A flow dynamic rationale for accelerated vascularized composite allotransplant rejection
Nicholas L Robbins1,2, Matthew J Wordsworth1, Bijaya K Parida1, Bruce Kaplan3, Vijay S Gorantla1,4, Erik K Weitzel1,5 and Warren C Breidenbach1
1RESTOR™ Program, 59th Medical Wing, JBSA Lackland AFB, San Antonio, TX, USA
2UT Health San Antonio, San Antonio, TX, USA
3Baylor Scott & White Health, Dallas, TX, USA
4Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC, USA
5San Antonio Military Medical Center, JBSA Fort Sam Houston, San Antonio, TX, USA
Background: The first modern vascularized composite allotransplants were a daring series of knee joint transplants carried out between 1996 and 2004.1–7 All six knee joint transplants were lost within 56 months. A similar loss of a hand transplant took place in Louisville. The definitive etiology for the losses remains a mystery. Without a clear explanation, as to why these failed, knee joint transplants have ceased.
Methods: All data were collected from two teams, one in Germany and the other in Louisville. The population under study is the six knee TXs and one HT. The factor of interest is the long donor artery that was used in all these cases. To our knowledge, these are the only vascularized composite allotransplants completed using a donor artery greater than 25 cm. The outcome measurements are the knee and HT survival time and histology.
Results: There are only seven published vascularized composite allotransplant cases where a long donor artery (>25 cm) was used. In all cases, the vascularized composite allotransplants were lost. The etiology of these vascularized composite allotransplant losses remains unexplained. The long donor artery suffered not only from T cell–mediated rejection but also ischemia secondary to the mandatory separation of the EVV from the donor artery.
Conclusion: We hypothesize that the length of the donor artery resulted in ischemia and IH, leading to loss of the windkessel effect producing loss of the vascularized composite allotransplant. By solving this mystery, we hope to make knee joint transplants a safe and viable option for joint reconstruction.
References
1. Hofmann GO, Kirschner MH, Wagner FD, et al. Allogeneic vascularized transplantation of human femoral diaphyses and total knee joints–first clinical experiences. Transplant Proc 1998; 30: 2754–2761.
2. Hofmann GO, Kirschner MH, Brauns L, et al. Vascularized knee joint transplantation in man: a report on the first cases. Transpl Int 1998; 11(Suppl 1): S487–S490.
3. Kirschner MH, Menck J, Hennerbichler A, et al. Importance of arterial blood supply to the femur and tibia for transplantation of vascularized femoral diaphyses and knee joints. World J Surg 1998; 22: 845–851; discussion 852.
4. Diefenbeck M, Nerlich A, Schneeberger S, et al. Allograft vasculopathy after allogeneic vascularized knee transplantation. Transpl Int 2011; 24: e1–e5.
5. Hofmann GO and Kirschner MH. Clinical experience in allogeneic vascularized bone and joint allografting. Microsurgery 2000; 20: 375–383.
6. Diefenbeck M, Wagner F, Kirschner MH, et al. Management of acute rejection 2 years after allogeneic vascularized knee joint transplantation. Transpl Int 2006; 19: 604–606.
7. Diefenbeck M, Wagner F, Kirschner MH, et al. Outcome of allogeneic vascularized knee transplants. Transpl Int 2007; 20: 410–418.
Is skin the most allogenic tissue in vascularized composite allotransplantation and a valid monitor of the deeper tissues?
Nicholas L Robbins1,2, Matthew J Wordsworth1, Bijaya K Parida1, Bruce Kaplan3, Vijay S Gorantla1,4, Erik K Weitzel1,5 and Warren C Breidenbach1
1RESTOR™ Program, 59th Medical Wing, JBSA Lackland AFB, San Antonio, TX, USA
2UT Health San Antonio, San Antonio, TX, USA
3Baylor Scott & White Health, Dallas, TX, USA
4Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC, USA
5San Antonio Military Medical Center, JBSA Fort Sam Houston, San Antonio, TX, USA
Background: Since the 1960s, skin has been considered to be the most allogenic tissue in humans. This tenant has remained unquestioned in the reconstructive transplant arena which has led to skin serving as the sole monitor for early rejection in vascularized composite allotransplantation. In this article, we question the validity of this belief. Our hypothesis is that skin is not always an accurate monitor of rejection in the deep tissues, thus questioning the positive and negative predictive values of the punch biopsy for suspected vascularized composite allotransplantation rejection.
Methods: A literature search was carried out identifying vascularized composite allotransplantation publications where the allogenicity of transplanted skin was evaluated.
Results: A total of 18 publications claimed skin was found to be the most allogenic tissue in humans justifying it to be the superior monitor for rejection. Eight publications demonstrated skin to be a poor monitor of rejection deeper to the skin. Two vascularized composite allotransplantation animal studies demonstrated skin rejecting simultaneously with the deeper tissues. Finally, three publications exemplified a skin and kidney allograft transplanted simultaneously indicated skin allogenicity was equivalent to that of the kidney allograft.
Conclusion: Much of the literature in human vascularized composite allotransplantation claim skin to be an excellent monitor of the deep tissues. The conclusion from this study is that skin does not always function as a good monitor for what could be rejecting in the deep tissues. We believe continued research is necessary in order to focus on expanding novel monitoring techniques and technologies to accurately diagnose vascularized composite allotransplantation rejection without tissue destruction.
Public Health Service increased risk donors and their potential impact on vascularized composite allograft transplantation
Cameron Robert Wolfe, Gabe Vece, Susan Tlusty, Ricardo La Hoz and Marian Michaels
United Network for Organ Sharing, Richmond, VA, USA
Background: Understanding the epidemiology of potential donors, especially with the opiate epidemic, is vital to understand infection risk and to safely expand the limited vascularized composite allograft donor pool. Donors are stratified according to the Public Health Service–increased risk assessment, given behavioral risks that are associated with acute hepatitis B/C or HIV. Wide risk variation exists in the designation, yet traditionally many have been declined by the vascularized composite allograft community.
Methods: We retrospectively reviewed the 2017 Organ Procurement Transplant Network database. We extracted vascularized composite allograft donor epidemiology, Public Health Service behavioral data, and infectious diseases screening results.
Results: Of the total 10,286 donors, 2704 (26.3%) were Public Health Service–increased risk donors, up from 11.9% in 2012. Six vascularized composite allograft transplants occurred during 2017; zero reports of unanticipated vascularized composite allograft donor-derived transmission events were received. Many donors died secondary to intravenous drug use or drug overdose, especially in the northeast United States (up to 20%–25% of all donors), yet none became vascularized composite allograft donors. Zero vascularized composite allograft donors in 2017 were Public Health Service–increased risk donors, and only 1 of 23 vascularized composite allograft donors between July 2014 and March 2018, even though the Organ Procurement Transplant Network Ad Hoc Disease Transmission Advisory Committee data reveal a low risk of inadvertent hepatitis or HIV during that time. No unexpected HIV transmissions occurred since 2009; seven unexpected hepatitis C virus infections occurred in the first 10 months of 2017, but all were from intravenous drug use donors. In donors who were hepatitis C virus seropositive, yet non-viremic, the transmissions occurred only in donors who were with active intravenous drug use. Only 8 cytomegalovirus-seropositive donors were used, including 3 cytomegalovirus donor–recipient mismatches out of 23 vascularized composite allograft recipients.
Conclusion: The rates of Public Health Service–increased risk donors continue to rise. The vascularized composite allograft community historically appears risk averse when considering these donors, as with cytomegalovirus + donors. Given the significant difference in risk between different Public Health Service–increased risk donors, there may be safe opportunities to expand the donor pool by revisiting real-world infection transmissions. Donors, other than those with active intravenous drug use or drug overdose, appear to be at very low risk. Lower cytomegalovirus utilization may reflect a desire to avoid cytomegalovirus mismatched transplants, especially, for example, in uterine vascularized composite allograft. With new cytomegalovirus prevention therapy now available, cytomegalovirus-seropositive donors can be more routinely considered.
Role of flow magnetic resonance imaging in the monitoring of facial allotransplantations: preliminary results on graft vasculopathy
Jérémie Bettoni1,2, Olivier Balédent2,3, Palmina Petruzzo4,5, Sylvie Testelin1,2, Lionel Badet5, Bernard Devauchelle1,2, Olivier Thaunat6,7, Jean-Marc Constans2,8, Jean Kanitakis9, Jérôme Duisit10, Benoit Lengele11, Emmanuel Morelon6,7 and Stéphanie Dakpé1,2
1Departement of Maxillo-Facial Surgery, University Hospital of Amiens Picardie, Amiens, France
2EA CHIMERE, Amiens, France
3Bioflow Laboratory, Amiens, France
4Department of Surgery, University of Cagliari, Cagliari, Italy
5Department of Transplantation, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
6Department of Transplantation, Nephrology and Clinical Immunology, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
7INSERM U1111, Lyon, France
8Department of Radiology, University Hospital of Amiens Picardie, Amiens, France
9Department of Dermatology, Edouard Herriot Hospital, Hospices Civils de Lyon, Lyon, France
11Department of Plastic and Reconstructive Surgery, Université Catholique de Louvain, Cliniques Universitaires Saint-Luc, Bruxelles, Belgium
Background: Chronic vascular rejection characterized by myointimal proliferation of smooth muscle cells that progressively obstruct the arterial graft lumen might become the main cause of long-term graft loss in vascularized composite tissue allotransplantation as observed in solid organ transplantation, requiring new diagnostic tools.
Methods: The objective of this study was to evaluate the usefulness of flow magnetic resonance imaging in the qualitative and quantitative monitoring of vascularized composite tissue allotransplantation in three patients transplanted between 2005 and 2012 (Figure 1). Between 2015 and 2017, seven flow magnetic resonance imaging acquisitions were performed concurrently with standardized clinical and histological monitoring.
Results: Our study demonstrated a progressive reduction in the average flow rate and intraluminal diameter of the arterial pedicle of the grafts of 11.9 mL/min (37.7%) and 0.38 mm (15.9%) per year (Figure 2). During the follow-up, two patients developed chronic vascular rejection requiring partial resection of the graft. In these patients, flow magnetic resonance imaging acquisitions were characterized by a significant reduction in vascular signal, rendering quantitative acquisitions impossible.
Conclusion: The results of our study confirm the feasibility of reproducible, non-invasive, and non operator-dependent morphometric and hemodynamic radiological analysis providing clinicians with new information on the vascular status of vascularized composite tissue allotransplantation over time and offering the prospect of an imaging technique specific to vascular outflow.
AMD3100 as a single-dose stem cell mobilizing agent in vascularized composite allograft transplantation in a canine model
Bruce J Swearingen1,2, Scott S Graves2,3, Rainer Storb2,3 and David W Mathes1,2
1University of Colorado School of Medicine, Aurora, CO, USA
2Fred Hutchinson Cancer Research Center, Seattle, WA, USA
3University of Washington Medical Center, Seattle, WA, USA
Background: Vascularized composite allograft transplantation is a clinical reality but limited by toxicities of chronic immunosuppression and rejection. Current clinical tolerance protocols rely on recipient conditioning and donor cell mobilization limiting use to living donor transplants. We sought to design a clinically relevant protocol applicable to cadaveric organs using AMD3100 (plerixafor) as a single-dose agent for stem cell mobilization in our existing canine non-myeloablative vascularized composite allograft transplant model in both DLA-haploidentical, related and DLA-mismatched, unrelated canine donor–recipient pairs.
Method: A total of eight DLA-haploidentical, related canine recipients (Group I) and five DLA-mismatched, unrelated canine recipients (Group II) received conditioning with 350-450 cGy total body irradiation, AMD3100-mobilized donor stem cells + bone marrow aspirate transfusion, and simultaneous vascularized composite allograft transplantation with a short course of immunosuppression (mycophenolate mofetil: 56 days/cyclosporine: 70 days (Sirolimus: 28 days as third agent for Group II)). CD34+ hematopoietic progenitor cells were quantified by flow cytometry. Peripheral blood chimerism was evaluated by polymerase chain reaction weekly. Vascularized composite allograft survival was followed clinically and histologically.
Result: All 13 canines tolerated the conditioning regimen. Stem cell engraftment and donor chimerism were seen in all dogs. Mean COBE apheresis count of 4.05 × 108 cells/kg and mean bone marrow aspirate count of 1.47 × 108 cells/kg (across both groups) were obtained. Five dogs were not followed long term (>70 days) due to complications from pulmonary hemorrhage, intussusception, or graft-versus-host disease. Mean dog survival was 229 days; outcomes varied. From eight long-term survival recipients, two dogs showed evidence of acute rejection and one self-limited. Four dogs demonstrated evidence of graft-versus-host disease (skin and liver), and one was lost to pulmonary hemorrhage, all while seemingly tolerant to the vascularized composite allograft. One dog had persistent stable mixed chimerism without evidence of graft-versus-host disease or vascularized composite allograft rejection throughout the study.
Conclusion: This study demonstrates proof of principle for AMD3100 as a single-dose stem cell mobilizing agent for a clinically relevant tolerance protocol in both DLA-haploidentical, related and DLA-mismatched, unrelated donor–recipient pairs. Use of AMD3100 led to stem cell engraftment in all animals transplanted with only two canines demonstrating evidence of acute rejection in the vascularized composite allograft. AMD3100 use limited by thrombocytopenia in our previous studies continue to appear be resolved with the addition of bone marrow aspirate in this model.
Comparison of normothermic and hypothermic ex-vivo extremity perfusion
Catherine J Stewart1, Max T Buchko1, Xiuhua Wang1, Adil Ladak1, Gerald Brandacher2, Darren H Freed1 and Jayan Nagendran1
1University of Alberta, Edmonton, AB, Canada
2School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: The potential of extremity transplantation is critically limited by 4–6 h of preservation time currently offered by standard cold static preservation. Ex-vivo extremity perfusion is an evolving platform striving to safely extend the preservation time of donated vascularized composite allografts allowing for greater applicability of upper limb transplants. There is yet to be optimization of ex-vivo extremity perfusion protocols to determine ideal conditions for safe extended ex-vivo extremity perfusion preservation times. Specifically, there remains controversy whether vascularized composite allografts should be perfused at normothermia with a blood-based perfusate or at hypothermia with an acellular perfusate during ex-vivo extremity perfusion. We hypothesize that normothermic ex-vivo extremity perfusion will allow for improved vascularized composite allograft preservation during extended ex-vivo extremity perfusion protocols.
Methods: Porcine forelimbs are perfused for 12 h on a novel mobile ex-vivo perfusion system that was developed at our institution with an acellular perfusate similar to STEEN with 25% bovine serum albumin. The ex-vivo extremity perfusion protocols were stratified to limbs being perfused in either a hypothermia (10°C) group with acellular perfusate or a normothermia (38°C) group perfused with autologous packed red blood cells added to the perfusate (cellular perfusate). Parameters to be compared include the following: histological analysis of tissues, compartment pressure, muscle response to electrical nerve stimulation, edema formation, myoglobin and creatine kinase muscle (CK-MM) levels, and perfusate cytokine profiles.
Results: Initial ex-vivo extremity perfusion runs show a marked difference in edema formation with the hypothermic conditions correlating with a greater weight gain (23.16% hypothermic group vs 0.32% normothermic group). Throughout the 12-h perfusions, the normothermic group displayed muscle contraction in response to electrical nerve stimulation, comparatively muscle contraction was absent at all time points in the hypothermic group. Differences in histopathology, lactate concentrations, CK-MM concentrations, and myoglobin concentrations are also observed between groups.
Conclusion: Preliminary results indicate that normothermic conditions may be superior to hypothermic conditions when using ex-vivo extremity perfusion to preserve and potentially enhance upper limb vascularized composite allografts.
Nine-year outcomes after facial vascularized composite allotransplantation: a case report
Branislav Kollar, Sotirios Tasigiorgos, Bridget Perry, Miguel I Dorante, Anna E Rutherford, George F Murphy, Francisco M Marty, Leonardo V Riella, Stefan G Tullius and Bohdan Pomahac
Brigham and Women’s Hospital, Boston, MA, USA
Background: The long-term outcomes after facial vascularized composite allotransplantation are not well described. Here, we present the 9-year follow-up of the first patient who received partial facial vascularized composite allotransplantation at Brigham and Women’s Hospital in April 2009.
Methods: Motor function was evaluated with Daniels and Worthingham’s manual muscle testing where scores ranging from 0 (absent movement, 0% recovery) to 3 (full movement, 100% recovery) were assigned to every facial muscle. Facial sensation was assessed by two-point discrimination, calorimetric and monofilament testing. Quality of life was tested with Facial Disability Index on a scale from 0 (worst quality of life) to 100 (best quality of life) points.
Results: At 9 years, allograft motor function was restored to 66% (average of all facial muscles). The patient can discriminate two points 15 mm apart, feel pressure of 2 g monofilaments, and discriminate hot or cold sensation in the entire allograft area. Immunosuppressive therapy currently consists of tacrolimus (target levels: 6–8 ng/mL), mycophenolate (500 mg daily), and prednisone (5 mg daily), while steroids were completely weaned between 1 and 6.5 years after transplantation. One acute cellular rejection episode of grade II or higher occurred on average per year and all rejection episodes were successfully managed. Neither acute antibody mediated rejections nor persistent donor-specific antibodies were recorded so far. Chronic clinico-pathologic skin changes such as skin thinning and papillary dermal sclerosis were observed over time. Despite of hepatitis C virus treatment resulting in undetectable viral load prior to transplantation, early reactivation occurred and led to slowly progressing liver cirrhosis (most recent Model of End-stage Liver Disease score: 12). Two courses of antiviral therapy 8 years after transplantation failed to generate sustained reduction in viral load, although third course is currently ongoing with a sofosbuvir, velpatasvir, voxilaprevir, and ribavirin drug combination. Hepatocellular carcinoma at post-operative years 6 and 9 was successfully treated with local radio- and cryoablation, respectively, without evidence of progression to metastatic disease. Social/Well-Being Function score of the Facial Disability Index testing varied from 56 to 88 points throughout the follow-up.
Conclusion: Facial vascularized composite allotransplantation successfully restored significant long-term facial function. For favorable management of complications, close follow-up with multidisciplinary team and adherence to the medical treatment are crucial.
Candidate non-invasive biomarkers for face transplant rejection
Branislav Kollar1, Andrey Shubin2, Thiago J Borges1, Sotirios Tasigiorgos1, Thet Su Win1, Christine G Lian1, Simon T Dillon3, Xuesong Gu3, Iris Wyrobnik3, George F Murphy1, Bohdan Pomahac1, Towia A Libermann3 and Leonardo V Riella1
1Brigham and Women’s Hospital, Boston, MA, USA
2Harvard University, Cambridge, MA, USA
3Beth Israel Deaconess Medical Center, Boston, MA, USA
Background: Acute rejection episodes occur in more than 80% of face transplant recipients in the first postoperative year. The gold standard to diagnose rejection is the skin biopsy assessed by Banff criteria. However, Banff grading is semiquantitative and might be prone to intra- and interobserver variability. In addition, neither a correlation between histological severity of rejection and treatment response nor systemic surrogate markers of rejection in face transplantation are available for clinical routine. Therefore, we aimed to evaluate a next generation aptamer-based SOMAscan proteomics platform for non-invasive rejection biomarker discovery in face transplantation.
Methods: A total of 24 longitudinal serum samples from 6 face transplant recipients with long-term follow-up were subjected to biomarker discovery with SOMAscan. The acute rejection episodes were stratified according to the treatment response into severe (needed steroid boluses or more potent drugs for resolution) and nonsevere (resolved with topicals and/or maintenance immunosuppression adjustment) rejections. Reproducibility of the results was evaluated with ELISA (enzyme-linked immunosorbent assay).
Results: From the 1310 proteins analyzed by SOMAscan, 5 proteins (MMP3, ACY1, IL1R2, SERPINA4, and CPB2) were found to be significantly upregulated during severe rejection and could discriminate severe rejection from no-rejection samples. Technical validation on ELISA platform showed high correlation with the SOMAscan data for the MMP3 protein (rs = 0.99). In addition, MMP3 levels significantly increased during severe rejection as compared to no-rejection (p = 0.0009) and nonsevere rejection (p = 0.0173) episodes. Stratification of samples according to the Banff grades of rejection could not show any significant differences in MMP3 levels between any grades of rejection. Pathway analyses revealed significant activation of the metallopeptidase activity during severe face transplant rejection.
Conclusion: This report provides one of the first pieces of evidence that molecular non-invasive markers could enhance the diagnostic armamentarium available to clinicians who manage rejection in vascularized composite allotransplantation. Further validation in a larger independent patient cohort is needed.
Building on the expertise of the Certified Clinical Transplant Coordinator in a Reconstructive Program
Lynette Fix and Kevin Praska
Mayo Clinic, Rochester, MN, USA
Background: Certified Clinical Transplant Coordinator Registered Nurse staff have had a vital role in solid organ transplant programs. The Certified Clinical Transplant Coordinator Registered Nurse expertise is recognized in the solid organ transplant community to be integral to successful long-term transplant patient outcomes. Their role in Reconstructive Transplant Program (vascularized composite allotransplantation) development is less known.
Methods: The Certified Clinical Transplant Coordinator Registered Nurses actively served on multidisciplinary planning committees and used the American Academy of Ambulatory Care Nursing standards to develop resources that laid the foundation for the Mayo Clinic’s reconstructive transplant program. Living donor and kidney pre-transplant patient screening tools and processes were reviewed for similarities with the vascularized composite allotransplant patient screening needs. Certified Clinical Transplant Coordinator Registered Nurses developed patient education resources and patient screening or assessment tools through a collaborative approach with multidisciplinary team input.
Results: As a result of this program’s multidisciplinary collaboration, an innovative approach to screening potential vascularized composite allotransplant patients was created. The process comprised the following: a screening tool used with all patients, a phone interview conducted on all patients, a scheduled phone interview with a social worker, schedule for the patient’s first steps of evaluation, and a patient referral tool.
Conclusion: The Certified Clinical Transplant Coordinator Registered Nurses have contributed significantly to the development of a reconstructive transplantation by utilizing their knowledge, skills, and expertise gained from solid organ transplant patient populations. These nursing attributes assisted in the organization’s overall Reconstructive Transplant Program development as well as the development of an effective patient screening process.
