
Abstract
This study applying the health services utilization model examined the importance of predisposing, enabling, and need variables to the social mechanisms explaining lifetime HIV testing across racial/ethnic groups. Data for the study were derived from the National Health Interview Survey (collected 2013–2014), our final sample numbering 18,574 adults. Four subsamples reflected race/ethnicity: 13,347 Whites, 2267 Blacks, 2074 Hispanics, and 886 Asians. Logistic regression established respondent odds of ever having received HIV testing. Further statistical testing evaluated race/ethnicity’s potential moderating role in HIV testing. The findings generally support a role for Aday’s predisposing, enabling, and need factors in explaining HIV testing. Across the four subsamples, female gender, older age, and sexual minority status consistently increased lifetime HIV testing. However, we found racial/ethnic differences in HIV testing’s associations with these factors and others. Our study made a beginning in the effort to specify mechanisms leading to HIV testing—and reliable diagnosis—among four racial/ethnic groups. Understanding these mechanisms might multiply opportunities to raise testing rates for all, in turn reducing racial/ethnic disparities in HIV treatment.
Introduction
As medical knowledge and technological knowledge advance, so do the screening and testing available to properly diagnose illness in time to treat it and sustain life. Consider the human immunodeficiency virus (HIV). Initially considered to mean death for those infected, HIV and the syndrome it causes, AIDS (acquired immune deficiency syndrome), today are approached instead as chronic conditions requiring ongoing treatment; this is thanks to the development of antiretroviral therapy.1,2 Progress of this kind has also made HIV diagnostic testing significant in prevention efforts. 3 Access to HIV testing has been made ever easier for people, at medical clinics, substance abuse treatment centers, community health centers, and other sites, not to mention van-based mobile testing.
Even with improved access, it is estimated that in 2015, 14.5% of HIV-infected Americans aged 13 or older lacked diagnosis, the undiagnosed including disproportionate numbers of minority Americans and men who have sex with men. 3 Disproportionate numbers of Asian Americans, too, do not know their HIV status; in 2014, an estimated 19.6% of Asian Americans living with HIV had undiagnosed HIV. 4 A 2016 report noted racial/ethnic disparities characterizing HIV infection, stating that for each 100,000 population, 5.2 Whites had been diagnosed with HIV, as had 43.6 Blacks, 17 Hispanics, and 5.5 Asian Americans. 2 Hispanics’ overall prevalence rate was three times Whites’, while Blacks’ rate was eight times Whites’. 3 According to one 2016 report concerning Americans, 41% of Whites, 46% of Hispanics, and 65% of Blacks had received HIV testing while 42% of those of other ethnicity (including Asian Americans) had undergone HIV testing. 5 In a 2004–2006 study of Washington, D.C., residents of Southeast Asian ethnicity stated that 31% had received HIV testing. 6 Today, new HIV infections continue to emerge, with new diagnoses made disproportionately in minority Americans, especially minority women and minority gay men, lesbians, and bisexuals.2,3,7
The literature shows that the likelihood of HIV testing is higher among females, those never married, minority Americans including Blacks and Hispanics (vs Whites), and younger adults.5,8–11 Among Americans of Southeast Asian ethnicity, knowing HIV facts has been found to increase HIV testing. 6 In addition, while the literature indicates Blacks and Hispanics know less about HIV than Whites do, minority groups show greater likelihood of having received HIV testing than Whites. 10 Immigration status, too, is a relevant factor in behavior related to HIV testing. Prior to 2010, immigrants were often required to receive HIV testing before entering the United States, since HIV was deemed a communicable disease significant to public health.8,12 For such immigrants, HIV testing did not constitute voluntary behavior. Finally, obtaining education about HIV creates awareness of the importance of early diagnosis—that is, of testing and treatment.8,11
Individuals who are relatively well off, financially, and/or have health insurance are observed to use healthcare relatively often. 13 Despite this, the literature offers no consistent pattern linking income to HIV testing where young adults, mentally ill adults, and male adults who have sex with other men have been included in the research.11,14,15 At least one study of Americans of Southeast Asian ethnicity showed no link between having health insurance and receiving HIV testing at any point in life. 6
Often, HIV is transmitted via unprotected sex with someone infected with the virus; often, it spreads during drug use, as someone infected shares a syringe, and virus, with another user. 16 These facts have been well publicized, meaning HIV testing rates indicate not just willing participation (and, for some immigrants, involuntary participation) in diagnostic screening, they also indicate awareness of potential exposure to the virus and resulting concern for health.8,17 Prior research found that a higher likelihood of lifetime HIV testing characterized individuals who self-identified as having sexual minority status, as well as individuals self-reporting their health as poor. 8 Also entering into decisions to receive HIV testing is a history of taking risks by having multiple sex partners or by forgoing condom use during casual sex, increasing the odds of exposure to the virus. 6 In addition, heavy drinking and mental illness appear to be associated with exposure to HIV. Research has linked more-frequent HIV testing to presence of mental illness and engagement in heavy drinking, both of which can facilitate behaving in ways linked to HIV exposure.6,8,11
Why do some populations exhibit less use or later use of HIV testing than others? Are the reasons social in nature? This study used the behavioral model of health services utilization18–20 to explain likelihood of lifetime HIV testing. 21 Moreover, the study simultaneously examined race/ethnicity’s role in this explanation.
