
Abstract
Objectives:
Appearance is a factor within head and neck cancer health-related quality of life measures; however, the issue of self-perceived appearance has received scant attention. Self-portraiture may provide insight into the patient’s perspective, allowing people to provide viewpoints that are not easily accessible. This research investigates the methodology of drawing and responses from patient-completed questionnaires in a head and neck cancer population.
Methods:
A sample of 30 people at least 3 months post-treatment for head and neck cancer were recruited. Participants completed the Derriford Appearance Scale, University of Washington Quality of Life scale, and two drawings: (1) how they recall themselves pre-treatment and (2) how they see themselves post-treatment. They were asked to discuss the methodology and their experience of it.
Results:
Correlations with Derriford Appearance Scale, University of Washington Quality of Life scale, and size drawings failed to find relationships between these variables. Post-treatment drawings were significantly smaller than pre-treatment. Qualitative analysis of the drawings found differences between the images. Participants related how drawing gave an opportunity to voice concerns that questionnaires and clinic appointments did not.
Conclusion:
Drawing can elicit distinctly different information about a person following treatment for head and neck cancer than that provided by health-related quality of life measures. Further research would clarify if clinical opinion matches patients’ drawing.
Introduction
It is recognised that patients can develop negative perceptions of their body after treatment for cancer.1,2 Loss of function and external alterations in body structure have been associated with depression that can exacerbate difficulties in communication and feelings of social rejection for people who have had treatment for head and neck cancer (HNC). 3 Disfigurement is a key domain that is included in Health-Related Quality of Life (HRQoL) questionnaires specific to HNC. 4
Even though appearance is present as a factor or domain within HNC HRQoL measures, the specific issue of the self-perceived appearance of people who have been treated for HNC has received relatively scant attention.5,6 Most ‘body image’ measures have their roots in work on weight and obesity and do not accurately assess distress and dysfunction in relation to appearance issues faced by people living with cancer. An exception to this is the Derriford Appearance Scale (DAS24), which was developed through a collaboration between plastic/reconstructive surgeons and psychologists with both clinical and non-clinical populations, 7 including oncology patients. In addition, there is some evidence that the appearance-specific domain of the University of Washington Quality of Life (UW QoL) Questionnaire can identify individuals with appearance concerns; however, the UW QoL has not typically been used to evaluate appearance-related adjustment specifically.5,8,9
Self-portraiture, or simple drawings of own body image, may provide a valuable insight into the patient’s perspective. 10 It offers a way to communicate other than speech, which can allow the drawers to explore the meaning of their situation by accessing material which could be suppressed and repressed by the conscious mind. 11 Therefore, drawing may allow people to provide viewpoints that are not easily accessible through interviews or questionnaires. 12 The produced drawings may ‘illustrate ideas in a more concrete and specific way than words’. 13 Harrow et al. 14 found that some women have mental images of their (breast) cancer, which can be accessed through verbal description and drawing. These images may embody both positive and negative beliefs about cancer, which can contribute to more meaning and informed decision-making and thus, ideally, improved outcomes. Drawing may therefore be a useful method to gain insight into people’s views and experiences. This may especially be the case when they have difficulties verbally either due to functional or language barriers. It may also allow individuals to access and communicate different aspects of their concerns than traditional methods. 15 Drawings have been used with children to understand their cancer experiences, 16 but it is still a rarely utilised method with adults. 17 However, the process required to draw could lead to a more succinct presentation of meaningful facets of the participants’ experiences.
The aim of the presented research is to use the novel methodology of drawing and relate that to the traditional responses from patient-completed questionnaires in a HNC population.
Methods
Ethical approvals were obtained from the local National Health Service (NHS) regulatory body (REC reference no. 10/H0107/24). Individuals provided written consent.
Participants
As a new data collection method (drawing) for this patient cohort, an opportunistic sample of 30 people at least 3 months post-treatment for HNC was recruited during a routine follow-up visit to the maxillofacial department. Thirty was selected as approximately 20% of the total patient cohort seen in the clinic during a year and 50% of the patients seen over the 5-month recruitment time frame. All people approached agreed to participate in the study. It was also the average size of previous samples used in studies designed to explore patients’ perceptions of their illness. 17 Although the sample was obtained by approaching people as they attended clinic (opportunistically), this sample matched the gender split for HNC and gave a representative range of cancer stages and treatment regimens (Table 1). 18
Psychosocial characteristics of participants.