Nicole Shockcor1, Bryan Buckingham1, Wessam Hassanein1, Benson Akinsiku2, Jeffrey Gimble3, Thomas Davis4, Eric Elster4, Arthur Nam1, Stephen Bartlett1 and Rolf N Barth1
1University of Maryland, Baltimore, MD, USA
2Uniformed Services University of the Health Sciences, Bethesda, MD, USA
3LaCell LLC, New Orleans, LA, USA
4USU Walter Reed Surgery, Uniformed Services University of the Health Sciences, Bethesda, MD, USA
Background: Adipose-derived stem cells have increased levels of anti-inflammatory and immunoregulatory factors. Murine studies have shown stable macrochimerism and long-term full-thickness skin graft survival after a co-infusion of adipose-derived stem cells and bone marrow cells. We hypothesized that co-infusion of adipose-derived stem cells and bone marrow cells with a depletional conditioning regimen would promote chimerism and prolong graft survival in an established non-human primate facial transplantation model.
Methods: Two cynomolgus macaques underwent heterotopic facial subunit transplantation from major histocompatibility complex–mismatched donors. Anti-CD4 and Anti-CD8 monoclonal antibodies were administered (50 mg/kg) on postoperative days 0, 2, 5, 7, and 14 in addition to a non-myeloablative dose of busulfan (5 mg/kg). On postoperative day 7 (20 × 106 cells/kg) adipose-derived stem cells and donor vertebral bone marrow cells were infused. Tacrolimus and mycophenolate mofetil were then administered for maintenance immunosuppression. Clinical evidence of graft rejection was assessed via gross appearance and histopathologic analysis according to Banff classification. Peripheral chimerism was determined via flow cytometry.
Results: After administration of monoclonal antibodies, CD3+ cells decreased to a mean of 44.9% of baseline, CD4+ cells decreased to a mean of 0.5% of baseline, and CD8+ cells decreased to a mean of 66.8% of baseline. Animal 1 achieved 37 days of rejection-free survival; pathology at the time of necropsy demonstrated Banff 4 rejection. Animal 2 was ongoing without gross or histopathologic evidence of rejection. The maximum level of peripheral chimerism achieved was 6.01% and 13.48% in Animals 1 and 2, respectively.
Conclusion: With the ease of acquiring adipose-derived stem cells in the clinical setting and chimerism noted in pre-clinical models, utilizing adipose-derived stem cells is a promising method for promoting tolerance and graft survival in highly antigenic transplanted allografts. Developing well-tolerated regimens that lead to improved engraftment is imperative in eliminating complications associated with high levels of long-term immunosuppression.
Using vascularized composite allotransplantation for functional reconstruction of urogenital tissue defects: a novel microsurgical penis transplant model, and clinical and histological rejection classification
Samuel AJ Fidder1,2, Georg J Furtmüller2, Brian Simons2, Barbara Kern2, Denver Lough2, Byoung Chol Oh2, Maria Chicco2, Cory Brayton2, WP Andrew Lee2, Damon Cooney2, Richard James Redett2 and Gerald Brandacher2
1Erasmus University Medical Center, Rotterdam, The Netherlands
2School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: Defects of male urogenital structures subsequent to major trauma are associated with severely reduced function and quality of life. Recently, penis transplantation represents an exciting avenue for restoration of male urogenitalia. However, little is currently known about the immunological features of these grafts. To fill this void, we established a new animal model, and clinical and histological rejection classification.
Methods: In male Brown Norway and Lewis rats, the penis was dissected to design a penile graft including prepuce skin. A non-suture cuff technique was employed for the anastomosis of the graft vessels to the recipient inferior epigastric vessels. A total of 30 syngeneic and allogeneic transplants were performed. Grafts were followed clinically and histologically at post-operative days 3, 5, 7, 9, 11, 13, 14, 16, and 18.
Results: The graft design using anastomosis of the dorsal penile vein and the internal pudendal artery yields optimal perfusion of all graft tissues. The non-suture cuff technique allows for successful anastomosis by a single surgeon in an average of 2.5 h (91% surgical success rate). Long-term graft survival (>45 post-operative days) was observed in syngeneic transplants. Graft rejection follows a four-stage clinical progression, with all untreated allografts fully rejected by post-operative day 16. Histological analysis allowed for the development of a specific four-grade rejection classification in analogy to the 2007 Banff criteria for hand transplantation. Of note, graft skin and urethral lining tissue are first targets of rejection, which follows a distal to proximal pattern.
Conclusion: We established a robust and reproducible murine model to study the immunobiology of urogenital tissue in the context of transplantation. The graft design ensures vascular perfusion of all penile tissues and allows for standardized visual monitoring of graft viability. We propose a novel four-grade histological rejection scale based on graft skin and urethral lining as the main targets of rejection.
Patterns of rejection in porcine vascularized composite allografts using clinical, histologic, and immunohistochemical analysis
Michael Grzelak1, Joanna Wolf Etra1, Georg J Furtmüller1, Felix Naegele1, Ali Ahmadi1, David Meyerholz2, Sarah Beck1, Damon Cooney1, Inbal Sander1, Cory Brayton1 and Gerald Brandacher1
1School of Medicine, Johns Hopkins University, Baltimore, MD, USA
2School of Medicine, University of Iowa, Iowa City, IA, USA
Background: Vascularized composite allotransplantation is an advancing field that provides a valid therapeutic option for patients suffering from traumatic tissue loss. Toxicities resulting from the chronic immunosuppressive therapies after transplantation are common, however, and in order to widen the clinical applicability of vascularized composite allotransplantation, specialized labs throughout the world are working to develop therapeutic regimens with lower side-effect profiles. While animal models are a necessary part of this research, there are very few papers that have performed an in-depth analysis of the rejection patterns in these animal models. In this study, we performed a comprehensive analysis of swine hind-limb model using clinical, histologic, and immunohistochemical comparisons to both describe the overall rejection patterns seen in vascularized composite allotransplantation tissues and characterize swine vascularized composite allotransplantation rejection.
Methods: A detailed clinical, histologic, and immunohistochemical examination of rejection in the swine vascularized composite allotransplantation model was performed, and inflammatory infiltrations were characterized in both skin and lymphoid tissue.
Results: Although the mouse vascularized composite allotransplantation model is more cost effective, the swine vascularized composite allotransplantation model is the best pre-clinical model because of its similarity to human vascularized composite allotransplantation tissue with regard to tissue architecture, clinical appearance, and progression to clinical rejection. Among rejection samples, grafts that are in histologic grade-3 rejection (according to the 2007 Banff criteria) showed profound CD3+ and FoxP3+ cell infiltration with sparse B cell infiltration, and grafts that were in histologic grade-4 rejection were mainly infiltrated by neutrophils in the epidermis while lymphocytes were densely localized to perivascular regions. Further immunohistochemical comparisons between models as well as an in-depth analysis of swine lymphoid tissue in rejecting animals are ongoing.
Conclusion: In the swine model, rejecting samples tended to have inflammatory patterns that were largely T cell-dominated, with both T effectors and T regulatory cells densely populating the tissues.
Seth Jason Concors1, David Aufhauser1, Zhonglin Wang1, Guanghui Ge1, Tricia Bhatti2, L Scott Levin3, Wayne W Hancock2 and Matthew H Levine1
1University of Pennsylvania, Philadelphia, PA, USA
2Children’s Hospital of Philadelphia, Philadelphia, PA, USA
3Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
Background: Vascular composite allotransplantation of the limb involves cold and warm ischemia, further limiting organ availability beyond the constraints of blood type, human leukocyte antigen compatibility, age, size, skin color, and gender. No therapy exists to mitigate ischemia reperfusion injury. We have previously demonstrated that histone deacetylase inhibition (HDACi) mitigates renal ischemia reperfusion injury, and we wished to assess the impact of HDACi on limb ischemia reperfusion injury tolerance.
Methods: Female wild-type C57BL/6 mice were treated with pan-HDACi trichostatin A, class I HDACi (MS-275), HDAC6i (tubastatin A), or control (dimethyl sulfoxide) at 16 h and 30 m pre-ischemia reperfusion injury. Mice were subjected to 55 m of unilateral limb ischemia under strict temperature control at 36.5°C. Ischemia was performed with the placement of a dental band just proximal to the knee joint, with complete vascular occlusion and subsequent band lysis. Histopathologic analysis was conducted at 24 h post injury and scored based on muscle necrosis and granulocyte demarcation. Contralateral limbs served as internal controls.
Results: Trichostatin A and tubastatin A pre-treatment yielded protection from limb warm ischemia reperfusion injury, with significantly decreased muscle damage (p < 0.05 and p < 0.001, respectively). No differences were observed in inflammatory infiltrate between groups.
Conclusion: Pan-HDAC6i mitigates limb injury after ischemia reperfusion injury. Further studies will focus on HDACi protection from cold ischemia in a vascular composite allotransplantation model, and the use of additional endpoints such as tissue perfusion imaging is underway.
CXCR4+ Foxp3+ Treg cells resident within donor bone marrow are essential for costimulation blockade-induced long-term survival of murine limb transplants
Wayne W Hancock1, Liqing Wang1, L Scott Levin2 and Matthew H Levine3
1Children’s Hospital of Philadelphia, Philadelphia, PA, USA
2Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
3University of Pennsylvania, Philadelphia, PA, USA
Background: Vascularized composite allotransplantation procedures that include donor bone marrow cells are of particular interest, given concerns these cells may promote graft immunogenicity or provoke graft-versus-host disease. As a result, depletion of donor bone marrow cells might be expected to enhance vascularized composite allotransplantation survival.
Methods: We used murine models of heterotopic and orthotopic limb transplantation (BALB/c → C57BL/6) to assess the efficacy of peri-transplant therapy in achieving long-term vascularized composite allotransplantation survival.
Results: Injection of CD40L mAb and donor splenocyte transfusion (5 × 106 cells), plus 30 days of rapamycin (2 mg/kg per day), induced long-term vascularized composite allotransplantation survival (>100 days, p < 0.01). Similarly, CTLA4Ig (500 µg, i.p., on days 0, 2, and 4) plus rapamycin also induced long-term vascularized composite allotransplantation survival (>100 days, p < 0.01). The success of either protocol required the presence of a bone-associated, radiation-sensitive component since removal of the long-bone or pre-transplant donor irradiation (800 cGy) prevented long-term allograft survival. Efficacy also required a T- or B-cell component since allograft rejection occurred when Rag1-/- donors were used. Long-term allograft acceptance could not be restored by infusion of donor bone marrow cells peripherally at the time of engraftment (p < 0.05). Use of a CXCR4 inhibitor to mobilize donor bone marrow cells pre-transplant abrogated the efficacy of either protocol (p < 0.01). Analysis of donor bone marrow showed that ~40% of CD4+ T cells were Foxp3+ Treg (regulatory T) cells, constituting the largest population of Treg cells within the immune system. Finally, donor Treg cell depletion by diphtheria toxin administration to DEREG donor mice (whose Foxp3+ Treg cells express the diphtheria toxin receptor) restored rejection with either protocol, whereas without Treg cell depletion, long-term survival was associated with an active trilineage bone marrow.
Conclusion: Long-term vascularized composite allotransplantation survival is possible across a full major histocompatibility complex disparity using costimulation blockade-based approaches. Surprisingly, the efficacy of costimulation blockade in these models depends on the presence of a population of radiation-sensitive, CXCR4+ Foxp3+ Treg cells resident within donor bone marrow cells. The mechanisms by which these cells promote vascularized composite allotransplantation survival post-transplant, including migration of donor Treg cells to recipient lymphoid tissues, and the interactions of recipient lymphoid cells with donor bone marrow cells resident within long-bones, are under investigation.
Ex vivo expanded regulatory T cells combined with short-term costimulation blockade prevent rejection of vascularized composite allografts
Byoung Chol Oh1, Georg J Furtmüller1, Michael Grzelak1, Linh Vuong2, Marcos Iglesias1, Madeline Fryer3, Damon Cooney1, WP Andrew Lee1, Giorgio Raimondi1 and Gerald Brandacher1
1School of Medicine, Johns Hopkins University, Baltimore, MD, USA
2School of Medicine, Washington University in St. Louis, MO, USA
3University of Massachusetts Medical School, Worcester, MA, USA
Background: Routine clinical application of vascularized composite allografts is hampered by the toxicity of long-term maintenance immunosuppression. This study investigated a novel approach using ex vivo expanded Treg (regulatory T) cells combined with a short-term immunomodulatory strategy in a murine hind-limb transplantation model.
Methods: Fully major histocompatibility complex–mismatched orthotopic hind-limb transplants were performed from BALB/c to C57BL/6 mice. Recipients in the experimental groups received a combination regimen consisting of 0.5 mg CTLA4-Ig on days 0, 2, 4, and 6 post-transplant; T-cell depletion on postoperative day 1; and 1 mg/kg rapamycin (postoperative days 0–9), and in one group, 1-week expanded CD4+ CD25+ Treg cells. Allograft survival was monitored, and flow cytometric analysis was performed to evaluate mixed chimerism and clonal deletion of alloreactive T cells. Treg-cell activity was assessed in vitro using suppression assays.
Results: Combination of T-cell depletion and CTLA4-Ig plus short course of rapamycin increased vascularized composite allograft survival significantly while untreated controls rejected allografts (mean survival time: 105 days; untreated, mean survival time: 9 days; CTLA4-Ig only, mean survival time: 17 days; rapamycin, mean survival time: 20 days; T-cell depletion, mean survival time: 20 days; p < 0.01). In order to further prolong allograft survival, 1-week expanded Treg cells were then included in the combination therapy. The suppressive activity of Treg cells was confirmed with in vitro suppression assays. The addition of ex vivo expanded Treg cells further increased vascularized composite allograft survival to more than 200 days and induced long-term stable mixed chimerism with 16.7% ± 1.5% of CD11b cells being donor-derived on postoperative day 55 after administration of expanded Treg cells.
Conclusion: The combination of T-cell depletion, costimulation blockade, and a short course of rapamycin prevents vascularized composite allograft rejection and significantly prolongs graft survival without the need for myeloablative conditioning or maintenance therapy. Moreover, Treg cells added in the early post-transplant period further optimize immune regulation.
Designing and implementing a multi-parametric bioreactor for the functional preservation of vascularized composite allografts
Vanessa Guarnizo
School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: Machine perfusion is arising as an alternative to cold storage for organ preservation. The purpose of this project was to incorporate machine perfusion into a novel multi-parametric bioreactor system for preserving murine abdominal wall grafts. The bioreactor is a closed-environment chamber that provides electrical muscle stimulation to improve function and prevent atrophy. It also allows real-time monitoring of perfusate metabolites via in-line sensors to determine viability.
Methods: SolidWorks was used to create prototype models that were three-dimensional printed. The prototypes provided the following: (1) sterile assembly, (2) closed environment, (3) humidity, (4) electrical stimulation, and (5) ports for perfusate in/out flow. This three-dimensional-printed chamber was used in conjunction with a peristaltic pump, a data acquisition system, and an electrical stimulation circuit (Figure 1). In-line sensors measured pH, temperature, oxygen, and pressure. After harvest, the abdominal wall graft was transferred to the bioreactor chamber, connected to inflow tubing, and wire electrodes placed on the graft surface. Perfusion with histidine–tryptophan–ketoglutarate solution with 12.5% albumin was conducted for 12 h. The electrodes delivered 7 V every 5 s. Following perfusion, the graft was harvested for tissue analysis.
Results: Initial pilot experiments showed that necrosis scores following perfusion ranged between 2 and 4, with evident vacuole formation. Muscle fiber separation was also seen, indicating pressure-induced injury (Figure 2). The electrical stimulation circuit was able to induce muscular contractions, although stimulation response gradually decreased until no contraction was seen.
Conclusion: These preliminary experiments have shown that our bioreactor system can perfuse the vasculature of the murine abdominal wall graft. The custom bioreactor facilitates perfusion and enables electrical stimulation and perfusate monitoring. The perfusate used, however, was insufficient to extend graft survival. The perfusate composition must be optimized to support tissue metabolism. The electrical stimulation protocol must also be optimized to minimize fatigue. The prototype also needs further refinements to optimize acquisition of force sensor and in-line sensor data.
The enigmatic impact of donor T-cell subsets on the therapeutic efficacy of tolerogenic protocols for transplant rejection
Marcos Iglesias, Maria Chicco, Darrel Bibicheff, WP Andrew Lee, Gerald Brandacher and Giorgio Raimondi
School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: Costimulation blockade-based regimens are a promising immunomodulatory strategy to promote long-lasting transplant tolerance. However, their efficacy is affected by multiple factors, many of which remain unknown. Recently, some reports have highlighted the unexpected capacity of passenger donor lymphocytes to directly fuel the recipient’s anti-graft response. Further studies are then necessary to understand their possible role in settings of regulation of alloreactivity. In this study, we aimed to assess whether T lymphocytes contained in the donor-specific transfusion inoculum, used as part of a very effective costimulation blockade regimen, contribute to the observed limited regulation of skin transplant rejection.
Methods: C57BL/6 mice recipients of full mismatch BALB/c skin allografts received a peri-transplant regimen based on donor-specific transfusion (107 splenocytes; day 0) and anti-CD154 mAb (MR-1; days 0, 7, and 14). To study the role of donor T cells, donor-specific transfusion inocula were depleted in total T cells, CD8, or CD4 subpopulations by negative selection. IgG donor-specific antibodies in serum were determined by flow cytometry.
Results: A peri-transplant regimen based on donor-specific transfusion + anti-CD154 has a profound protective effect on mouse skin allotransplantation. However, it does not induce long-term survival. When T cells were depleted from the donor-specific transfusion, transplant survival was almost doubled. T-cell subset-depletion studies indicated, unexpectedly, that donor CD8 T cells were responsible for limiting the efficacy of the tolerogenic regimen. Even more surprisingly, the presence of CD4 T cells in donor-specific transfusion induced a remarkable improvement in transplant survival, beyond that observed with full T-cell depletion. Ongoing experiments are aiming to determine the role of donor memory CD4/CD8 T cells in the effect observed and what correlation exists among the presence, absence, type of donor T lymphocytes, and the levels of donor-specific antibodies, or variations in the strength of the direct and indirect alloresponses.
Conclusion: Overall, these data reveal the existence of a novel and very important opposing role for donor passenger lymphocytes in the modulation of recipient’s alloimmunity by donor-specific transfusion + MR1-based regimens: a deleterious role for donor CD8, and a beneficial one for CD4 T cells. Identification of the specific mechanisms through which these divergent roles are exerted will be pivotal for the optimization of clinically effective tolerogenic therapies.
Topical tacrolimus and steroid as adjuvant therapies suppress acute rejection in hand allotransplantation
Yur-Ren Kuo1,2, Yi-Ting Chen1,2, Rong-Fu Chen1 and Ya-Ping Hou1
1Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2Kaohsiung Medical University, Kaohsiung, Taiwan
Background: Acute rejection is not uncommon after vascularized composite allotransplantation. The aim of this study is to investigate the effects of a topical immunosuppressant using topical tacrolimus (Protopic®) and steroid cream (clobetasol®) in hand-transplantation patients with acute rejection.
Methods: Two patients with hand and forearm deficiency underwent transplantations. Immunosuppression drugs including anti-thymocyte globulins and methylprednisolone (Solu-Medrol) were given at induction. Maintenance therapy consisted of tacrolimus, mycophenolate mofetil, and prednisone. Regular skin biopsies were performed to monitor the transplanted limb. The first case with acute rejection was noted at days 105 and 810 after surgery. The second case had one episode of skin rejection at day 63 post-transplantation. Both cases applied topical tacrolimus and clobetasol as an adjuvant therapy. Histology and immunohistochemical studies were performed and analyzed.
Results: In clinical observation, the transplanted hand of both cases recovered gradually after using topical immunosuppressive creams (tacrolimus and clobetasol) combined with systemic immunosuppressants. The histologic morphology showed that peri-vascular lymphocyte infiltration significantly decreased after using the topical immunosuppressant compared to that with control (rejection) status. Immunohistochemical stains showed that the CD3+ T cells and CD20+ B cells were suppressed in the recovery phase. FoxP3-positive regulatory T cells were also influenced by treatment.
Conclusion: Topical tacrolimus and clobetasol ointments are useful adjuvant methods to control acute hand allotransplant rejection and modulate lymphocyte activation, especially in T cells.
Immunomodulatory effect of adipose-derived mesenchymal stem cell on dendritic cells via Notch and non-canonical NF-κB pathways
Rong-Fu Chen1, Yu-Chi Wang1 and Yur-Ren Kuo2
1Kaohsiung Medical University Hospital, Kaohsiung, Taiwan
2Kaohsiung Medical University, Kaohsiung, Taiwan
Background: Adipose-derived stem cells are considered as potential immunomodulators and prolong the survival of vascularized composite allotransplantation. Mature dendritic cells present the alloantigen to effector T cells and induce the immune rejection or tolerance. The aim of this study is to investigate the role of Notch pathway in adipose-derived stem cell–modulated dendritic cell maturation, resulting in the suppression of the immune response.
Methods: Adipose-derived stem cells, myeloid dendritic cells, and CD4+ T cells were isolated from Lewis rats’ groin fat pad, femur bone marrow, and spleen, respectively. Dendritic cells were directly co-cultured with adipose-derived stem cells to evaluate the suppressive effect of adipose-derived stem cells. CD4+ T cells were co-cultured with dendritic cells pretreated with or without adipose-derived stem cells. Among all the Notch receptors and their ligands, Notch 1 and Jagged 1 were highly expressed on adipose-derived stem cell–treated dendritic cells and adipose-derived stem cells, respectively.
Results: The percentages of CD80 and CD86, and major histocompatibility complex class II of dendritic cells in the adipose-derived stem cell–treated group were significantly reduced as compared to that in mature dendritic cells without adipose-derived stem cell treatment. DAPT, a Notch inhibitor, could restore the dedifferentiation effects in the adipose-derived stem cell–treated dendritic cells. The levels of transforming growth factor-β were significantly increased in the culture supernatant of adipose-derived stem cell–treated dendritic cell group, as compared to that in the other groups. Furthermore, adipose-derived stem cell–pretreated dendritic cells induced the expansion of CD25+/FOXP3+/CD4+ Treg (regulatory T) cell population, but this effect was reversed by the DAPT pre-treatment or silencing of NF-κB-induced kinase, a noncanonical NF-κB pathways.
Conclusion: The results indicate that adipose-derived stem cells induce the tolerogenicity of dendritic cells by inhibition of maturation and promotion of down-stream Treg cell generation, which is associated with the activation of Notch 1 and noncanonical NF-κB pathways. This result could be applied as a potential strategy to improve vascularized composite allotransplantation survival.
