
Abstract
Objectives:
This blinded random-assignment, placebo-controlled pilot study investigated the effects of Maharishi Light Technology with Gems on three self-report measures: a questionnaire with a 5-point Likert-type scale, the Profile of Mood States (POMS), and an open-ended question. This pilot is the beginning of a research program to test the effects of this therapy.
Methods:
In total, 18 meditating subjects received two treatments on consecutive days, randomly either Maharishi Light Technology or placebo, then 2 weeks rest, and then the other treatment on consecutive days.
Results:
In comparison to placebo treatments, Maharishi Light Technology treatments were (1) rated as being significantly more settled, (2) higher on the Positive Self-Esteem subscale of the POMS and (3) described by the terms: healing, wholeness, and bliss.
Conclusion:
These treatments lead to significant improvements on self-report measures. Future research could assess their effects across both meditating and nonmeditating populations, using physiological measures to probe possible mechanisms of the effects.
Introduction
Energy therapies, which are part of complementary and alternative medicine, act on the level of energy fields to affect mental and physical health. One therapy, laying-on-of-hands, has been tested with random-assignment controlled studies. A study with 41 adults reported that three 10-min treatments of laying-on-of-hands, given on consecutive days, led to significant reductions in anxiety scores and significant increases in oxygen saturation compared to sham and no intervention. 1 Another study with 13 newborns reported that three 10-min treatments of laying-on-of-hands given on consecutive days resulted in lower breath rates and lower cortisol levels compared to controls. 2 Another practice, Therapeutic Touch, has been tested on wound healing. A meta-analysis found that in two studies, wound healing was improved, in another it worsened, and in a fourth, there was no difference with Therapeutic Touch. 3
Light has also been used as therapy. Thirty years ago, Rosenthal developed “Bright Light Therapy” (>1000 lumens full spectrum light) to combat depression (Seasonal Affective Disorder) during the winter months when daylight hours are reduced. 4 A recent meta-analysis of 19 studies compared effects of Bright Light Therapy, dim light (<400 lumens), and negative-ion generators on depression symptoms. Bright Light Therapy compared to the two control conditions significantly decreased depression ratings. 5
While Rosenthal used full spectrum light to treat Seasonal Affective Disorder, another class of light therapies, chromotherapy, applies individual colors to treat different health problems. 6 Chromotherapy is often considered pseudoscience and meta-analyses have yielded no consistent effects of chromotherapy. 7 However, a recent review of advances in photobiology and photobiomodulation suggests cellular and molecular effects of the visible color bands. 8
Blue light affects depth of sleep. 9 After 2 weeks wearing short wavelength (blue light)-blocking glasses for 4 h prior to bedtime melatonin levels were higher (saliva samples), sleep latency was faster (actigraph) and sleep quality was improved (Pittsburgh Sleep Quality Index) in 21 subjects. 10 Blue light is reported to reduce organ injury by comparison with red light or ambient white fluorescent light in liver and kidney ischemia/reperfusion by reducing myeloperoxidase within each organ. 11 Red and green light, compared to full spectrum light, led to significant improvements in cognitive ability in elderly subjects, as measured by an adapted Mini-Mental State Exam in a random-assignment study with 45 subjects in each group. 12 Finally, a random-assignment study tested 117 subjects assigned to three groups, who were presented modulations of three different color bands: warm colors (Red, Orange, Yellow), cool colors (Green, Blue, Indigo), all colors in the spectrum, and white light as a control. The three color bands affected autonomic functioning: heart rate, heart rate variability, and skin conductance; the Profile of Mood States (POMS); and a subjective evaluation questionnaire. 13
Another intervention that uses light is Maharishi Light Technology with Gems (MLG). Color therapy projects light through large (>5 cm) colored plastic filters rather than gems. This produces colored light which is diffuse rather than focused. MLG uses battery powered light-emitting “pens” that focus light through 13 different gem stones. 11 The effect of MLG treatment would include contributions of the orderly, crystalline structure of the gems; the colors of the gems due to their trace elements; and the light shining through the gems, which is said to amplify their effects.
