
Abstract
Objective:
Treatment of infantile idiopathic scoliosis remains vague. Because implantation of temporary telescopic devices carries a high risk of complications, interest in the older technique of serial casting is growing as a temporising measure before invasive procedures. The goal of this review was to meta-analyse studies examining the effect and safety of casting in infantile idiopathic scoliosis.
Methods:
Two reviewers independently searched for relevant studies in PubMed and Embase databases through November 2018. The studies included were limited to infantile idiopathic scoliosis patients who underwent casting, had a mean Cobb angle of 20 or more and written in English. The methodological quality of the chosen studies was assessed. The primary outcome was the difference in Cobb angle means from before and after casting. The secondary outcome was adverse events of casting. Heterogeneity was explored and a funnel plot was drawn.
Results:
Of the 366 studies screened, 10 studies were included in the meta-analysis (243 subjects) and all were non-randomised. The casting was consistently associated with a reduction in the mean Cobb angle. The pooled mean difference was 24.85° (95% confidence interval: 19.25 to 30.46, p < 0.001). A number of reversible adverse events were reported, most commonly skin irritation and transient pulmonary symptoms. Heterogeneity between studies was high. In the meta-regression analysis, the starting Cobb angle did not influence Cobb angle change, but there was an inverse correlation between the mean difference in Cobb angle and mean age.
Conclusion:
Casting seems to be effective and safe in decreasing Cobb angle even in high curve magnitudes. In older patients, casting showed less Cobb angle correction.
Introduction
The proposed definition of infantile idiopathic scoliosis (IIS), which is typically left thoracic and more common in males, is an idiopathic scoliosis diagnosed before 3 years of age. 1 The term ‘progressive’ is added to IIS to differentiate it from the spontaneously resolving type. Scott and Morgan alluded to the risk of premature death in this category. 2 Casting in the treatment of IIS had early widespread adoption and it was done for patients who cannot conform to the Milwaukee jacket. 3
Mehta described the rib vertebral angle difference of more than 20° and the overlap between the convex-side rib and apical vertebra as indicators of a high probability of progression in infantile scoliosis. 4 She later reported prospective data on 136 patients who underwent elongation-derotation-flexion plaster casting according to Cotrel and Morel.5,6 Thirty-six patients in the cohort were non-idiopathic, and the remaining were termed a sturdy or slender phenotype. A total of 94 patients resolved completely; however, it is impossible to ascertain if the recovery was spontaneous or induced by the cast, but the effect of casting was evident on the remaining 42 who had a partial correction.
For curves that do not respond to bracing or are larger than 50°–70°, Moe used a thick smooth subcutaneous Harrington rod without fusion in addition to an orthosis for IIS, with serial lengthening or replacement every 3–6 months. 7 This evolved to the current state of dual growing rods, which can be magnetically controlled, but still with a high implant-related complication rate, yet only serves as a temporary treatment until near lung and skeletal maturity, when final surgery can be done. 8 Such ‘growth friendly’ instrumentation demonstrates diminishing returns on repeated lengthening, so the efficacy of those implants deteriorates with time making it imperfect as the first line of treatment. 9 The resurgence of interest in serial casting for infantile scoliosis is stimulated by the cost and risk profile of telescopic devices that provide no definitive solution.
However, casting is not without adverse events. Skin irritation is a commonly cited complication, and casting has been shown to affect gastrointestinal and respiratory systems.10,11,12 In addition, compression on the axilla may cause subclavian vein thrombosis. 13 This review sought to evaluate the efficacy and safety of casting as a temporary measure for the treatment of IIS.
Methods
This is a ‘before and after’ comparison of casting effect on IIS patients. The protocol was determined a priori. The reporting is in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14
Data sources
A comprehensive electronic search of PubMed and Embase databases from the earliest researchable time to 19 November 2018 was performed. There were no restrictions applied to the search strategy. The following keywords were used: (cast OR plaster) AND scoliosis AND idiopathic in all fields. For Medical Subject Headings (MeSH) terms, the following were used: ((‘scoliosis’ (Mesh)) AND ‘child’ (Mesh)) AND ‘casts, surgical’ (Mesh). A manual search was performed for relevant citations within articles.
Study selection criteria
Selected full-text articles were retrieved if there were data on IIS, which is defined as onset before the age of three without any identifiable cause, and a mean Cobb angle of 20° or more. All techniques of serial casting were considered. Case reports, non-English manuscripts, non-idiopathic scoliosis patients and animal studies were excluded. When the full-text article was not available, journals and authors were contacted by email, and if this was unsuccessful, the study was excluded. Initial screening of titles and abstracts was done independently by two authors, followed by a full-text review when appropriate.
Data abstraction
The extraction of relevant information was performed by two independent reviewers and discrepancies were addressed by discussion and consensus. Extracted information included the following: year of publication, study type, sample size, patient demographics, aetiology of scoliosis, type of intervention, casting material, number of casts, duration of cast wear, adverse outcomes and peri-intervention Cobb angles.
Assessment of methodological quality
The authors independently evaluated each study design using criteria validated by Downs and Black as suggested by the Cochrane handbook, 15 which included domains on reporting, external validity, internal validity and power. The maximum score is 31, with a higher score indicating better methodological quality. 16 Disagreements between authors’ assessments were solved by discussion and consensus.
Outcome measures
The primary outcome was stabilisation or improvement of scoliosis during the casting period as quantified by the change in mean coronal Cobb angle of the major curve, before initiation of casting and after removal of the last cast. Secondary outcomes were all reported complications related to the treatment. When the mean Cobb angles and standard deviations were not reported, an email was sent to the corresponding author and if the mean was still unavailable, the study was excluded from the quantitative analysis, missing standard deviations were imputed.
Statistical analysis
A meta-analysis based on the primary outcome mean difference and a 95% confidence interval (CI) was conducted. A random effect model was chosen to create a forest plot using the generic inverse-variance method. Statistical heterogeneity was quantified with an I 2 statistic and a value of 75% or higher was set as ‘considerable’, which would be explored by meta-regression for the continuous variables mean age and pre-treatment Cobb angle of each study. Subgroup analysis was done according to the type of casting material. Publication bias was evaluated visually by a funnel plot. Analyses were performed using the Review Manager (RevMan) version 5.3 (The Nordic Cochrane Centre, Rigshospitalet, Copenhagen, Denmark) and the statistical software R version 3.5.1 (The R Development Core Team, The R Foundation, Vienna, Austria).
Results
The search strategy is outlined in a PRISMA flow diagram (Figure 1). The electronic database search revealed 481 studies and the manual search yielded 23 studies. After removing duplicates, 366 papers were screened by reading the title and the abstract. Subsequently, 21 full-text articles were reviewed for eligibility, 12 were part of the qualitative analysis, and 10 were quantitatively analysed. In one included study, the pre- and post-casting standard deviations were imputed via direct substitution with a value from another similar study. Two eligible studies were excluded from data pooling for missing final mean Cobb angle.