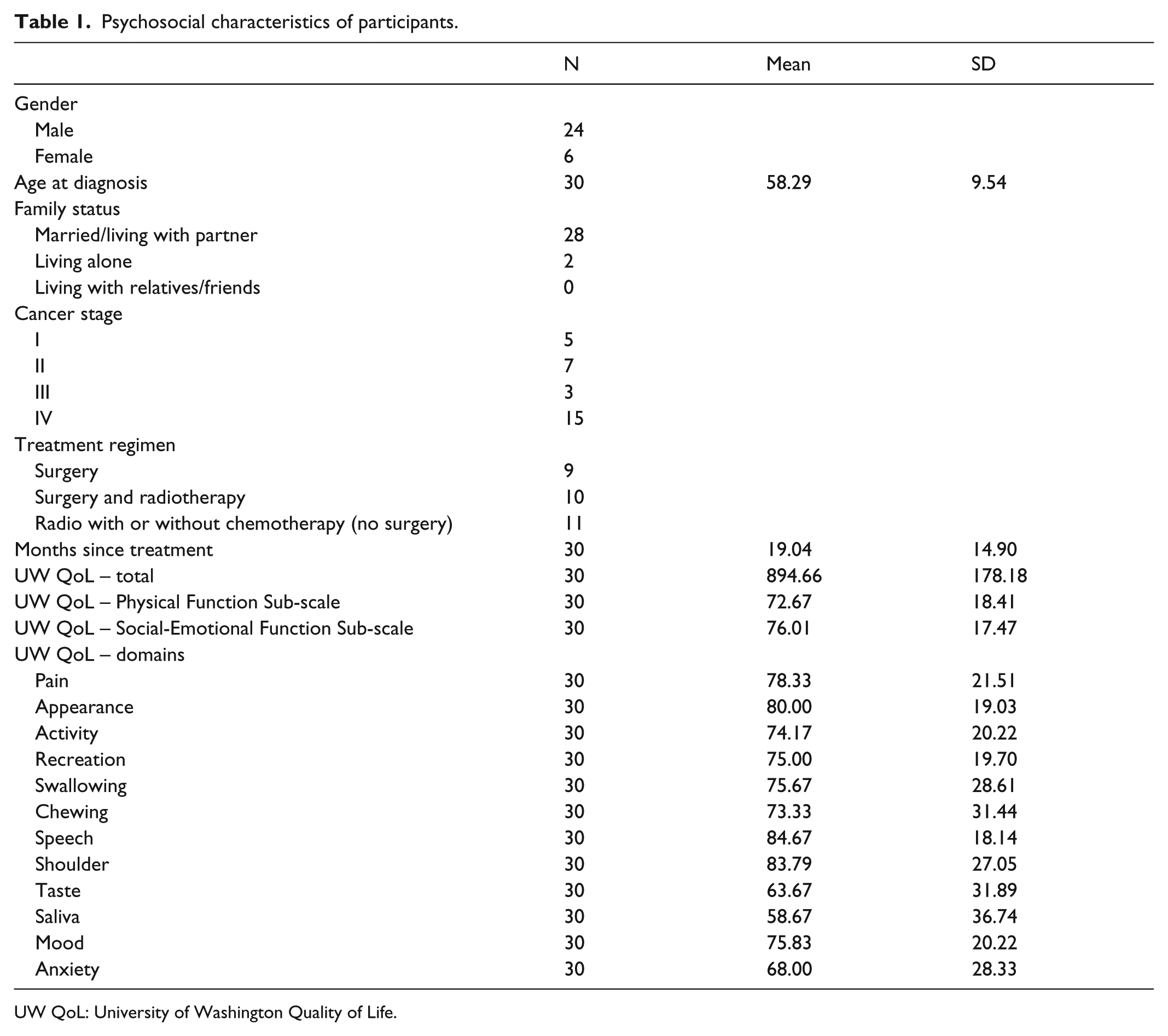
UW QoL: University of Washington Quality of Life.