This is a pilot research study intended to explore possible effects of MLG. Subjective reports were measured as the first step in this research program. If significant subjective reports are found, then future research can explore physiological mechanisms of any observed effects.
Hypothesis
If MLG therapy has significant effects, then subjects will report more positive self-report measures compared to placebo treatments. We used a random-assignment, placebo-controlled blinded study to assess subjective experiences while having an MLG treatment compared to placebo treatments.
Materials and methods
Design
This was a double-blind random-assignment placebo-controlled pilot study that included two treatments on sequential days, 2 weeks rest, and then two more treatments again on sequential days. The two sequential treatments after the rest period were on the same days of the week as the two initial treatments. The 2-week rest reduced possible carryover effects of one set of treatments to another. Each set of two treatments was randomly either MLG or placebo treatment. The research was conducted over a 2-month period from August to September 2018. All subjects received both sets of treatments.
We used a random-assignment design to strengthen cause/effect conclusions from the study. In this study, we measured healthy normal subjects free from chronic diseases.
Subjects
In total, 18 subjects participated in this study. They were an average age of 66.6 ± 10.5 years. We did not intend to test a geriatric population. They were the ones who responded to our posters. They were healthy in mind and body. Since this is the first study on MLG, we did not have data to calculate effect sizes to determine the number of subjects that should yield statistical significance.
We looked for subjects who regularly explored inner subjective experiences through meditation practice and were familiar with experiences during MLG. These subjects were tested because they might be more aware of possible effects of MLG. The subject inclusion criteria were as follows:
Currently practicing Transcendental Meditation,
Having had MLG sessions before,
Mentally and physically healthy.
Exclusion criterion was anyone who did not meet the inclusion criteria.
Seventy-two percent of the subjects were female. Subjects practiced Transcendental Meditation for an average 43.7 ± 6.7 years and had received MLG treatments before the study (average 3.9 ± 4.9 times). This study was approved by the Institutional Review Board (IRB) at the university. Subjects signed a consent form before beginning the experiment. To maintain confidentiality, subject numbers were used in data files. The research was partially funded. We asked subjects to pay $30 toward each treatment. The typical cost is $120/treatment.
Procedure
Subjects responded to a flyer posted in the community meditation halls. The second author contacted each subject and set up an appointment to come to her office to receive four treatments: two treatments on sequential days, 2 weeks rest, and then two more treatments again on sequential days. Her office is in a residential building. The subjects laid down on a comfortable padded table in the office. The first two treatments were randomly either MLG or placebo. The second two treatments were the other. Figure 1 presents the flow of subjects through the study.

Flow of subjects through the study.
This study followed the standard MLG protocol, which is to test the client’s reaction to each of the gem light pens. No individuals reported negative reactions to a specific gem. Many (about 3/4) felt neutral toward Zircon, green tourmaline, and carnelian in the testing phase. To standardize treatments, we administered those 10 of the 13 possible gems, to which a participant felt more positive.
This study was fully blinded.
Subjects were blind to the study hypotheses—none knew that there were placebo treatments.
The second researcher who administered the treatments was also blind to the nature of the light-emitting “pens”—MLG or placebo. The third author placed the light-emitting “pens” (either authentic MLG or placebo) in a tray according to a randomized list of 0’s and 1’s, computed by the online software, https://stattrek.com/statistics/random-number-generator.aspx, and left the tray for the second author to use in that treatment. There was no communication between the second and third author.
The first author, who analyzed the data, was blind to treatment status when he analyzed the data.