To explain individual access to and use of healthcare the health services utilization model weighs important predisposing, enabling, and need factors. 18 Predisposing factors include demographic characteristics, social structural variables, and an individual’s basic beliefs, attitudes, and knowledge pertaining to health services. Enabling factors speak to the resources available, whether individually or in a community. Need factors include the illnesses, conditions, and health statuses requiring health services. 18 Choosing to use health services, then, is closely related to conditions or illnesses individuals exhibit and, additionally, to the presence of specific demographic characteristics and knowledge of HIV and relevant resources available to address infection. Numerous empirical studies have evaluated many predisposing, enabling, and need factors in efforts to explain HIV testing or HIV treatment22–26—although not all such studies have employed Aday’s health services utilization model.
Methods
Our data were derived from the 2013 and 2014 National Health Interview Survey (NHIS). The annual household survey was started by the National Center for Health Statistics (part of the Centers for Disease Control and Prevention) in 1957 and collects cross-sectional data on illness and disability among civilian noninstitutionalized residents of the United States. NHIS researchers used a multistage area probability sampling design, revising their sampling plan every decade. Despite such revision, many similarities persist across plans. In 2013 and 2014, NHIS used a sampling plan implemented in 2006. That plan had oversampled Blacks and Hispanics (as the survey had also done during 1995–2005). In 2013 and 2014, NHIS oversampled Asians as well as Blacks and Hispanics. Our present final sample comprised 18,574 adult (18 or older) respondents and yielded four subsamples: 13,347 Whites, 2267 Blacks, 2074 Hispanics, and 886 Asians. Among adult respondents, the 2013 and 2014 NHIS had response rates of 81.7% and 80.5%, respectively.
Measures
Our study measured a dichotomous outcome: 1 indicated that a respondent had received HIV testing at some point, while 0 indicated no receipt of HIV testing. Applying the health services utilization model, we also measured eight predisposing variables, two enabling variables, four need variables, and one control variable. All predisposing variables were measured dichotomously, the following factors being indicated with a 1: male gender, at least 47 years of age, live-in partner or spouse, employed or worked in the past week, at least some college, worked/volunteered in healthcare setting, US born, and (in year preceding interview) Internet for health information. The factors’ alternative measures were indicated by 0 (not male, no college, foreign born, etc.). We obtained our age categories by calculating the median age, which was 47. We treated worked/volunteered in healthcare setting and also Internet for health information as proxy measures of relative positive attitude toward the healthcare system and relative medical knowledge including of HIV.27,28
The enabling variables measured for our study were family income-to-poverty ratio and insurance coverage. Measuring the first involved four response categories: 1 (ratio lower than 1.0, or below poverty level); 2 (ratio of 1.00–1.99); 3 (ratio of 2.00–2.99); and 4 (ratio of 3.00 or higher). We measured insurance coverage (in year preceding interview) dichotomously, a 1 indicating possession of coverage, a 0 no possession of coverage.