Demographic data included date of birth, sex, ethnic-ity, and Index of Multiple Deprivation 19 calculated from postcode at time of diagnosis, occupation, and family status (married, living with partner, living alone, and living with relative/friends). Medical data included tumour site, stage at diagnosis, date of diagnosis, treatment, and date of treat-ment completion. Five possible treatments or combination of treatments were represented across the responders: surgery (N = 9); surgery and radiotherapy (N = 5); surgery, radiotherapy, and chemotherapy (N = 5); radiotherapy (N = 2); and radiotherapy and chemotherapy (N = 9). Four tumour locations were represented: oral cavity (N = 15), oropharynx (N = 7), hypopharynx (N = 2), and larynx (N = 6). Respondents were on average 25.79 months (range: 3–80; SD: 21.3) post-treatment.
Materials
The research used patient self-portraits as a means to elicit subjective representations in a non-verbal way. Patients were asked to produce two pencil drawings or sketches. They were provided with two sheets of A4 plain white paper and asked to do a simple pencil drawing without the use of colour. The first sheet was headed ‘How I remember myself prior to treatment for head and neck cancer’ and the second ‘How I see myself now’. This approach makes no verbal demands, which may cause discomfort to a HNC population, and operates on an entirely subjective representation. Although interviews were not planned to be included within the current research due to the study population potentially experiencing discomfort due to restricted mouth opening and/or xerostomia as a side effect of their treatment, 10 participants requested the opportunity to speak to (S.H.) to discuss their drawings and also the experience of the methodology.
The DAS24 assesses levels of distress and dysfunction in relation to cosmetic concern. Normative data are available for both clinical and non-clinical populations. 7 The DAS24 has been validated and demonstrated to have good psychometric properties. 7 All 24 items contribute well to the total score, and internal consistency is high (α = 0.92) and test–retest reliability (6 months) is good (r = 0.82). 7 The DAS24 has also been identified as a measure that shows promise as a research tool for improving understanding of how appearance affects quality of life (QOL) in HNC patients. 20
The UW QoL scale is a disease-specific broad measure of HRQoL for use with people who have had HNC. It has good patient acceptability, practicality, validity, reliability, and responsiveness. 21 The UW QoL covers 12 domains: pain, appearance, activity, recreation, swallowing, chewing, speech, shoulder function, taste, saliva, mood, and anxiety. It also has two sub-scales: physical functioning and social-emotional functioning. The UW QoL has been validated by comparison to the Karnofsky scale and Sickness Impact Profile, demonstrating an average criterion validity of 0.85. 21 It has also been found to have internal consistency between α = 0.80 and 0.79 and Test–retest of r = 0.91. 8
Procedure
One week prior to the clinic, potential participants were sent a letter inviting them to participate in the research. Included was an information sheet consent form and questionnaires. After their visit with the clinician, the researcher approached them to obtain consent. If completed, the questionnaire battery was collected and the participants were given the two sheets of white A4 paper noted in the “Materials” section above. The participants were asked to ‘draw a picture of what you think you looked like before your cancer treatment and another picture of what you think you look like now’. It was made clear that the researchers were not interested in drawing ability and that a sketch was fine. Participants that had not completed the questionnaires or did not want to undertake the drawings while in the hospital were provided with a freepost return envelope. Those participants that indicated they wanted to discuss their drawings with the researcher (S.H.) were taken into a private room and field notes taken.
To minimise observer bias, one researcher who evaluated the drawings was not present at data collection. The author undertaking the data collection was a health psychologist (S.H.) and had worked with a HNC cohort previously. While both authors were PhDs with experience in both qualitative and quantitative research methods, the second author (J.B.) had minimal experience with people who had HNC.
Statistical analysis
Data from the completed scales were entered into SPSS, version 23. Patients’ drawings were scanned and imported into National Institutes of Health (NIH) Image-J software. 22 The outside perimeters of the drawn head and neck and any part of the head and neck drawn as damaged were traced and their areas, in pixels, computed by the software, and this was entered into SPSS. The percentage of the area drawn as showing change (damaged) was calculated by dividing the damaged area by the total area of the head and neck.
Wilcoxon tests were used to investigate whether those patients whose drawing included damage differed from those who did not draw damage. Spearman’s rank correlation coefficients were calculated to investigate the relationships between the percentage of the head and neck drawn as damaged.
Qualitative analysis
Each drawing was qualitatively assessed by identifying prominent features in a similar fashion to that described by Broadbent et al. 23 The authors independently evaluated each drawing and recorded their notes prior to discussion. A short discussion was held for each drawing to explore any features that might be particularly important or noteworthy, such as size of the graphic or the boldness of the line. The initial assessments were used to develop a framework group of features related to the drawings, for example, the size of drawings and facial expressions/emotions. Field notes written during and directly following each (N = 10) discussion with patients were reviewed with content analysis.