Long-term tolerance to vascularized composite allografts across a class I barrier in swine employing a clinically applicable protocol with CTLA4-Ig (belatacept®) and anti-Il6R (tociluzimab®)
Alexandre G Lellouch1,2, Gaelle Saviane1, Laura C Burlage1,3, Ilse M Schol1, Laurent L Lantieri2, Mark A Randolph1, Gilles Benichou1 and Curtis L Cetrulo1
1Harvard Medical School and Massachusetts General Hospital, Boston, MA, USA
2Georges-Pompidou European Hospital, Paris, France
3University Medical Center Groningen, Groningen, The Netherlands
Background: Vascularized composite allografts have been proven an effective option for restoration of complex soft tissue defects. The limiting factor for vascularized composite allograft remains the risks of chronic immunosuppression. We sought to optimize our mixed hematopoietic chimerism vascularized composite allograft tolerance protocol with the addition of costimulatory blockade, regulatory T-cell augmentation, inflammatory cytokine inhibition, and augmentation of hematopoietic cell engraftment.
Methods: Prior to vascularized composite allografts, MGH (Massachusetts General Hospital) swine received non-myeloablative conditioning with 300 cGy total body and 700 cGy thymic irradiation on day 2. Osteomyocutaneous hind-limb vascularized composite allografts were transplanted into major histocompatibility complex class I–mismatched recipients (n = 8). Tacrolimus was administrated for 45 days (target level: 10–15 ng/mL). CTLA4-Ig (20 mg/kg) was administered on postoperative day 0 and on days 2, 4, and 6. Anti-IL6R (10 mg/kg) was given on postoperative days 0, 7, 14, 21, and 28. Vascularized composite allograft skin and muscle biopsies were performed on postoperative days 30, 50, and 100. Systemic immune function and chimerism status were assayed. Split thickness skin grafts were placed at postoperative day 150 from self, donor, and third-party donor to assess acceptance/rejection of the original donor skin.
Results: Three animals out of eight completed the protocol: swine 23645 became tolerant of the vascularized composite allograft, including the skin, and was terminated at 251 days, corresponding to the endpoint of the study. For other animals, we elected to extend the endpoint to 400 days. Swine 24087 has been tolerant up to postoperative day 330. One episode of acute epidermal rejection occurred at postoperative day 252 (after 207 days of immunosuppression), but resolved spontaneously without needing additional immunosuppression. Swine 24356 was currently tolerant through postoperative day 130. All animals showed mixed hematopoietic chimerism in the blood. Split thickness skin grafts placed at postoperative day 150 showed acceptance of self and donor skin grafts, whereas the third-party graft was rejected in the normal 8- to 12-day time frame.
Conclusion: We report a clinically relevant protocol for vascularized composite allograft tolerance induction using donor bone marrow as a hematopoietic cell source in a class I–mismatch swine model of vascularized composite allograft tolerance to all the components of a vascularized composite allograft (epidermis included). This protocol is being tested in full major histocompatibility complex–mismatch swine in anticipation of clinical translation.
Study of retinochoroidal circulation after whole-eye transplantation using fluorescein angiography
Chiaki Komatsu1, Maxine R Miller1, Jila Noori2, Yong Wang1, Touka Banaee1, Bing Li1, Joshua Barnett1, Wendy Chen1, Kira L Lathrop3, Ian A Rosner1, Wensheng Zhang4, Mario G Solari4, Andrew W Eller1 and Kia MM Washington1,5,6
1University of Pittsburgh Medical Center, Pittsburgh, PA, USA
2University of Miami, Miami, FL, USA
3Swanson School of Engineering, University of Pittsburgh, Pittsburgh, PA, USA
4Department of Plastic Surgery, University of Pittsburgh, Pittsburgh, PA, USA
5McGowan Institute for Regenerative Medicine, Pittsburgh, PA, USA
6VA Pittsburgh Medical Center, Pittsburgh, PA, USA
Background: Whole-eye transplantation could provide viable optical system and retina to people with vision loss. As a first step toward realizing this goal, we developed an orthotopic whole-eye transplantation rodent model. Perfusion of the retina is crucial for functional visual return, thus we evaluated the structural integrity of the retinochoroidal circulation after transplantation using fluorescein angiography, which is the gold standard to evaluate retinal circulation.
Methods: Brown Norway rats underwent syngeneic whole-eye transplantation (n = 4). Animals were examined at post-operative week 1. Wide-field fluorescein angiography images were obtained to evaluate retinochoroidal blood flow. Ocular examinations were performed by an ophthalmologist with retina specialization to evaluate the anterior and posterior segments of the eye. A second group of naive Brown Norway rats (n = 3) served as controls.
Results: Naive eyes of fluorescein angiography demonstrated complete filling of vessel and normal optic disc. Fluorescein angiography revealed that retinochoroidal circulation was restored in all transplanted eyes exhibiting normal choroidal background, arterial and venous filling, and no leakage from the vascular tree, which were comparable to normal naive eyes. In two of the transplants, retinal arteries were narrowed in fluorescein angiography, while in the other two transplants’ retinal vasculature seemed similar to the control eyes.
Conclusion: Fluorescein angiography results have confirmed that retinochoroidal circulation can be established after whole-eye transplantation in a rat model. Although two out of four rats with transplanted eyes appeared to have some vascular attenuation in comparison with the eyes of control animals, all rats exhibited a normal vascular filling pattern and the absence of vessel leakage which indicates that there is no endothelial cell damage, and the structural integrity of blood–retinal barriers can be maintained after whole-eye transplantation.
OPTN waiting list trends for vascularized composite allograft transplants
Jennifer Wainright, Christopher Wholley, Wida Cherikh, Jennifer Musick and David Klassen
United Network for Organ Sharing, Richmond, VA, USA
Background: The OPTN (Organ Procurement and Transplantation Network) was granted oversight of vascularized composite allograft transplants on 3 July 2014 and developed vascularized composite allograft policies that went into effect on that date. At the same time, the OPTN implemented a national vascularized composite allograft waiting list, transitioning from localized practices to a national allocation system. This study characterizes the OPTN vascularized composite allograft waiting list in terms of composition, waiting time, and transplants.
Methods: The cohort includes all candidates on the OPTN vascularized composite allograft waiting list between 3 July 2014 and 30 March 2018 (n = 57). Transplant data include all vascularized composite allograft transplants that occurred between 3 July 2014 and 30 March 2018, regardless of listing date (n = 29).
Results: Since 3 July 2014, 57 candidates—52.6% male, 78.9% White, and 73.7% younger than 45 years—were added to the waiting list. They were waiting for upper limb (n = 21), head and neck (n = 13), uterine (n = 16), abdominal wall (n = 4), and penile (n = 3). New vascularized composite allograft registrations increased in 2016 (n = 18) after uterine and penile transplants were introduced in the United States, with fewer new registrations in 2017 (n = 10), then an increase in the first three months of 2018 (n = 7). The size of the vascularized composite allograft waiting list remained fairly constant over the past year, but the waiting list shifted over time from mostly upper limb and craniofacial candidates to more penile and uterine candidates in 2017. Upper limb and craniofacial registrations increased in early 2018, with a total of 19 candidates on the vascularized composite allograft waiting list as of 30 March 2018 (15.8% bilateral upper limb, 21.1% unilateral upper limb, 26.3% craniofacial, 5.3% craniofacial/scalp, and 31.6% uterine). In total, 23 candidates received deceased donor transplants (6 bilateral upper limb, 4 unilateral upper limb, 5 craniofacial, 1 scalp, 1 abdominal wall, 2 penile, and 4 uterine), and 6 received living donor uterine transplants. Waiting times for vascularized composite allograft vary; median time waiting for those transplanted was 161 days (interquartile range: 79.5–373.0).
Conclusion: The composition of the vascularized composite allograft waiting list has evolved over time as new vascularized composite allograft procedures have developed. Continued monitoring of vascularized composite allograft waiting list activity is needed to assess and plan for changes in this field.
Rapamycin therapy impairs Treg expression of CXCR3 and limits Treg-dependent survival of vascularized composite allotransplants
Heng Xu1, Wayne W Hancock2, L Scott Levin3 and Yixin Zhang4
1Shanghai 9th People’s Hospital, Shanghai, China
2Children’s Hospital of Philadelphia, Philadelphia, PA, USA
3Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
4Shanghai 9th People’s Hospital, Medicine school of Shanghai Jiaotong University, Shanghai, China
Background: Vascularized composite allotransplantation, a non-life supporting procedure used, for example, to restore limb function or facial appearance to an injured patient, elicits complex host immune responses. Many groups use rapamycin in efforts to preserve host Treg (regulatory T) function and number, while suppressing Teff (effector T) cells.
Methods: We established a mouse forelimb orthotopic Tx model, using BALB/c donors and C57BL/6 recipients, to test the effects of rapamycin (3 mg/kg, 28 days). Flow cytometry, in vivo Treg assay, and immunohistochemical analysis were performed in the study.
Results: Mediated by Tregs in dominant, rapamycin prolonged vascularized composite allograft survival for ~5 days compared to untreated controls (p < 0.005). No differences in Treg function were observed in vitro, using Tregs isolated from spleens of mice in each group. However, in vivo studies indicated that rapamycin-treated Tregs + WT Teff, which were injected into Rag1-/- mice and received transplantation then, decreased allograft survival significantly compared to the control group Tregs + WT Teff (p < 0.05). By immunohistochemical analysis, fewer CXCR3+ Foxp3+ Tregs (p < 0.05) were found in allografts of rapamycin-treated versus control mice-treated allografts, suggesting that rapamycin might impair Treg migration. An in vivo Treg assay using WT Teff combined with cd4cre-tbx21fl/fl or WT Tregs showed that Tregs with decreased CXCR3 expression had impaired migration ability, which was controlled by T-bet (p < 0.05) and could be rescued by WT Tregs (p < 0.05). While host CD8 T cells were suppressed effectively, the number of CD4+ Foxp3−CD44+ CD62L− T cells were higher in the rapamycin-treated group (p < 0.05), again consistent with impaired Treg migration.
Conclusion: Thus, we conclude that in vascularized composite allotransplantation, though high-dosage rapamycin can prolong allograft survival for several days, it downregulates CXCR3+ on Tregs and impairs their migration ability significantly. Maintenance of CXCR3 expression by recipient Foxp3+ Treg cells may be important to further efforts to enhance vascularized composite allotransplantation survival.
Composite tissue xenopreservation: a novel strategy for staged transplantation of vascularized composite allografts
Fatih Zor1, Rezarta Kapaj2, Yalcin Kulahci3, Huseyin Karagoz1, Yildirim Karslioglu2 and Vijay S Gorantla1
1Wake Forest Institute for Regenerative Medicine, Winston Salem, NC, USA
2Gulhane Military Medical Academy, Ankara, Turkey
3University of Pittsburgh, Pittsburgh, PA, USA
Background: The need for preserving composite tissues for reconstructive indications is a clinical necessity in modern plastic surgery practice. In certain instances, tissues need to be preserved and used at a future date, as in the amputation patient whose medical status precludes a long surgical procedure, or a concomitant transplantation is planned. However, long-term preservation beyond 24 h has not been successful for composite tissues. Here, we described a novel strategy of xenopreservation (via xenotransplantation) to preserve composite tissues for 7 days, followed by staged transplantation.
Methods: Two concordant species, Sprague Dawley rats (n = 6) and mice (n = 6), were used. The groin flap of the rat was used as a xenograft and xenotransplanted to the neck area of the carrier mouse. Immunosuppression was administered in order to prevent rejection. After a 7-day period of preservation on the mouse neck, xenotransplanted groin flap (called, xenopreserved flap) was reharvested; tissue samples were collected from the skin and vascular structures for histopathological evaluation; and the xenopreserved flap was transplanted to the donor’s opposite groin area. Anastomoses were performed between the flap’s pedicle, and the femoral artery and vein. The xenopreserved flap was monitored daily. After 15 days of the second surgical procedure, the rats were euthanized, and tissue samples were collected.
Results: All xenopreserved groin flaps except one survived. Tissue evaluation indicated prominent inflammation in carrier mouse, but these changes were found to be reversible when the xenopreserved tissue was transplanted to the donor rat.
Conclusion: A novel strategy for composite tissue preservation is described and a basic model for further investigation has been developed in this study. Preservation of composite tissues may be the key factor to solve the challenges related to concomitant transplantation. Additional translational studies are needed to modulate the tissue changes following xenopreservation.
Who are the vascularized composite allograft deceased donors?
Jennifer Wainright, Christopher Wholley, Wida Cherikh, John Rosendale and David Klassen
United Network for Organ Sharing, Richmond, VA, USA
Background: Life-changing vascularized composite allograft transplants are made possible by the generosity of vascularized composite allograft donors. This study provides the first detailed description of vascularized composite allograft deceased donors in the United States.
Methods: Transplant programs performed 72 deceased donor vascularized composite allograft transplants, including 17 unilateral upper limb, 15 bilateral upper limb, 13 craniofacial, 19 abdominal wall, 4 uterine, 2 larynx, 1 penile, and 1 scalp transplant between 1998 and 2017. The cohort included all vascularized composite allograft donors recovered between 1998 and 2017, excluding 2 larynx and 2 abdominal wall donors where data were not available. Of the 70 vascularized composite allograft deceased donors, 2 were both craniofacial and upper limb donors. The final cohort included 66 vascularized composite allograft deceased donors.
Results: About 30% of vascularized composite allograft donors were female, with about a quarter of craniofacial (27.3%), upper limb (26.7%), and abdominal wall (23.5%) donors being female. Most vascularized composite allograft recipients received a transplant from a donor of the same sex, but two upper limb recipients and eight abdominal wall recipients received an organ from a different sex donor. The vast majority of vascularized composite allograft donors (86.4%) were White. All craniofacial donors were White, as were 93.3% of upper limb donors (3.3% black and 3.3% Hispanic). A smaller proportion of abdominal wall donors were White (70.6%), with 23.5% Hispanic and 5.9% Black. The ABO blood types of vascularized composite allograft donors were O (57.6%), A (30.3%), B (9.1%), and AB (3.0%). Most vascularized composite allograft donors were between 18 and 54 years, with a median age of 27 years (interquartile range: 18–44; range: 0–65 years). Kidney Donor Profile Index, a measure of time a donated kidney is expected to function, varied greatly among vascularized composite allograft donors. Kidney Donor Profile Index ranged from 2.0 to 96.0 for craniofacial donors, from 1.0 to 78.0 for upper limb donors, and from 1.0 to 88.0 for abdominal wall donors. Body mass index varied widely, especially for upper limb donors (range: 15.7–36.3) and for craniofacial donors (range: 22.5–36.2).
Conclusion: Deceased vascularized composite allograft donors in the United States are a diverse group in terms of sex, age, race, ABO, Kidney Donor Profile Index, and body mass index.
An experimental model of whole-eye transplantation for assessment of viability and immunological outcomes
Fatih Zor1, Murat Polat2, Yalcin Kulahci3, Huseyin Karagoz1, Bulent Kurt2, Bilal Battal2 and Vijay S Gorantla1
1Wake Forest Institute for Regenerative Medicine, Winston Salem, NC, USA
2Gulhane Military Medical Academy, Ankara, Turkey
3University of Pittsburgh, Pittsburgh, PA
Background: This study aimed to establish a novel whole-eye vascularized composite allotransplantation model that includes the eyeball, adnexa, and soft tissues with the optic nerve to evaluate the immunological, neuroregeneration, and graft survival outcomes.
Methods: Sprague Dawley rats received heterotopic vascularized whole-eye transplants. Each periorbital flap included the globe, and surrounding tissues based on common carotid artery and external jugular vein as vascular pedicle (Figure 1). Viability was confirmed by angiography, magnetic resonance imaging, and clinical examination. Histopathology of protocol skin biopsies was scored for Banff grading. The globe, adnexal, and optic nerve tissues were analyzed for acute rejection and/or nerve regeneration at endpoint of 30 days or grade-3 rejection (whichever was earlier).
The figure shows the harvested composite eyeball flap, based on common carotid artery and external jugular vein. Note the optic nerve at the inner side of the flap.
Results: Macroscopic evaluation confirmed flap viability (Figure 2). The magnetic resonance evaluation revealed loss of globe volume by 35% after transplantation, but the overall orbital integrity was maintained. Histological exam of globe and adnexal tissues, especially cornea and retina, showed unique and differential patterns of rejection, predominantly involving macrophage and neutrophil infiltration. Optic nerve sectioning revealed a degeneration pattern with no evidence of regeneration.
The figure shows the viable eyeball transplant at 30 days.
Conclusion: This is the first study of successful heterotopic whole-eye transplantation in the literature. This model offers promise and potential in immunological, neuroregeneration, drug delivery, cellular therapies, imaging, and tissue engineering studies involving optic nerve, retina, or eyeball tissues.
Solid organ yield for vascularized composite allograft donors
Jennifer Wainright1, Gabe Vece1, Christopher Wholley1, John Rosendale1, Wida Cherikh1, Christopher Curran2, Amanda Robinson1, Darren DiBattista1 and David Klassen1
1United Network for Organ Sharing, Richmond, VA, USA
2New England Donor Services, Waltham, MA, USA
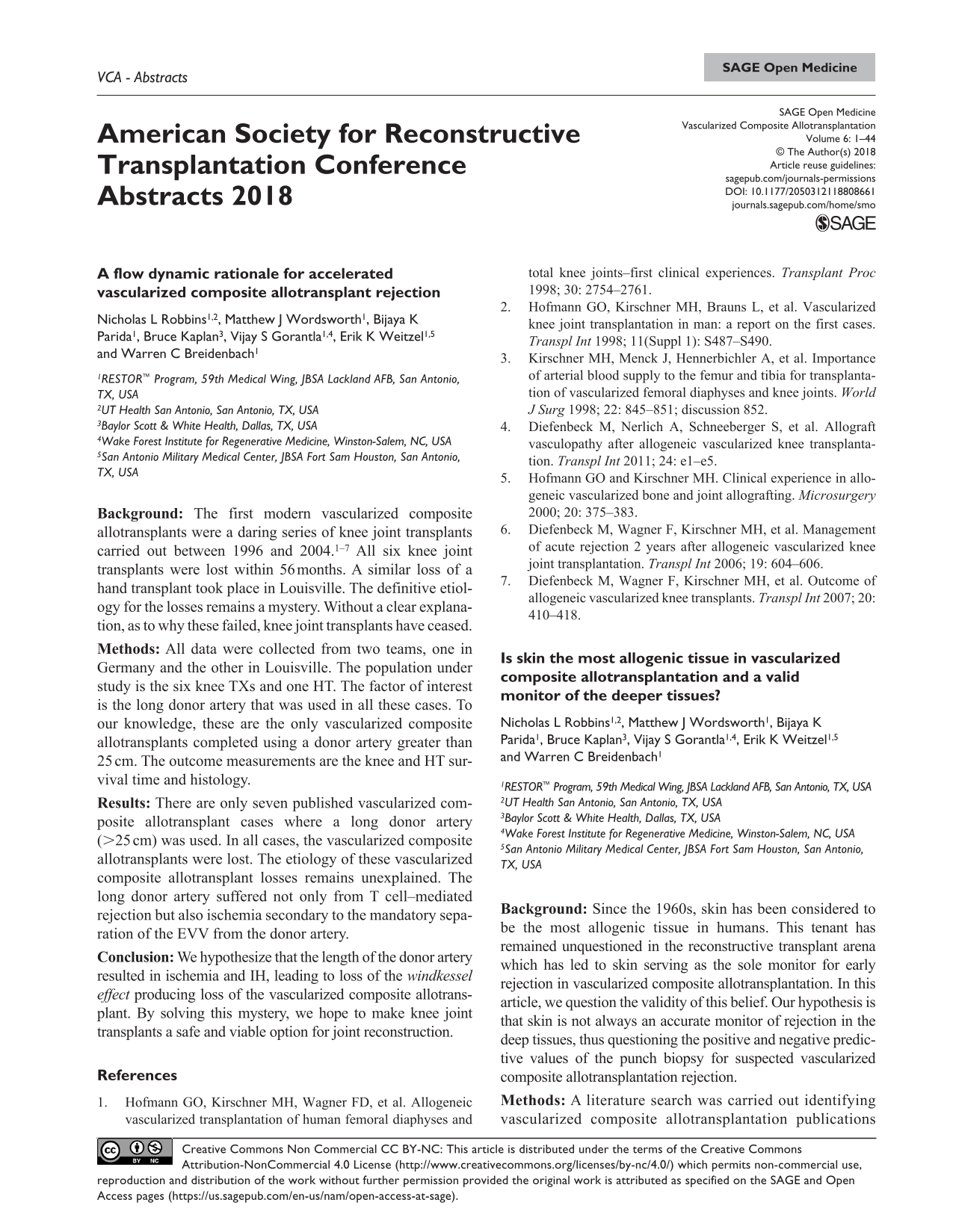
Background: Vascularized composite allograft transplantation provides life-changing transplants, but vascularized composite allograft procurement complicates the donation process and timing and has the potential to impede solid organ donation. Descriptive analyses to date are reassuring; this study examines the predicted versus observed number of solid organs donated by vascularized composite allograft donors.
Methods: The cohort included vascularized composite allograft donors in the United States, from 1 January 2008 to 31 December 2017 (n = 51). We used OPTN (Organ Procurement and Transplantation Network) Deceased Donor Registration Form data to calculate observed-to-expected (O:E) yield ratios with 2017 SRTR donor yield models.
Results: Almost all vascularized composite allograft donors’ livers (48 of 51; 94.1%) and kidneys (92 of 102; 90.2%) were transplanted. Fewer hearts (28 of 51; 54.9%), lungs (46 of 102; 45.1%), pancreata (15 of 51; 29.4%), and intestines (3 of 51; 5.9%) were transplanted. O:E ratios for overall organ yield was as predicted for non-vascularized composite allograft donors (1.04; 95% confidence interval: 0.98–1.10). This finding remained when analyzed separately by vascularized composite allograft type. We found that donors of unilateral upper limbs, craniofacial, or abdominal wall had overall organ yields that were as predicted. Bilateral upper limb and uterine donors had higher-than-expected organ yields. Results were similar when we analyzed the data separately by solid organ type, with better-than-expected liver yields (1.07; 1.04–1.09) and lung yields (1.31; 1.06–1.57). We found as predicted organ yields for kidney (0.99; 0.94–1.03) and pancreas (1.08; 0.81–1.36). Yields for hearts were lower than predicted (0.89; 0.80–0.99), with a total expected mean yield of 31.4 versus a total actual yield of 28 for hearts. Of the nine recovered vascularized composite allograft donors who had an expected heart yield of more than 0.5 (i.e. >50% chance a similar donor would donate a heart), but were not heart donors, six (66.7%) had a left ventricle ejection fraction of less than 40, suggesting that these donors were not suitable heart donors.
