
Abstract
Objectives:
Acute muscle injury and potentially fatal rhabdomyolysis may occur with the use of statins and certain enzyme inhibitors, but data on this topic from China are quite limited. This study aimed to measure the concomitant exposure of patients to different statins and their enzyme inhibitors or interacting medications in 76 hospitals in six Chinese cities.
Methods:
Prescription database was retrieved from Hospital Prescription Analysis Cooperation Project from January 2015 to December 2015, covering 76 tertiary facilities in six cities in China. Every evidence-based enzyme inhibitor was included, and labeled enzyme inhibitors and other relevant information were identified and obtained using the Drug Safety Update from the UK Medicines and Healthcare Products Regulatory Agency. The proportions of different statin types among all patients and those co-medicated with their inhibitors were examined.
Results:
A total of 296,765 patients exposed to statins were included in this study. 80% of patients (n = 144,863, 80.5%) were concomitantly prescribed a CYP3A4-metabolized statin with an interacting drug during the study period. Among those prescribed a non-CYP3A4-metabolized statin, 40.0% of patients were concomitantly given an interacting drug, and approximately 20% of patients were concomitantly given a labeled inhibitor, predominantly calcium channel blockers, other statins, and fibrates. Rates of co-prescription were higher in patients aged over 65 years and in patients taking high-dose statins.
Conclusion:
Statins were frequently co-prescribed with metabolic inhibitors in China, where drug safety strategy on highlighting warnings and contraindications of statins are still lacking. For high-dose statins patients who are over 65 years and co-administered with any metabolic inhibitors, prescribers and pharmacists should be more concerned in order to prevent adverse drug reactions.
Introduction
Cardiovascular disease (CVD) is the most common disease in China, according to the Report on Cardiovascular Diseases in China (2015). 1 Reducing blood lipids has, therefore, become a major therapeutic strategy to prevent or control the progression in patients with or more susceptible to CVDs. 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) inhibitors, which are more widely known as statins, comprise lipid-lowering agents that revolutionized the pharmacotherapeutics of CVDs. 2 The benefits of statins in decreasing cardiovascular morbidity and mortality have also been demonstrated in several studies.3–5 Since the launch of lovastatin in 1987, a number of different statins have been developed successively. Frequently used statins include atorvastatin, rosuvastatin, pravastatin, simvastatin, pitavastatin, and lovastatin.
However, safety problems concerning statin therapy drew great attention after the withdrawal of cerivastatin from the world market in 2001. The reason behind this callback was a much higher rate of fatal rhabdomyolysis for cerivastatin, according to the US Food and Drug Administration (FDA).6,7 The adverse effects could also be possibly severe and more prevalent in real situations, since patients cannot be monitored as closely as in clinical trials. 8 A study on statin-associated side effects indicated that statins should be administered carefully due to the risk of side effects, including myalgia, liver injury, and kidney injury, as well as myopathy and rhabdomyolysis as documented side effects of statins. 9
Patients at high risk or with more comorbidities usually have to take a number of different types of medications at the same time. Drug–drug interaction (DDI) is one of the most important components in comprising the safety profile of almost every medication, including statins inevitably. 10 Thompson et al. 11 performed an extensive FDA search on statin-associated rhabdomyolysis over a 12-year period. They revealed that among 3339 reports of rhabdomyolysis, 58% were associated with concomitant medications which affect the normal metabolism of statins in human body. These medications included fibrates, cyclosporine, digoxin, warfarin, macrolides, and azole antifungals. Besides DDIs, drug–disease interactions also play an important role in determining drug safety profile.
Siriangkhawut et al. 12 found a prevalence of 9.1% patients in a Thailand that had potential simvastatin-drug interactions, in which gemfibrozil, colchicines, and amlodipine were the three most common concomitant drugs. Ming et al. 13 showed that, in US administrative claims data and electronic medical records, 25%–30% of patients given a CYP3A4-metabolized statin were concomitantly exposed to a CYP3A4 inhibitor, and the largest proportion of concomitant prescribing with a statin was observed with the labeled inhibitors such as calcium channel blockers. Bakhai et al. 14 found that approximately one-third (30%) of patients prescribed a CYP3A4-metabolized statin had also been prescribed a concomitant CYP3A4 inhibitor, predominantly involving macrolide antibiotics and calcium channel blockers co-prescriptions. These inconsistent results could be due to differences in research settings, criteria for selecting potential statin-drug interactions, availability of medication in hospital formularies, the reimbursement policy and clinical practice guidelines during the study period.