Test instruments: intervention and placebo
MLG pens
The MLG pens are roughly 1.5 cm in diameter and 15 cm long. They are battery powered. The light is shown through 13 gems: zircon, amethyst, diamond, blue sapphire, green tourmaline, emerald, amber, yellow sapphire, coral, pearl, carnelian, ruby, and cat’s eye. The light is projected through the gems and aligned along the midline of the feet, abdomen, chest, throat, and top of the head. A typical treatment lasts 25 min. Gem stones have a characteristic crystalline structure and corresponding color that is predicted to produce optimally beneficial effects. 14 The light is focused in a small circle, a few centimeters in diameter, depending on how far the pens are placed from the client’s body.
Placebo pens
A set of placebo light-emitting “pens” was created. These placebo “pens” were identical in shape, color, and outer material (gray metal) to the authentic MLG light-emitting “pens.” The placebo light-emitting “pens” projected light through colored glass, while the authentic MLG light-emitting “pens” projected light through gems. The light from both sets of light-emitting “pens” was similar in color and diameter. It was not apparent from looking at the pens or the light on the clothes which were the MLG pens and which were the placebos.
Test instruments: subjective measures
5-point Likert-type scales, Y/N questions, and open-ended questions
Self-report measures were created for this study to identify differences in the subjective experiences during the two different treatments. These were created specifically for this study. The second author gave all instruments to the subjects as well as the open-ended questionnaire.
After each treatment
The subjects rated the treatment with (Y/N) questions that probed: (1) Feeling sleepy? (2) Feeling agitated? and (3) Transcended during the treatment? They also compared on a 5-point Likert-type scale (1 = “less deep” to 5 = “more deep,” with 3 being “the same”) their experiences during the treatment with typical experiences during their daily meditation practice. “Deep” is a subjective measure that is meaningful to these subjects. It entails an experience of thoughts becoming secondary and inner silence becoming more primary.
Before the second and fourth treatments
The subjects rated the effect of the first and third day’s treatment on their sleep, meditation, and activity during the past 24 h, using a 5-point Likert-type scale. This scale assessed 24 h carryover effects from the treatments.
Before the third treatment and 2 weeks after the fourth treatment
The subjects rated the effect of the treatments on sleeping, meditation, and activity during the 2 weeks after a sequence of treatments (Y/N). This scale assessed 2-week carryover effects from the treatments.
Open-ended questions
After each treatment, subjects responded to this question: “Please describe your experiences during this treatment.” They could write as much as they wished.
Profile of Mood States
The subjects filled out the POMS after each pair of treatments. This scale lists 72 descriptors of emotional states, such as clear, confused, or happy. The responses ranged from “0” if the specific adjective did not describe them at all to a “4” if it described them perfectly. This instrument yields a score for total mood disturbance and subscale scores for tension/anxiety, depression/dejection, and anger/hostility subscales. The POMS has high construct and criterion validity, 15 and internal consistency coefficients range from 0.90 to 0.95. 16
Data analysis
The Y/N answers were converted to 1 and 0. The responses to the Likert-type scales were summed. ATLAS.ti was used to assess the descriptions of experiences to generate codes and to group these codes into super-codes.
Statistical analysis
Nonparametric statistics were used to assess the responses to the Y/N answers. F tests were used to assess the response to the Likert-type scale and the POMS. The frequency of use of different codes and super-codes was compared in a narrative analysis.
Results
(Y/N) questions
There were no significant differences in the self-report questions assessing sleepiness, agitation, or settling during the treatments, F(1, 17) = 1.3, p = .28.
Likert-type-scale question
The responses on the Likert-type scale were summed for each pair of treatments (MLG or placebo) and compared with an analysis of variance (ANOVA). On this analysis, subjects rated their experiences during the MLG treatment as significantly deeper than during the placebo, F(1, 17) = 6.6, p = .021. The experiences during the placebo were similar to their daily Transcendental Meditation practice, as indicated by an average of 3. Figure 2 presents the averages of self-evaluation of experiences during the two sets of treatments.

Subjective evaluation of experiences during MLG was significantly higher than their typical Transcendental Meditation practice, F(1, 17) = 6.6, p = .021. In this scale, 5 = deeper, 3 = same, and 1 = less deep.