Flow diagram of the identification and selection of studies.
All the selected studies had a retrospective cohort design, some of them included non-idiopathic scoliosis, but IIS data were separate (Table 1). Other than one case report, no other study designs were encountered during the search. The main outcome measure in all studies was the coronal Cobb angle. Four studies included various data on spinal length. Three studies included radiographic vertebral rotation measures and one study measured sagittal Cobb angles. None of the studies included formal power analysis. The overall methodological quality using the Downs and Black checklist, which applies to non-randomised studies, is listed in Table 1.
The included studies and quality assessment.

NR: not reported; POP: plaster of Paris; FG: fibreglass; VEPTR: vertical expandable prosthetic titanium rib.
The Downs and Black checklist, the maximum score is 31.
Entire cohort, including non-idiopathic scoliosis patients.
With respect to Cobb angle change after casting, 10 studies were included for meta-analysis, which included a total of 243 subjects (Figure 2). The pooled mean Cobb angle improvement from before to after casting was 24.85° (95% CI: 19.25 to 30.46, p < 0.001, I 2 = 78%). In terms of complications, superficial skin lesions and non-fatal pulmonary complications were the most common adverse events reported (Table 2). To explore heterogeneity indicated by the high I 2 , subgroup analysis of six studies that explicitly indicating the use of plaster of Paris for the initial cast moulding did not reduce I 2 or positively influence treatment effect, rendering cast material unlikely to be the cause of heterogeneity. Likewise, subtracting studies with lower Downs and Black scores did not alter the pooled mean or improved heterogeneity. Results of the meta-regression which was based on age and initial curve magnitude are shown in Table 3. Age reduced improvement in Cobb angle after casting and the residual I 2 was 55%. Controlling for curve severity reduced I 2 but was not associated with the mean difference in Cobb angle from before to after casting in this review. The bubble plot with the meta-regression line showed an inverse relationship between age at the first cast and Cobb angle correction immediately after casting (Figure 3). Moreover, the drawn funnel plot was asymmetrical, and the cylindrical contour is suggestive of a large heterogeneity between studies rather than reporting bias (Figure 4).
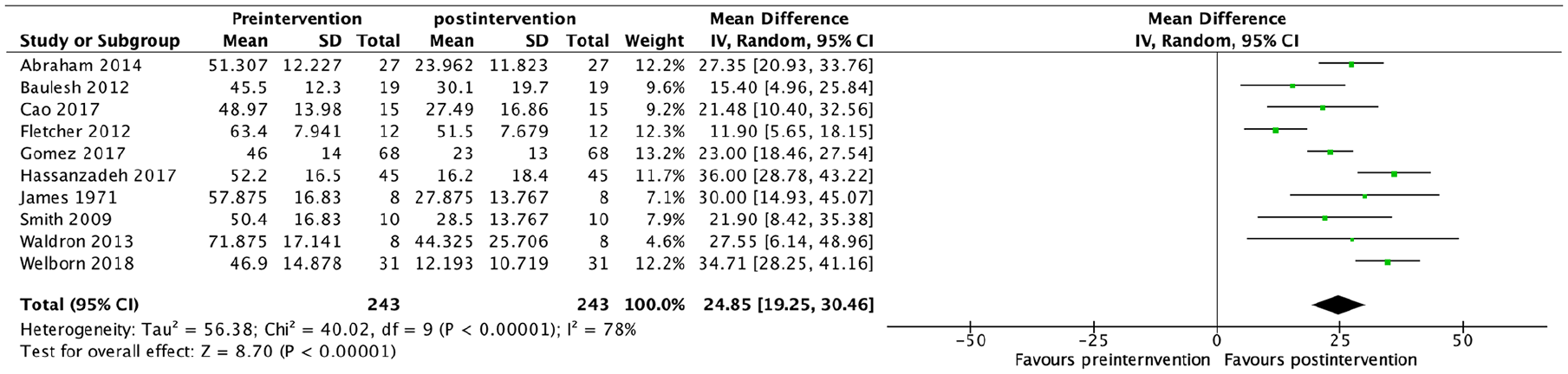
Forest plot showing changes in pre- and post-casting coronal Cobb angle.
Reported complications of casting in infantile idiopathic scoliosis.