The proportion of patients who may potentially suffer from the side effects of statin-related co-prescriptions is still unknown in China. This study aimed to measure the concomitant exposure of patients to statins and their inhibitors/interacting drugs in Chinese population. We reviewed all cases from our target hospitals of concurrent use of atorvastatin, simvastatin, rosuvastatin, pravastatin, fluvastatin, or pitavastatin over a 1-year period.
Methods
Data source and sample selection
This was a retrospective study focusing on patients receiving statin treatment concurrently with their enzyme inhibitors or certain interacting drugs from January 2015 to December 2015. Different types of statins including atorvastatin, simvastatin, rosuvastatin, pravastatin, fluvastatin, and pitavastatin prescription were analyzed. The information-traced period for each statin-treated patient started from his or her first exposure to a statin until another type of statin was used or the study period reached December 2015.
Data were retrieved from Hospital Prescription Analysis Cooperation Project, which was initiated by Dr Dakui Li from Peking Union Medical College Hospital in 1997 and technical supported by Beijing Prescription Consulting Ltd. The project contains anonymized patient medical records covering 76 third-tier hospitals in six cities in China: Beijing, Chengdu, Guangzhou, Hangzhou, Shanghai, and Tianjin. Local pharmaceutical societies in various areas are responsible for organizing and expanding local work of data collection. The hospitals agree to adhere to “recording guidelines” that are subject to detailed quality control checks of data at both practice and individual patient level. These 76 hospitals can share data free of charge. After all these years, a large amount of important historical data were gathered and reserved, which enable us to observe inappropriate drug treatments in a macroscopic view. Details of the three-tiered health system in China are provided in Appendix 1.
The study was implemented in line with Declaration of Helsinki and its amendments. Ethics Committee of Huashan Hospital (No. KY 2015-324) approved the research plan and granted written informed consents from all 76 hospitals. Patient informed consent was bypassed for this is just an observational study without interventions or disruptions to patients’ lives.
Inclusion/exclusion criteria
Only individuals defined as statin exposure patients were included in the analyses. A statin exposure patient was defined as an individual who received one or more prescriptions of the same statin type during 2015.
Concomitant exposure
The exposure of statin-treated patients to mediations with potential DDIs was examined. DDIs were identified using Micromedex-DrugReax and Drug-interactions checker tool available on www.drugs.com.15,16 Drug interactions with statins can be divided into three components: (1) “major” interactions stands for drugs which should be predominantly avoided due to its significant risk of clinical adverse events, (2) “moderate” interactions represent the possibility of co-administration exists only under some special circumstances, and (3) “minor” interactions indicate a relatively low risk of interactions but consideration of an alternative drug is still needed.
The exposure of patients prescribed with a CYP3A4-metabolized statin and a CYP3A4 inhibitor or with a CYP2C9-metabolized statin and a CYP2C9 inhibitor was also examined. All CYP3A4 and CYP2C9 inhibitors, including those listed in the precautions sections, and potential CYP3A4 and CYP2C9 inhibitors are presented in Table 1. 17 Protease inhibitors are not listed and examined because these medications are prescribed only by the Centers for Disease Control (CDC) in China, although they are strong CYP3A4 inhibitors.
All statins and their inhibitors included in analysis.
