
Abstract
Superficial myofibroblastoma of the lower female genital tract is a rare benign, recently recognized neoplasm that mostly affects the vulvovaginal area. Our report discusses a case of cervical superficial myofibroblastoma of the lower female genital tract in a 45-year-old patient who is presented with menometrorrhagia. On examination, she had multiple uterine fibroids and a circumscribed submucosal mass lesion involving the anterior lip of cervix. At hysterectomy, histopathological examination of the cervical mass revealed a relatively hypocellular tumor consisted of bland spindled and stellate cells. An immunohistochemistry evaluation revealed reactivity for CD34, desmin, and smooth muscle actin. This neoplasm should be included in the differential diagnosis of cervical mass lesions. This tumor also needs to be differentiated from other mesenchymal lesions of lower female genital tract.
Introduction
Over the last 15 years, a characteristic tumor of the lower female genital tract has been recognized in the literature. 1 This distinctive tumor has been named as either superficial cervico-vaginal myofibroblastoma (MFB) or superficial MFB of the lower female genital tract (SMFGT). This tumor has been classified as one of the mesenchymal tumors that are relatively specific to the lower female genital tract, such as aggressive angiomyxoma, angiomyofibroblastoma (AMF), and cellular angiofibroma.2,3 SMFGT typically arises from the subepithelial stroma of the vagina (41 cases have been described) and, less frequently, of the vulva (5 cases have been described) and cervix (4 cases have been described).1,4–6 Only one case has been described in the ovary 7 and only one case has been reported during pregnancy. 8 Its clinical presentation has been described as a polypoid or nodular mass of variable size (2–65 mm) in women ranging in age between 23 and 80 years.1,4,5 The pathogenesis is still unknown; however, it may be hormone-related, as a substantial number of cases had been administering tamoxifen.1,4,9 No association with viral infection, for example, human papillomavirus (HPV), Epstein–Barr virus (EBV), or human herpesvirus 8 (HHV8), has been found. 10 Histologically, the tumor has variable cytologic features and growth patterns. The tumor is un-capsulated, though, well-circumscribed. It is superficial, where it is separated from the overlying epithelium by a rim of collagenized stroma (“grenz zone”). 11 It is typically composed of ovoid, stellate to spindle-shaped cells; arranged in variable patterns including lace-like, reticular, or sieve-like pattern; and settled in a fine collagenized stroma.1,2,4 Mitotic activity is minimal or absent. 11 There has only been one case reported to have distinct pseudosarcomatous morphology suggested by nuclear pleomorphism and hyperchromatism of the tumor cells. 12 Myofibroblastic differentiation is strongly suggested by reactivity for desmin and α-smooth muscle actin (α-SMA).1,4,5 Majority of the tumors were also positive for CD34, vimentin, estrogen, and progesterone receptors, whereas staining of the tumors with calponin, CD99, and bcl-2 was variable and inconsistent. 11 There have been two cases reported, harboring ectopic, extra-uterine glands with expression of mammary markers (mammaglobin and GCDFP-15) or prostatic markers (prostate-specific antigen (PSA) and prostate-specific acid phosphatase (PSAP)).9,13 Clinically, the tumor has a benign course with no evidence of metastasis or recurrence with follow-up up to 20 years1,4 with the exception of one vaginal case where local recurrence developed 9 years after initial incomplete excision.5,11
Case
Clinical history and examination
A 45-year-old African American female, gravida 4, para 2, presented with a 5-month history of menometrorrhagia. She has denied any hormonal therapy in the past, her Pap smear was up-to-date and normal, and there was no history of sexually transmitted diseases. She was not pregnant and denied any significant current or past medical conditions. The rest of her history and system review was within normal limits.
There was no abnormalities detected in the general and systematic examination. The gynecologic examination revealed a well-circumscribed submucosal mass that was about 4 cm in size, involving the anterior lip of the cervix which was clinically consistent with a cervical fibroid. The uterus was enlarged, 15–16 weeks in size, with irregular contour that was consistent with multiple uterine fibroids.
Transvaginal ultrasound examination revealed multiple uterine fibroids, the largest being 4 × 5 cm. An endometrial biopsy revealed a proliferative endometrium with no hyperplasia or malignancy identified.
The patient underwent a total abdominal hysterectomy which was uneventful. The uterus submitted to the Department of Pathology for intraoperative consultation, to evaluate the cervical lesion as well as for a subsequent full pathological evaluation. The patient postoperative course was also deemed uneventful.