Conclusion: Solid organ recovery among vascularized composite allograft donors was as predicted or better for most organs, suggesting that vascularized composite allograft donation does not compromise recovery and transplantation of abdominal and thoracic organs.
Facial allotransplantation: an early look at OPTN data
Jennifer Wainright1, L Scott Levin2, Linda Cendales3, Christopher Wholley1, Wida Cherikh1, David Klassen1 and Bohdan Pomahac4
1United Network for Organ Sharing, Richmond, VA, USA
2Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
3School of Medicine, Duke University, Durham, NC, USA
4Brigham and Women’s Hospital, Boston, MA, USA
Background: Craniofacial vascularized composite allograft transplantation is a developing area in the field of transplantation.
Methods: The cohort included all craniofacial vascularized composite allograft recipients (n = 14) in the United States who received transplants through 30 April 2018.
Results: A total of 14 craniofacial transplants have been performed in the United States since 2008. Follow-up time for patient and graft status ranged from 0.1 to 9.4 years post-transplant (median = 4.6 years; interquartile range: 2.7–7.0). Of the 14 transplants, 10 (71.4%) were male. Recipients’ age ranged from 21 to 60 years, and five (35.7%) were 18–34 years, four (28.6%) 35–44 years, two (14.3%) 45–54 years, and three (21.4%) 55 years and above. All 14 (100.0%) were White. Of the 13 with reported data, 8 (61.5%) required a transplant because of trauma and 5 (38.5%) because of burns or explosions. As of 30 April 2018, no craniofacial vascularized composite allograft recipients in the United States have died after transplant, and all recipients have intact grafts. Of the recipients with reported data, none has developed new onset diabetes or metabolic complications. Of the 10 with reported data, 4 had infectious complications, 1 had other complications, and 9 had at least one acute rejection episode.
Conclusion: Craniofacial vascularized composite allograft recipients in the United States are relatively diverse in terms of recipient sex and age. Patient and graft survival to date have been encouraging, but continued follow-up is needed to obtain long-term outcome data.
Brain reorganization and grasping with a transplanted hand
Scott Frey1, Kenneth Valyear2, Benjamin Philip3, Christina Kaufman4 and Daniela Mattos1
1University of Missouri, Columbia, MO, USA
2 Bangor University, Bangor, UK
3Washington University in St. Louis, MO, USA
4Christine M. Kleinert Institute for Hand and Microsurgery, Louisville, KY, USA
Background: Hand loss can now be reversed through surgical transplantation years or decades after amputation. Remarkably, these patients come to use their new hand to skilfully grasp and manipulate objects. The brain mechanisms that make this possible are unknown. Here, we test the hypothesis that the anterior intraparietal cortex—a multimodal region implicated in hand preshaping and error correction during grasping—plays a key role in this compensatory grasp control.
Methods: High spatio-temporal resolution motion capture and functional magnetic resonance imaging are used to characterize hand kinematics and brain responses, respectively, during visually guided grasping with a transplanted hand at 26 and 41 months post-transplant in patient DR, a former hand amputee of 13 years. Functional magnetic resonance imaging was also used to map activity associated with simple open–close movements of the affected hand.
Results: Compared with matched controls, DR shows increasingly normal grasp kinematics paralleled by increasingly robust grasp-selective functional magnetic resonance imaging responses within the very same brain areas that show grasp-selectivity in controls, including the anterior intraparietal cortex, premotor, and cerebellar cortices. Paradoxically, over this same time, DR exhibits significant limitations in basic sensory and motor functions, and persistent amputation-related functional reorganization of primary motor cortex. Movements of the non-transplanted hand positively activate the ipsilateral primary motor hand area—a functional marker of persistent interhemispheric amputation-related reorganization.
Conclusion: Our data demonstrate for the first time that even after more than a decade of living as an amputee, the normative functional brain organization governing the control of grasping can be restored. We propose that the anterior intraparietal cortex and interconnected premotor and cerebellar cortices enable grasp normalization by compensating for the functional impact of reorganizational changes in primary sensorimotor cortex and targeting errors in regenerating peripheral nerves.
The functional relevance of reorganization in sensory cortex in current and former upper extremity amputations
Scott Frey1, Benjamin Philip2, Kenneth Valyear3, Christina Kaufman4, Carmen Cirstea1, Nathan Baune2 and Pin-Wei Chen2
1University of Missouri, Columbia, MO, USA
2Washington University in St. Louis, MO, USA
3Bangor University, Bangor, UK
4Christine M. Kleinert Institute for Hand and Microsurgery, Louisville, KY, USA
Background: Numerous sources of evidence demonstrate large-scale reorganizational changes in sensory cortex following upper extremity amputation and associated deafferentiation. Remarkably little, however, is known about the functional correlates of these changes or their reversibility. Here, we address this issue through use of functional magnetic resonance imaging and sensory psychophysics in a cohort of current and former amputees, as well as healthy matched controls.
Methods: A total of 19 chronic, unilateral, upper extremity amputees; 5 former amputees (2 hand transplant and 3 hand replant recipients); and 28 healthy matched controls underwent functional magnetic resonance image scanning during cutaneous stimulation of the fingers of the intact hand, and left or right sides of the lower face. Patients were also evaluated for phantom limb pain and/or residual limb pain, referred sensations, and the ability to localize light touch in the absence of vision.
Results: A total of 13 current amputees reported phantom limb pain, while 9 reported residual limb pain. In contrast to earlier reports, none experienced referred sensations during stimulation of the face or upper extremities. In amputees, the somatosensory hand area contralateral to the injury (i.e. “former hand area”) responded to stimulation of the intact hand, but not to face stimulation, as previously shown in non-human primates. Critically, these ipsilateral responses were absent in controls and unrelated to phantom limb pain, residual limb pain, or the ability to localize stimuli on the intact hand. Furthermore, despite engaging somatosensory hand areas bilaterally, touch localization did not differ between amputees and controls, who exhibit only contralateral responses. The ability to localize touch accurately on a replanted or transplant hand was, however, correlated positively with levels of activity within the former hand area.
Conclusion: Human somatosensory cortex undergoes major bilateral reorganization following amputation. In particular, the former hand area of amputees responds vigorously to stimulation of the intact hand. Remarkably, we failed to identify any relationship between these dramatic reorganizational changes and either pain or sensory function. We do, however, find that engagement of the former hand area by touch on a transplanted or replanted hand is a biomarker of recovery of sensory function.
Nailfold capillaroscopy: potential use in vascularized composite allotransplantation of the hand
Mélissa Roy, Siba Haykal, Kevin J Zuo, Danny Ghazarian and Steven J McCabe
University of Toronto, Toronto, ON, Canada
Background: The diagnosis of acute rejection in vascularized composite allograft is based on physical examination and the interpretation of skin biopsies. Nailfold capillaroscopy allows direct visualization and quantification of the microcirculation at the base of the nail. Nailfold capillaroscopy has been used for early diagnosis of rheumatological disorders and to assess perfusion of replanted digits. Since acute rejection in vascularized composite allograft is a microvascular phenomenon and changes around the nail have been seen in chronic rejection, we are interested in the potential of nailfold capillaroscopy to aid in detection of the rejection process. We describe our exploration of this tool for the assessment of microvascular changes in vascularized composite allograft of the hand.
Methods: Our patient, transplanted at the proximal forearm level, underwent a series of 4 mm punch biopsies as per protocol and concurrent nailfold capillaroscopy. Biopsies were graded by a dermatopathologist according to the Banff working classification. Nailfold videocapillaroscopy was performed using a binocular microscope (Nikon SMZ800 N). Nailbeds from the patient’s transplanted and non-transplanted hands were examined. We were able to obtain biopsies and nailfold capillaroscopy images during grade-1, grade-2, and grade-3 rejection episodes. Images were reviewed to determine whether specific changes could be identified at each level of rejection.
Results: Our patient has been followed for 28 months post transplant. During that period of time, pathology has revealed episodes of grade-1, grade-2, and one grade-3 rejection. We have seen changes on nailfold capillaroscopy such as peri-vascular edema and capillary drop out, but we have not yet been able to discern specific patterns or changes that clearly correlate to each rejection grade or to diagnose early rejection.
Conclusion: Nailfold capillaroscopy is easy and safe, with no donor-site morbidity. Despite our inability to identify specific changes that could help diagnose acute rejection, we acknowledge our experience to date is limited. We have not used the technique in the face of chronic rejection. We will continue to refine our use of this technique in order to better delineate its potential role as an adjunct for identification of rejection.
Nailfold capillaroscopy of the VCA index finger during grade-3 rejection.
Total penis, scrotum, and partial abdominal wall transplantation
Richard James Redett1, Damon Cooney1, Gerald Brandacher1, Sami Tuffaha1, Carisa Cooney1, Jaimie Shores1, Justin Sacks1, Steven Bonawitz2, Devin Coon-O’Brien1, Trinity Bivalacqua1, Arthur Burnett1 and WP Andrew Lee1
1School of Medicine, Johns Hopkins University, Baltimore, MD, USA
2Cooper University Health Care, Camden, NJ, USA
Background: Patients with severe penile defects can suffer from debilitating physical and psychosocial problems and a profound loss of quality of life. While traditional reconstructive options produce satisfactory outcomes in many cases, it is limited by a high rate of complications involving the erectile prosthesis and urethra. For patients who have either failed autogenous reconstruction or are not appropriate candidates, penile allotransplantation can offer a viable alternative. We describe our experience performing a total penis, scrotum, and partial abdominal wall transplant in a patient who suffered a devastating blast injury to his pelvis.
Methods: After obtaining institutional review board’s approval, we evaluated patients with severe traumatic genitourinary defects with a characteristic injury pattern involving the lower abdominal wall, penis, and scrotum. Cadaver dissections were undertaken to determine how to perform multiple vascular anastomoses to perfuse a penile, scrotum, and adjacent abdominal wall. Cadaver study results were confirmed using SPY fluorescent imaging during a research procurement.
Results: Recovery of the donor graft included part of the lower abdominal wall, the entire penis and scrotum, and skin paddles extending over both groins to include the external pudendal vascular system. Multiple anastomoses including inferior epigastric vessels to both penile dorsal arteries and veins, bilateral saphenous to saphenous veins (donor saphenous contained external pudendal veins), and left end to side femoral artery (included external pudendal arteries) were performed to perfuse the allograft. SPY fluorescent imaging demonstrated uniform perfusion of the allograft. The patient returned to the OR 7 h after surgery for evacuation of a hematoma. He received a donor bone marrow infusion on day 14. The urinary catheter was removed at week 5 and he was urinating normally. By week 8, he had spontaneous, partial tumescence of the penis. Immunosuppression consists of alemtuzumab induction and subsequent tacrolimus monotherapy. He had one episode of mild, acute, cell-mediated skin rejection (Banff grade I) which was successfully treated with topical clobetasol and tacrolimus cream.
Conclusion: Penile allotransplantation provides the potential for restoring normal anatomy and near-normal urinary and sexual function and should be considered in appropriate candidates, when conventional reconstruction is unavailable.
Evaluation of phenotype and safety of novel universal multi-chimeric cell therapy in the NSG mouse model: a preliminary study
Maria Siemionow, Joanna Cwykiel and George Rafidi
University of Illinois at Chicago, Chicago, IL, USA
Background: Stem cells were proposed to induce tolerance and eliminate lifelong immunosuppression for patients following solid organ and vascularized composite allotransplantation. We introduce a universal cell therapy of ex vivo created umbilical cord blood–derived multi-chimeric cells as an alternative approach to bone marrow–based therapies in support of vascularized composite allotransplantation. This study aimed to establish the ex vivo fusion protocol and characterize the phenotype, genotype, viability, proliferative potential, and safety of human multi-chimeric cells.
Methods: A total of 30 fusions of umbilical cord blood cells derived from 3 unrelated donors were performed. Briefly, umbilical cord blood cells were stained separately by PKH26, PKH67, and eFluor670 proliferation dye and fused using polyethylene glycol. Triple PKH26/PKH67/eFluor670 stained multi-chimeric cells were sorted and assessed by microscopy and flow cytometry for the efficacy of the fusion procedure. The viability of multi-chimeric cells and distribution of hematopoietic markers were performed by flow cytometry. PCR-rSSOP (polymerase chain reaction–reverse sequence-specific oligonucleotide probe) and STR-PCR (short tandem repeat–polymerase chain reaction) characterized the genotype of multi-chimeric cells. Proliferative potential of multi-chimeric cells was assessed by colony forming unit assay. The safety of multi-chimeric cells was tested in the NSG mouse model. Twelve animals divided into two groups received intraosseous injection of Group 1, umbilical cord blood derived from three donors (control, total: 0.6 × 106 cells), and Group 2 (0.6 ×106) of multi-chimeric cells. Mice were observed for 90 days for changes in weight, activity, posture, and hair loss. Mice were evaluated three times per week by palpation for tumor growth.
Results: Flow cytometry and confocal microscopy confirmed creation of human multi-chimeric cells. PCR-rSSOP and STR-PCR assays determined that multi-chimeric cells share class I and II human leukocyte antigens, and selected loci specific for all three umbilical cord blood donors used for fusion. Multi-chimeric cells’ viability ranged between 85% and 95%. Distribution of hematopoietic markers on the surface of multi-chimeric cells was comparable to umbilical cord blood. Colony forming unit assay confirmed maintenance of proliferative properties by multi-chimeric cells. No multi-chimeric cell–derived tumor-like growth was detected up to 90 days post-injection.
Conclusion: We have successfully confirmed creation of human multi-chimeric cells. We characterized in vitro the phenotype, genotype, viability, and proliferative potential of multi-chimeric cells. We confirmed safety of multi-chimeric cells in vivo. This unique concept of multi-chimeric cells introduces a universal therapy for tolerance induction in solid organ and vascularized composite allotransplantation.
Three-dimensional virtual planning in facial transplantation
Andrew John Lindford, Jyrki Törnwall and Patrik Lassus
Helsinki University Hospital, Helsinki, Finland
Background: In facial transplantation involving soft tissue and maxilla and/or mandible, the correct alignment of the bony structures is essential for normal dental occlusion and function. We present our technique using virtual planning with computer-aided design and computer-aided manufacturing that was utilized in the first two Helsinki face transplantation cases.
Methods: Both patients had earlier sustained a severe facial ballistic injury and had a characteristic central facial avulsive defect with severe midface collapse and loss of facial height. Three-dimensional computed tomographic scans were obtained to evaluate the skeletal anatomy and determine the size and configuration of the defect. The computer-aided design and computer-aided manufacturing methods were used to manufacture generic donor and customized recipient patient osteotomy guides that were used in rehearsed cadaver cases. Once a suitable donor became available, three-dimensional computed tomographic data from the actual donor were used to simulate virtual osteotomies by superimposing the donor facial skeleton onto the recipient. Donor-specific osteotomy guides were then manufactured expediently prior to surgery and used to obtain maximal accuracy in the reconstruction.
Results: In both cases, the donor facial transplant consisted of a Le Fort II maxilla and central mandible. The maxilla and mandible were transplanted timely to the recipient with nearly correct anatomical alignment and did not require any bone trimming. The occlusion was determined using intermaxillary screws and the mandible was fixed with two reconstruction plates.
Conclusion: Three-dimensional virtual planning enabled the development of customized osteotomy guides for donor and recipient patients for both face transplant cases. This enabled prompt and more precise osteotomies, thus reducing operating time as well as allowing preoperative simulation using different donor anatomies.
Vascularized composite allograft transplants in the United States: donor infections and their risks—an OPTN review
Cameron Robert Wolfe, Gabe Vece, Susan Tlusty, Ricardo La Hoz and Marian Michaels
United Network of Organ Sharing, Richmond, VA, USA
Background: The OPTN (Organ Procurement and Transplantation Network) Ad Hoc Disease Transmission Advisory Committee evaluates unanticipated potential donor-derived transmission events, including infections, malignancies, and other pathologies, to assess for likelihood of donor transmission. The field of vascularized composite allograft transplant is growing, and understanding the range of deceased donor infections that may be present at the time of organ donation is valuable to prevent transmission.
Methods: Between 3 July 2014 and 27 April 2018, 22 deceased donors were involved in 23 vascularized composite allograft transplants. The OPTN received only two potential donor-derived transmission event reports regarding vascularized composite allograft recipients. A structured review of the OPTN database was carried out, looking at mandated donor cultures (blood, urine, and sputum).
Results: A total of 10 upper limb, 5 craniofacial, 2 penile, and 4 deceased donor uterine transplants were completed, along with an abdominal wall and scalp transplant. Only 1 of 22 donors was classified as Public Health Service (PHS)–increased risk donor. Nineteen donors were Epstein–Barr virus IgG+ donors (86%; general donor seroprevalence: 89%), including four mismatches (D+/R−). Nine donors were cytomegalovirus IgG+ donors (41%; general donor seroprevalence: 61%). All 22 donors were negative for HIV, hepatitis B, and hepatitis C. Donations occurred from a geographically diverse range of 13 Organ Procurement Organizations; the most productive Organ Procurement Organization facilitated four vascularized composite allograft transplants. Only two donors were noted to have positive blood cultures, with Staphylococcus aureus and Enterobacter cloacae in one; Pseudomonas aeruginosa and Staphylococcus aureus in the other. Seven donors had positive respiratory cultures, including Staphylococcus aureus (four), Streptococcus pneumoniae, Enterobacter species, Enterococcus faecalis, and Haemophilus influenzae. No recipients reported transmitted bacterial disease in our cohort, whether or not their donor had positive cultures.
Conclusion: Unexpected donor-derived infections have rarely been reported in vascularized composite allograft transplants in the United States. While under-recognition and under-reporting may play a role, our data suggest that the risk associated with positive blood, sputum, or urine cultures in vascularized composite allograft donors can be acceptable under certain circumstances and prophylaxis mitigates the risk. Additional tissue-specific infectious screening may be of value, for example, sinus culture for craniofacial vascularized composite allograft or sexually transmitted infection screening in penile or uterine transplants. The vascularized composite allograft community is encouraged to look for and report unexpected donor-derived transmission events to the OPTN Patient Safety Portal.
Circulating donor-derived cell-free DNA as a non-invasive biomarker for allograft rejection in vascularized composite allotransplantation
Sotirios Tasigiorgos1, Yanan Kuang2, Branislav Kollar1, Thet Su Win1, Leonardo V Riella1, Simon G Talbot1, Cloud P Paweletz2 and Bohdan Pomahac1
1Brigham and Women’s Hospital, Boston, MA, USA
2Belfer Center for Applied Cancer Science, Dana-Farber Cancer Institute, Boston, MA, USA
Background: Donor-derived cell-free DNA has demonstrated potential as a minimally invasive diagnostic tool in solid organ transplantation. Multiple recent studies show that the relative contribution of circulating donor-derived cell-free DNA to the total cell-free DNA in the circulation of solid organ transplantation recipients is predictive of acute rejection. However, its potential to play a similar role in vascularized composite allotransplantation remains unexamined.
Methods: We conducted a preliminary, prospective study where we identified and measured donor-derived cell-free DNA in the recipients’ post-transplant plasma with droplet digital polymerase chain reaction. Using TaqMan chemistry, we designed genotyping assays on single nucleotide polymorphisms in exons 2 and 3 which encode human leukocyte antigen (HLA) alpha1 and alpha2 domains. The single nucleotide polymorphisms were chosen based on the pre-transplant human leukocyte antigen genotyping of the donors and the recipients. Post-transplant plasma at times of no rejection for two upper extremity transplant recipients was collected and donor-derived cell-free DNA extracted. Donor alleles and recipient alleles were measured in serially drawn plasma samples.
Results: For the first patient, we were able to detect separate clusters which have donor and recipient alleles (HLA-A2/A3) in droplet digital polymerase chain reaction analysis. In the second patient, we also generated well-separated clusters of donor and recipient alleles for two single nucleotide polymorphism assays, HLA-A1/A2 and HLA-B8/HLA-B51. The absolute copy numbers of donor alleles in both single nucleotide polymorphism assays followed the same trend in four serial draws, lending credibility of this method to quantify donor-derived cell-free DNA in recipient’s plasma. Our results suggest that we can successfully design droplet digital polymerase chain reaction assays on exons 2 and 3 of human leukocyte antigen genes, which are specific for each donor–recipient pair. Moreover, we can identify different human leukocyte antigen types in paired donor–recipient samples and we can evaluate quantitation changes in cell-free DNA in recipient’s blood using serial draws.
Conclusion: It is imperative to implement a quick, non-invasive and hopefully predictive way of diagnosing rejection in vascularized composite allotransplantation recipients, so that they are not over burdened with immunosuppression and its negative side effects. Monitoring donor-derived cell-free DNA in the recipient’s plasma during follow-up visits can provide an early, minimally invasive, and personalized biomarker that enables individualized post-transplant management and fills a long-term need in vascularized composite allotransplantation patient care.
Assessment of facial nerve regeneration in vascularized composite allotransplantation: establishing a large swine animal model and literature review
Anita T Mohan, Marissa Suchyta, M Diya Sabbagh, James Schmelzer, Karim Bakri, Saad A Alsubaie, Chunfeng Zhao, Eric J Sorenson, Phillip A Low, Peter Dyck, Hatem Amer and Samir Mardini
Mayo Clinic, Rochester, MN, USA
Background: Facial composite tissue allotransplantation provides a new realm in reconstructive surgery for complex injuries. There is a critical gap in knowledge in axonal regeneration and long-term functional motor recovery. We developed a long-term survival swine hemi-facial transplantation model and present a review of available nerve regenerative models.
Methods: A total of 16 live pigs were used in this study. In phase 1, a hemi-facial composite flap was harvested isolated on the superficial temporal vessels in domestic pigs (N = 11), in conjunction with facial nerve anastomosis of the buccal, posterior auricular, and cervical branches. Nerve function was measured quantitatively using both serial compound muscle action potentials and electroneurograms for 4 months (Figure 1). At euthanasia, facial nerve branches were collected, cross-sectioned, and stained with toluidine blue. Utilizing a novel algorithm, the nerves’ axonal and fiber density, myelination ratio, and diameter were calculated along the regenerating nerve. In phase 2, five more extensive hemi-facial composite flaps were harvested in adult Sinclair pigs, and the nerve regeneration was assessed using previous methodology.