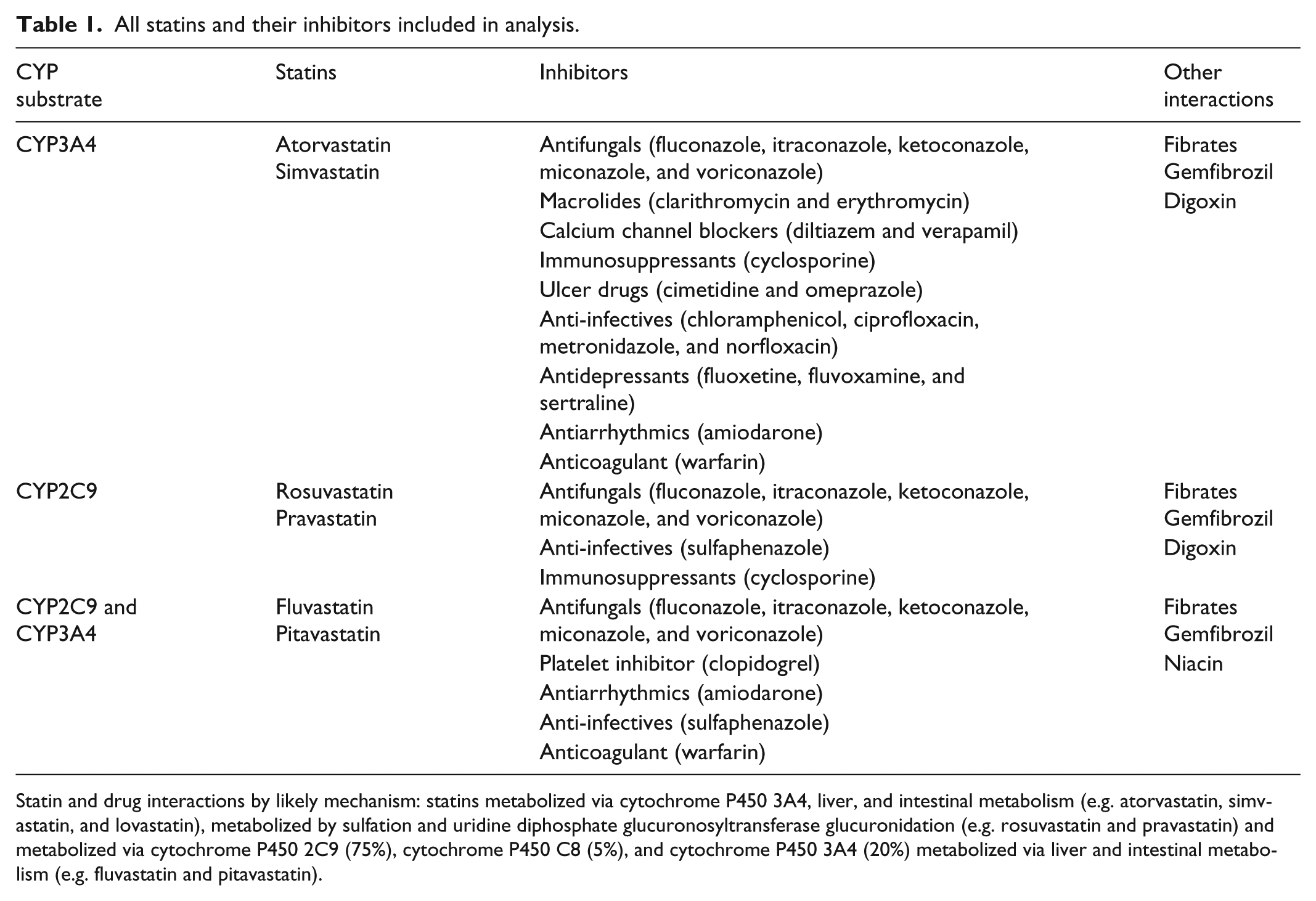
Statin and drug interactions by likely mechanism: statins metabolized via cytochrome P450 3A4, liver, and intestinal metabolism (e.g. atorvastatin, simvastatin, and lovastatin), metabolized by sulfation and uridine diphosphate glucuronosyltransferase glucuronidation (e.g. rosuvastatin and pravastatin) and metabolized via cytochrome P450 2C9 (75%), cytochrome P450 C8 (5%), and cytochrome P450 3A4 (20%) metabolized via liver and intestinal metabolism (e.g. fluvastatin and pitavastatin).
Concomitant exposure was defined as a patient taking any of the following three combinations of drugs on the same day: a statin with an interacting drug, a CYP3A4-metabolized statin with a CYP3A4 inhibitor, and a CYP2C9-metabolized statin with a CYP2C9 inhibitor. Rosuvastatin, pravastatin, fluvastatin, and pitavastatin were classified as CYP2C9-metabolized statins to distinguish them from statins more extensively metabolized through the CYP3A4 pathway.
Statistical analysis
Patient demographics contained a patient’s age, gender, types of visited department, diseases or conditions, and so on. Information regarding the drug usage pattern included the type and duration of statin use, its enzyme inhibitor/interacting drug use, and the duration of combined use. This information was withdrawn from patients receiving their first statin therapy during the study period.