Results
Wilcoxon tests on age at time of diagnosis, gender, tu-mour staging, treatment regimen, or responses to the questionnaires found no statistical difference between those respondents that did or did not draw any visual damage on their sketches. Table 1 shows the psychosocial characteristics of participants.
Questionnaires
Spearman’s rank rho correlations were performed on the responses obtained from the participants on the DAS24 and UW QoL, including the appearance domain of UW QoL, and no relationships were found.
Drawings
In total, 27 patients returned the drawings. Figure 1 shows examples of drawing done by the participants. Of the returned data, 23 did at least two drawings; one ‘How I remember myself prior to treatment’ and one ‘How I see myself now’. Four people simply wrote ‘No Change’ and did not do a second drawing. Mann–Whitney tests failed to reveal any difference on age, gender, or staging of tumour between those that did and did not return the drawing, or those that did not complete a second drawing.

Patient drawings.
Features of drawings
View
Of the 23 people returning two drawings, 3 of them did multiple drawings for how they see themselves now. This took the format often seen in arrest photography of one facing forward and the other from the side.
Size of drawings
NIH Image-J software produces a pixel count as a proxy for area of the drawing (Table 2). Where two drawings were returned by participants, the post-treatment image was smaller than the pre-treatment picture. This was supported by statistical analysis using the Wilcoxon signed-rank test between each of the dimensions (e.g. pre horizontal length and post horizontal length), which showed significant differences between the ‘Horizontal’ dimension (z = –2.581, P ⩽ 0.010), ‘Vertical’ dimension (z = –2.094, P ⩽ 0.036), and the ‘Area’ (z = –3.068, p ⩽ 0.002), with all these dimensions getting significantly smaller following treatment.
Pixel data as proxy measure of area.

The unit of measurement for all columns excluding those containing calculated percentages and percentage change is a ‘pixel’ as defined by the Image-J software. 22
Post area drawing–pre area drawing.
An increase in drawing dimension in post-treatment drawings.
A decrease in drawing dimension in post-treatment drawings.
Facial expressions/emotions
Although three respondents wrote ‘no change’ on their second picture and a further three showed neutral emotions unchanging between pictures, other respondents clearly depicted a change in emotion between drawings, sometimes with the addition of text to provide clear understanding. The authors independently rated the emotions shown in each drawing and then discussed their thoughts and found a 100% agreement in their interpretation of the facial expressions. Table 3 shows how drawings changed in relation to the emotion shown. One picture showed the respondent crying.
How drawings changed in relation to the emotion shown.

Intensity of pen strokes/shading
Where people identify scaring or a change in shape, they use thicker/heavier/shaded penmanship and often supported this highlighting with text, for example, ‘scars’. Shading was also used to show areas of change such as missing teeth.
Clarifying text
Sometimes, respondents provided interesting textual information supporting the drawing or providing additional information.
One person wrote, ‘Sorry, but I put the operation on the right side, and it should have been on the left side’. Where another person added explanatory text on their pictures; on the first picture ‘almost always happy’ and on the second ‘almost always depressed’
Not all texts were apologetic or negative. One person wrote, ‘I’m hopeless at art. “FAT” 19 stone’, followed by on the second picture, ‘Great 10’ 6lbs looking good’.
Most frequently, people provided short phrases often with arrows to highlight areas of change such as patchy beard, scar, no teeth, and dimple in chin due to where scare starts.
Drawings and questionnaires
Spearman’s rank correlation coefficients did not find any significant relationship between the size or percentage of the area of facial damage in the drawings and any of the questionnaires totals or sub-scale scores.
Field notes
A total of 10 people spoke to the researcher about their drawings. These discussions fell into two areas: (1) interpreting the content of the drawings and (2) the experience of the methodology.
Interpreting the content
Some similarities to the clarifying text were voiced; ‘I’m rubbish at drawing’. Others wanted to discuss what they had included in the picture and why. For example, one lady talked about how her first drawing (Figure 1) was ‘striding out’ and how this showed that she liked exercise and ‘getting out and meeting with people’. The second drawing showed how she currently felt ‘meh’ and did not really want to go out and meet with people. This indicated that the drawing allowed for more information beyond that of appearance to be communicated.