The four need variables were also dichotomous. Sexual minority status indicated (1) self-reported gay, lesbian, or bisexual status. People who are gay/lesbian/bisexual are relatively at risk for HIV infection, the very highest risk being observed among men who have sex with men. 22 We treated binge drink and depression/anxiety as need variables because binge drinking (consuming five or more drinks per day) and mental illness have links to elevated likelihood of risk taking, behavior that can prompt pursuit of HIV testing. 8 A 1 was assigned to respondents who reported binge drinking at least once in the year preceding interview. A 1 was also assigned to respondents who reported chronic presence of depression, anxiety, or both. In addition, a 1 was assigned to respondents who rated their personal overall health as fair/poor; considering one’s health to be less than good is another indicator of need for testing. Each of these need factors’ alternative measures was indicated by 0 (no sexual minority status, no depression/anxiety, etc.). The study’s sole control factor was survey year, with 1 indicating 2014, 0 indicating 2013. It was measured dichotomously in light of our use of data from two annual surveys. Finally, we employed a categorical variable, race/ethnicity, coded into the dichotomous measures Black, Hispanic, Asian, and (providing the reference) White.
Data analysis
We analyzed our data in a multivariate context, using logistic regression techniques to link our predictors (predisposing, enabling, and need factors, plus a control variable) to respondent likelihood of receiving HIV testing at some point. The process was carried out separately for subsamples of Whites, Blacks, Hispanics, and Asian Americans. We used the odds ratios to determine how strong the association was between each independent variable and the likelihood of HIV testing. We used the Wald chi-square statistic to determine if the model did or did not significantly explain our outcome. Race/ethnicity’s power to moderate any relationships among the outcome HIV testing likelihood) and independent variables was evaluated by weighing the interactions of predictors in the model with race/ethnicity. Such interactions were weighed by including all respondents in a single regression analysis, one concerned with interactions of race/ethnicity with each predisposing, enabling, and need variable. Such analysis allowed us to compare, across all groups, the coefficients for each independent variable, while controlling all other independent variables in the model.
The following steps preceded the regression analysis. First, we dummy coded racial/ethnic minority status to generate three dichotomous variables (using the majority status, White, as the reference). Second, we created interaction terms, in turn linking Black, Hispanic, and, finally, Asian American with one of the independent variables. Then, in a series of logistic regression models, we included (a) the variables Black, Hispanic, and Asian American (but not the reference, White); (b) the independent variable in question; (c) the interaction terms involving said independent variable plus the 3 minority-ethnicity variables; and (d) all other independent variables. Statistically significant interactions indicated significant differences between the White majority group and minority groups as to an independent variable’s relationship to the outcome (with other independent variables controlled). Table 2 presents these interactions; significant interactions are indicated by boldface, underlined odds ratios, for Whites and minority groups alike. The multivariate data analysis was conducted with STATA and included the reported sample weight for each NHIS survey.
Results
Table 1 presents descriptive statistics for all variables included in the study. Depending on the nature of a variable, analysis of variance (ANOVA) or chi-square was used to test for racial/ethnic differences in its measure. Excepting worked/volunteered in healthcare setting, all variables were found to differ significantly across racial/ethnic groups. Black and Hispanic respondents were more likely than White and Asian American respondents to have received HIV testing at some point.
Descriptive statistics for all included variables drawn from 2013 and 2014 NHIS for American adults (N = 18,574).

ANOVA was used to test racial/ethnic differences in each of the continuous variables and chi-square was used for dichotomous variables.
p < 0.05.
p < 0.01.
Table 2 presents logistic regression results concerning HIV testing for all the subsamples. We used odds ratios to interpret logistic regression results; an odds ratio above 1 showed that an independent variable had a positive association with the HIV testing outcome. The 0.80 odds ratio for male gender among White respondents was thus interpreted to mean that White males were 20% less likely than White females to have received HIV testing In addition, among White respondents, according to our results, completed HIV testing was associated with female gender, younger age, working or volunteering in healthcare settings, having at least some college, birth outside the United States, acquiring health information from the Internet, not possessing health insurance, self-identified sexual minority status, binge drinking, chronic depression and/or anxiety, and fair/poor personal health.
Multivariate logistic regression explaining lifetime HIV testing for Whites (N = 13,347), Blacks (N = 2267), Hispanics (N = 2074), and Asians (N = 886), per selected 2013 and 2014 NHIS data.