Statin exposure was examined in the calculation of percentage for three subgroups, respectively, in all patients, patients over 65 years, and those prescribed higher doses of statins. High statin doses were defined as 40 mg or greater for atorvastatin, fluvastatin, pravastatin, simvastatin, and pitavastatin and 20 mg or greater for rosuvastatin.14,18 Statistical analysis was performed by the application of SPSS (Statistical Product and Service Solutions) Version 19.0 for Windows.
Results
Patient demographics and statin prescription
The number of total sampled patients exposing to statin was 296,765 with an average age of 63.9 years. The proportion of patients older than 65 years reached 46.8% of the overall population. Patient demographics and patients at increased cardiovascular risk who received statin therapies are described in Table 2. Cardiopulmonary disorder (n = 111,286, 37.5%), neurology disorder (n = 50,450, 17.0%), kidney disorder (n = 38,876, 13.1%), and endocrine disorder (n = 37,985, 12.8%) were the four highest-ranked major diagnoses in our investigated patients.
Patient demographics and clinical characteristics.

59% (n = 179,955, 59.0%) of all patients were exposed to a CYP3A4-metabolized statin during the study period, with the majority receiving treatment of atorvastatin (n = 141,580, 52.5%), followed by simvastatin (n = 38,375, 6.5%). 41% (n = 116,810, 41.0%) of all patients had been exposed to any type of non-CYP3A4-metabolized statins, in which rosuvastatin accounting for 28.3% (n = 76,669), pravastatin for 6.6% (n = 18,166), fluvastatin for 3.1% (n = 12,276), and pitavastatin for 3.0% (n = 7291). The proportion of each statin in each hospital department of the 76 hospitals is presented in Table 3.
Patient demographics of statin prescribing during the study period.

ATV: atorvastatin; SMV: simvastatin; RSV: rosuvastatin; PRV: pravastatin; FLV: fluvastatin; PIT: pitavastatin.
Patients exposed to atorvastatin and simvastatin were generally older; one in every two (n = 69,091, 48.8% and n = 19,532, 50.9%, respectively) of the patients was more than 65 years old. 27.3% (n = 38,646) of patients exposed to atorvastatin received higher doses, while 28.9% (n = 11,110) of patients were exposed to higher doses of simvastatin. All statin patient groups consisted of higher proportions of elderly patients (i.e. 65 years or older), except those prescribed pitavastatin. 59.6% (n = 4374) of pitavastatin patients were younger than 65 years old, but they comprised only 3% of the overall population. Besides, higher doses of pravastatin (n = 9357, 51.5%), fluvastatin (n = 6756, 55.0%), or pitavastatin (n = 3902, 53.5%) were prescribed to over half of the statin-treated patients.
Concomitant medication use
The percentage of patients co-prescribed CYP3A4-metabolized statins and inhibitors/interacting drugs is illustrated in Figure 1. 80% of patients (n = 144,863, 80.5%) were concomitantly prescribed a CYP3A4-metabolized statin with an interacting drug during the study period, including 89% of simvastatin-treated patients, and 71% of atorvastatin-treated patients. For patients taking simvastatin, 19% also received an interacting drug of major effects when used in combination with statins; the moderate and minor interactions was 67% and 2%, respectively. In terms of non-CYP3A4-metabolized statins, the proportion of concomitant prescriptions ranged from pravastatin in 18% patients to fluvastatin in 80% patients, with almost 40% related to co-prescription with an interacting drug. Drugs with moderate interactions with statins were prescribed for 67% of fluvastatin patients, which accounted for 83% of all fluvastatin-related interacting drugs (shown in Figure 2).

Concomitant exposure to CYP3A4-metabolized statins and drug–drug interactions.

Concomitant exposure to non-CYP3A4-metabolized statins and drug–drug interactions.
Type of inhibitors and percentage
For both CYP3A4-metabolized and non–CYP3A4-metabolized statins, the proportions of co-prescribing a statin and an inhibitor were similar, irrespective of whether the inhibitors were labeled or all identified potential inhibitors were assessed (Tables 4 and 5 show all classes of concomitantly prescribed labeled medications by the types of statin).
Exposure to labeled CYP3A4 inhibitors during the study period by CYP3A4-metabolized statins.

ATV: atorvastatin; SMV: simvastatin.
The calcium channel blocker mainly being used was amlodipine.
Exposure to labeled CYP2C9 and CYP3A4 inhibitors during the study period by non-CYP3A4-metabolized statins.