Tumor pathology and immunohistochemical analysis
The specimen was fixed in formalin 10% and embedded in paraffin. The slides were stained with hematoxylin and eosin. Immunohistochemistry was done for desmin (clone DE-R-11), α-SMA (clone 1A4), CD99 (clone O13), and CD34 (clone QBEnd/10) per standard procedures on the Ventana Benchmark Ultra machine.
Gross examination showed a 3.8 × 2.5 × 2.5 cm pink-tan-circumscribed submucosal mass involving the anterior lip of cervix. The cut surfaces were homogeneous pink to tan and soft to firm, without any necrosis, induration, or infiltration (Figure 1).
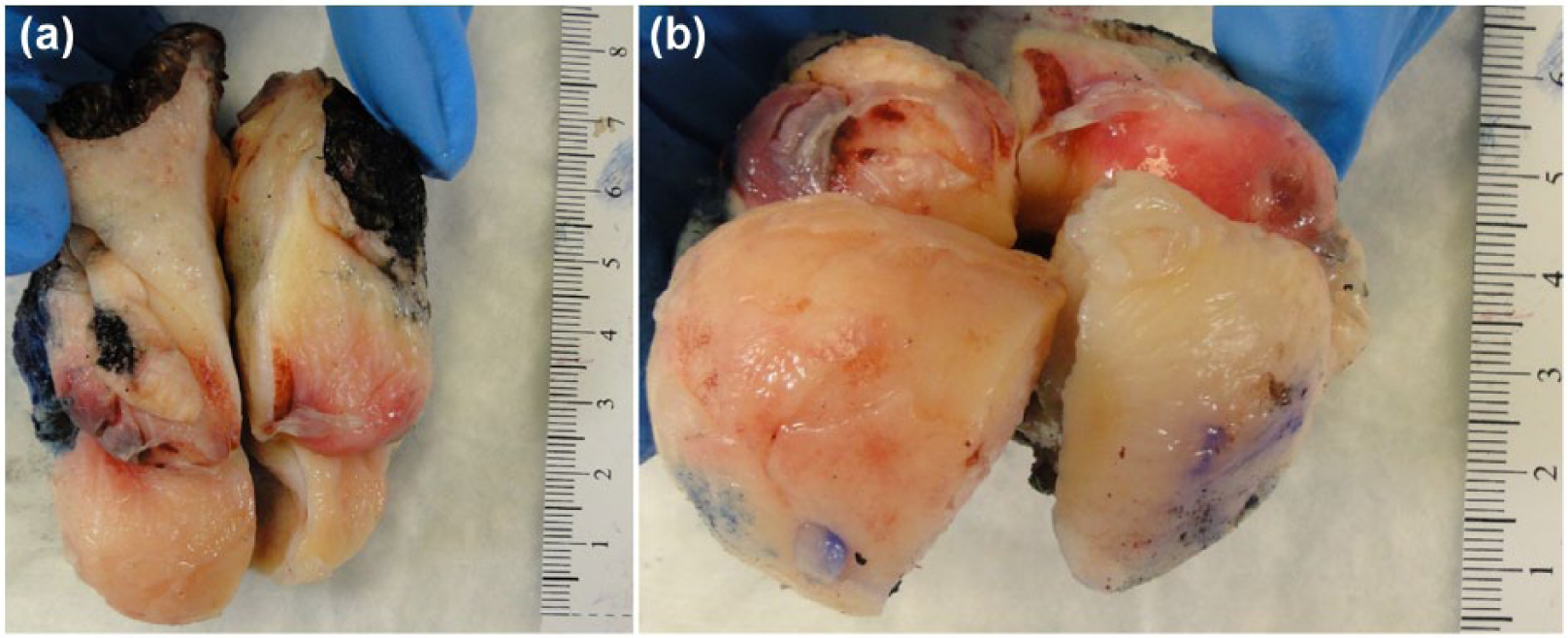
(a) and (b) A 3.8 cm well-circumscribed submucosal mass lesion involves the anterior lip of cervix and has yellow-tan and gelatinous external and cut surfaces. No hemorrhage or necrosis is identified.
Microscopic examination revealed a well-circumscribed, un-encapsulated tumor, composed of ovoid, stellate to spindle-shaped cells often with a wavy bland nuclei in an edematous, variably collagenized, hyalinized, and vascularized stroma. The vessels ranged from thick-walled vessels to capillaries, some of which were irregularly stag-horn shaped (Figure 2(a)). There was a small quantity of smooth muscle cells that were randomly intermixed. There was no mitotic activity or necrosis identified (Figure 2(b) and (c)).