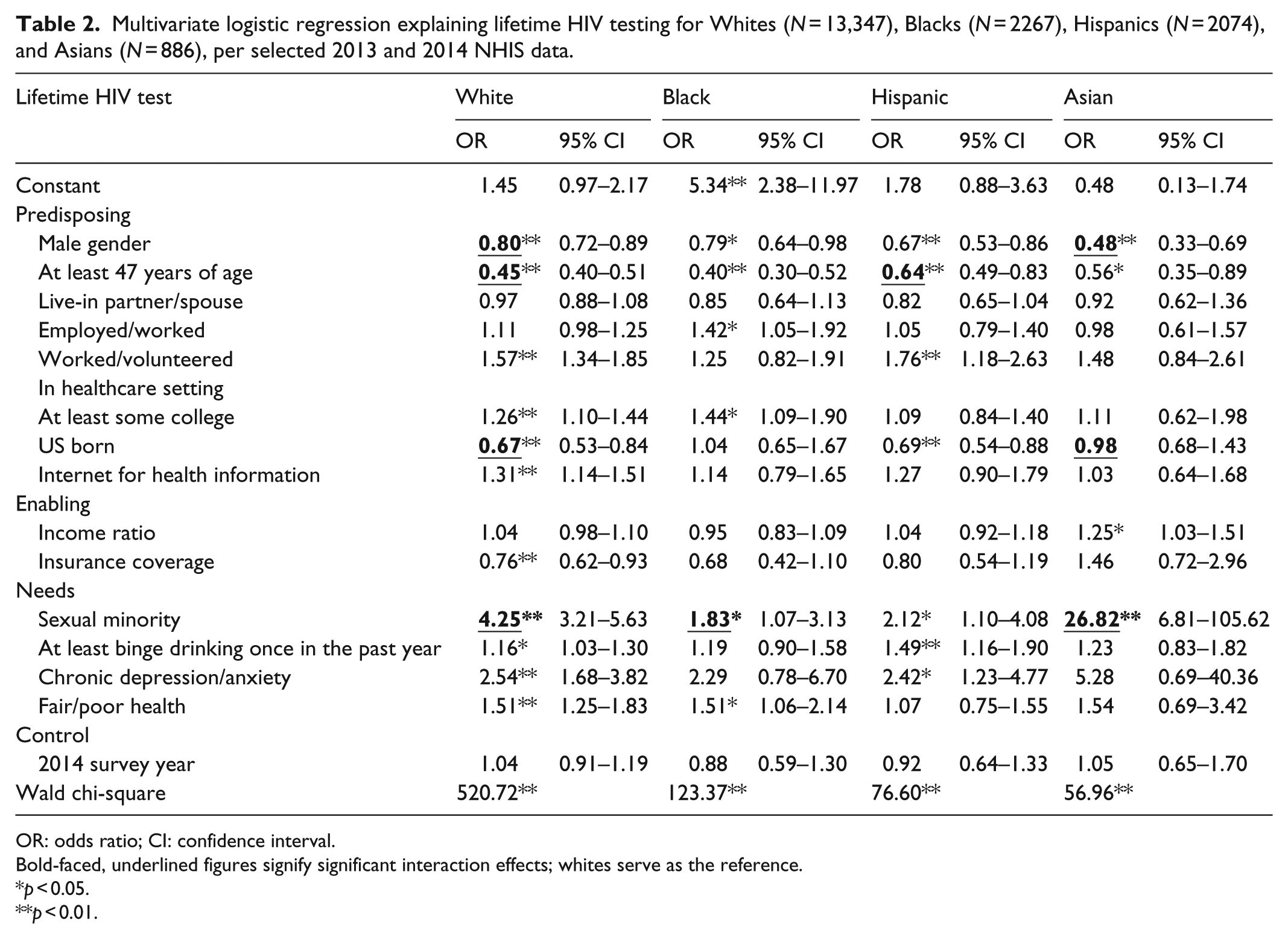
OR: odds ratio; CI: confidence interval.
Bold-faced, underlined figures signify significant interaction effects; whites serve as the reference.
p < 0.05.
p < 0.01.
