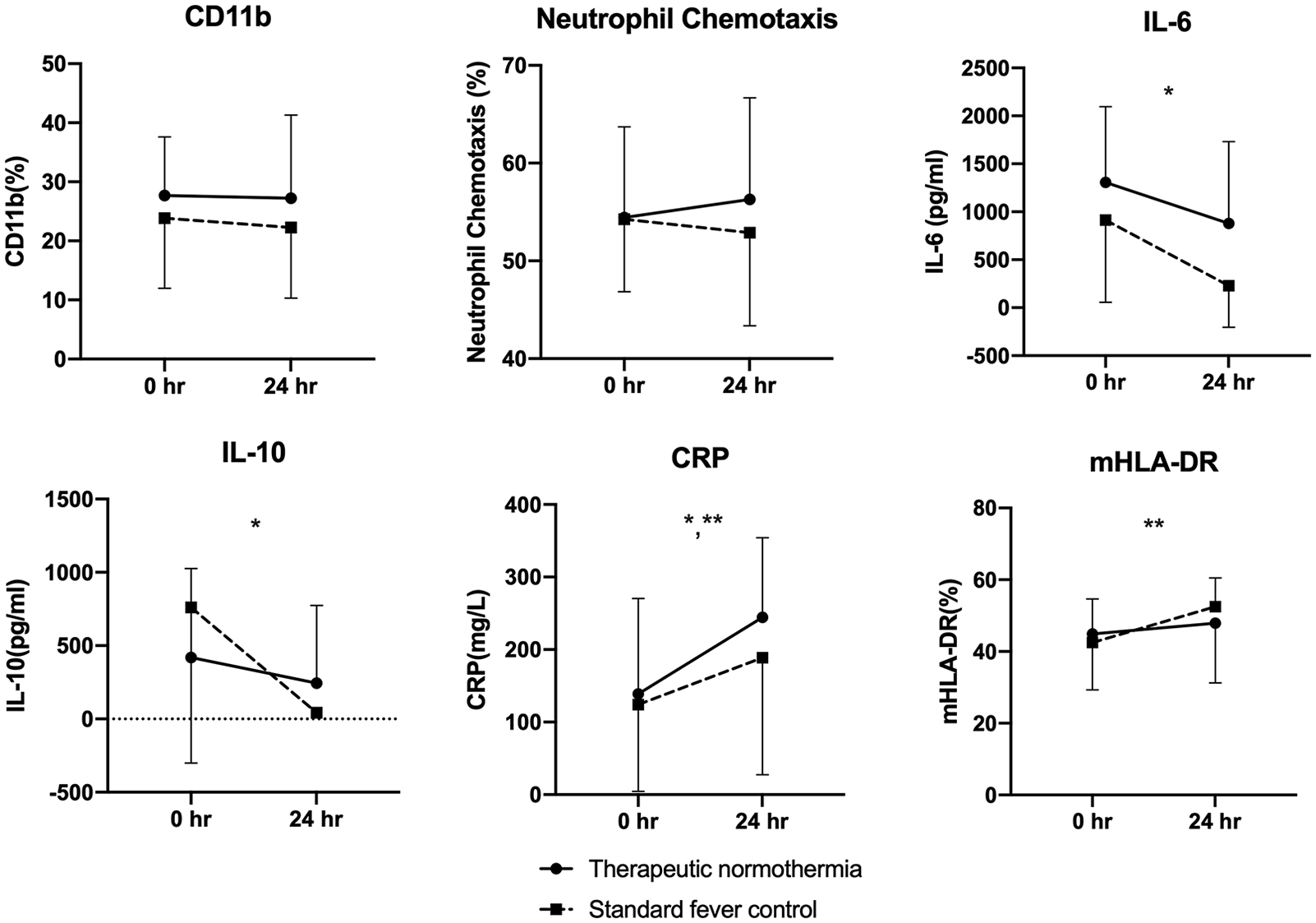
Changes in biomarkers at baseline and 24 h since the onset of the intervention. Data are presented as the mean, and one-sided error bars represent the SD. There were no significant differences in any of the biomarkers between the two groups. *p < 0.05 within the therapeutic normothermia and **standard fever control groups.