Profile of Mood States
A repeated-measures ANOVA with treatment as the repeated measures and the seven subscales of the POMS as variates yielded significant interactions between the treatment and the seven subscales, F(6, 12) = 4.0, p = .027. Sub-analyses found no significant treatment differences in the five negative moods: anger, confused, depressed, fatigue, and tension, F(1, 17) = 2.3, p = .15. This could reflect the small sample size and a floor effect. These subjects were very low in these negative moods at pretest. There were also no significant treatment differences for vigor, F(1, 17) = 1.5, p = .25. However, positive self-esteem was significantly higher after the MLG treatments, F(1, 17) = 5.0, p = .04. These data are presented in Figure 3.

Significantly higher positive self-esteem was reported after the MLG treatments, F(1, 17) = 5.0, p = .04. On this scale, a “0” indicates that the specific adjective does not describe the person at all; a “4” indicates that it describes them perfectly.
Content analysis of open-ended question
The responses to the open-ended questions were transcribed and grouped by treatment (MLG versus placebo) and content analyzed using ATLAS.ti. This software allows the researcher to read through the transcriptions and highlight “units of meaning”—words or phrases that express a unique and coherent idea. In ATLAS.ti, these phrases are called “quotations.” Once quotations had been highlighted, each was assigned a code. For example, one subject said, “Wow. I loved the treatment.” This was coded as “deep appreciation.” After coding of quotations was completed, codes with three or fewer quotations were reviewed to see if they fit into other, similar codes. Next, codes were grouped by common themes into higher order codes called super-codes.
The number of words used in describing experiences during the MLG and the placebo treatments was similar—1888 versus 1735. The content analysis yielded 15 codes for each treatment. These 15 codes were combined into five super-codes: Healing, Blissful, Wholeness, Restful, and Everyday Experiences. Table 1 presents the details of the super-codes, including their constituent codes, the number of times each code was used in parentheses, and a few examples of quotations that were assigned this code.
Details of each super-codes with its constituent codes, the frequency that each code was used, and a few examples of quotations that were assigned this code.

MLG: Maharishi Light Technology with Gems.
Figure 4 presents the average times each super-code was used to describe experience during each treatment. The most substantial treatment differences were in Healing, which was used over five times more frequently to describe the MLG treatments, and in Everyday Experiences, which was used almost two times more to describe the placebo treatment. The super-codes of Wholeness and Blissful were also higher for the MLG treatment and levels for Restful were similar.
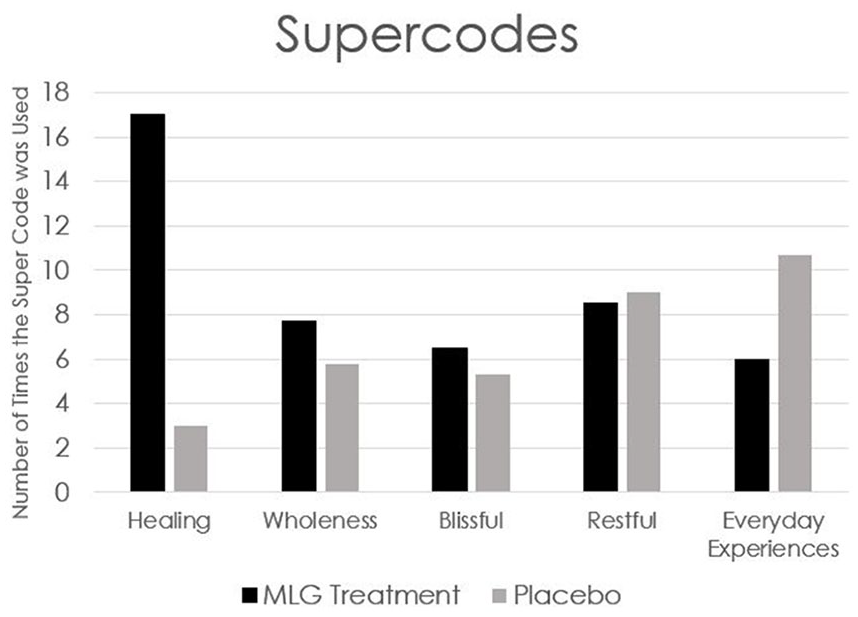
The frequency of healing was used substantially more during the MLG treatment. Wholeness and Blissful were also used more to describe the MLG treatment. In contrast, Everyday Experiences was used much more in the placebo treatment.