(a) Neoplasm composed of relatively hypocellular ovoid, stellate to spindle-shaped cells in a patternless distribution in an edematous to myxoid, variably collagenized, and vascularized stroma. The vessels range from thick walled to capillaries some of which irregularly stag-horn shaped (H&E 50×). (b) and (c) Individual neoplastic cells are mostly stellate with bland to mildly pleomorphic hyperchromatic ovoid to spindle nuclei. No epithelioid, multinucleated, or perivascular cuffing by tumor cells is seen. No anaplasia or mitosis was identified (H&E 200×).
An immunohistochemical analysis showed diffuse positivity for desmin in spindle and stellate lesional cells (Figure 3). Staining with CD34 was positive in a large subset of spindle and stellate cells (Figure 4). Alpha-SMA staining was positive in a small subset of cells (internal control staining of vessels and smooth muscle cells noted; Figure 5). CD99 staining was non-contributory (weakly positive in some cells; most of the section washed off even on repeat stain; data not shown). Two age-matched and site-matched (anterior) non-neoplastic cervix sections from unrelated cases were used as controls (Figure 6).
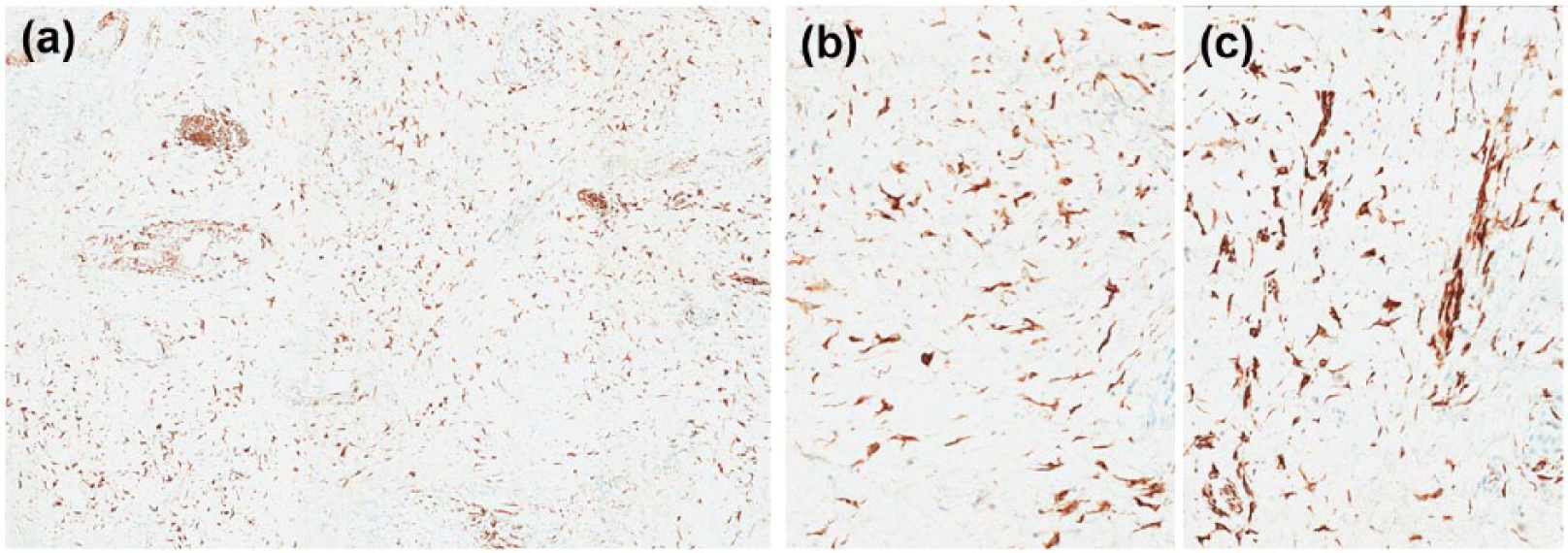
Neoplastic cells exhibited diffuse immunopositivity for desmin in spindle and stellate lesional cells: (a) desmin 50× and (b and c) desmin 200×.

Staining with CD34 was positive in a large subset of spindle and stellate cells (CD34 200×).