Adverse events
Shivering was significantly more common in the TN compared with the control group (5/7 versus 0/8, p = 0.007) (Table 2), but there were no significant differences in any other adverse outcomes.
Adverse events.
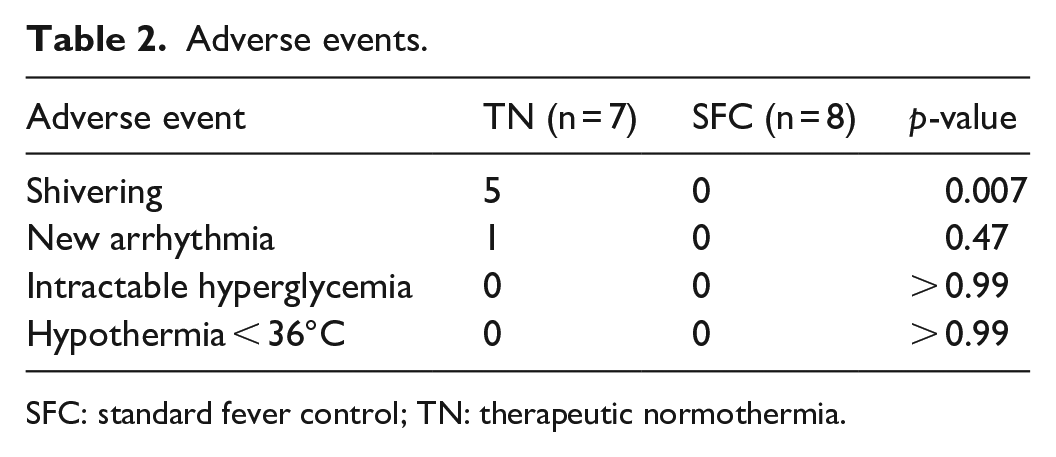
SFC: standard fever control; TN: therapeutic normothermia.
Discussion
Controlling fever has been shown to be beneficial in patients with septic shock in intensive care settings. We therefore aimed to explore the feasibility of initiating early aggressive fever control as soon as the patient enters the emergency department. TN was feasible and resulted in more effective temperature control than the SFC protocol, though the difference was not significant because of the limited sample size. Comparable changes in immunomodulatory effects over time occurred in both groups; however, the TN protocol was associated with more shivering and early protocol termination.
Fever, if naturally occurring in infected patients, was associated with better outcomes. An early peak temperature during the first 24 h in the intensive care unit was associated with decreased mortality in critically ill patients with infection. 11 Moreover, increased mortality was found in septic patients with hypothermia. 12 Fever represented a promotion of host resistance in physiologically fit patients, while hypothermia served as an adaptation to increase host tolerance in those without physiological fitness, as in the critically ill patients. 13 The value of controlling fever in septic patients, however, has long been debated. A prospective observational study also showed that the pharmacologic treatment of fever was independently associated with increased 28-day mortality. 14 In contrast, clinical trials in an intensive care setting found that controlling the body temperature to normothermia resulted in decreased early mortality and vasopressor requirements.4,5 Nevertheless, another study indicated that lowering the temperature to hypothermic levels in septic patients might be harmful. 15
The current study found no advantage of using the TN protocol to lower the body temperature compared with SFC. This may have been primarily because of the significantly greater level of shivering in the TN group. Shivering has adverse effects by not only decreasing the chance of successful temperature control but also increasing oxygen demand.16,17 The stepwise administration of acetaminophen and magnesium, sedation with opioids and the use of a muscle relaxant is a known effective protocol for controlling shivering. 10 However, these final steps are limited to intubated patients, which did not include most patients in the current study and does not generally represent the majority of patients with early septic shock in the emergency department. Moreover, shivering occurred in the TN group even though there were no hypothermic episodes. The hypothalamic cutoff point for regulating body temperature is higher than normal in febrile individuals. Lowering the temperature below this cutoff point can thus cause shivering, even if the body temperature is within the normothermic range. 18 In addition, the body temperature remained lower than the initial temperature in the SFC group during the first 24-h period, despite no aggressive fever control, which could partly be explained by the effect of temperature lowering induced by fluid resuscitation. 19
In the current study of fever control in patients with septic shock, patients in both groups showed changes in immunomodulation markers over time, regardless of the fever control strategy. Neutrophil chemotaxis and mHLA-DR expression are important biomarkers characterizing immunoparalysis and later secondary infection in septic patients. The neutrophil function was impaired prior to nosocomial infection. 20 Decreasing levels of mHLA-DR are characterized by monocyte unresponsiveness and predict secondary infection and late mortality in sepsis patients. 21 Previous studies showed an association between temperature and these markers, with extreme hyperthermia or hypothermia decreasing neutrophil chemotaxis,22,23 and increased expression of mHLA-DR in the hyperthermic range. 24