Participants also commented on how they liked the ‘freedom to draw’ what they wanted rather than it being prescriptive. Although one person did say that they ‘draw what I thought you [the researcher] would be most interested in’ and went on to describe the content of the post-treatment image, size of the scaring and then how they felt about the treatment and their hopes for the future and symptom improvement.
Experience of the methodology
One gentleman who had undertaken the drawing and questionnaires at home returned them during his next clinic visit. He became emotional once in the private room, saying, ‘I’ve never been given the chance to express myself this way. I felt kinda awkward, but it meant that I ended up drawing stuff I have not been asked about and have not felt able to talk about before’. Others drew a comparison to interview studies or clinic visits and related how this exercise gave them a chance to think about things in a different way before seeing the clinical team or researcher and to include things that were important to themselves.
A couple of people commented that ‘It would have been great to have been able to use colour’, but that they would have to be given the pencils as it is not something they have at home.
Overall, participants said that ‘drawing is fundamentally more enjoyable that ticking boxes’ and that ‘I enjoyed the process. Doing something a bit different opens up new ways of exploring my experience of cancer’. They also suggested that if this methodology was going to be used with everyone that it ‘needs to be voluntary, because although I enjoyed it, I am sure some people would hate it’ and that being given time to talk the clinician through the picture is also vital as ‘they might not get it, you know what I have drawn and why it’s important’.
Discussion
The aim of the reported research was to use the novel methodology of drawing and investigate if the images relate to traditional responses from patient-completed questionnaires in a HNC population. No statistical relationship was found between the questionnaire totals or the appearance domain of the UW QoL or size elements of the drawings.
Although some of the participants did not complete a second drawing, reporting no change in their appearance, no-one indicated to the researcher at the time of consenting, during the process, or on the returned forms that drawing was an invalid request and not relevant to their experience of HNC. The lack of statistical agreement and the details found in the drawings indicate that the method of data collection has a direct bearing on the information communicated by the participant.
The UW QoL scale describes important daily living dysfunction or limitations that patients complain of as part of HNC or due to its treatment effects, whereas the DAS24 provides an opportunity for the respondent to recognise self-conscious elements of appearance. It focuses on the distress and dysfunction arising from body image disturbance. The patients’ visual representations revealed personal and emotional accounts of their illness experience and demonstrated potential for benefits for patients. By facilitating richer data collection, drawing has been shown to be a powerful adjunct to traditional questionnaire data. The authors’ observations are consistent with Guillemin’s, 24 who claims that, despite some disadvantages, drawings, as a research method, are a means to gain the insight into a patient’s world and a source of information about many aspects of illness.
Previous studies investigating the use of drawing as a research tool have found that when face-to-face interviews supplemented data from drawings, they highlight how the interview provides an opportunity to initiate further discussions. 24 This is supported in the presented research through not only the inclusion of clarifying text but also the informal discussions requested by a number of participants. Care needs to be exercised where researchers interpret participants’ drawings without the artists input. Although formal interviews were not conducted, general conversation was entered into if initiated by the patient. It was clear from these interactions that the participants found that the drawings function as a catalyst, which helped them reflect and articulate things that they had previously found difficult to define or discuss.
These informal observations and discussions informed the drawing analysis. It was interesting to note that while the authors agreed on the drawing analysis, evaluating without additional context did elicit further questions around meaning and interpretation and the impact a post-analysis interview would have had had it been possible with the patient group. It would be of interest in future to undertake a formal interpretive interview with patients which takes into account the potential discomfit caused by treatment side effects.
