
Abstract
Background:
Treatment with ultrasound and colour Doppler–guided minimally invasive Achilles tendon scraping and plantaris tendon removal has shown promising short-term results in patients with chronic painful midportion Achilles tendinopathy.
Methods:
In a follow-up study, 182 consecutive patients (241 tendons) who had undergone Achilles tendon scraping and plantaris tendon removal were contacted on telephone by an independent investigator. The patients who answered the telephone call were included, and they answered a questionnaire on telephone and then also sent their written answers. The questionnaire included information about patient satisfaction with the result of the treatment, time to return to full Achilles tendon loading activity, and a pain score (Visual Analogue Scale-VAS).
Results:
The follow-up period was 5.8 years (mean) (range of 2–13 years) after surgery. Altogether, 110 patients (136 Achilles tendons), 52 years (mean)(range 18-73) old at surgery could be reached and were included. In total, 81 tendons were operated with the Achilles scraping procedure alone, and for 55 Achilles operations also a plantaris tendon removal was performed. For 93% of the operated tendons, the patients were satisfied with the surgical outcome and the VAS had decreased from 74 preoperatively to 8 postoperatively. Nine male patients (9 tendons), five operated with scraping + plantaris removal, had remaining tendon pain during loading and were not satisfied. Their VAS score ranged from 22 to 91. For 21% of the operated tendons, some occasional mild discomfort not preventing from full tendon loading, was reported. There were no differences in pain reduction and satisfaction rates between men and women, and between Achilles scraping alone and scraping plus plantaris removal.
Conclusion:
Ultrasound and colour Doppler–guided surgical Achilles tendon scraping and plantaris tendon removal in patients with chronic painful midportion Achilles tendinopathy show remaining good clinical outcomes and high satisfaction rates in this longer-term follow-up.
Introduction
Chronic midportion Achilles tendinopathy is a relatively common and often disabling condition among sports and recreationally actives, as well as non-active individuals.1,2 The aetiology is still unknown and heavily debated. It has been suggested to be associated with overuse,2,3,4 but interestingly, also non-active individuals suffer from this condition.5,6 Also, there is increasing evidence for a connection between metabolic factors and tendinopathy. 7 Men and women have been found to be equally affected by midportion Achilles tendinopathy. 1
Patients suffering from chronic painful midportion Achilles tendinopathy have been shown to suffer both physically (lowered activity level) and emotionally, 8 and there is an obvious need to find a successful treatment method. Exercise such as painful heavy load eccentric training has been shown to be efficient.9,10 However, not all are cured by this treatment approach, and not all can do the exercises because of other limiting conditions. Recently, involvement of an interfering plantaris tendon has been suggested to be a key factor in a sub-group of patients with midportion Achilles tendinopathy. These patients often respond poorly to treatment with eccentric training. 11 For patients where non-surgical treatment is not successful, surgery is indicated. The minimally invasive method ultrasound and colour Doppler (US+CD)–guided surgical Achilles scraping, in certain cases combined with plantaris tendon removal, has been demonstrated to give good clinical results with a quick return to Achilles tendon loading activities in short-term follow-up studies.8,11,12,13,14
This study aimed to show the longer-term follow-up results of patients with chronic painful midportion Achilles tendinopathy who had been operated with the US + CD–guided Achilles scraping and plantaris removal technique. The follow-up consisted of a telephone interview and written answers on a questionnaire, including information about patient satisfaction with the result of the treatment, time to return to full Achilles tendon loading activity, and a pain score (VAS) evaluating Achilles tendon pain during the habitual type of loading.
Material and Methods
In this retrospective follow-up study, consecutive patients with chronic painful midportion Achilles tendinopathy who had undergone surgical treatment with the minimally invasive Achilles scraping and plantaris tendon removal procedure were evaluated with a telephone interview and a questionnaire (written answers).
Material
Before surgery, all patients had suffered from midportion Achilles tendon pain for at least 3 months (range 3-120 months), and all had tried treatment with different types of loading regimens. The majority also had tried rest and non steroidal anti-inflammatory drugs.