Smooth muscle actin staining was positive in a small subset of cells (SMA 200×).

Two age-matched and site-matched (anterior) non-neoplastic cervix sections from unrelated cases used as controls: (a and b) H&E 200×, (c and d) desmin 50×, and (e and f) desmin 200×.
Discussion
To this date, there have only been four cases of superficial MFB of the cervix reported. A summary of these cases is presented in Table 1. Differential diagnosis of this clinical presentation is broad, including cervical leiomyoma, nabothian cysts, other rare benign tumors of the cervix, and cervical cancer. Imaging of the cervix can easily identify the cystic nature of a nabothian cyst. Cervical cancer typically has abnormal covering mucosa on colposcopy; and biopsy is diagnostic in these cases. Histologically, cervical leiomyoma resembles their uterine counterparts, although much less common with an estimated frequency of about 0.6% of hysterectomy specimens. Leiomyomas with myxoid/hydropic change can have hypocellular areas and resemble SMFGT. Both SMFGT and leiomyoma are characteristically well-circumscribed lesions. However, the small quantity and arrangement of smooth muscle cells in SMFGT are different from leiomyomas and, in the current case, do not support a leiomyoma. 12 The well-circumscribed appearance in this case does not support aggressive angiomyxoma14,15 or fibroepithelial stromal polyps.16,17 Both SMFGT and AMF are typically well-circumscribed, but the lack of perivascular epithelioid cells do not support AMF.18–20 The overall histologic appearance, along with extensive co-expression of CD34 and desmin, with a subset staining for SMA in our case, are most consistent with the benign superficial MFB.
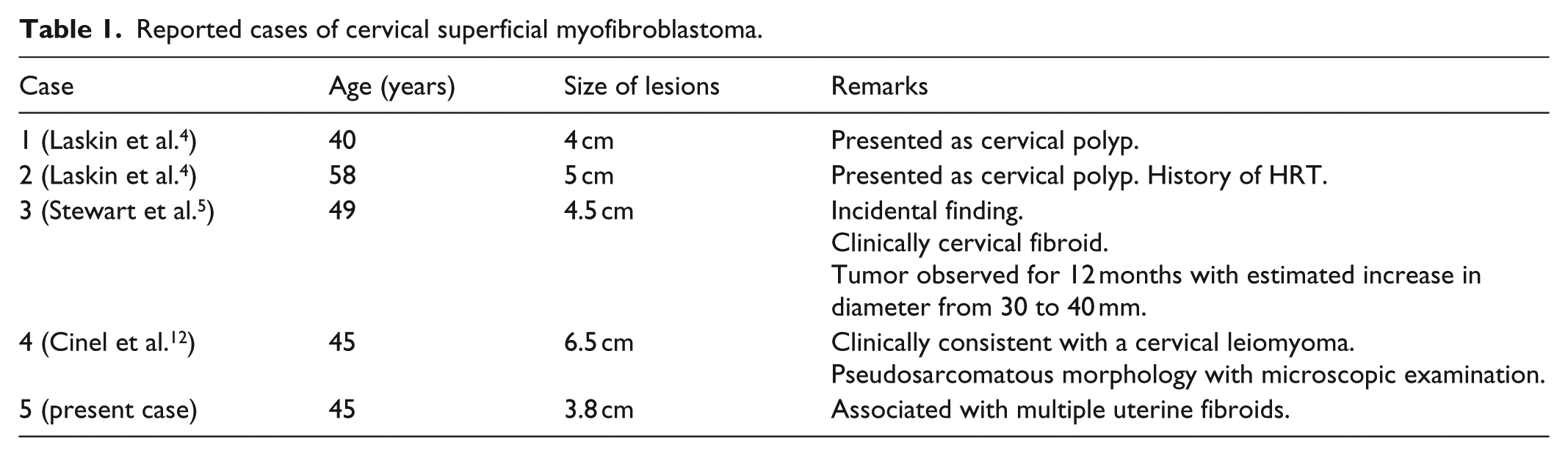
Reported cases of cervical superficial myofibroblastoma.
Conclusion
The overall findings in our case are most consistent with the rare entity of benign superficial MFB of the cervix. In our report, we introduced a literature review, reported the fifth case in the literature, and discussed the differential diagnosis of such presentation. Although this tumor is rare, it should be included in differential diagnosis of soft tissue tumors of the lower female genital tract.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for her anonymized information to be published in this article.