Results: All surgery was successful and long-term follow-up to 4 months (or greater) was deemed possible. In phase 1, non-invasive electroneurograms and compound muscle action potential studies demonstrated results consistent with regeneration along the nerve. Nerve regeneration could be qualitatively assessed along the buccal branch of the facial nerve that provided the most consistent reading. Electromyogram of the depressor labii superioris in phase 1 reached 37% of preoperative values at 16 weeks. Average myelin thickness and myelinated fiber diameter was comparable to control at 7 cm from the anastomosis. In phase 2, wherein muscle and nerve were harvested within the flap, no electromyogram was detected at 16 weeks. However, electroneurograms in the harvested nerve was comparable to the control side at 9 cm from the site of anastomosis. Fascicular diameters and myelinated fiber at 4 months provided supportive histological evidence of axonal regeneration (Figure 2).
Conclusion: This study validated techniques for a hemi-facial composite flap to evaluate facial nerve regeneration in a large animal model that can be utilized in vascularized composite allotransplantation research and potential to inform clinical protocols in the context of face transplant.
Reinventing extremity amputation in the era of vascularized composite allotransplantation
Matthew Jonathan Carty and Simon G Talbot
Brigham and Women’s Hospital, Boston, MA, USA
Background: The advent of vascularized composite allotransplantation as a restorative option for those suffering from limb loss has introduced a biological solution to the vexing challenges faced by amputees. While the technical aspects of limb allotransplantation have been vetted and refined over the past 20 years, our approach to amputation itself has not been updated in conjunction with these advances.
Methods: We review the reconstructive options available to provide more optimal preparation of a residual limb for downstream receipt of an allotransplantation. This review includes not only repurposing of tried and true spare parts techniques but also more recent innovations including targeted muscle reinnervation, regenerative peripheral nerve interfaces, and agonist–antagonist myoneural interfaces.
Results: We propose a new algorithm for the management of severely injured extremities not amenable to salvage, based on the availability of viable distal tissues. This algorithm describes reconstructive approaches to acute amputation designed to optimize the residual limb for subsequent vascularized composite allotransplantation.
Conclusion: We advocate for a new paradigm in acute limb amputation that frames limb loss as a reconstructive procedure designed, in part, to make the residual limb more optimized for vascularized composite allotransplantation.
Three-dimensional angiography and anatomic modeling in facial composite tissue allotransplantation research: establishing a large animal swine model
Anita T Mohan, Marissa Suchyta, M Diya Sabbagh, Karim Bakri, Saad A Alsubaie, Jane Matsumoto, Chunfeng Zhao, Hatem Amer and Samir Mardini
Mayo Clinic, Rochester, MN, USA
Background: Vascularized composite tissue allotransplantation can provide a superior reconstructive solution to restore physical integrity and critical organ function for highly complex and devastating facial injuries. There is a lack of long-term large animal survival models in vascularized composite allotransplantation research. Swine models have recognized advantages in characterization of major immunohistocompatibility complex, wound healing, and facial nerve research in trauma. To establish a large animal swine model, we used three-dimensional angiography and three-dimensional printing to determine vascular territories and anatomic relationships to inform and refine facial vascularized composite allotransplantation flap design.
Methods: A total of eight cadaveric adults and 16 live pigs were used in this study. Eight cadaveric pigs underwent selective angiography of branches of the external carotid artery using a barium sulfate and latex mixture followed by using ultra-high resolution three-dimensional computed tomographic angiography and a detailed anatomical dissection. Qualitative analysis of vascular territories and perforator distributions in facial subunits were documented. Overall, 16 live pigs underwent limited hemi-facial (N = 11) and extended hemi-facial composite tissue flaps including bone (N = 5) and auricle. Three-dimensional anatomic modeling was used in planning and surgical execution of an extended composite hemi-facial composite tissue flap with or without bone. Intra-operative laser-assisted indocyanine green fluorescence angiography was used to assess flap viability.
Results: 100% of all hemi-facial composite tissue flaps were successfully harvested with follow-up to at least 4 months, and the use of three-dimensional modeling assisted in the design of further flap modifications to incorporate bone. We demonstrated two principal vessels supplying the hemifacial tissues: internal maxillary artery and superficial temporal artery. An anatomical topography map of pig facial anatomy and perforator distribution to the facial subunits was generated to delineate safe territories for flap design in facial transplantation or reconstructive surgery using large animal swine models.
Conclusion: This study describes a new swine facial transplantation model with successful outcomes and reliable vascularity confirmed with anatomic, in-vivo computed tomographic studies. We validated techniques for a hemi-facial composite flap and long-term survival in a large animal model that can be utilized in vascularized composite allotransplantation and has applications to other realms of craniofacial research.
Targeted delivery of immune therapeutics in transplantation
Baharak Bahmani1, Mayuko Uehara1, Liwei Jiang1, Farideh Ordikhani1, Naima Banouni1, Takaharu Ichimura1, Zhabiz Solhjou1, Georg J Furtmüller2, David Alvarez3, Ulrich H von Andrian3, Kenji Uchimura4, Qiaobing Xu5, Ishaan Vohra1, Osman A Yilmam1, Martina M McGrath1, Vivek Kasinath1, Gerald Brandacher2 and Reza Abdi1
1Brigham and Women’s Hospital, Boston, MA, USA
2School of Medicine, Johns Hopkins University, Baltimore, MD, USA
3Harvard Medical School, Boston, MA, USA
4Unite de Glycobiologie Structurale et Fonctionnelle, Villeneuve, France
5Tufts University, Boston, MA, USA
Background: The key to the success of organ transplantation has been the development of potent immunosuppressive agents. However, the use of immunosuppressive agents is associated with significant toxicities and side-effects. Nanotechnology provides a great opportunity to improve the therapeutic index of immunosuppressive agents. A promising clinical application of nanotechnology is the selective delivery of immunosuppressive agents to lymph nodes to suppress alloimmunity more efficiently. High endothelial venules are specialized segments of the vasculature in the lymph node that uniquely express peripheral node addressin molecules. Peripheral node addressin molecule is recognized by the MECA79 monoclonal antibody (mAb). Here, we tested a novel platform for the localized delivery of an immunosuppressive agent to the lymph node using nanotechnology and immune engineering to exploit the affinity of MECA79-mAb for peripheral node addressin molecules.
Methods: We have synthesized a nanoparticle that encapsulates anti-CD3 and optimized our conjugation strategy to coat the surface of this nanoparticle with MECA79-mAb (MECA79-anti-CD3-NP). First, we tested the trafficking of a MECA79-mAb-conjugated nanoparticle (MECA79-NP) to a draining lymph node (DLN) in comparison with a non-conjugated nanoparticle, utilizing a murine skin transplant model (BALB/c to C57BL/6). Then, we examined its clinical efficacy and mechanism of action in a murine heart transplant model by treating recipient animals with MECA79-anti-CD3-NP and proper controls. Finally, we tested the delivery of MECA79-NP in a preclinical porcine model of limb transplantation.
Results: As compared to a non-conjugated nanoparticle, MECA79-NP accumulated in a significantly greater concentration in the draining lymph node. We observed that T cells and dendritic cells within the lymph node absorbed MECA79-NP robustly. The short-term treatment of murine heart allograft recipients with MECA79-anti-CD3-NP resulted in a significant prolongation of heart allograft survival, as compared to the controls (Figure 1). The population of regulatory T cells also increased significantly in the draining lymph node and heart allografts. Depletion of regulatory T cells abrogated the prolongation of heart allograft survival. We also noted increased trafficking of MECA-NP to the draining lymph node of a limb-transplanted pig (Figure 2).
Conclusion: This high endothelial venule-targeted drug delivery platform has the potential to improve the delivery of immune therapeutics markedly in the field of transplantation.
Characterization of pro-tolerogenic hematopoietic stem cell/mesenchymal stem cell di-chimeric cell therapy for tolerance induction in vascularized composite allograft and heart transplantation: a preliminary report
Maria Siemionow, Joanna Cwykiel, George Rafidi and Erzsebet Szilagyi
University of Illinois at Chicago, Chicago, IL, USA
Background: Supportive therapy of stem cells presenting immunomodulatory properties has been proposed to treat patients after solid organ and vascularized composite allotransplantation to minimize immunosuppression. We have developed an innovative di-chimeric cell therapy via ex vivo fusion of hematopoietic stem cells (HSCs; CD90/CD34 cells) and/or mesenchymal stem cells (MSCs) to eliminate the need for lifelong immunosuppression and induce tolerance in vascularized composite allotransplantation and solid organ transplantation. This study aimed to create and characterize phenotype, viability, proliferative, and immunomodulatory properties of HSC/HSC and HSC/MSC di-chimeric cells for future application in in vivo study.
Methods: Hematopoietic stem cells from the bone marrow of 10 ACI and Lewis donor rats and mesenchymal stem cells from the bone marrow of 10 Lewis donor rats were isolated and characterized for phenotype marker expression (CD29, CD73, CD45, CD90, and CD34) by flow cytometry. Isolated cells were stained with PKH26 and PKH67, and five HSC(ACI)/HSC(Lewis) and five HSC(ACI)/MSC(Lewis) ex vivo fusions were performed using polyethylene glycol. Created di-chimeric cells were sorted and assessed by confocal microscopy and flow cytometry for fusion efficacy, di-chimeric cell purity, and phenotype. Di-chimeric cell’s viability was assessed by trypan blue. Mitogen suppression and regulatory T-cell induction assays evaluated in vitro di-chimeric cell immunosuppressive activity.
Results: Flow cytometry and confocal microscopy confirmed creation of both di-chimeric cell lines. Di-chimeric cell exceeded 85% viability and all assessed hematopoietic and mesenchymal markers were expressed on their surface. Both di-chimeric cell lines showed in vitro immunomodulatory properties and reduced allogenic lymphocyte proliferation with respect to allogeneic hematopoietic stem cell parent cells. In vitro HSC(ACI)/MSC(Lewis) di-chimeric cell maintained levels of regulatory T cells (~7%) comparable to mesenchymal stem cells.
Conclusion: The feasibility of ex vivo fusion to create HSC/HSC and HSC/MSC di-chimeric cells has been confirmed. Moreover, the phenotype, viability, immunosuppressive activity, and regulatory T-cell induction of di-chimeric cell have been determined. Introduction of our novel donor- and recipient-specific di-chimeric cell therapy will facilitate tolerance induction and improve allograft survival in solid organ and vascularized composite allotransplantation transplantation.
What it takes to succeed: mobilizing insights from partners and caregivers of hand transplant recipients
Emily Herrington1 and Vijay S Gorantla2
1University of Pittsburgh, Pittsburgh, PA, USA
2Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC, USA
Background: In many fields of chronic care medicine, the role played by caregivers and family members in supporting patients is recognized by clinical providers. Research aimed at understanding and enhancing involvement of caregivers and family members has been published in journals of oncology, palliative care, transplantation, and psychiatry, among others—however, investigations into this aspect of the hand transplant process have not yet been robustly presented in the reconstructive transplant literature.
Methods: Through mixed qualitative methods, we investigate and describe the contributions made by caregivers to the hand transplant process, including aspects of emotional support and direct physical care and observation of graft hands and recipient health. A total of 17 oral history interviews have been conducted with hand transplant patients and their closest caregivers (5 of the 17 interviews were with caregivers). Oral history interviews comprised open-ended questions and carried out in one-on-one, exhaustive conversations ranging from 40 to 140 min per interview. The oral history process adheres to the twin principles of (1) questioning rather than measuring and (2) generating hypotheses using theoretical coding.
Results: Caregivers’ testimony of the hand transplant process illuminates their role in supporting patients through the challenges of taking post-transplant medications and completing daily therapy. Caregivers also bear witness to the physical and emotional demands of hand transplant recovery on the patient.
Conclusion: Highly involved caregivers have provided critical support to adherence efforts in many cases of hand transplantation. In this talk, we translate relevant highlights from oral history interviews with hand transplant caregivers and argue based on these data that (1) further research is needed to identify the impact of hand transplant/reconstructive transplant on caregivers’ quality of life, to develop methods for facilitating communication between hand transplant caregivers and providers, and to help caregivers navigate the challenges of reconstructive transplant; (2) increased involvement of caregivers during the evaluation process, and increased attention to their needs by behavioral health staff in the years after transplant, may be warranted because substantial burdens of longitudinal care fall on them and their level of participation can affect outcomes.
Induced pluripotent stem cell (iPS) derived Schwann cells to enhance functional recovery following nerve injury and limb allotransplantation
Barbara Kern1,2, Karim Sahane1, Bipasha Mukherjee-Clavin3, Zuhaib Ibrahim1, Chris Cashman3, Kellin Krick4, WP Andrew Lee1, Hai-Quan Mao4, Gabsang Lee3 and Gerald Brandacher1
1Department of Plastic and Reconstructive Surgery, Johns Hopkins University School of Medicine
2Department of Surgery, CVK & CCM, Charté University Medicine, BIH, Berlin, Germany
3Department of Neurology and Neuroscience, Institute for Cell Engineering, Johns Hopkins University School of Medicine
4Department of Materials Science and Engineering, Johns Hopkins University School of Medicine
Background: Stem cell–based therapies have provided new aspects for functional recovery. Utilizing human induced pluripotent stem cell–derived Schwann cells supported by the effect of nerve growth factors was investigated to improve functional recovery.
Materials and methods: Experiments were first conducted in a chronic tibial denervation and later implemented into a hind-limb transplant rat model. Human induced pluripotent stem cell–derived Schwann cells were generated through dual SMAD inhibition and isolated by fluorescence-activated cell sorting. For Schwann cell differentiation, CD49d+ cells were isolated. Growth factor delivery systems were constructed using fibrin gel containing growth factor glial cell line–derived neurotrophic factor with or without chondroitinase. Endpoints for the growth factor delivery were 5 weeks (histomorphomtery and retrograde labeling) and 12 weeks (functional analysis).
Results:Figure 1 shows the successful derivation of Schwann cell precursors; cells assume a typical Schwann cell long fusiform bipolar morphology (Figure 1(a)), stain positive to S100 (Figure 1(b)), and were also successfully transfected with a green fluorescent protein adenovector (Figure 1(c)). In growth factor delivery group, 5 weeks after repair, histomorphometry demonstrated a significant increase in the number of regenerating myelinated axons in the glial cell line–derived neurotrophic factor + chondroitinase group as compared to glial cell line–derived neurotrophic factor, chondroitinase, and negative control groups. In cellular therapy group, animals treated with induced pluripotent stem cell delivery demonstrated significantly greater axonal diameters and myelin thickness compared to control group. Electromyogram functional testing did not show any significant difference, neither at 5 nor at 12 weeks, although there was a positive trend in the induced pluripotent stem cell group observed at 12 weeks. There were no statistically significant differences in functional outcome analysis (CatWalk) between experimental and control groups.
Successful derivation of Schwann cell precursors from human embryonic stem cells: (a) typical fusiform bipolar morphology; (b) S100-immuno-positivity visualized in red with Cy5-conjugated secondary antibodies; and (c) successful transfection with GFP adenoviral vector.
Conclusion: Schwann cell precursors can be successfully isolated from human induced pluripotent stem cells. Growth factor delivery vehicles (fibrin and collagen hydrogels) and chondritinase result in higher axonal counts. Human induced pluripotent stem cells result in greater axonal diamters and myelin thickness. Further studies are needed to demonstrate functional benefits of cellular therapies for nerve regeneration.
Full-facial allotransplantation including the temporomandibular joints: an anatomical study and surgical protocol
Teresa Nunez-Villaveiran1, Vahe Fahradyan1, Edoardo Dalla Pozza1, Majid Rezaei1, Richard Drake1, Lyman Jellema2, Frank Papay1, Bahar Bassiri Gharb1 and Antonio Rampazzo1
1Cleveland Clinic, Cleveland, OH, USA
2Cleveland Museum of Natural History, Cleveland, OH, USA
Background: Face allotransplantation shifted the reconstruction paradigm of complex facial defects. Incorporation of temporomandibular joint in total face allotransplant can further improve functional outcome in these patients. The purpose of our study was to develop a surgical protocol of a total face allotransplantation including temporomandibular joint.
Methods: A total of 100 skulls and mandibles and 100 facial computed tomographic scans were evaluated to characterize the variability of temporomandibular joint dimensions. Eight fresh cadavers were injected with red-colored latex and dissected for visualization of the vascular branches entering the temporomandibular joint. Four fresh cadavers were used to perform a temporomandibular joint which included full-face transplantation. Donor allografts were harvested using a Le Fort III approach combined with a bilateral sagittal split osteotomy and temporal craniotomy to include the total temporomandibular joint. The allograft was transferred to the recipient’s face. Temporomandibular joints were secured on the zygomatic processes of temporal bones.
Results: Statistically significant difference between genders was observed in all parameters measured on dry skulls except for intercondylar and condyle-symphysis angles. There was a statistically significant difference of frontal ramal inclination between genders in computed tomographic measurements. The temporomandibular joint received 1–3 direct branches (maximal diameter: 0.7–0.8 mm) from the maxillary and middle meningeal arteries medially, and the superficial temporal artery laterally. Transplanted temporomandibular joints were located more lateral, inferior, and anterior compared to their normal anatomical position. Class 1 original donor occlusion was achieved with a normal mandibular range of motion.
Conclusion: To our knowledge, this was the first study demonstrating the technical feasibility of cadaveric temporomandibular joint which included full-face allograft procurement and transplantation.
Oncologic complications in vascularized composite allotransplant hand recipients
Allan Ramirez1, Tuna Ozyurekoglu2, Huey Y Tien2, Rodrigo Moreno2, Michelle D Palazzo2, Elkin Galvis2, Scott Farner2, Emily Goldman2, Christina Kaufman2 and Christopher M Jones1
1Jewish Hospital Trager Transplant Center, Louisville, KY, USA
2Christine M. Kleinert Institute, Louisville, KY, USA
Background: Oncologic complications occurred in three of nine evaluable hand recipients. Cancer risk is increased by systemic immunosuppression. In addition, the patients are in an age group and have lifestyles associated with increased malignancies.
Methods: Annual screening for malignancy is based on National Cancer Institute criteria. The series includes eight males and one female. The average current age is 50 ± 9 years.
Results: Patient 3 (65 years, male) was diagnosed with a marginal zone lymphoma at 18 months, which was pre-existing to transplant. The B-cell clone is still present, but reduced in number. At year 10, this same patient had a squamous cell carcinoma removed from his back. At his year-11 examination, a positron emission tomography scan performed to monitor his marginal zone lymphoma found an axillary lymph node positive for squamous cell carcinoma. The patient received radiation treatment and is currently negative. This patient spends his winters in Arizona camping. Patient 2 (53 years, male) had a squamous cell carcinoma on his right shoulder at year 16. This was removed with clear margins. At year 17, a brown macule with irregular border/coloration was noted on his right shoulder. A shave biopsy indicated lentigo, not squamous cell carcinoma. This patient works outside installing gutters. Finally, patient 8 (60 years, male) had a prostate-specific antigen of 22 at his year-5 visit. A repeat prostate-specific antigen bone scan, magnetic resonance imaging, and needle biopsy of both the testis and the iliac crest were performed. The prostate biopsy was positive and the patient was treated with Casodex, Lupron, and 44 radiation treatments. At his year-6 visit, his prostate-specific antigen was 0.37, and there was no evidence of cancer. Recently, a suspicious mole on his ear was removed which showed no evidence of malignancy. This patient is a commercial farmer. All three patients were maintained on immunosuppression while they were being treated for their malignancy.
Conclusion: Patients on long-term immunosuppression are at a higher risk for malignancies. However, the age and environmental exposure of these three individuals likely add to their risk. Nevertheless, this data can be used to council future vascularized composite allotransplant hand candidates as they decide whether the risk of immunosuppression is acceptable or not.
Multifactorial graft loss with chronic neural inflammation in a vascularized composite allotransplant hand recipient 8 years post transplant
Tuna Ozyurekoglu1, Allan Ramirez2, Huey Y Tien1, Rodrigo Moreno1, Michelle D Palazzo1, Elkin Galvis1, Scott Farner1, Tiffany Roberts3, Emily Goldman1, Christina Kaufman1 and Christopher M Jones2
1Christine M. Kleinert Institute, Louisville, KY, USA
2Jewish Hospital Trager Transplant Center, Louisville, KY, USA
3Tissue Typing Lab, Jewish Hospital Trager Transplant Center, Louisville, KY, USA
Background: A 42-year male with a right forearm amputation from an industrial accident received a unilateral transplant in 2008.
Methods: The patient recieved a Campath 1H steroid sparing regimen. At 9 months, he was switched to Tac/Siro. The first 6 years were notable for minimal rejection. The patient underwent bariatric surgery at 3 and 5 years. He had a Carroll score of 69 by year 2, with incomplete pronation and thumb abduction.
Results: Metabolic issues resulted in increase in HgbA1c and creatinine of 1.7–1.8 as early as 22 months. At year 6, denovo CII DSA developed, but because of increasing creatinine, tacrolimus was discontinued for ~18 months. Creatinine decreased, but rejection resulted in conversion back to tacrolimus at year 8. Subsequently, the patient underwent rotator cuff surgery and shortly after reported shooting pain in transplanted hand with swelling and rash, which responded to prednisone. Night pain, numbness, and sensitivity complaints continued. An electromyography or nerve conduction study confirmed severe nerve compression at wrist level. CT cortisone injection provided 75% relief but tingling/impulses remained. Five months after shoulder surgery, the patient underwent a carpal tunnel release or Guyon’s canal release. An enclosed abscess of Staphylococcus aureus in the native tissue was excised. Skin biopsy was grade 2 and biopsy of the median/ulnar nerves showed chronic inflammation. Arterial vessels showed thickening consistent with chronic rejection. At 2 weeks, the incision dehisced. A debridement and repeat closure was done with no healing. He was subsequently admitted for intravenous antibiotics and I&D with wound vacuum-assisted closure treatment. Later, two fingers became purple, and the patient was offered the option of amputation of the two fingers and a flap coverage. He requested removal of the hand, which was performed 8.9 years post-transplant. Histology showed marked arterial intimal hyperplasia. The medial and ulnar nerve showed chronic active and necrotizing acute inflammation and fibrosis.
Conclusion: The cause of graft loss was multifactorial. Inadequate immunosuppression due to metabolic changes, decreased kidney function, and multiple surgeries contributed. Increased use or trauma following rotator cuff surgery along with wound dehiscence and infection and rejection likely contributed to the vasculopathy. This case was notable for nerve pain associated with infiltration or inflammation of the nerves.