Ultrasound and colour Doppler (US+CD) examination
In all patients, before surgery the clinical diagnosis had been confirmed with US + CD examination. The US + CD showed a thickened Achilles tendon midportion with irregular tendon structure and locally high blood flow outside and inside the regions with structural tendon changes on the ventral (deep) side of the Achilles. The surgical procedure was guided by the US + CD findings.
Surgical treatment-US + CD–guided Achilles scraping and extirpation of the plantaris tendon
After washing, 5–10 mL of a local anaesthetic (Xylocaine + Adrenaline, 5 mg/mL) was injected into the medial and ventral sides of the Achilles midportion. The skin was then draped with a sterile paper-cover, exposing only the midportion of the Achilles tendon. A longitudinal skin incision (1–1.5 cm) was placed on the medial side of the Achilles midportion, and the Achilles tendon was carefully identified. If the plantaris tendon was found to be positioned close to, or invaginated into, the medial side of the Achilles (Figure 1), it was carefully released. The plantaris was followed proximally and cut slightly above the level for the lower medial soleus insertion, and followed distally and cut to as close as possible to the distal insertion. Most often 5–8 cm of the plantaris tendon was removed. There was often a richly vascularized fat tissue inter-positioned between the Achilles and the plantaris tendon. This tissue was removed, followed by the traditional Achilles tendon scraping procedure.11,13 In the regions with US–verified changes inside the tendon and high blood flow (CD-verified) on the ventral side of the tendon, the tendon was completely released from the ventral soft tissues by sharp dissection with a scalpel (staying close to the ventral side of the tendon). This was followed by hemostasis using diatermia. The skin was closed by single non-resorbable sutures.

Picture showing the minimally invasive surgical treatment of a patient with chronic painful midportion Achilles tendinopathy and plantaris tendon involvement. The scissor is positioned in between the thickened plantaris tendon (right) and the thickened Achilles tendon (left). The plantaris tendon is located very close to the medial side of the Achilles, and only a thin and richly vascularized fat layer is separating the tendons.
Postoperative rehabilitation
Day 1 (surgery day): rest, elevated foot.
Day 2: ROM (range of movement) exercises, short walks.
Day 3–7: gradually increased walking, slow tempo.
Day 8–14: increased walking distances and tempo, start bicycling.
From 2 weeks and forward: sutures out, gradually increased Achilles tendon loading up to free activity.
Follow-up procedure
In total, 182 consecutive patients (241 tendons), operated between 2002 and 2014, were by an independant assistant (A.R.) contacted via telephone. The patients who answered the telephone call and agreed to participate in the follow-up were included. These patients answered questions in a telephone interview and also sent in their written answers in a specific questionnaire. All telephone calls were performed between August and October 2015. All questionnaires (written answers) were received by the end of 2015.
Outcome measures
The same questionnaire was used for the telephone interview as for the written answer questionnaire. The questionnaire included general questions about smoking habits, on-going treatment for hypertension, type 2 diabetes mellitus, and high blood lipids, and more specific questions related to the Achilles operation such as; activity level and satisfaction with the result of the treatment. Satisfaction was evaluated by stating yes (satisfied) or no (not satisfied). Pain during the patients’ habitual tendon loading activity was evaluated by scoring on a 100-mm-long VAS, 15 where no pain was recorded as 0 and worst pain as 100.
Included patient material
The study included 110 patients, with 65 men who were 51 (mean) (range of 18–73) years old at surgery, and 45 women who were 54 (mean) (range of 34–73) years old at surgery (Table 1). The operation was performed 5.8 years (mean) (range of 2–13 years) prior to the follow-up.
Patient data.

There were 5 smokers (3 men and 2 women) and 13 snuff users (11 men and 2 women). Several patients were on treatments due to on-going diseases including hypertension (36; 24 men and 12 women), high blood lipids (25; 18 men and 7 women), and type 2 diabetes mellitus (9; 5 men and 4 women) (Table 1).