Limitations
There are a number of limitations in this work, the most notable of which is the sample size. As an exploratory study to assess the use of this methodology in a HNC cohort, 30 participants represented an attainable figure in the possible time frame. It also closely matched the median average number of 32 participants (range: 4–160) from previous drawing research. 17 However, the sample in this research did not provide sufficient data to allow for statistical analysis between the questionnaires and the drawing data. A further challenge was the sampling strategy used. While the opportunistic sample did match the gender split and gave a representative range of cancer stages and treatment regimens for people that had been diagnosed with HNC, 18 greater insight into a patient’s perception or understanding may have been elicited if a purposive or stratified sample had been sought. An element of the methodology which could have introduced bias into the data is the location where the drawings were undertaken. In the presented research, participants could complete the drawings in the clinical environment or at home. This could mean that respondents in a clinical setting report less negative factors in order to maintain positive relationships with the clinical team and that those undertaking the research at home spend more time considering their responses. Before undertaking future research using drawing with a HNC cohort, the authors suggest working with the patient cohort to refine the methodology and to include a more prescribed data collection protocol, informed by the patients experiences of when, where, and how often drawing and questionnaire data should be requested. In this study, a number of participants sought out the opportunity to speak with the researcher following their completion of the questionnaires and drawing; this, to some extent, allowed the research to check their interpretation of the drawing and to reflect back the participants’ means. However, a formal participant check was not undertaken at the end of the data analysis, and this would need to be addressed taking the work forward.
The way in which participants were encouraged to draw could have influenced the findings obtained. In this study, people were asked to do a simple pen or pencil drawing and not to use colour. However, as shown by Michie and Abraham, 25 the different elements of a study’s design can affect participant behaviour. Increasing the range of drawing materials available to the drawers would provide options for expression, for example, colour may reduce the use of crosshatching or heavily drawn line to highlight an area. Requesting a drawing of a specific area of the body can target a particular topic of research interest, while a general drawing request can be open to interpretation. The latter option allows freedom of expression but can lead to uncertainty among participants about what to draw and may add in additional variables to be interpreted within research. Although reassurance that the activity was not an assessment of drawing skill was given to the participants in the presented research, it is likely that it may be insufficient to overcome, at least some, participants’ initial hesitation to draw.
Interventions which incorporate imagery are already present with the cancer setting. For example, guided imagery where participants are felt to gain an increasing sense of control over cancer-related pain and anxiety using mental images 26 and art therapy as a medium through which stress may be reduced 27 and emotions expressed. 28 This study shows that drawing may be a useful method for eliciting conversations during clinic visits.
This study invited a before and after drawing, done in a single sitting. Future work should consider additional time points post-treatment and drawings conducted over multiple sittings. Further work with members of the patient cohort would allow researchers and clinicians to identify which members of the multi-disciplinary team would be best to initiate the drawing, when, to which patients, and in what context.
Previous research of drawings over time of non-clinical people has observed that structural and formal aspects of drawing size, line, and placement are less subject to variability than content, such as body details, clothing, and accessories. 29 Whether an individual makes their figure large or small, where they place it on the page, what the essential proportions of the figure are, whether symmetry is observed, or shading is used are all features that have been shown to be stable in the non-clinical population. 29 It is especially interesting to note in this study that all the post-treatment drawings were smaller than the ‘before cancer’ drawings. It could have been hypothesised that the post-treatment drawings would have been larger than the pre-cancer ones, allowing for greater area to depict areas of change. However, as this was not the case, it may be that the respondents were fatigued following the completion of the questionnaires and the first drawing and the second one was undertaken more quickly. The authors do not think this is the case, due to the detail added to the second picture. Further investigation with a larger sample may find a relationship with the severity of the tumour or the nature of the treatment regimen.
It has been suggested that drawings can uncover multiple dimensions of living with disease, especially psychosocial, 30 and this can provide healthcare professionals with a suggestion of how the patient is coping with their illness. This creativity involved in drawing offers patients a way to express themselves, which can minimise healthcare professionals’ imposition of their own views. Drawing can also have potential benefits for patients. Drawing can be an informal opportunity to offer time and space for reflection; for some patients, this activity can access perceptions and emotions which may have been unknown previously. The uncovering of buried or unacknowledged aspects that may be causing distress could help patients better understand their post-treatment selves and needs. Not all patients will benefit from or be comfortable with one technique. However, drawing is another way for people, especially those who are visually or creatively orientated, to represent themselves.
Conclusion
This study suggests that drawing elicit distinctly different information and understanding about a person’s body image following treatment for HNC than provided by HRQoL questionnaires. Further research is needed to clarify if clinical opinion matches the patients’ drawing and if drawings would be feasible in a clinical appointment.
Footnotes
Acknowledgements
The authors would like to thank Dr T.P. Moss for his support with the development of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from local (Bristol) NHS regulatory body (REC reference no. 10/H0107/24).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was self-funded by the lead author.
Informed consent
Written informed consent was obtained from all subjects before the study.