RSV: rosuvastatin; PRV: pravastatin; FLV: fluvastatin; PIT: pitavastatin.
The calcium channel blocker mainly being used was amlodipine.
The calcium channel blocker mainly being prescribed was amlodipine. Other statins and fibrates were prescribed at the highest frequency with both CYP3A4-metabolized and non-CYP3A4-metabolized statins. Patients who were concomitantly prescribed statins with fibrates and other statins accounted for 1.7%–4% of all prescriptions of statins and their inhibitors, with only 10 patients prescribed gemfibrozil and a statin concomitantly.
The antiplatelet medication, clopidogrel, was the second most frequently concomitant medication for non-CYP3A4 statins. Clopidogrel was concomitantly prescribed in 15.2% of pitavastatin patients and 10.3% of fluvastatin patients. Ulcer drugs, antidepressants, warfarin, and digoxin were less likely to be co-prescribed than statins and fibrates, but they still accounted for a high percentage of prescriptions in patients prescribed CYP3A4-metabolized statins. Similar proportions of prescriptions for warfarin and digoxin were also seen in non-CYP3A4-metabolized statins.
Higher dose statins with concomitant calcium channel blockers
As shown in Table 6, 7190 patients were concomitantly prescribed simvastatin and calcium channel blockers, including 474 patients prescribed higher doses of simvastatin (40 mg or more), and 278 patients are older than 65 years. The drug combinations included (1) simvastatin, amlodipine, and atorvastatin; (2) simvastatin, amlodipine, and amiodarone; (3) simvastatin, amlodipine, and diltiazem; (4) simvastatin, amlodipine, amiodarone, and diltiazem. Patients prescribed higher doses of pravastatin accounted for 39.8% (1212 patients) of patients concomitantly exposed to pravastatin and calcium channel blockers, in which 61.6% (747 patients) were more than 65 years old. Similar rates were also observed in fluvastatin patients.
Patients exposed to higher dose of statins concomitant calcium channel blockers.

ATV: atorvastatin; SMV: simvastatin; RSV: rosuvastatin; PRV: pravastatin; FLV: fluvastatin; PIT: pitavastatin.
Annualized median days of prescribing inhibitors
The duration of concomitant prescription was generally similar for both CYP3A4-metabolized and non-CYP3A4-metabolized statins, irrespective of age and dosage (Tables 4 and 5). The annualized median days of overlap with calcium channel blockers were approximately 340 days for CYP3A4-meta-bolized statins and 308 days for non-CYP3A4-metabolized statins. Such index with immunosuppressant cyclo-sporine ranged from 289 days for fluvastatin to 341 days for atorvastatin. Amiodarone was concomitantly prescribed in approximately 0.2% of both atorvastatin and simvastatin patients with annualized median overlaps of 221 and 236 days, respectively. It is also notable that macrolides had the shortest duration of concomitant medication use (10–18 days).
Discussion
Statins have strong selective inhibiting effect on HMG-CoA reductase. These medications normally show little affinity for other enzymes or receptors, which indicates that statins are much less likely to interact with other drugs in pharmacodynamic processes. However, statins share the common metabolic pathways with a number of drugs; therefore, potential DDIs for statins are quite significant. 2 CYP3A4 enzymes are responsible for the metabolism of atorvastatin, simvastatin, and lovastatin, which differ from fluvastatin and pitavastatin mainly metabolized by CYP2C9 (75%), CYP2C8 (5%), and CYP3A4 (20%) via liver and intestinal metabolism. The metabolism of pravastatin and rosuvastatin are shown to be related to sulfation and uridine diphosphate glucuronosyltransferase glucuronidation, respectively.2,19 Concomitant use of a statin and a related medication can possibly alter the concentration levels of the statin in the plasma, causing a higher risk of side effects, such as myopathy or rhabdomyolysis.