Most patients were recreationally active on different levels, and some were involved in multiple activities. Classified as heavier loading activities were jogging/running (n = 29; 19 men and 10 women), cross-country skiing (n = 18; 13 men and 5 women), cycling (8; 5 men and 3 women), gym training (n = 8; 4 men and 4 women), floorball (n = 2; 2 men), and badminton (n = 1; 1 man). Lighter loading activities were walking (n = 48; 22 men and 26 women) and swimming (n = 3; 2 men and 1 woman).
Surgical treatment with the Achilles scraping procedure alone was performed in 81 tendons, and for 55 tendons, there was also a plantaris tendon removal. There were three superficial wound infections (Staphylococcus aureus) successfully treated with oral antibiotics, but there were no other complications related to the surgical treatment.
Statistical methods
t-tests were performed using SPSS (Statistical Package of Social Science; SPSS Inc., Chicago, IL, USA) to analyse the data. Significant levels were defined as p < 0.05.
Ethics
The study was approved by the Regional Ethical Board in Umeå (DNR 04-157M; 2011-83-32M). The patients were informed that data from the follow-up were likely to be submitted for publication, and all gave their written consent.
Results
Patient satisfaction with treatment
Telephone interviews from 110 patients with 136 operated tendons showed that 101 patients (92%) (127 tendons, 93%) were satisfied with the result after surgery. Nine male patients (8%) (9 tendons, 7%), five operated with Achilles scraping + plantaris removal, had remaining tendon pain during loading and were not satisfied. There were no differences in the satisfaction rates between patients undergoing scraping alone and those with additional plantaris tendon removal.
Among the satisfied patients for 28/136 tendons (21%) there was a mild degree of tendon pain during Achilles tendon loading activity. This pain did not prevent them from full Achilles tendon loading activity. For altogether 99 Achilles tendons (73%) there was no pain during full Achilles tendon loading.
Pain levels after surgery (VAS)
Overall, the VAS scores decreased from 74 (mean) preoperatively to 8 (mean) at the follow-up (p < 0.001). There were no significant differences between men and women (Figure 2). However, there was a trend towards women having slightly better results (p = 0.07). There was no significant difference in the pain levels among the patients who underwent the Achilles scraping procedure alone and those that had additional plantaris tendon removal (Figure 3). Patients that were not satisfied with the treatment scored pain during tendon loading activity ranging from 22 to 91 on the VAS. Among the satisfied patients a minor group reported a mild degree of tendon pain during activity, their VAS score ranged from 2 to 58.
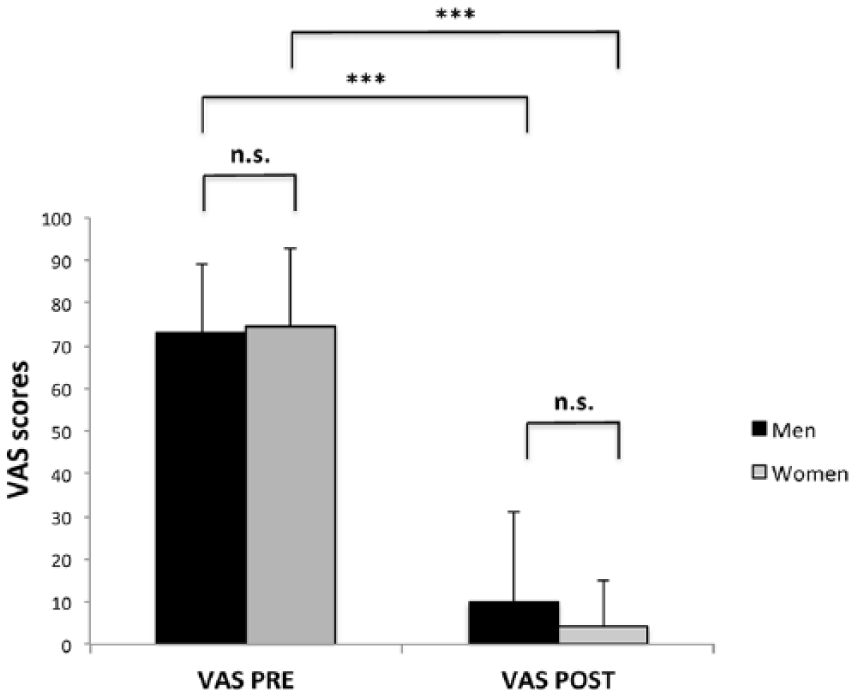
Graph showing pain scores before (VAS pre) surgery and at the longer-term follow-up (VAS post). Both male and female patients had significantly lower pain levels after surgery. There were no significant differences in the VAS scores between men and women. Significance levels: ***p < 0.001 n.s. = not significant.