Ex-situ normothermic perfusion of human upper extremity
Vahe Fahradyan, Edoardo Dalla Pozza, Maria Madajka, Carlos Xavier Ordenana, Sayf Al-deen Said, Majid Rezaei, Frank Papay, Antonio Rampazzo and Bahar Bassiri Gharb
Cleveland Clinic, Cleveland, OH, USA
Background: Ischemia time remains a significant limiting factor for successful extremity replantation and transplantation. Compared to the cold storage, normothermic ex-situ perfusion is a novel method of limb preservation by maintaining physiologic cellular metabolism avoiding the deleterious effects of hypoxia and cooling. The purpose of our study was to establish the efficacy of normothermic ex-situ perfusion in preserving viability and function of human upper extremities.
Methods: A total of 10 upper extremities were procured from brain-dead organ donors. Five limbs were perfused using an oxygenated colloid solution at 38°C containing packed red blood cells, plasma, and albumin. Five were preserved at 4°C as a control. Electrolytes were kept within physiologic range by partial perfusate exchanges. Limb viability was assessed by muscle contractility, compartment pressure, tissue oxygen saturation, creatine kinase and myoglobin concentrations, indocyanine green angiography, and thermography.
Results: Perfused arms retained physiological parameters and function up to 51 h with a final weight change of −1.26% ± 14.15%, compartment pressure of 21.2 ± 16.39 mmHg, mean muscle temperature of 35.1°C ± 0.86°C, and tissue oxygen saturation of 90.54% ± 7.98%. Average values of final myoglobin and creatine kinase concentrations were 51330 ± 31913.86 ng/mL and 34785.8 ± 16136.54 U/L. Thermography and indocyanine green angiography depicted uniform peripheral perfusion throughout the experiment. Electrical stimulation of median, ulnar, and radial nerves displayed no muscle contraction at the beginning; however, it recovered gradually and preserved until the end of perfusion.
Conclusion: Ex-situ normothermic limb perfusion shows potential in overcoming the present standard of care (cold preservation) improving ischemia time for large segments and envisioning a radical change in the management of traumatic amputations and upper extremity transplantation.
Vascularized tongue extracellular matrix production in a porcine model
Jérôme Duisit1, Hadrien Amiel2, Jérémie Bettoni3, Adeline Dedriche2, Geoff Chiu4, Pierre Bonnefont5, Caroline Bouzin2, Pierre Gianello6 and Benoit Lengele7
2Université catholique de Louvain, Brussels, Belgium
3Departement of Maxillo-Facial surgery, University Hospital of Amiens, Amiens, France
4Royal Derby Hospital, Derby, UK
5Rouen University Hospital, Rouen, France
6SSS/IREC/CHEX, Université catholique de Louvain, Brussels, Belgium
7Department of Plastic and Reconstructive Surgery, Université catholique de Louvain, Cliniques Universitaires Saint-Luc, Bruxelles, Belgium
Background: Tongue reconstruction is a true challenge due to its very specific and complex functions, motor and sensory. Despite the most advanced autologous surgical techniques, functional outcomes remain poor. To overcome the current limitations, vascularized composite tissue engineering is thus a promising solution.
Methods: Seven porcine tongues were harvested with their vascular lingual arteries and nervous pedicles. Perfusion decellularization was achieved with a detergent-based protocol. Cell removal was established by conventional stainings and DNA quantification. The extracellular matrix structural preservation was appreciated with Masson’s trichrome and laminin stainings, three-dimensional histology, and scanning electron microscopy. Vascular bed preservation and access was assessed by angioscopy and Indian ink gel injection. To study cell compatibility, tongue extracellular matrix biopsies were cultured with C2C12 muscle progenitor cells. In vivo biocompatibility was examined by scaffold implantation in rat quadriceps for 4 weeks.
Results: Complete decellularization of porcine tongues could be obtained within 8 days. Cell clearance was confirmed by absence of nuclei on hemotoxylin and eosin sections, and a significant DNA content reduction. Masson’s trichrome staining, three-dimensional histology, and scanning electron microscopy showed a well-preserved microscopic structure. Laminin, an important factor for muscle regeneration, was highly preserved. The vascular bed was patent, for both large and small vessels. Seeded cells were viable and implanted scaffolds demonstrated a satisfying integration in the recipient muscle, at macro- and microscopic levels.
Conclusion: We could produce complete porcine tongue graft extracellular matrix, with a patent and accessible vascular tree, which was cyto- and bio-compatible. These results enable future research in whole-tongue vascularized composite tissue engineering.
Vascularized human finger decellularization: a subunit approach to hand tissue engineering
Jérôme Duisit1, Donovan Debluts2, Louis Maistriaux2, Thomas Roels2, Catherine Behets2, Pierre Gianello3 and Benoit Lengele4
2Université catholique de Louvain, Brussels, Belgium
3SSS/IREC/CHEX, Université catholique de Louvain, Brussels, Belgium
4Department of Plastic and Reconstructive Surgery, Université catholique de Louvain, Cliniques Universitaires Saint-Luc, Bruxelles, Belgium
Background: In hand surgery, conventional autologous techniques are limited for the reconstruction of lost digits, with a high impact on hand function. Finger subunit allotransplantation has been described, but is restricted by limited applications due to immunosuppressive treatment. From previous report in acellular porcine ear graft matrix production, we applied the perfusion-decellularization technique to human finger subunit grafts obtained from cadaveric source, then extended to whole hands.
Methods: Nine long-digit grafts were procured postmortem, along with their collateral ulnar and radial pedicles, from four fresh human donors at the Department of Anatomy. The specimens were decellularized by sequential arterial perfusions of heparinized saline, 1% sodium dodecyl sulfate, isopropanol, phosphate-buffered saline, and type-I DNAse. Cellular clearance was assessed by DNA quantification and hematoxylin and eosin staining. Extracellular matrix preservation was assessed by Masson’s trichrome for soft tissues and bone mineral density for phalangeal bones. Acellular samples from skin, bone, and tendon were cultured with NIH-3 T3 fibroblastic cell line for 4 days, and examined with live/dead staining. Finally, a scaffold was re-anastomosed in a porcine recipient, for a short reperfusion study. Finally, decellularization was applied to three whole human hands, and vascular tree assessed by angio-computed tomographic scan.
Results: Digital grafts were successfully decellularized, with quick epidermolysis, nail loss, and complete bleaching. Cell clearance was demonstrated by absence of nuclei on hematoxylin and eosin sections, and an overall 95.3 % DNA content reduction, compared to native tissues (p < 0.0001). Masson’s trichrome staining showed microscopic structural preservation. Decellularized phalanx mean bone mineral density was 510 mg hydroxyapatite/cm3, similar to control. Seeded NIH-3 T3 cells were viable and homogeneously distributed on all scaffolds. In vivo, blood quickly reperfused the whole scaffold; after 3 h, the vascular tree was still patent, as demonstrated by fluoroscopy, fingertip pulse, and oxygen saturation at 93%. The extension to a whole-hand graft decellularization was achieved successfully, with an excellent preservation of the superficial and deep vascular tree.
Conclusion: Following our subunit approach strategy, we could produce finger and hand extracellular matrix scaffolds from human cadaveric source, with a preserved and perfusable vascular tree. These results could represent a true alternative to upper extremity allotransplantation.
Extended normothermic ex-situ limb perfusion preserves limbs viable and functional up to 44 h
Carlos Xavier Ordenana, Vahe Fahradyan, Sayf Al-deen Said, Edoardo Dalla Pozza, Eliana Duraes, Maria Madajka, Kihyun Cho, Nadeera Dawlagala, Hirsh Shah, Rusell Frautschi, Frank Papay, Antonio Rampazzo and Bahar Bassiri Gharb
Cleveland Clinic, Cleveland, OH, USA
Background: Ischemia and reperfusion injury remains one of the major limiting factors for the success of both replantation and vascularized composite allotransplantation. Compared to cold storage of preserved/procured organs, normothermic ex-situ perfusion is a novel approach that prolongs viability of the limb by maintaining physiologic cellular metabolism avoiding the deleterious effects of both hypoxia and cooling. This study aims to develop an ex-situ normothermic limb perfusion protocol to preserve the viability and function of amputated limbs for over 24 h.
Methods: A total of 23 swine limbs were perfused using an oxygenated colloid solution at 38°C containing washed red blood cells. The first 13 limbs were used to optimize the perfusion protocol. The subsequent five limbs (Group A) were perfused for 12 h and the following five (Group B) as long as muscle contractility/peripheral perfusion was present. Electrolytes were balanced by partial perfusate exchanges. Limb viability was compared in the two groups by muscle contractility, compartment pressure, tissue oxygen saturation, indocyanine green angiography, and thermography.
Results: Perfused limbs were able to retain physiological parameters and function for 12 h in Group A and up to 44 (24–44) h in Group B. Limbs in Group A had lower final weight increase (0.54% ± 0.07 vs 14.11% ± 16.27; p = 0.008) and compartment pressure compared to Group B (16.23 ± 7.10 vs 24.75 ± 7.79; p = 0.175). Final myoglobin and creatine kinase mean values were lower in Group A compared to Group B (875 ± 291.4 ng/mL vs 1010.6 ± 323.6 ng/mL and 53,344 ± 14850.34 U/L vs 71,881 ± 20,475 ng/mL). In Group B, thermography and tissue oxygen saturation were significantly higher than in Group A (respectively, 35.37°C ± 0.69°C vs 33°C ± 1.44°C; p = 0.01 and 69.31% ± 9.3% vs 58.69% ± 8.4%; p = 0.048). Contractility and indocyanine green angiography were comparable in the two groups.
Conclusion: The normothermic perfusion protocol has the potential to significantly impact outcomes in limb replantation and transplantation. Our results suggest that limbs in the 12-h perfusion group retained better physiologic parameters at the end-point. However, the continuous optimization of the protocol allowed to maintain limb’s function and preserved peripheral perfusion for up to 44 h.
Markov decision analytic model of the cost-utility of composite tissue allotransplantation, myoelectric prosthetics, and body-powered prosthetics in bilateral transradial amputation
Heather L Baltzer1, Steven J McCabe1, Murray Krahn1 and Christina Kosar2
1University of Toronto, Toronto, ON, Canada
2The Hospital for Sick Children, Toronto, ON, Canada
Background: Canadians’ bilateral upper limb amputees have access to body-powered prosthetics, which limit functional improvement and are often rejected, and two emerging technologies: myoelectric prosthetics and composite tissue allotransplantation. The purpose of this study is to evaluate the cost-effectiveness of these three strategies from the Canadian Health System perspective.
Methods: A state transition cohort decision analytic model was used to evaluate the treatment options for improving functional status in bilateral upper limb amputees. The model reflected three treatment strategies: (1) bilateral body-powered prosthetics, (2) bilateral myoelectric prosthetics, and (3) bilateral composite tissue allotransplantation. Both quality-adjusted life years and costs were modeled over a lifetime time horizon. Utilities, probabilities, and costs were identified through a targeted literature search, local case costing, or expert opinion. Model validity was tested, base case incremental cost-effectiveness ratios were calculated, and one- and two-way and probabilistic sensitivity analyses were conducted.
Results: Over a 44-year time horizon, the preferred strategy was body-powered prosthetics, which resulted in 14.45 quality-adjusted life years at a cost of CAD281,795. Relative to body-powered prosthetics, myoelectric prosthetics and composite tissue allotransplantation had incremental cost-effectiveness ratios above the standard willingness-to-pay threshold (CAD50,000 per quality-adjusted life years) at CAD75,895 and CAD780,061 per quality-adjusted life years, respectively. Composite tissue allotransplantation was neither favored nor cost-effective in one-way sensitivity analysis. The model was sensitive to the costs and utilities of myoelectric prosthetics and body-powered prosthetics on both one- and two-way analyses. When myoelectric prosthetics device cost is <CAD31,000, myoelectric prosthetics is the preferred strategy over body-powered prosthetics and when <CAD25,000, body-powered prosthetics is not cost-effective and removed from the model. PSA demonstrated that body-powered prosthetics and myoelectric prosthetics met the willingness-to-pay threshold (CAD50,000 per quality-adjusted life years) of 57.5% and 42.3%, respectively.
Conclusion: This decision analytic model found that body-powered prosthetics is the preferred strategy using median costs; however, myoelectric prosthetics can be cost-effective when using less-expensive devices (<CAD31,000 per device), which is within a plausible range. Myoelectric prosthetics can also be cost-effective with improved effectiveness, which is expected as the technology advances in the future. The current risks and associated cost of immunosuppression for composite tissue allotransplantation do not result in a cost-effective strategy. This is a dynamic model that will change with reduced risk of immunosuppression, improved technologies, and reduced cost of myoelectric prosthetics.
Bioengineering localized and controlled drug delivery to actuate Enhanced Costimulation Blockade and promote long-term transplant survival
Poulami Majumder1, Xiomara Calderon-Colon2, Marcos Iglesias3, WP Andrew Lee3, Gerald Brandacher3, Joel Schneider1, Julia Patrone2 and Giorgio Raimondi3
1National Cancer Institute, Frederick, MD, USA
2Johns Hopkins Applied Physics Laboratory, Laurel, MD, USA
3School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: We recently demonstrated that a transient daily administration of the Jak inhibitor Tofacitinib (Tofa) combined with CTLA4-Ig exerts what we call “enhanced costimulation blockade” and promotes long-term transplant survival in a mouse heart transplant model. To minimize the systemic exposure to Tofa and maximize its immune-modulatory effect, we explored two innovative drug delivery methods based on a peptide-based hydrogel (Tofa-Hydro) and solid lipid nanoparticles (Tofa-SLN).
Methods and results: Tofa-Hydro is a safe injectable hydrogel. A one-time application of Tofa-Hydro in the area surrounding the transplanted heart (combined with systemic CTLA4-Ig) rendered long-term graft survival (mean survival time = 127 days vs CTLA4-Ig-only mean survival time = 36, p < 0.05). Importantly, application of Tofa-Hydro to a distal site ablated this synergistic improvement of survival, demonstrating the importance of the site of delivery. Tofa-SLN showed the unique property of accumulating in the lymphatics, reaching draining lymphoid tissues, and being taken up by immune cells. Tofa-SLN-conditioned dendritic cells were profoundly inhibited in their maturative response to lipopolysaccharide. These cells were less stimulatory for alloreactive T cell and worked in concert with CTLA4-Ig to minimize T-cell activation.
Conclusion: Our results highlight two promising strategies for controlled and localized immune modulation. Injectable hydrogels allow a sustained localized delivery that requires a fraction of the dose of Tofa required when delivered systemic. Tofa-SLN can be passively directed to lymphoid tissues and effectively target and modulate antigen presenting cells. Overall, these strategies can maximize the immunomodulatory impact of Tofa while minimizing its toxic side-effects.
The posterior tibial artery flap as a sentinel flap in face transplantation: technical aspects of a novel and ideal sentinel flap
Marissa Suchyta, Brian Carlsen, Hatem Amer, Karim Bakri and Samir Mardini
Mayo Clinic, Rochester, MN, USA
Background: Face transplant can enable immense functional, psychosocial, and quality-of-life improvement for patients who had exhausted all other reconstructive options. However, a continued risk of face transplant is that of immune rejection. Sentinel flaps are utilized for remote-site rejection monitoring in facial vascularized composite tissue allotransplantation, thus minimizing biopsies of the facial graft. We present the first utilization of the posterior tibial artery flap as a sentinel flap in face transplant.
Methods: The posterior tibial artery sentinel flap was procured and inset concurrently with the facial vascularized composite allotransplantation procedure. The recipient was a 32-year-old male with a history of a gunshot wound on the face. The donor was a 21-year-old man who was declared brain dead. The posterior tibial artery flap was procured based on the posterior tibial artery and vein. The flap was inset into the groin of the recipient, with the vascular pedicle anastomosed with the recipient’s lateral femoral circumflex artery and saphenous vein.
Results: The utilization of this flap enabled concurrent harvesting of the flap alongside the solid organ transplant teams, leading to more streamlined coordination. Postoperatively, the flap healed well. Drain output remained high for 4 weeks and then quickly tapered off. High output was likely due to extensive dissection around the femoral vessels to expose the lateral femoral circumflex. The flap is doing well without any issues at 12-month follow-up. Routine biopsies were performed on this transplanted tissue on a regular basis post operatively (weekly, until 2 months postop; biweekly, 2–4 months; monthly, 4–8 months, and then every 3 months).
Conclusion: This flap is an ideal donor sentinel flap due to its location far from the face transplant and solid organ procurement teams, its reliable vascular pedicle, and its ease of harvest. We demonstrate the first utilization of this flap in transplant surgery and believe that the use of this flap could maximize the ability for solid organ transplant teams to simultaneously perform solid organ harvesting while the sentinel flap is being raised, thus enabling a more streamlined process and better coordination in composite tissue allotransplantation.
Functional outcomes of the world’s first pediatric bilateral hand transplant at 32 months
Shaun D Mendenhall1, Todd J Levy2, Sandra Amaral2, Oded Ben-Amotz1, Christine T McAndrew1, Benjamin Chang2 and L Scott Levin1
1Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
2Children’s Hospital of Philadelphia, Philadelphia, PA, USA
Background: Pediatric hand transplantation is a recent addition to the field of vascularized composite allotransplantation. We hypothesized that bilateral hand transplantation in children will lead to excellent functional outcomes based on the accelerated nerve regeneration and cortical reorganization in children.
Methods: After careful patient selection, thorough preoperative planning, and repeated rehearsals by a large multidisciplinary team, we completed the world’s first bilateral distal forearm-level hand transplantation in an 8-year-old child who was already on immunosuppression following a living donor kidney transplant. The patient had undergone amputation of all four distal extremities at the age of 2 years after staphylococcal sepsis. He underwent a rigorous but carefully adapted hand therapy regimen tailored toward his interests and attention span. His functional progress has been tracked with the box and block, nine-hole peg, and Semmes-Weinstein monofilament tests, among others. Cortical reorganization has been followed with diffusion tensor magnetic resonance imaging and magnetoencephalography.
Results: At 32 months of follow up, the patient continues to progress in motor function, sensibility, and integration of the hands as his own. He has remarkably improved in his ability to provide self-care and to experience play in a manner similar to his peers. Results of the box and block and nine-hole peg tests have shown steady improvement compared to baseline (Figures 1 and 2). He has obvious functioning of the intrinsic muscles of the hands and has no evidence of clawing. His Semmes-Weinstein monofilament testing currently puts him in the “emerging normal sensation” range with many of the finger pulps with some fingers having a two-point discrimination of 8 mm. His growth plates have all remained open and his ossification centers have expanded since transplant. Non-invasive brain imaging has demonstrated a reversal of the massive cortical reorganization associated with amputation back to similar patterns to the pre-amputation state.
Conclusion: Functional outcomes of bilateral hand transplantation in a child at 32 months are very promising in terms of motor and sensory recovery, and brain cortical reorganization.
Virtual surgical planning and computer three-dimensional modeling in face transplantation
Marissa Suchyta, Karim Bakri, Uldis Bite and Samir Mardini
Mayo Clinic, Rochester, MN, USA
Background: Three-dimensional computed tomographic imaging, computer modeling, and virtual surgical planning offer practical tools for advanced head and neck reconstruction and composite facial allotransplantation. Virtual surgical planning has demonstrated benefits in surgical accuracy and in reducing operative time in craniofacial reconstruction. However, the effectiveness of three-dimensional surgical guides and accuracy of surgical planning in face transplant has not previously been investigated. Furthermore, we perform novel investigation of the correlation between surgical planning and esthetic outcome through cephalometric analysis. We present the use of virtual surgical planning and three-dimensional computational modeling in cadaveric face transplantation.
Methods: A total of 17 pairs of recipient and donor fresh cadaveric head specimens underwent a computed tomographic scan and virtual surgical planning of a Le Fort III–based facial segment including the distal mandibular segment. The face transplant team collaborated with a team of biomedical engineers to create patient-specific three-dimensional printed models, cutting guides, and positioning guides according to the virtual surgical plan. These guides were then utilized to perform the cadaveric face transplantation. The postoperative reconstructed recipient underwent a second computed tomographic scan. Scans were three-dimensional reconstructed to determine osteotomy and positional accuracy, volumetric measurements for both donor and recipient, and reconstruction. These measurements were then analyzed to determine surgical plan accuracy.
Results: Overall, 17 cadaveric facial transplantation simulations were completed. Postoperative reconstruction analysis demonstrated that the three-dimensional surgical guides enabled execution of the surgical plan to an extremely high degree of accuracy. The resultant osteotomies of the zygoma, posterior nasal cut, pterygoid, and mandible were all 0–4 mm of the surgical plan. There was no significant difference in volumetric measurements of the predicted and actual results of the skull base, mid-face, and distal mandible.
Conclusion: Virtual surgical planning and computer-aided design and manufacturing have had a major impact on craniofacial and head and neck reconstruction. This study demonstrates that virtual surgical planning can improve both planning and accuracy outcomes in composite facial allotransplantation as well as increase efficiency and precision of complex bone osteotomies and reconstruction.
What are ethicists’ current views on face transplant? The first large-scale survey study
Marissa Suchyta, Richard Sharp, Hatem Amer, Elizabeth Bradley and Samir Mardini
Mayo Clinic, Rochester, MN, USA
Background: Face transplant can offer functional and esthetic restoration to patients who have exhausted the armamentarium of reconstructive options, thus improving quality of life and psychosocial integration. Ethical issues in face transplant still abound, including practical questions of patient selection. Despite these current controversies, there has been no study regarding ethicists’ viewpoints regarding face transplant.
Methods: A large-scale online survey of attendees of the 2015 International Conference on Clinical Ethics Consultation (N = 401) was performed to assess ethicists’ opinions on issues in face transplant. Questions were asked regarding the risk–benefit ratio of immunosuppression, permissibility of face transplant for more recipient subpopulations (including children and blind patients), donor–recipient age, gender, and ethnicity mismatches, and ethics committee make-up.
Results: Among 84 respondents, 84% agreed it is permissible to perform a face transplant on an adult with no medical contraindications as well a demonstration of high permissibility toward performing other types of vascularized composite allotransplantation. The majority of respondents agreed that it is permissible to perform a face transplant on a child or blind recipient. An issue of continued concern was risk of immunosuppression, with a steep decrease in acceptability responses when the risk of immune rejection was increased. Respondents had a high threshold of permissibility for ethnic mismatches between donor and recipient, and 43% reported it is permissible to have a gender mismatch. A 10-year age difference between donor and recipient was the most commonly accepted. Free text additional responses stressed the necessity of clear communication, questions of ethics of consent, and concerns about transplants in vulnerable subpopulations. Questions regarding the ideal composition of a face transplant ethics committee demonstrated consistent consensus on the roles that should ideally be represented.