Cardiovascular drugs with inhibitory activity toward CYP3A4 enzymes, such as verapamil, diltiazem, amlodipine, ranolazine, and amiodarone, can increase the plasma concentrations of simvastatin and lovastatin by up to fourfold. It has already been reported that severe rhabdomyolysis attributes to a major interaction between amiodarone and simvastatin. 20 Therefore, the FDA recommends a maximum dose of simvastatin of 10 mg/day when used in combination with cardiovascular drugs. Particularly, if the patient is taking amiodarone, amlodipine, or ranolazine, the doses for simvastatin should not exceed 20 mg/day, considering the outcome of dramatic elevation in plasma levels.19,21 The statin-induced myopathy case reported as adverse drug reaction (ADR) to the Beijing Center for ADR Monitoring has already been summarized, 18 it showed severe statin-induced myopathy, like rhabdomyolysis, is more likely to occur in old patients, in patients taking high-dose statin. 18 While in this study, 7190 patients were taking amlodipine, amiodarone combined with simvastatin, including 6.6% of patients (474 patients) prescribed simvastatin 40 mg/day, and 58.6% of these patients were 65 years or older (Table 6).
The hepatic function damage induced by the concomitant use of statins and fibrates is likely to increase plasma levels of statins, or even worse, myopathy. Approximately 0.12% of the prevalence of creatine kinase-related myopathy has been attributed to a combination of statins and fibrates. 22 In patients with mixed hyperlipidemia, the prescribers should know that gemfibrozil, rather than fenofibrate, interferes with the process of statin glucuronidation, which might lead to an elevated statin level and possibly myopathy. The combination of gemfibrozil and statins should, therefore, be avoided.
Patients with chronic kidney diseases or kidney transplant history are more vulnerable to suffering from adverse events of myalgia, myopathy, and rhabdomyolysis, even though they rarely happen. 23 Notably, such effect is associated with dosage and can be hastened by drugs inhibiting CYP3A4 enzymes. Survivors of organ transplantation may develop hyperlipidemia, which is driven not only by post-operative weight gain but also by the use of prednisone and cyclosporine. 24 Cyclosporine has documented interactions with statins for substrate competition, and a reduced dose is invariably required (10 mg/day for simvastatin and atorvastatin and 20 mg/day for lovastatin). Hence, cautions should be taken when co-prescribing any CYP3A4-metabolized statin with other drugs, particularly fibrates, cyclosporine, and azole antifungals.
Some studies have found out that the anticoagulant effects of warfarin can be enhanced by some statins (e.g. simvastatin, fluvastatin, and rosuvastatin). 25 In this study, the prevalence of statin–warfarin combination ranged from 0.2% to 0.4% with rosuvastatin, fluvastatin, and pravastatin, although the total number of patients was not large. Anticoagulation function should be assessed and monitored in patients requiring warfarin before the initiation, withdrawal, or modification of any statin therapy, while adjustments might be needed upon the dose of warfarin accordingly. Normally, such an adjustment is small but clinically relevant changes in patients’ anticoagulant function could still happen. Restraint is warranted in co-prescribing warfarin with statins since fluvastatin and, to a lesser extent, rosuvastatin are substrates for CYP2C9 enzymes, which are also responsible for metabolizing warfarin. 21 Consistent evaluation of the international normalized ratio during warfarin therapy is recommended for patients who need to simultaneously take simvastatin, fluvastatin, or rosuvastatin.
The majority of Chinese patients have LDL–C baseline levels much lower than that of Caucasians, that most Chinese patients could achieve the target level with medium- or low-dose statins. Chinese patients experience a 10-fold ADR rate and more severe ADR than Caucasians when taking medium-dose simvastatin. 18 Considering the potential risk of side effects, education on how these inhibitors have a major impact on the metabolism of statins, or to a larger extent, how drugs interact with each other in many other ways is essential for Chinese prescribers and pharmacists to prevent related adverse events in patients.
Besides, several different strategies could be implemented to reduce the risk of potential drug interactions in clinical settings. 26 First, pharmacists need to get involved in the process of tailoring therapeutic treatments and actively alert potential problems to physicians, especially emphasizing the importance of considering the potency of the inhibitor, the age, and the organ function of the patient. Second, pharmacists should try to provide possible alternatives from their professional point of view, which may reduce or even avoid drug interactions. Atorvastatin is less sensitive than simvastatin to CYP3A4 inhibition. 14 Switching to a statin without strong cytochrome P450 interactions (pravastatin seems to have the lowest interaction potential with CYP3A4 inhibitors27,28) may be more clinically appropriate when concomitant medications with similar enzymatic metabolism is present. Third, patients’ conditions should be monitored more closely if the doses of the interacting statin need to be 40 mg or higher. More specifically, if the use of an inhibitor with short half-life period or short therapeutic duration such as macrolides and ketolides is needed, suspending the statin prescription until the inhibitor prescription is complete may be required. 14 At a minimum, a critical appraisal of both pharmacokinetics and DDIs should lead to safer statin use in the hospital, improve the compliance of patients, and consequently improve primary and secondary cardiovascular prevention outcomes.