Among Black respondents we observed completed testing to be associated with female gender, younger age, being employed, having at least some college, self-identified sexual minority status, and fair/poor personal health. For Hispanic respondents, we observed completed testing to be linked to female gender, younger age, working or volunteering in healthcare settings, birth outside the United States, self-identified sexual minority status, binge drinking, and chronic depression and/or anxiety. In Asian American respondents, finally, we observed completed testing to be associated with female gender, younger age, relative wealth, and self-identified sexual minority status. Across all subsamples, our analysis generated significant measures for the Wald chi-square statistic; this indicates that, for each group, the model facilitated explanation of HIV testing
We studied how race/ethnicity moderated associations between past HIV testing and predisposing, enabling, and need variables, using interaction terms we created as outlined above. These terms included five that were statistically significant (see boldface, underlined entries in Table 2). We observed a much stronger link between gender and testing among our Asian American respondents than among our White respondents (odds ratio (OR) = .58, p < 0.01). In addition, among Hispanic respondents compared to White, an observed inverse link between age and completed testing was less strong (OR = 1.32, p < 0.05). Also, US-born Whites in our study appeared less likely to have been tested for HIV than Whites born elsewhere, while no nativity-based difference in the outcome characterized the Asian American subsample (OR = 1.58, p < 0.05). Across all four groups, respondents with self-identified sexual minority status were more likely than others to have been screened for HIV. The relationship between sexual minority status and HIV testing was found to be much stronger for White respondents than for Black respondents (OR = .48, p < 0.05). In addition, HIV testing’s association with sexual minority status was much stronger for Asian Americans than for Whites (OR = 6.5, p < 0.05).
Discussion
Employing the health services utilization model to explain HIV testing we observed—with one exception—that, across races/ethnicities, testing was associated generally with the studied predisposing, enabling, and need factors, and in the anticipated directions. The exception involved the widely used enabling factor insurance coverage. Most often, research finds this variable to be associated with health services utilization; this study instead observed an inverse relationship between insurance coverage and HIV testing among Whites. This may reflect a fear among this population that an HIV diagnosis would threaten their employment (since insurance is typically obtained from employers).23,29 The literature suggests that Blacks and Hispanics have been more likely than Whites and Asians to receive HIV testing. 5 In this study, though, even Blacks’ and Hispanics’ relatively high likelihoods of receiving testing did not approach proportionality with their relatively high prevalence rates for HIV.2,3,16 The results imply that Blacks and Hispanics continue to be disadvantaged populations where HIV infection is concerned. 30 Our results also confirmed that race/ethnicity moderated several associations between the predisposing, enabling, and need factors and the HIV-testing outcome variable. Without HIV testing early detection and treatment of HIV is curtailed.
Two important interpretations and implications warrant discussion here. First, our results for each of the four racial/ethnic groups outline certain social mechanisms that lead to HIV testing. Beyond the established linkage between race/ethnicity and HIV testing we found race/ethnicity’s role in HIV testing to involve interaction with predisposing, enabling, and need factors. For instance, Whites of self-identified sexual minority status were 325% more likely to have been tested for HIV, while among Blacks, self-identified sexual minority respondents were just 83% more likely than others to have been tested. Thus the link between sexual minority status and HIV testing was much stronger among Whites than Blacks in our study. The results may reflect the reality that HIV prevention campaigns often target racial minorities because, whether in or outside the sexual minority, Americans of minority race/ethnicity are at higher risk of infection than White Americans.
Although Asian Americans are counted a racial minority in the United States, their rate of HIV infection resembles that of the majority, Whites. 2 Most of the Asian Americans who have been diagnosed with HIV have been gay or bisexual men. 3 Our finding that Asian Americans of self-identified sexual minority status were significantly more likely than other Asian Americans to have received HIV testing suggests the former perceived a greater personal risk of infection with HIV than the latter did. Among Asian Americans in this study, the relationship between minority sexuality and HIV testing was stronger than it was among Whites.
Our finding that, across ethnic groups, females were more likely than males to have been tested for HIV may reflect standards of care in obstetrics, which dictate prenatal HIV testing. We also found that among Asian Americans specifically (compared to Whites), a larger proportion of females than males reported being tested for HIV. In our study, Asian Americans in the sexual minority were significantly more likely than other Asian Americans to have received HIV testing. Therefore, the relationship we observed between gender and HIV testing among Asian Americans in the sexual minority may indicate that females in this study had relatively stronger concern for personal health and/or HIV infection risk than males did. Furthermore, this relationship may indicate that, among Asian Americans in the sexual minority, males’ sexuality-related shame is stronger than females’.