Graph showing pain scores before surgery (VAS pre) and at the longer-term follow-up (VAS post) in patients with chronic painful midportion Achilles tendinopathy who underwent the Achilles scraping procedure and plantaris tendon removal (‘scraping + p’) or scraping alone (‘scraping’). In both groups a significant decrease in the VAS was observed after surgery. There were no significant differences in the postoperative pain scores between the groups. Significant levels: ***p < 0.001 n.s. = not significant.
Results of treatment over time
A comparison of the postoperative VAS levels registered at 1–3, 4–6, 7–9, and 10–13 years after surgery revealed no significant differences. Thus, the outcome of surgery did not decrease over time (Figure 4).

Graph showing pain scores before surgery (VAS pre) and at follow-up (VAS post) in patients with chronic painful midportion Achilles tendinopathy. Patients are sub-grouped in relation to the duration after surgery at follow-up. There were no differences in the postoperative VAS scores between patients who received surgery 1–3 (n = 22) years prior to follow-up and those who were operated 4–5 (n = 74), 7–9 (n = 26), or 10–13 (n = 14) years prior to the follow-up. Significant levels: ***p < 0.001 n.s. = not significant.
Discussion
This longer-term follow-up study on patients with chronic painful midportion Achilles tendinopathy, operated with the US + CD-guided mini surgical Achilles scraping procedure and plantaris tendon removal, showed very good clinical results with 92% satisfied patients (93% of all operated tendons) being back in full Achilles tendon loading activities.
The minimally invasive surgical scraping procedure and plantaris tendon removal has in previous short-term studies been shown to be a successful treatment method for patients with chronic painful midportion Achilles tendinopathy.8,11,12,13,14 This is the first longer-term follow-up study after this specific surgical procedure.
It is important to note that even though stating that they were satisfied with the result of the surgical treatment, and fully active in Achilles tendon lading activities without restrictions, some patients (28 tendons, 21%) scored some remaining Achilles tendon pain during loading. Taken together with the nine patients (nine tendons) who had a poor outcome there seems to be some remaining pain in 27% of the operated Achilles tendons. Anyhow for 73% the of operated tendons the patients scored that they were pain-free during Achilles tendon loading activities, clearly showing the potential of this type of surgical treatment. Also, the results were not deteriorating over time.
The patient material in this study consisted of relatively old individuals, where the majority were operated when they were around 50 years of age. This age group is representative for patients suffering from midportion Achilles tendinopathy in the northern part of Sweden. The activity levels, where more than 60% are very active in relatively demanding recreational sports, and the distribution between the sexes (59% men and 41% women), are also representative.
There are some limitations with this study. Not all patients could be reached, and not all who answered the telephone interview later answered the written questionnaire. Another weakness is the use of only a questionnaire follow-up. It would have been ideal to also perform a clinical and ultrasound follow-up, but it was unfortunately not possible due to logistical reasons with patients spread over long distances. However, we believe that there are some major strengths with this study. The patient material is randomly selected, only the ones who answered the telephone call were included. Also, the assistant who performed the telephone interviews, sent out the questionnaires, and filled in the data, is independent (has no medical education and has no knowledge about the management of these patients).
Compared with other surgical methods for treatment of midportion Achilles tendinopathy, like the commonly used open tenotomy and the percutaneous ultrasound-guided tenotomy methods,16,17 there are major differences. The US+DP-guided Achilles scraping method is performed outside the tendon, while the open tenotomy and percutaneous tenotomy methods are performed inside the tendon. This is a major difference where the US+CD-guided Achilles scraping procedure outside the tendon allow for immediate loading and a more aggressive rehabilitation, while for the intra-tendinous methods the rehabilitation needs to be kept significantly longer. After the Achilles scraping procedure outside the tendon the patients start walking the first day after the operation, and only very few patients having very heavy Achilles tendon loading occupations, need to be on sick-leave for a couple of weeks. Most patients are back in full Achilles tendon loading sports within 4–6 weeks after the operation.