The inflammatory markers CD11b, IL-6, IL-10, and CRP were associated with the severity and clinical outcomes of sepsis.25–32 Though no difference was found between group regarding difference fever control strategy, previous studies showed that these markers were associated with temperature. An in vitro study showed that CD11b expression was increased under conditions of hypothermia and hyperthermia, 33 while IL-6 and IL-10 levels were reduced by hypothermia in both animal and human studies,34–37 and CRP levels at 24 h were lower in hypothermic compared with normothermic postcardiac arrest patients. 38
This was the first randomized trial to explore the feasibility of early intensive fever control in patients with septic shock. However, this study had several limitations. The limited number of participants could have led to imbalanced baseline characteristics and inadequate statistical power in terms of both the primary and secondary outcomes. Moreover, limited laboratory availability meant that participants could not be screened or recruited outside business hours, and there could thus have been some discrepancy between the study population and the general population of patients with septic shock. In addition, despite an established protocol to decrease shivering during TN, a high level of shivering still developed and led to early protocol termination in two (28.6%) cases. The apparent nature of the interventions in this trial meant that the subjects and investigators could not be blinded to the group allocation, although potential biases were mitigated by measuring objective outcomes and by blinding of the statistician.
Further studies are needed to explore the effects of intensive fever control, with an emphasis on managing shivering. A future study population could be limited to intubated patients, which would allow aggressive sedation or muscle relaxation to control the level of shivering. Nevertheless, the results of the present study warrant further exploration of the optimal body temperature in patients with septic shock.
Conclusion
Intensive fever control by TN is feasible in febrile patients with septic shock. However, the current, small randomized controlled trial found no significant benefit of TN over SFC in terms of average body temperature and host defense function. Shivering was more frequent in the TN group.
Footnotes
Acknowledgements
The authors would like to thank Pornjira Wongnate, Panadda Chaypradap, and Kanchana Prasith for data management, Sasipha Tachaboon for assistance with laboratory testing, Pimnara Peerawaranun for valuable help with statistical analysis, and all the residents and nurses in the Emergency Medicine and Internal Medicine Departments. They also express gratitude to the participants in this study.
Author note
Nattachai Srisawat is now affiliated to Critical Care Nephrology Research Unit, Chulalongkorn University, Bangkok, Thailand and Academic of Science, Royal Society of Thailand, Bangkok, Thailand.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board, Faculty of Medicine, Chulalongkorn University (IRB No. 580/58).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ratchadaphiseksomphot Endowment Fund of Chulalongkorn University [CU-59-001-HR] and the Ratchadapiseksompotch Fund, Faculty of Medicine, Chulalongkorn University [RA59/040]. The funders had no role in designing or analyzing the results.
Informed consent
Written informed consent was obtained from all subjects or their legally authorized representatives before the study.
Trial registration
Thai Clinical Trials Registry (TCTR20160321001).