Conclusion: This study provides insight into ethicists’ viewpoints on face transplant, which demonstrates a high level of permissibility toward the procedure. This may be due to the early success of face transplants and the shifting ethical issues in the field to practical aspects of the procedure. This research also provides guidance to programs regarding questions of donor and recipient selection, ethics committee composition, and offers insight into strengthening the ethical framework of the field.
A novel multi-thermic, antiseptic, and anthropomorphic system for ex-vivo face perfusion
Joanna Wolf Etra, Damon Cooney and Gerald Brandacher
School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: Facial disfigurement is profoundly disabling, and great relief follows resolution by facial transplantation, now a technical reality at multiple centers worldwide. However, distance between potential donor and recipient is a significant obstacle in allograft availability, and cold-ischemia time constraints prevent in-depth cross-matching and pretreatment. Hypothermic perfusion has shown immediate functional benefit in transplanted kidneys, and oxygenation and brief subnormothermia have shown benefits in perfusion homogeneity in experimental hearts. Moisture-managing, ergonomic support surfaces are beneficial for skin tissue integrity. We have combined these elements anticipating an additive effect with the goal of improved face function and tissue viability at 24-h preservation duration.
Methods: We have designed new functional modules onto an existing perfusion system including a radiant in-line perfusate sterilizer, heater for subnormothermia, and a perfusion bioreactor configured for faces. Along with our collaborators, we have engineered vapor-transporting, anthropometrically-sized support surfaces, located in the bioreactor’s oxygenated headspace. A swine hemi-facial flap was designed on a carotid pedicle. The flap was surgically mobilized, flushed, and placed into the pre-cooled perfusion machine with optimized perfusate. Pressure, flow, temperature, and perfusate chemistry will be measured at set intervals as subnormothermia maintained for 60 min at higher pressure followed by decrease in both using a thermal camera to image the temperature response. After 24-h preservation, the weight and chemical effect on the hemiface is determined.
Results: Successful swine hemifacial grafts were harvested containing muscle, bone, oral mucosa, and skin on a carotid pedicle. Adequate flap perfusion was confirmed with dye studies. Preliminary results offer insight into the ability of the perfusion device to maintain uniformity and consistency of thermal modulation and pressure with minimal edema. These results will optimize the perfusate for tissue support without significant mechanical damage to the tissue.
Conclusion: This study aims to show feasibility in achieving uniform perfusion, acceptably minor edema, and a viable, functional face graft suitable for transplantation following 24-h preservation. This highly-translatable approach addresses key hurdles to prolonged vascularized composite allotransplantation perfusion preservation. These technical elements for face preservation could be rapidly applied in potential face transplant recipients by implementing key modifications to existing clinical kidney perfusion systems.
Defining T-cell subsets involved in rejection of vascularized composite allografts
Veronika Malek1, Georg J Furtmüller2, Byoung Chol Oh2, Madeline Fryer3, Xianyu Zhou2, Marcos Iglesias2, Giorgio Raimondi2, Gerald Brandacher2 and Damon Cooney2
1Johns Hopkins University, Baltimore, MD, USA
2School of Medicine, Johns Hopkins University, Baltimore, MD, USA
3University of Massachusetts Medical School, Worcester, MA, USA
Background: Vascularized composite allotransplantation is a clinically feasible therapeutic option for complex tissue defects. The highly immunogenic skin component of vascularized composite allotransplantation represents a particular therapeutic challenge with more than 85% of allograft recipients experiencing at least one acute cellular rejection episode. An improved understanding of acute skin rejection in vascularized composite allotransplantation could elucidate possible mechanisms and reveal novel therapeutic targets.
Methods: We performed orthotopic hind limb transplantats between fully mismatched mouse strain combinations. Male wild-type (Wt) BALB/c were donors and C57BL/6 Wt, RORγT−/−, IL-4−/−, T-bet−/−, and Foxp3DTR were recipients. Mice were assessed daily for rejection. Tissue biopsies, histology, tissue digestion and T-cell tissue extraction for flow analysis were performed on postoperative day 8. Treatment groups consisted of C57BL/6 Wt mice receiving 2.0 mg/kg/dTarolimus, MR1 + CTLA4-Igor MR1 + CTLA4-Ig + total body irradiation.
Results: All untreated mice underwent acute cellular rejection. Analysis of CD4+ T cells revealed Tbet+ cells as predominant in the skin of RORγT−/−, IL-4−/− and Foxp3DTR groups. In the spleen, RORγT−/−, IL-4−/− and T-bet−/− mice had predominantly Foxp3+ cells. For the untreated Wt control, Tbet+ cells predominated in both tissues. Treated animals showed no visual rejection signs at the time of tissue harvest. Tacrolimus resulted in a significantly higher relative Tbet+ and lower Foxp3+ expressions in the skin, compared to the co-stimulation blockade (Figure 1). In the spleen, Foxp3+ cells were predominant in all treatment groups.
All untreated mice underwent acute cellular rejection with erythema and epidermolysis of the skin that progressed to necrosis (C-L). However, groups showed variance in the duration of each rejection stage (B). The untreated wild-type controls rejected their allografts on POD 10, while the mean allograft survival time for both IL4-/- and Foxp3DTR animals was 9 days. In contrast, Tbet-/- recipients had a mean survival time of 14 days and RORγT-/- mice had a significantly prolonged allograft survival of 17 days (A).
Conclusion: Our findings reveal a tissue-specific accumulation pattern of CD4+ T cells. The preferential sequestration of Tbet+ cells in allograft skin and spleen affirm the importance of Th1 cells in acute cellular rejection. Tacrolimus lead to a discrepancy between local and systemic T-cell phenotypes. This differential effect of immunosuppression offers a possible explanation for the high frequency of acute cellular rejection and should be explored further.
In vitro and in vivo characterization of human hematopoietic chimeric cells: a novel strategy to induce tolerance in transplantation
Maria Siemionow, Ewa Bryndza Tfaily, Katarzyna Futoma, Joanna Cwykiel, George Rafidi, Malgorzata Cyran, Rafal Gendek and Erzsebet Szilagyi
University of Illinois at Chicago, Chicago, IL, USA
Background: Cell-based therapies represent a promising approach for tolerance induction in transplantation. We propose a new cell therapy of the ex vivo created human hematopoietic chimeric cells as an alternative approach to bone marrow–based therapies in support of solid organ and vascularized composite allograft transplantation. This study aimed to characterize in vitro the phenotype, genotype, clonogenic and tolerogenic potential of human hematopoietic chimeric cells, and assess in vivo cytotoxicity and safety of human hematopoietic chimeric cells in a nude rat model.
Methods: A total of 30 ex vivo fusions were performed to create human hematopoietic chimeric cells. Briefly, CD34+ cells isolated from two unrelated bone marrow donors were stained separately by PKH26 and PKH67 and fused with polyethylene glycol. Double PKH26 and PKH67 stained cells were sorted and subjected to further analysis. Flow cytometry, confocal microscopy, PCR-rSSOP (polymerase chain reaction–reverse sequence-specific oligonucleotide probe), FISH, colony forming unit assay, real-time polymerase chain reaction, TUNEL, and COMET assay were used to characterize phenotype, genotype, clonogenic and tolerogenic potential, cytotoxicity, and DNA stability of created human hematopoietic chimeric cells. Migratory pathways of human hematopoietic chimeric cells following intraosseous delivery (n = 6) were assessed in vivo in athymic nude rat model by confocal microscopy and flow cytometry.
Results: Flow cytometry and confocal microscopy confirmed fusion of CD34+ cells. Human hematopoietic chimeric cells expressed hematopoietic markers, such as CD34, CD133, CD117, CD4, and CD19, as showed by flow cytometry, and shared human leukocyte antigen class I and II specific for both fusion donors as confirmed by PCR-rSSOP. COMET assay determined that human hematopoietic chimeric cells maintained DNA stability. After fusion, ~99% of human hematopoietic chimeric cells were viable with low (1.2%) level of apoptosis. The percentage of polyploid cells was low (0.48%). Human hematopoietic chimeric cells differentiated into myeloid and erythroid progenitor cells, and presented tolerogenic potential by expressing pro-tolerogenic cytokines: interleukin-10 and transforming growth factor-β. Human hematopoietic chimeric cells were present in the peripheral blood and lymphoid organs of athymic nude rat recipients up to 6 weeks after intraosseous injection. No human hematopoietic chimeric cells cytotoxicity toward recipient’s spleen, liver, or lymph nodes was observed.
Conclusion: We successfully characterized in vitro the viability, phenotype, genotype, DNA stability, and clonogenic and tolerogenic properties of human hematopoietic chimeric cells. In vivo experiments confirmed migratory properties, long-term survival and safety of human hematopoietic chimeric cells. Application of human hematopoietic chimeric cells as a supportive therapy represents a new approach for tolerance induction in vascularized composite allograft transplantation.
Belatacept and rapamycin with short-term use of tacrolimus delay allograft rejection in a novel, large animal vascularized composite allotransplantation model
Tarek Y Elgendy1, Deokyeol Kim2, Mattias Waldner2, Alan Zahorchak1, Mohamed Ezzelarab1, Wensheng Zhang2, Marta Minervini3, Kia M Washington2, Mario G Solari2 and Angus W Thomson1
1Thomas E. Starzl Transplantation Institute, University of Pittsburgh, Pittsburgh, PA, USA
2Department of Plastic Surgery, University of Pittsburgh, Pittsburgh, PA, USA
3Department of Pathology, University of Pittsburgh, Pittsburgh, PA, USA
Background: Vascularized composite allotransplantation is a clinical reality with over 80 hand and 20 facial transplants to date globally.1 Although costimulation blockade with CTLA4-Ig (belatacept) and rapamycin together with bone marrow transplantation–based therapy has shown encouraging results in solid organ transplantation,2 its efficacy has remained unclear in vascularized composite allotransplantation, especially without donor bone marrow components. The aim of this study was to evaluate whether belatacept and rapamycin with or without short-term3 tacrolimus, a calcineurin inhibitor, could prolong allograft survival in a novel major histocompatibility complex–mismatched swine vascularized composite allotransplantation model that did not contain donor bone tissue.
Methods: A total of seven transplants were performed in MGH mini-swine across a full major histocompatibility complex mismatch and were assigned into control and experimental groups. Vertical rectus abdominis musculocutaneous composite flaps were transplanted on one side of the recipients’ necks. Control animals were treated with rapamycin and belatacept immediately after the surgery. In the experimental groups, tacrolimus was administered from postoperative days 0–13, followed by rapamycin and belatacept, which were started on day 0 or 7. Allograft survival was compared among the groups by clinical assessment and histological analysis.
Results: Six allografts survived immediately after transplantations and one technical failure was noted due to arterial insufficiency. Vascular characteristics and ischemic time were similar to an established hind-limb transplantation model.4 In the control group (no tacrolimus), allografts reached acute grade-I rejection by day 9 after transplant and were fully rejected by day 20. In the experimental groups (tacrolimus), allografts reached grade-I rejection on day 33 and were fully rejected by day 59.
Conclusion: Short-term tacrolimus and delayed belatacept or rapamycin therapy offer promise to delay early acute rejection and prolong allograft survival in vascularized composite allotransplantation. The vertical rectus abdominis musculocutaneous surgical model can be used in various preclinical trials for evaluating strategy to promote donor-specific tolerance without the influence of donor bone marrow components.
Proximal and distal forearm-level transplantation using virtual surgical planning and three-dimensional-printed cut-guides for improved pre-operative planning and osteosynthesis
Shaun D Mendenhall1, Joshua T Mirrer1, Oded Ben-Amotz1, Christine T McAndrew1, Benjamin Chang2 and L Scott Levin1
1Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA, USA
2Children’s Hospital of Philadelphia, Philadelphia, PA, USA
Background: One of the technical challenges of upper extremity transplantation is achieving adequate cortical contact of the radius and ulna to provide a good healing osseous surface without disrupting the distal radio ulnar joint. Recently, three-dimensional modeling and virtual surgical planning have been utilized for enhanced preoperative planning and surgical execution for complex bony reconstructive surgery. We hypothesized that the use of virtual surgical planning and three-dimensional-printed cut-guides for hand transplantation will optimize preoperative team planning, precision and accuracy of transplant osteotomies/osteosyntheses, and decrease ischemia time.
Methods: Virtual surgical planning and three-dimensional-printed custom cut-guides were first utilized in nine hand transplant cadaver rehearsals followed by two clinical cases of bilateral hand transplantation. We rehearsed transplantation at the specific level of amputation of our patients on the waiting list. Each level of transplant had a custom cut-guide that was affixed to the donor and recipient bones with K wires (Figures 1 and 2). Predrilling of screw holes was performed through the cut-guides followed by osteotomies. Once this was complete, the donor limbs were plated and the transplant osteosynthesis was performed.
Preoperative virtual surgical planning for distal forearm transplant in a patient with a partial hand.
Intraoperative photo of a hand transplant recipient with custom 3D-printed cut-guides in place.
Results: Although there was a small learning curve with utilizing the custom cut-guides for hand transplant osteosynthesis, after two rehearsals, surgeon comfort level and time for osteosynthesis surpassed traditional free-hand osteosynthesis. Furthermore, the accuracy of osteosynthesis, the bone-to-bone contact, and revision rate all improved. In our two clinical cases, we saved approximately 1 h of ischemia time compared to our first bilateral proximal forearm transplant case that was done with free-hand osteosynthesis. The virtual surgical planning proved efficient for both proximal and distal forearm-level transplants.
Conclusion: The use of virtual surgical planning with custom three-dimensional cut-guides offers a novel technique for upper extremity transplantation osteosynthesis. The precision of osteotomies with three-dimensional-printed cut-guides offers a time efficient, accurate, and reliable alternative to free-hand osteosynthesis in hand transplantation.
Effects of static cold storage, pulsatile hypothermic perfusion, and pulsatile near-normothermic perfusion on the metabolism and function of rat hind-limb allografts
Kagan Ozer, Emre Gok, Carrie Kubiak and Stephen Kemp
University of Michigan, Ann Arbor, MI, USA
Background: Static cold storage is currently the standard of care for the preservation of vascularized composite tissue allografts. This approach not only limits the time available to perform the procedure but also has detrimental effects on the muscle microcirculation, resulting in extensive damage particularly during the reperfusion phase. Continuous machine perfusion may have the potential to change the current practice. However, ideal perfusion parameters including the perfusate and the temperature are currently unknown. In this study, we aimed to test competing perfusion modalities on a cost-effective vascularized composite allotransplantation model established to study neuromuscular regeneration.
Methods: A total of 60 male Lewis rats were distributed into 8 groups according to Table 1. Amputated limbs in groups 6, 7, and 8 were perfused using custom-made mini ex-situ perfusion system for 6 h (Table 1). All transplantations were performed between Lewis rats (isograft) eliminating the confounding effects of potential immune rejection. Evaluations were performed at the completion of sciatic nerve regeneration in 3 months after the transplantation. Extensor digitorum longus muscle force was used as the primary outcome measure in this study. Metabolomic results including five energy pathways and nerve axon counts are currently pending.
Results: Among perfusion groups and static cold storage, near-normothermic pulsatile perfusion using diluted blood and plasma exchange provided the best outcome after 6 h of perfusion. Maximum twitch and titanic force measurements in this group showed no statistically significant difference compared to immediately transplanted limbs with 75 min of ischemia (p > 0.05), while other groups had significantly lower values (p < 0.05) on both parameters. Interestingly, cold preserved allografts (static G5, and dynamic pulsatile G6) demonstrated very low compound muscle action potential amplitude indicating axonal loss, despite relatively preserved twitch and titanic forces, which reflects.
Conclusion: Pulsatile perfusion at hypothermic temperatures using histidine–tryptophan–ketoglutarate solution is superior to static cold storage in protecting limb allografts after 6 h of perfusion. Pulsatile perfusion at near-normothermic temperatures is superior to all other modalities only if combined with continuous plasma exchange. Finally, hypothermic temperatures appear to affect the nerve structure more than the muscle.
What has gone well: 20 years of follow-up in a unilateral hand transplant recipient
Christopher M Jones1, Huey Y Tien2, Rodrigo Moreno2, Michelle D Palazzo2, Elkin Galvis2, Scott Farner2, Allan Ramirez1, Emily Goldman2, Christina Kaufman2 and Tuna Ozyurekoglu2
1Jewish Hospital Trager Transplant Center, Louisville, KY, USA
2Christine M. Kleinert Institute, Louisville, KY, USA
Background: In 1999, a hand transplant was performed on a 37 year old male recipient. In January of 2019, he will be the first vascularized composite allograft recipient to achieve 20 years of graft survival. This case and this gentleman serve as an example of what can go well in vascularized composite allograft.
Methods: A large and multidisciplinary team of surgeons, physicians, researchers, therapists, nurses, administrators and our local Organ Procurement Organization (KODA) established the collaborative Louisville vascularized composite allograft program. Based on medical, psychological and social support data, the first patient listed for transplant was a 37-year-old EMT who lost his dominant left hand in a fireworks accident 13 years previously. His history was significant for insulin dependent diabetes mellitus since the age of 27. He was listed for transplant on 11 December 1998 and received a mid-forearm allograft on 24 January 1999. Immunosuppression consisted of Simulect induction, and standard tacrolimus/MMF/prednisone. Tacrolimus target levels were maintained 8–10 ng/mL until year 3.
Results: The patient recovered some return of intrinsic muscles and a peak Carroll score of 72, with recent scores of 60. The patient had two episodes of grade-3 rejection in the first year post transplant and none since. He had one grade two skin biopsy in year 16. Edema in lower extremities and in the hand, and cold related vasoconstriction have presented intermittently. His serum creatinine was 1.0 at the time of transplant, and rose to 1.3–1.5 in the first year post transplant, and have remained 1.3–1.9 to date. His latest creatinine is 1.6. Mild focal vasculopathy is present in the native and transplanted hand. His graft is remarkable for a lack of fibrosis, stiffness or other markers of chronic rejection.
Conclusion: This patient has had a positive course, and serves as an ambassador for the field of hand transplantation, actively participates in the education of hand transplant candidates and serves as UNOS VCA committee member. In retrospect, his case is remarkable for higher than average levels of tacrolimus in the first two years post-transplant, and a lack of significant acute or chronic rejection in the late post-transplant period.
Adapting an evidence-based communication training program to optimize requests for vascularized composite allografts
Heather M Gardiner, David Sarwer and Laura A Siminoff
Temple University, Philadelphia, PA, USA
Background: The single-most important rate limiting step to advancing the science of vascularized composite allografts and its therapeutic applications is the willingness of the family decision makers of solid organ donors to donate vascularized composite allografts in sufficient numbers to meet the growing demand. We review findings from our previous research in organ and tissue donation to inform the modification of an existing evidence-based training for Organ Procurement Organization request staff to make requests for vascularized composite allograft donation.
Methods: Data were collected via semi-structured telephone interviews with over 2500 family decision makers and surveys of nearly 900 Organ Procurement Organization requesters from 2004 to 2017. Across three separate studies, we assessed the impact of the intervention, “Communicating Effectively about Donation (CEaD),” which trains Organ Procurement Organization staff to use key elements of relational/affective, instrumental, and persuasive communication when making requests for solid organ and tissue for transplantation and research
Results: Improvements in family authorization were observed from pre- to post-CEaD training in all three studies. In the first study (2004–2007), authorization increased from 46.3% to 55.5% (p = 0.07) among 22 requesters employed at one Organ Procurement Organization. The second study (2008–2011) saw increases in authorization for both novice (78% to 89%, p = 0.03) and experienced requesters (89% to 92%, p = 0.03). In its most recent test (2013–2017), the CEaD resulted in increased authorization among requesters with three or more years’ experience (70% to 77%, p = 0.01). Importantly, the intervention also improved requesters’ comfort discussing and answering questions about donation and led to increased use of relational communication with family decision makers. Similarly, family decision makers reported greater satisfaction with the request process post-training.
Conclusion: These findings as well as data collected from semi-structured telephone surveys of Organ Procurement Organization requesters (N = 150) and focus groups with the general public and a sample of donor families will enable adaption of the CEaD for vascularized composite allograft requests. The adapted training program will add to requesters’ existing skillset, improve the quality of requests made for vascularized composite allograft donation and enhance the experiences of families approached about this donation option. The overall goal of the CEaD–vascularized composite allografts is to increase the number of vascularized composite allografts available for transplantation, a prerequisite for advancing the field.
A novel murine orthotopic forelimb transplantation model that allows for reliable assessment of functional recovery resulting from nerve regeneration
Barbara Kern1,2, Sami Tuffaha1, Joshua Budihardjo1, Georg J Furtmüller1, Jason Park1, Ahmet Hoke1, WP Andrew Lee1 and Gerald Brandacher1
1School of Medicine, Johns Hopkins University, Baltimore, MD, USA
2Charité, Berlin, Germany
Background: Improved nerve regeneration and functional outcomes would greatly enhance the utility of vascularized composite allotransplantation. However, research aimed at achieving this goal has been limited by the lack of a functional vascularized composite allotransplantation animal model.
Methods: To address this problem, we developed a novel rat mid-humeral forelimb transplant model with end-to-end cuff anastomosis of the brachial artery and vein (Figure 1) in which functional recovery is tested by scoring component forelimb motions involved with the IBB forelimb scale and by measuring progressive return of grip-strength within the transplanted forelimb at weeks 5, 7, 10, and 12 after transplantation. Median nerve histomorphometry and flexor digitorum myofiber cross-sectional area analysis was investigated at the end point (12 weeks).
Results: After an initial learning curve, forelimb transplantation can be performed with consistent success (operative time: 180–220 min). Grasping skills between the transplanted group and the cut-and-repair group showed no statistical significance, neither on weeks 5, 7, or 10 nor on week 12 (Figure 2). The transplanted group regained grip strength with a maximum of 56.4% ± 6.5% of baseline. Similar results were observed within the IBB scale measurements, mean score of transplanted group resulted in 2.8 ± 0.37 SEM at week 12 (1.7 ± 0.33 at week 5), which was comparable to cut-and-repair group with 2.6 ± 0.26 at week 12 (2.0 ± 0.0). Immunohistochemistry of flexor digitorum muscle showed greater myofiber cross-sectional area in the experimental group than in the negative control group (719.5 ± 56.9 SEM µm2 vs 224.7 ± 38.7 SEM µm2; p < 0.0001). Myofiber cross-sectional area of naive animals measured an average of 1325.7 ± 19.1 SEM µm2. Histomorphometric analysis of regenerating nerve fibers in the median nerve demonstrated robust axonal regeneration in the experimental group, with greater number and density of fibers in the experimental group than in naive median nerves (fiber count: 5324 ± 266 vs 2997 ± 231 SEM; p = 0.004; fiber density: 9500 ± 191 vs 25,269 ± 2664 fibers/mm2; p = 0.017).