As with similar observational studies, our investigation has some major limitations. First, patients that were included in our study were all receiving treatment from three-tiered hospitals; therefore, our results could only represent the general prescription manner of three-tiered hospitals in China, rather than the whole country. Second, it was performed with a retrospective, uncontrolled design. Many other variables outside our consideration may still exist and distort our results. Third, we did not examine whether the co-prescription manner of statins and its inhibitors would actually lead to clinically significant adverse events. In addition, we did not use medical records to identify signs and symptoms of muscle toxicity to further confirm the potential side effects. However, such uncertainty can be eliminated by other studies which complementarily investigated the real rates of adverse events in clinical establishments.29,30 Another limitation of this study exists in the insufficient data regarding Chinese herbs, since many patients would concomitantly and ignorantly take Chinese herbal medicines with statins.
Conclusion
At the 76 hospitals in China, statins were frequently prescribed with their metabolized inhibitors, increasing the risk of potential drug interactions. For high-dose statins patients who are over 65 years and co-administered with any metabolic inhibitors, prescribers and pharmacists should be more cautious of using interacting drugs. Education on how these inhibitors have a major impact on the metabolism of lovastatin, simvastatin, and atorvastatin is essential for prescribers and pharmacists to prevent statin-related adverse events in patients.
Footnotes
Appendix 1
The three-tiered healthcare system of hospitals in China.
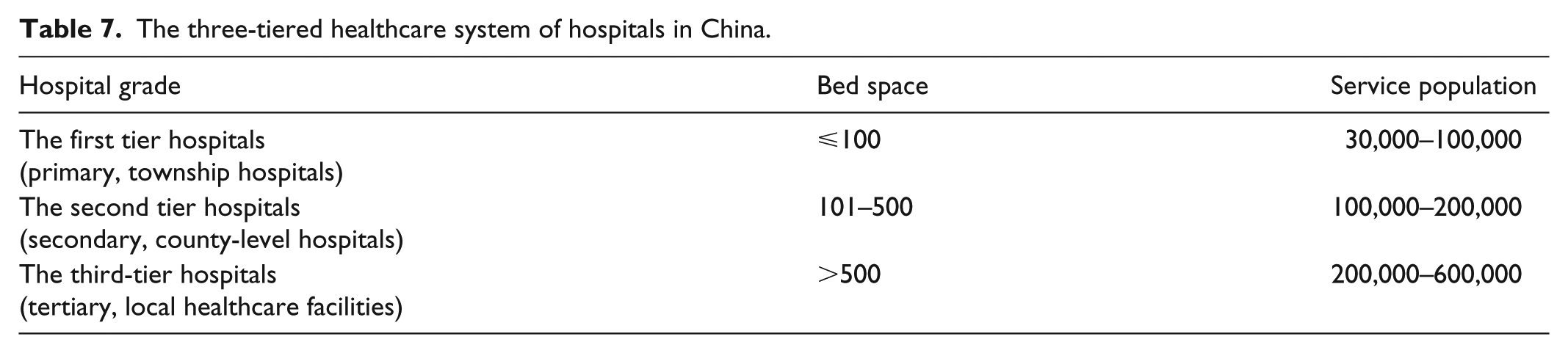
| Hospital grade | Bed space | Service population |
|---|---|---|
| The first tier hospitals (primary, township hospitals) | ⩽100 | 30,000–100,000 |
| The second tier hospitals (secondary, county-level hospitals) | 101–500 | 100,000–200,000 |
| The third-tier hospitals (tertiary, local healthcare facilities) | >500 | 200,000–600,000 |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of Huashan Hospital, Fudan University (No. KY 2015-324).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was sponsored by Shanghai Scientific Research Fund of Hospital Pharmacy (No. 2012-YY-01-08), 2016 Key Clinical Program of Clinical Pharmacy, and Weak Discipline Construction Project of Shanghai Municipal Commission of Health and Family Planning (No. 2016ZB0301-01).
Informed consent
The prescription analysis project contains only anonymized patient medical records, so patient informed consent was omitted.
Trial registration
This randomized clinical trial was not registered because this was a retrospective study focusing on patients’ prescription information only.