NR: not reported.
Denotes entire cohort, including non-idiopathic scoliosis patients.
Meta-regression analysis of the difference in Cobb angle from age and curve magnitude at baseline.

The value of the bold is to highlight statistical significance.

Bubble plot with fitted meta-regression line.

Funnel plot.
Discussion
Lack of consistent treatment guidelines creates intellectual, technical and ethical dilemmas for clinicians who deal with IIS. The present systematic review aimed to evaluate and integrate the existing evidence on casting and present it using meta-analysis and meta-regression methods. To reach a more meaningful conclusion, this review was limited to infantile age group and idiopathic aetiology. We found that casting for IIS predictably controls coronal Cobb angle regardless of scoliosis severity, but the effect diminished with age and the potential for harm is low. All included studies demonstrated an overall improvement in Cobb angle. In a study by Sanders et al., 27 55 infantile scoliosis patients of mixed aetiology were pooled from three hospitals, of whom 38 were idiopathic, only six patients did not show a decrease in Cobb angle after casting.
As expected, there was great heterogeneity when non-randomised studies were combined secondary to clinical diversity. The heterogeneity was reduced after controlling for curve severity and age, but only age significantly influenced the mean difference in Cobb angle (Figure 3). Gussous et al. demonstrated a similar inverse relationship in 41 patients with IIS. 28 Age at first cast was also associated with less curve correction in studies by Mehta, Gomez et al. and Stasikelis et al. in contrast to other reports.6,18,24,25,26 We did not find an association between the pre-treatment magnitude of the curve and the reduction of Cobb angle after casting. Similarly, Welborn et al. found no association between initial curve magnitude and final Cobb angle after casting. 26 In addition, while the authors of this review think that better moulding, and hence correction can be obtained with plaster of Paris compared to synthetic materials, this was not suggested by this review. A direct comparison study design may reveal differences.
Serious complications are possible after casting,10,13 but what was reported in this review appears manageable and without permanent consequence (Table 2). Johnston et al. compared the effect of serial casting in 27 patients, 11 were idiopathic, with a matched group that underwent growing rods. Intuitively, there was more correction in the growing rod group, but there was a 10-fold increase in the complication rate in favour of casting. 29
Considerable heterogeneity in this study led to an asymmetrical funnel plot. This heterogeneity among included studies may affect the precision of the effect estimate, but the overall positive effect of casting in reducing or at least stabilising curve progression is clear. The absence of scattering at the base of the plot may exclude underreporting of smaller studies. Spinal length, an indirect measure of lung growth, might be another useful measure to explain heterogeneity. Unfortunately, these data were not consistently reported in the included studies of IIS casting. Although repeat studies on the same cohort were excluded, we cannot rule out the possibility of having patients enrolled in more than one study. Owing primarily to the relative rarity of IIS and ethical constraints, there are no randomised trials examining the effect of casting and this review was built on non-randomised studies, which are prone to selection bias. Therefore, results should be interpreted with caution. According to the GRADE scheme for assessing the quality of evidence, the present review of a small collection of observational studies would be graded as ‘low’. 30 Finally, evidence on anaesthesia-associated neurotoxicity is conflicting and the current notion is that procedures should not be avoided or delayed if the indication is robust. 31
Conclusion
Casting in IIS seems to be safe and effective. We believe that casting has stood the test of time as a bridging method to control scoliosis during growth. Moreover, the complication rate is low, and none of the included studies reported irreversible complications. However, in the absence of randomisation, confounding could influence the results.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.