The background to the US+CD-guided Achilles scraping procedure is the recent research on the basic biology, were the richly innervated peritendinous tissue on the ventral side of the Achilles tendon has been demonstrated to be the source of pain in chronic painful midportion Achilles tendinopathy. 18 Interestingly, surgically targeting the ventral peritendinous tissues not only relief the pain but also improves the Achilles tendon structure.14,19
To be able to reliably find the target (regions with high blood flow outside the ventral side of the tendinopathic Achilles) for the surgical scraping, US + CD-guidance is needed. Combining these two techniques also make it possible to minimize the skin incision and the tissue trauma during the scraping procedure and also when there occasionally is plantaris tendon removal. This is, however, also a bit complicated, because US + CD equipment, and education how to use it and interpret the findings, is needed. This might, at least initially, limit the use of this treatment method. Anyhow, we believe that the benefits achieved motivate the increased use of this treatment method.8,13,14
In around 40% (55/136) of the operated tendons this study, the plantaris tendon was removed. This was because macroscopically there were signs of interference (signs of compression from the plantaris onto the medial side of the Achilles tendon midportion) from the plantaris. In a cadaver study it was shown that all cadavers had a plantaris tendon and that there were multiple positions of the plantaris tendon in relation to the medial side of the Achilles tendon. 20 The plantaris tendon can be located very close to and sometimes even inserting into the Achilles.11,20 For patients having a plantaris tendon located close to the medial side of the Achilles, seemingly interfering (Figure 1), surgical removal has successfully been used.8,11,12,14,21 It can, of course, be argued that there is no knowledge about in which cases there is a need for removal of the plantaris tendon. From this study, there was a high success rate despite not removing the plantaris tendon in around 60% of the cases, clearly showing that removal is not always needed. Further research is needed to try to find that sub-group where plantaris tendon removal is needed. Maybe the new modality Ultrasound Tissue Characterisation (UTC) 22 can be helpful to pick the cases with plantaris tendon interference. 23 In a recent study on patients with midportion Achilles tendinopathy, UTC changes located on the medial side of the Achilles midportion where the plantaris tendon was positioned 23 disappeared over time after plantaris tendon removal. 19 Furthermore, it has recently been shown that plantaris tendons taken out from patients with midportion Achilles tendinopathy showed tendinosis features, 24 and that in two-thirds of the samples there were sensory nerves inside the plantaris tendon. 25 Consequently, some plantaris tendons might be pain-generators and removal might be beneficial. This is in contrast to the Achilles tendon, where sensory nerve accumulation very rarely has been noticed inside the tendon, and consequently, there is no need to go inside the Achilles tendon for treatment of tendinopathy.
An interesting observation was that a high proportion (61/110) of the patients in this study was on medication for diseases included among so-called metabolic disorders, especially treatment for hypertension and high blood lipids. This finding might be of interest for the discussion about the unknown aetiology to midportion Achilles tendinopathy, where metabolic factors have been suggested to possibly play a role for the aetiology. 7
The very good longer-term results shown in this study, allowing for Achilles tendon loading activities at desired level, are likely to have positive physical effects and might be especially important for the group of patients suffering from metabolic disorders. It is likely that there are also positive psychological effects. In a previous study using the SF-36 questionnaire, it was shown that patients suffering from chronic painful midportion Achilles tendinopathy also suffered emotionally in daily life, and that successful surgical treatment significantly improved their emotional status. 8
Conclusion
In conclusion, for patients with chronic painful midportion Achilles tendinopathy, treatment with US + CD-guided mini-surgery and plantaris tendon removal showed very good clinical results in this longer-term follow-up study. The treatment method shows stable and good clinical results over time, allowing for the patients to be physically active in their habitual Achilles tendon loading activities.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Regional Ethical Board in Umeå (DNR 04-157M; 2011-83-32M).
Informed consent
Written informed consent was obtained from all subjects before the study.