Younger respondents were relatively likely to have received HIV testing; the relationship between age and HIV testing was stronger for Whites than for Hispanics. Furthermore, while US-born Whites in our study were less likely to have completed testing than Whites born abroad, no difference in HIV testing likelihood appeared to distinguish US-born Asian Americans from Asian Americans born elsewhere. Perhaps the contrast in nativity’s effect on Whites versus Asian Americans arose from very recent growth in Asian immigration; since 2010, relatively few immigrants have been White.8,12
The second important implication of our results is that ways exist to improve current policies and practices meant to reduce health disparities generally, and disparities in HIV testing particularly. We observed that, compared to Whites, Blacks’ likelihood of receiving HIV testing was relatively similar from one sexual status to the other (i.e. from minority to majority sexual status). This is consistent with the extant literature, which suggests minority Americans, especially Blacks, are more likely than Whites to receive HIV testing. 5 The finding indicates, too, that it is not unusual for Black Americans to be tested even when no elevated personal risk of infection is perceived. 31 The weaker relationship between sexual minority status and HIV testing that we found for the subsample of Black respondents may indicate that some barriers to utilization of services affect Blacks of sexual minority status who perceive a need for HIV testing. Barriers can be dismantled, through governmental and educational efforts. We need to reduce stigmatization of HIV infection afflicting members of sexual minorities, and we need to build Blacks’ trust in health services. 32 Mistrust might perhaps be reduced through peer mentorships featuring mentors and mentees of common race/ethnicity. Through these relationships, moreover, messages could be shared about the importance of early diagnosis for people in sexual minorities. 7 Considering the high rate of undiagnosed HIV infection in the United States, the present results also suggest that, in particular, male Asian Americans and younger Hispanic Americans should be encouraged to obtain HIV testing as part of a strategy to boost screening in all racial/ethnic groups. With testing comes increased early diagnosis, and with early diagnosis come reduced HIV transmission, longer life expectancy (especially for those of minority race/ethnicity), and lower treatment costs.30,33
Three important limitations affecting our study should be mentioned. First, the data’s secondary nature limited the variables available to our analysis and our explanation of HIV testing For example, injection drug use is relevant to HIV infection, clearly constituting a key need factor from the perspective of the health services utilization model. But NHIS data did not describe such drug use. As well, while HIV testing is at times attributable to personal behavior (deciding to be tested), it is at other times attributable to, or at least reflective of, systems factors in HIV screening. Our NHIS data were insufficient to differentiate the two attributions.
Second, to explain race/ethnicity’s role in HIV testing we derived from prior published research the assertion that racial/ethnic status reflects differential stigmatization, discrimination, and mistrust. In the future, specific, dedicated measures of stigmatization, discrimination, and mistrust should be developed and deployed to enhance understanding of social mechanisms that lead from race/ethnicity to explanation of HIV diagnosis.
Third, because NHIS collected its data on health, healthcare, and health behaviors via face-to-face interviewing, nonresponse may indicate a tendency among Americans to avoid confiding in a stranger. The matter raises the related difficulty that our sample could be susceptible to bias. Our respondents could include a few who had actually chosen to avoid HIV testing altogether, when indeed avoiders should have constituted most of the one-fifth (roughly) of contacted individuals who did not respond to NHIS researchers. This would, of course, also bias the study results. Due to the sample we employed, then, we specifically caution readers about possibly overestimated rates of HIV testing in our study. Moreover, unless any such overestimation happened to be distributed evenly across all four groups, we may have inaccurately identified race/ethnicity’s moderating role in HIV testing rates.
Conclusion
In the United States, higher rates of HIV diagnosis have been associated with Black Americans and Hispanic Americans than with White Americans. Among respondents in this study, Blacks and Hispanics were more likely than Whites and Asian Americans to report lifetime HIV testing. We found that the predisposing, enabling, and need factors identified by Aday make up a social mechanism that can explain racial/ethnic differences in HIV testing rates of White, Black, Hispanic, and Asian Americans. Across races and ethnicities, it is generally those Americans with the greatest need for HIV testing—namely, individuals of sexual minority status—who are more likely to have received it. Development of policies and practices should be guided by what our study observed about race/ethnicity’s role in HIV testing The objective for any policy or practice should be the minimizing of racial health disparities attributable to HIV infection.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
While collecting the data employed in the 2013 and the 2014 National Health Interview Survey, the National Center for Health Statistics (part of the Centers for Disease Control and Prevention) obtained voluntary consent from each respondent and provided written assurance of privacy for the information provided. Prior to the undertaking of the present analysis of this information, the Texas Woman’s University Institutional Review Board approved the research, finding it to meet strict ethical standards. Having the Texas Woman’s University Institutional Review Board’s approval means that written informed consent from all subjects was waived for this research project. Ethical approval for this study was waived by Texas Woman’s University’s Institutional Review Board because secondary data were used to conduct the study
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article was published with support from Texas Woman’s University Libraries’ Open Access Fund.