Discussion
This random-assignment controlled pilot study yielded significant differences during MLG compared to the placebo treatment on three self-report measures: a questionnaire with a 5-point Likert-type scale, a standardized paper-and-pencil test, and an open-ended question. The results present a coherent picture that MLG treatments were experienced differently than the placebo treatments.
The study design may be considered as strong for a pilot. (1) The sequence of treatments was randomized—half the subjects received MLG treatment first, the other received the placebo first. (2) All subjects received both treatments. (3) The study was blinded: the subjects did not know that they would receive placebo treatments; the technician was blind to group membership, the analysis was conducted blind. (4) A standardized test of emotions, the POMS, was used.
After the MLG treatments, subjects reported higher positive self-esteem. MLG is predicted to result in heightened self-awareness, 14 which could lead to higher positive self-esteem on this scale. (5) All subjects meditated regularly and had previously had MLG treatments. Their common meditation experiences served as a reference for their treatment evaluations. These subjects would be expected to settle down when simply lying with eyes closed, since they meditated daily. In spite of their tendency to naturally settle down, the MLG treatment was rated as being significantly more settled than the placebo. Multiple measures of inner experiences were used.
Finally, the content analysis on the descriptions of experiences during each treatment yielded a clear result. The MLG treatment led to more incidences of mentions of healing—17 during MLG treatments compared to 3 during the placebo treatments. In contrast, the placebo treatments led to more incidences of mentions of everyday experiences, which might occur whenever one closes the eyes.
Future research could assess MLG effects across meditating and nonmeditating populations, and use physiological as well as self-report measures to quantify the effects and to begin to explore the mechanism of the observed effects of MLG.
Limitations of this study
There are four limitations of this study. First, we used a small number of subjects so the study was underpowered. However, even with only 18 subjects, we found significant effects of MLG on subjective reports. Second, we used subjects who practiced Transcendental Meditation and had MLG treatments before. This severely limits the generalizability of these data to the general population. We used a criterion-rich group in this pilot study who were daily exploring subjective experiences during meditation practice, and so may be more sensitive to differences in MLG and placebo treatments. Third, we only used qualitative measures. Future research could measure physiological measures such as heart rate variability, breath rate, skin conductance, and electroencephalography (EEG) in meditating naïve subjects. The last limitation is more global. Do qualitative and quantitative measures exist that can accurately capture subtle, delicate changes in order and balance in the physiology, as well as calmness and clarity? Inner experiences cannot be directly measured. However, since our unconscious and pre-conscious thoughts and feelings affect functioning of mind and body, self-report measures and physiological measures such as EEG, magnetoencephalography (MEG), functional magnetic resonance imaging (fMRI), breath rate, heart rate, and skin conductance could give an indication of what is happening at very quiet levels of awareness.
Footnotes
Acknowledgements
We thank Joachim Roller for creating the placebo light “pens” for use in the placebo treatment in this research. We also thank Ellen Metropole for her help in transcribing the open-ended responses and editing the final manuscript. Last, we thank Martin Schmidt and Dr. Jane Schmidt-Wilk for translation of the German patent and descriptions of Maharishi Light Technology with Gems.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Frederick Travis and David Scharf have no conflict of interests. Ayala Melzer is a certified technician for administering Maharishi Light Technology with Gems, who was central in designing the study. She administered the treatments but was blind to group membership.
Ethical approval
Ethical approval for this study was obtained from the Institutional Review Board at Maharishi University of Management, approval number 2019_020, date July 2018.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.