Conclusion: Rat forelimb transplantation may represent the first vascularized composite allotransplantation model that allows for reliable and reproducible measurement of functional recovery. Statistical analysis of grip strength data will elucidate the degree of variability at each time-point and the degree of improvement from week to week as compared to non-innervated controls.
Psychosocial predictors of outcomes in upper extremity vascularized composite allotransplantation
Sarah Kinsley, Shah Sejal, Robert Edwards, George Dyer, Bohdan Pomahac, Matthew Jonathan Carty and Simon G Talbot
Brigham and Women’s Hospital, Boston, MA, USA
Background: Anecdotal evidence suggests that psychosocial factors are important in determining outcomes in vascularized composite allotransplantation patients. We have attempted to better delineate which variables are most predictive.
Methods: A survey was sent to all centers that have performed an upper limb transplant, with data collected and sent to the IRHCTT Registry. Data were collected on subjective evaluations of patients’ mood, anxiety, dependence, functioning, quality of life, posttraumatic stress disorder, pain, timeliness, compliance, participation, and social support.
Results: Approximately 26 centers had performed 98 transplants in 62 individual patients at the time of the survey. All centers were emailed a survey and surveys were re-sent 3 times. Centers who did not respond were personally approached at the ISVCA Conference in 2017. Responses were received regarding 42 (67%) patients. Survey responses were scored between 1 and 5 suggesting that patients with a wide range of psychosocial variables have been transplanted. On preliminary review, there are increased episodes of rejection in transplanted patients with difficult interpersonal functioning with dependent personality traits, anxiety, and/or depression.
Conclusion: Psychosocial factors are important in the success of upper extremity transplantations. In this study, we have examined factors assessed by clinicians and compared these with known outcomes in the IRHCTT. Ongoing work is examining qualitative data, interviewing patients, families, and clinicians; and finally attempting to quantify the significance of these factors with model scenarios.
Recognizing emotional expression as an outcome of face transplantation
Miguel I Dorante1, Branislav Kollar1, Sotirios Tasigiorgos1, Elif Koçak1, Sebastian Fischer1,3 and Bohdan Pomahac1
1Brigham and Women’s Hospital, Boston, MA, USA
2BG Clinic Ludwigshafen, Ludwigshafen, Germany
Background: Face transplantation outcome assessments focus on recovery of motor, sensory, and vital functions of the allograft. Although those measures are important, face transplantation recipients seek to reintegrate into society where facial emotional expression is integral to life-enhancing moments. Despite high relevance, limited data are available about this topic in face transplantation. This study aims to fill the gap by establishing an objective method to assess emotional expression as an outcome in face transplantation.
Methods: We used FaceReader (Noldus, Leesburg, VA) to perform software-based video analysis on 46 video recordings of 7 face transplantation recipients. Recordings were taken at 6-month intervals over a post-transplantation follow-up period of 8 years (range: 6 months–8 years, mean: 4.3 years). Video analysis relies on the Facial Action Coding System and Active Appearance Method to evaluate a series of facial movements performed by face transplantation recipients in each recording. Facial expressions are given an intensity score value between 0 (absent) and 1 (fully present) for the presence of six basic expressions of happiness, sadness, anger, fear, surprise, and disgust. According to the manufacturer, intensity scores above 0.5 are considered to be detectable by a human observer, with improvement or deterioration of emotional expression between time points determined by changes greater than or equal to 0.1.
Results: Preliminary data from one full- and one partial face transplantation recipient at three time points (6 months, 2 years, and 4 years post-op) show maximum intensity score values for happiness, sadness, anger, fear, surprise, and disgust as follows: 0.39, 0.50, 0.05, 0.76, 0.78, and 0.03 for Patient 1; 0.46, 0.60, 0.28, 0.34, 0.53, and 0.09 for Patient 2. Results suggest that happiness, sadness, fear, and disgust are facial emotional expressions that can be objectively recognized in face transplantation recipients. Happiness, surprise, and fear improved over 4 years by 0.11, 0.46, and 0.12 for Patient 1, and 0.41, 0.28, and 0.19 for Patient 2. The most improvement was seen between 6 months and 2 years post-op. This is an ongoing study.
Conclusion: This study is proof of concept that objective measurement of facial emotional expression is possible for face transplantation recipients via software-based video analysis.
Decellularized vascularized nerve scaffolds for the repair of peripheral nerves
Tsering Wüthrich1, Ioana Lese2, Jérôme Duisit3, Louis Maistriaux4, Ekkehard Hewer1, David Haberthür1, Cédric Zubler1, Ruslan Hlushchuk1, Pierre Gianello5, Benoit Lengele6, Robert Rieben1, Esther Vögelin1, Radu Olariu2 and Adriano Taddeo1,2
1University of Bern, Bern, Switzerland
2Inselspital, University Hospital, University of Bern, Bern, Switzerland
4Université catholique de Louvain, Brussels, Belgium
5SSS/IREC/CHEX, Université catholique de Louvain, Brussels, Belgium
6Department of Plastic and Reconstructive Surgery, Université catholique de Louvain, Cliniques Universitaires Saint-Luc, Bruxelles, Belgium
Background: Peripheral nerve injuries are devastating, life-altering injuries. Decellularized scaffolds, which act as guide-conduits for the regenerating nerves, represent a promising approach to increase availability of nerve grafts and effective nerve reconstruction when used as vascularized grafts. Here, we report the development of a vascularized nerve scaffold in which the preserved vascular tree can be used for perfusion and recellularization in order to improve cell engraftment, supply of nutrient and, thus, regeneration and functional recovery.
Methods: Seven vascularized porcine sciatic nerve scaffolds were retrieved and perfusion-decellularization was applied using a SDS/Triton X detergent protocol. Decellularized vascularized porcine sciatic nerve scaffolds were characterized analyzing cell and DNA content and preservation of extracellular matrix, vascular tree and cytokine content. Reendothelialization of decellularized scaffolds was conducted with porcine-aorta endothelial cells in a perfusion-bioreactor.
Results: Scaffold vascularization was confirmed by angiography before and after decellularization. Morphologic examination of decellularized vascularized porcine sciatic nerve scaffolds and analysis of the DNA content demonstrated cell and antigen clearance. Extracellular matrix content and structures of the nerve fascicles were preserved. The vascularized porcine sciatic nerve scaffolds’ vasculature was characterized in three dimensions using micro-computed tomography (microCT) imaging and showed optimal vasculature preservation down to the capillary level. Cytokine quantification demonstrated a strong preservation of growth factors and reduced preservation of pro-inflammatory cytokines. Reendothelialization experiments showed porcine-aorta endothelial cell viability and engraftment with repopulation of the scaffold’svessels.
Conclusion: This study shows that perfusion-decellularization can be used to generate vascularized nerve scaffolds with preserved extracellular matrix structure and a functional vascular tree, which can be reendothelialized in vitro. As compared to non-vascularized conduits, vascularized engineered nerve scaffolds may represent an ideal approach for promoting better nerve regeneration in larger nerve defect reconstructions.
Psychosocial factors affecting recipients of vascularized composite allografts
Sarah Rasmussen, Carisa Cooney, Jaimie Shores, WP Andrew Lee, Dorry Segev and Macey Henderson
School of Medicine, Johns Hopkins University, Baltimore, MD, USA
Background: While vascularized composite allotransplantation is an increasingly successful therapy, medication non-adherence appears to be an important cause of graft loss. Psychosocial factors predict medication adherence in solid organ transplant recipients, and early experiences suggest psychosocial factors may also play an important role in the success of vascularized composite allotransplantation.
Methods: We surveyed vascularized composite allotransplantation recipients to assess psychosocial factors associated with medication non-adherence in solid organ transplant recipients: anxiety, depression, personality, posttraumatic stress disorder, and perceived social support using validated tools (Generalized Anxiety Disorder 7-item Scale, Patient Health Questionnaire—9, 10-item Personality Inventory, Primary Care PTSD Screen for DSM-5, and Multidimensional Scale of Perceived Social Support).
Results: Three of four vascularized composite allotransplantation recipients at our transplant hospital participated (75% response rate; Table 1). Screening revealed that no participants had posttraumatic stress disorder, and that all participants had high levels of social support. All participants demonstrated high levels of emotional stability and two demonstrated high levels of extraversion; however, agreeableness, conscientiousness and openness to new experiences were each demonstrated by only one participant. One participant demonstrated minor depression, and two participants demonstrated mild anxiety (Table 2).
Participant characteristics (n).
Education
High school or GED
1
Associate’s degree
1
Graduate degree
1
Income
US$20,000–39,000
1
>US$120,000
2
All or part of income from disability
2
Marital status
Single
1
Married
1
Divorced
1
Prevalence of depression, anxiety, and personality traits among VCA recipients.
Depression
N
No symptoms
1
Minimal symptoms
1
Minor depression/major depression, mild
1
Major depression, moderately severe
0
Major depression, severe
0
Anxiety
N
No symptoms
1
Mild anxiety
2
Moderate anxiety
Severe anxiety
Personality traits
High levels (N)
Low levels (N)
Emotional stability
3
0
Extraversion
2
1
Agreeableness
1
1
Conscientiousness
1
0
Openness to experiences
1
0
Conclusion: In this study, vascularized composite allotransplantation recipients appeared to have sufficient social support, which has previously been associated with better medication adherence in solid organ transplant recipients. However, vascularized composite allotransplantation recipients may be affected by other psychosocial factors such as depression and anxiety, which have been associated with worse medication adherence in prior studies of solid organ transplant recipients.
Lymphangiogenesis and immune regulation in vascularized composite allograft containing donor lymph nodes
Radu Olariu1, Mai Abd El Hafez2, Catherine Tsai2, Ioana Lese1, Mihai Adrian Constantinescu1, Robert Rieben2, Esther Vögelin2 and Adriano Taddeo1
1Inselspital, University Hospital, University of Bern, Bern, Switzerland
2University of Bern, Bern, Switzerland
Background: Mounting evidences suggest that the lymphatic system plays an active role in modulating inflammation, pathogenesis of autoimmune disease and organ immune-rejection process. Importantly, lymphatic vessels and stromal cells residing in the lymph nodes may promote peripheral tissue tolerance by induction of tissue specific Treg and promotion of immunoregulatory mechanisms. However, little is known about the process of lymphatic reconstitution and how this process influences graft rejection in vascularized composite allotransplantation. We hypothesize that the transfer of donor lymph nodes within a vascularized composite allotransplantation graft may be used to influence rejection promoting graft survival and immune regulation.
Methods: A total of 16 Brown Norway and Lewis rat hind-limb transplantations were performed; 8 received grafts with popliteal and inguinal lymph nodes (DLN+) and 8 received grafts depleted of all lymph nodes (DLN−). Lymphangiogenesis was assessed by daily lymphography. Rejection was graded macroscopically and blood, lymph node, skin, spleen, thymus, and bone marrow were collected at endpoint to assess donor/recipient lymphocyte composition.
Results: Graft rejection started significantly later in rats receiving hind-limb allografts containing donor lymph nodes (DLN+) as compared to allografts depleted of all donor lymph nodes (DLN−) (median: 5 and 4 days after transplantation, respectively, p = 0.03). Lymphangiogenesis occurred earlier in the DLN+ group compared to the DLN− group (mean: 3.5 and 5 days, respectively). Moreover, we observed a significant increase in circulating donor cells in the DLN+ group, specifically regulatory T cells, granulocytes, and monocytes (p = 0.02, p = 0.03, p = 0.04).
Conclusion: Vascularized composite allograft containing donor lymph nodes showed faster lymphangiogenesis, delayed graft rejection, and increased number of circulating donor regulatory T cells, granulocyte, and monocyte. These results underline the potential of specifically targeting the lymph node component of a vascularized composite allotransplantation to influence graft rejection.
Ethics on facial allotransplantation: a systematic review
Xiangxia Liu1,2, Sarah Langsdon2, Wesley Holloway2, Shuqia Xu1, Yangbin Xu1, Qing Tang1, Sai Ramakrishna Velamuri2 and William Hickerson2
1Sun Yat-sen University, Guangzhou, China
2The University of Tennessee Health Science Center, Memphis, TN, USA
Background: Currently, there are 40 cases of facial allotransplantation performed by 12 different groups in 8 countries. Although it has become a potential option to reconstruct and restore the function and appearance of severe facial disfigured individuals, the ethical concerns of facial allotransplantation remain unsolved. We conducted a systematic review to better understand the ethical concerns on facial allotransplantation and the change trends of the ethical debate over time.
Methods: A systematic review of four databases was performed to identify articles related to ethical concerns of facial allotransplantation by two independent reviewers. The inclusion criteria were articles on the topics of ethical concerns and facial allotransplantation with language written in English, French, and Chinese. The ethical concerns extracted from the included articles were sub-grouped into four principles of ethics: autonomy, beneficence, nonmaleficence, and justice. By comparing the number of publications in statistics way, we presented the main topics on ethical concerns and the changing trends in ethical themes in facial allotransplantation.
Results: There were 857 articles identified initially. After 264 duplicated articles were excluded, 593 articles were included for abstract review, and 131 articles were included in final data analysis. The publication year was from 2002 to 2018. The most addressed topic was Nonmaleficence (95 of 131, 72.5%), followed by beneficence (82 of 131, 62.6%), autonomy (73 of 131, 55.7%), and justice (60 of 133, 45.1%). The ethic debate was more focused on principle topics and recipient initially, then slowly shifted to some practical topics such as risk–benefit evaluation, informed consent and donor related.
Conclusion: More and more articles support facial allotransplantation as a feasible procedure to reconstruct and restore the function and appearance of severe facial disfigured individuals. The requirement of lifelong immunosuppression therapy centers in most of the ethical debates. With more and more favorable long-term follow-up results, the ethical concerns have shifted to a more practical debate focusing on risk versus benefit evaluation and informed consent. Donor-related ethics have become an important topic in facial allotransplantation.
Can we predict adherence in face transplantation recipients? The Brigham and Women’s Hospital experience
Sotirios Tasigiorgos, Miguel I Dorante, Elaine Devine, Kevin McComiskey, Marie-Christine Nizzi, Zoe Fullerton, Branislav Kollar, Elif Koçak, Jan Sokol, David Molway, Bohdan Pomahac
Brigham and Women’s Hospital, Boston, MA, USA
Background: Non-adherence to medical management in face transplantation is of paramount importance due to the catastrophic consequences. To date, a single reported case of facial allograft loss has been attributed to non-adherence. This study is the first attempt to evaluate adherence in face transplantation recipients by assessing pre-transplantation risk factors that could predict non-adherence after the operation.
Methods: Two independent researchers collected clinical data relevant to pre-transplant risk factors that could predict adherence after face transplantation and markers of non-adherence post-transplant. We investigated social history, education, employment, financial and mental health status, and substance abuse as possible predictors of non-adherence. Communication with care team, appointment attendance, follow-up, and medication-taking were used as markers for non-adherence. These were identified from relevant literature on solid organ transplantation and our social work psychosocial assessment used before transplantation. Respective lists were created. A transplant nurse and a clinical social worker evaluated patients using the aforementioned lists by scoring each factor and marker based on clinical encounters. Overall scores from the lists were correlated for each patient.
Results: Our patient cohort includes four full-face and two partial-face allografts. Five patients were predicted to show adherence after surgery when they were assessed for pre-transplant predictors. However, only two of these five ultimately demonstrated adherence to post-transplant management, with one patient displaying a mix of adherent and non-adherent behaviors. Non-adherence in laboratory monitoring, medical therapies, and follow-up appointments resulted in complications and management difficulties such as over- and under-immunosuppression, acute kidney injury, and acute rejection.
Conclusion: No correlation was found between pre-transplant risk-factors and post-transplant instances of non-adherence. Results from our center showed great variability between patients. A longer follow-up, prioritizing a multidisciplinary approach including research and medical personnel in the management of face transplantation, is needed to ensure adherence. Prediction of adherence presents a myriad of complex issues which are difficult to resolve. Hopefully, with ongoing research, we will be able to better identify not only the tools needed to predict the risk of post-transplant non-adherence but also strategies to help patients minimize it, ensuring optimal post-operative care.
A call to accountability: reporting outcomes in vascularized composite allotransplantation
James Lloyd Bene1, Nicholas L Robbins2, Vijay S Gorantla3, Warren C Breidenbach2 and Bruce Kaplan4
1Duquesne University, Pittsburgh, PA, USA
2RESTOR™ Program, 59th Medical Wing, JBSA Lackland AFB, San Antonio, TX
3Wake Forest Institute for Regenerative Medicine, Winston-Salem, NC, USA
4Baylor Scott & White Health, Dallas, TX, USA
Background: Because nearly all the vascularized composite allotransplantations performed in the United States have been proposed and carried out as research, the ethical duty to report outcomes of research pertains. This ethical duty is noted in international statements, such as the World Health Organization’s Statement on Public Disclosure of Clinical Trial Results and the Singapore Statement on Research Integrity. The WHO Statement affirms the Helsinki Declaration, which states (1) “Researchers have a duty to make publicly available the results of their research” and (2) “Negative and inconclusive as well as positive results must be … made publicly available.” The WHO Statement further insists that “There is an ethical imperative to report the results of … unreported trials conducted in the past.” The Singapore Statement similarly calls for data sharing: “Researchers should share data and findings openly and promptly.” In 2014, the OPTN (Organ Procurement and Transplant Network) VCA Committee proposed data collection and submission requirements which took effect in September of 2015. While this appears to fulfill the ethical mandate to report outcomes, the OPTN proposal did not require data submission for vascularized composite allotransplantations performed prior to September 2015.
Methods: A review the international statements will demonstrate that there is ethical justification for the standards they propose. Their standards will be contrasted with the position taken by UNOS regarding vascularized composite allotransplantation and the actual publication and/or reporting which has taken place.
Results: The analysis reveals that the UNOS rule falls far short of the ethical standard set forth in the WHO Statement on Public Disclosure of Clinical Trial Results and the Singapore Statement on Research Integrity. Furthermore, it is clear that very few have elected to submit data on vascularized composite allotransplantations performed prior to September 2015.
Conclusions: With regard to data collection and reporting, WHO and UNOS have conflicting ethical standards. UNOS should align itself with international ethical standards by requiring all US vascularized composite allotransplantation teams to submit their outcome data between 1999 and September 2015, and to continue to report on the conditions of patients and grafts as these evolve.
Orthodontics and dental care in a face transplant recipient
Thomas J Salinas, Hatem Amer, Samir Mardini and John E Volz
Mayo Clinic, Rochester, MN, USA
Background: There is no information regarding the safety of orthodontic procedures in face transplant recipients.
Methods: A 31-year-old male received a face transplant that included the nose and all the maxilla and the mandible. As such, all the dentition and supporting tissues were donor derived. At the time of donation, significant dental caries and periodontal disease were noted as well as malalignment of the teeth. At the time of transplant, tooth extraction was considered, to avoid the risk of infection and possible abscess formation, but not performed. The transplant proceeded with T-cell depletion (antithymocyte globulin), and maintained with tacrolimus, mycophenolate mofetil, and prednisone. As with preventive measures for elective dento-alveolar surgery, routine antimicrobials were administered peri- and post-transplant. Strict oral hygiene was maintained with oral care performed by nursing staff and then the patient when able. Dental treatment began with a diagnostic phase that revealed dental caries, tooth malalignment, and significant periodontal inflammation. The periodontal disease was addressed by removal of calculus that was supra and subgingival. Caries were removed in all teeth followed by conservative restorations (fillings). Despite the immunosuppression, the periodontal healing response was favorable leading to a preferred environment to correct the teeth malalignment. To avoid risk of oral mucosal ulceration seen with conventional braces, a series of 31 Invisalign trays was created. There was concern as to whether this would work in a patient on immunosuppression as braces move the teeth by creating inflammation around the tooth roots. The possibility exists that orthodontics could cause the teeth to become excessively loose, exfoliate, and possibly trigger a rejection.
Results: 24 months after the transplant, the patient is currently on tray 31/31. Alignment has progressed as expected. After initiation of therapy there was one episode of rejection at 22-month post-transplant that appears to be triggered by sentinel flap trauma and not related to the orthodontic or periodontics procedure.
Conclusion: This case shows that braces and conventional periodontal therapy can be used for realignment of allograft dentition in the setting of standard triple immunosuppressive therapy. Assessment of safety and generalizability will require the study of more cases.
Trauma-induced discordant rejection of the sentinel flap of a face transplant recipient
Megha Tollefson, Hatem Amer, Rokea El-Azhary, Lynn D Cornell, Lawrence Gibson, Samir Mardini and Julia Lehman
Mayo Clinic, Rochester, MN, USA
Background: A 31-year-old-male patient received a face transplant consisting of all structures below the orbits. He had no prior donor-specific antibodies and was induced with antithymocyte globulin, and maintained on tacrolimus, mycophenolate mofetil, and prednisone. A posterior tibial flap was inset in the left inguinal area to allow for frequent surveillance biopsies.
Methods: One episode of rejection detected clinically at 8 weeks post-transplant. This manifested by a fixed erythema of the face that was accompanied by a punctate diffuse rash of the sentinel flap. Biopsies at that time showed a Banff composite tissue allotransplantation grade-2 rejection of the face and grade 1 of the sentinel flap. A short course of bolus steroids resulted in clinical recovery and follow up biopsies documented resolution of inflammation in both the sentinel flap and face graft. Surveillance biopsies 1-year post transplant remained quiescent.
Result: At 22 months post-transplant, he noted a new onset purpuric eruption in the middle of the sentinel flap. There were no other associated symptoms and the face remained clear. Earlier in the day he had worn a five-point harness for the first time and was suspended from it for approximately 2 h. One of the straps crossed the sentinel flap. Over the following days, the purpuric rash decreased but then a diffuse punctate rash developed over the sentinel flap. The face (donor skin) and neck (native skin) showed mild erythema consistent with sun exposure but no rash. Biopsies from the sentinel flap showed findings consistent with a Banff composite tissue allotransplantation grade-2 rejection, were negative for perivascular C4d by immune histochemistry, but were positive by immunofluorescence. Biopsies from the face graft and native skin from the neck did not show rejection. Following a course of corticosteroids, the rash resolved and follow-up biopsies showed normal skin. No anti-human leukocyte antigen donor-specific antibodies were detected during this event.
Conclusion: Trauma may have initiated a rejection episode. Prompt therapy may have abated the activation of the immune system prior to the development of rejection of the face. The value of C4d staining by immunofluorescence versus immunohistochemical remains in need of study in face transplantation.