
Abstract
Background:
Cognitive impairment is highly prevalent among older adults (aged ≥65 years) hospitalized for heart failure and has been associated with poor outcomes. Poor medication self-management skills have been associated with poor outcomes in this population as well. The presence and extent of an association between cognitive impairment and poor medication self-management skills in this population has not been clearly defined.
Objective:
We assessed the cognition of consecutive older adults hospitalized for heart failure, in relation to their medication self-management skills.
Methods:
We conducted a cross-sectional study of older adults (aged ≥65 years) who were hospitalized for heart failure and were being discharged home. Prior to discharge, we assessed cognition using the Mini-Cog. We also tested patients’ ability to read a pill bottle label, open a pill bottle safety cap, and allocate mock pills to a pill box. Pill allocation performance was assessed quantitatively (counts of errors of omission and commission) and qualitatively (patterns suggestive of knowledge-based mistakes, rule-based mistakes, or skill-based slips).
Results:
Of 55 participants, 22% were found to have cognitive impairment. Patients with cognitive impairment tended to be older as compared to those without cognitive impairment (mean age = 81 vs 76 years, p = NS). Patients with cognitive impairment had a higher prevalence of inability to read pill bottle label (prevalence ratio = 5.8, 95% confidence interval = 3.2–10.5, p = 0.001) and inability to open pill bottle safety cap (prevalence ratio = 3.3, 95% confidence interval = 1.3–8.4, p = 0.03). While most patients (65%) had pill-allocation errors regardless of cognition, those patients with cognitive impairment tended to have more errors of omission (mean number of errors = 48 vs 23, p = 0.006), as well as more knowledge-based mistakes (75% vs 40%, p = 0.03).
Conclusion:
There is an association between cognitive impairment and poor medication self-management skills. Medication taking failures due to poor medication self-management skills may be part of the pathway linking cognitive impairment to poor post-discharge outcomes among patients with heart failure transitioning from hospital to home.
Keywords
Introduction
Cognitive impairment (CgI) is highly prevalent among older adults hospitalized for heart failure (HF) and has been associated with poor post-discharge outcomes including hospital readmissions and mortality. 1 The mechanisms linking CgI and post-discharge risk have not been clearly defined.
A potential mechanism linking CgI to poor post-discharge outcomes may be medication non-adherence due to poor medication self-management skills. Several observations may support this. First, patients with HF are prescribed, on average, seven medications per day, 2 each with different dosages and varying frequencies. Prior studies have shown that medication adherence drops as more medications are added and multiple doses per day are required,3–8 and that poor medication self-management skills are associated with increased healthcare utilization, including emergency department visits. 9 Second, CgI in patients with HF has been associated with poorer medication adherence and worse self-care.10–12 Third, abnormal cognitive function is a known determinant of inadequate health literacy, defined as “the degree to which individuals can obtain, process, and understand basic health information and services needed to make appropriate health decisions,” 13 in both older adults and patients with chronic HF.14,15 Components of medication self-management, including the ability to read a pill bottle label, are reflective of health literacy. 16 Low health literacy has been associated with higher all-cause mortality in outpatients with HF. 13
Adherence to medications requires patients to initiate a prescribed medication appropriately (first phase), implement dosing correctly (second phase), and avoid inappropriate discontinuation (third phase). 17 Root causes of medication non-adherence are not clearly understood, but are presumed to involve a complex interplay between healthcare system factors, medical illness, pharmacotherapy, socioeconomic factors, and patient factors.4,5,7,18 Little attention has been paid to medication self-management skills as a driver of medication non-adherence among patients hospitalized for HF, and it is unknown to what extent CgI may make it worse.
Medication-self management has been defined by one group of investigators as “the extent to which a patient takes medication as prescribed, including not only the correct dose, frequency, and spacing but also its continued, safe use over time.” 19 To our knowledge, several approaches have been developed to formally assess medication-self management skills,20,21 though there is a lack of consensus about which tool clinicians should use. Furthermore, to our knowledge, these tests have not been studied in populations of older adults hospitalized for HF. Common elements of these tools include assessment of the ability to read a pill bottle label, open a pill bottle, and correctly allocate pills.
We hypothesized that there is an association between CgI and poor medication self-management skills among older adults hospitalized for HF. To test this hypothesis, we assessed the cognition of consecutive patients hospitalized for HF, in relation to their ability to (1) read a pill bottle label, (2) open a pill bottle, and (3) allocate pills into a pill box.
Methods
Study population
We performed a cross-sectional study at Cleveland Clinic, a large academic hospital in Cleveland, Ohio, involving hospitalized HF patients ≥65 years of age, whose medical team intended to discharge them home. We focused on a home-going population as these patients are anticipated to have appropriate medication self-management skills, specifically being able to initiate and implement 17 their medications as prescribed. Inclusion criteria included the following: able and willing to sign informed consent, aged ≥18 years, hospitalized for primary diagnosis of HF as defined by the ASCEND-HF (Acute Study of Clinical Effectiveness of Nesiritide and Decompensated Heart Failure) 22 enrollment criteria (dyspnea at rest or with minimal activity and treatment with intravenous diuretics for HF during the hospitalization, at least one of the two clinical signs of HF (respiratory rate of >20 breaths/min or rales at least one-third above lung base), and at least one of the four objective measures of HF (evidence of congestion or edema on chest radiography, a B-type natriuretic peptide (BNP) level ≥400 pg/mL or an N-terminal pro-BNP level ≥1000 pg/mL, pulmonary-capillary wedge pressure >20 mm Hg, or left ventricular ejection fraction <40% in the previous 12 months)), and anticipated discharge to home as indicated by the hospital ward’s care manager or social worker. Exclusion criteria included the following: anticipated discharge to nursing home or rehabilitation facility, or anticipated discharge to hospice. We inquired about the use of reading glasses at the start of testing, and if patients required glasses, we made sure they had them before proceeding. The study was approved by the Institutional Review Board at Cleveland Clinic.
Recruitment and study procedures were carried out by two internal medicine resident physicians who are also co-authors of this work (E.H.H. and A.S.). Potential patients for this study were identified from a daily hospital admissions list that was cross-verified by the above-mentioned inclusion criteria. A total of 30 to 60 min were allotted for study completion per enrolled subject.
Assessment of cognition
We assessed cognition with the Mini-Cog, a three-item recall and clock-drawing test.1,23 We scored this test on a 5-point scale (1 point for each correct word recalled and 2 points for correct clock drawing), with a score of ≤2 defining presence of CgI. 23 We chose this instrument because of its brevity, speed of application (on average, it takes approximately 3 min to complete), and prior literature describing its utility in patients hospitalized for HF.1,10 The Mini-Cog has been shown to classify moderate and severe dementia with excellent accuracy, mild dementia with good accuracy, and mild CgI with mild accuracy.10,24
Assessment of medication self-management skills
Patients were provided 5 pill bottles representing common HF medications, each filled with 30 mock pills, and a weekly pill box with 4 pill slots per day. Pill bottles (16 dram) were labeled with standard pharmacy directions (Arial font, size 10) for each medication, including the following: Furosemide, take one capsule by mouth daily; Lisinopril, take one capsule by mouth daily; Carvedilol, take one capsule twice daily; Hydralazine, take one capsule by mouth three times daily; and Isosorbide Dinitrate, take one capsule by mouth three times daily.
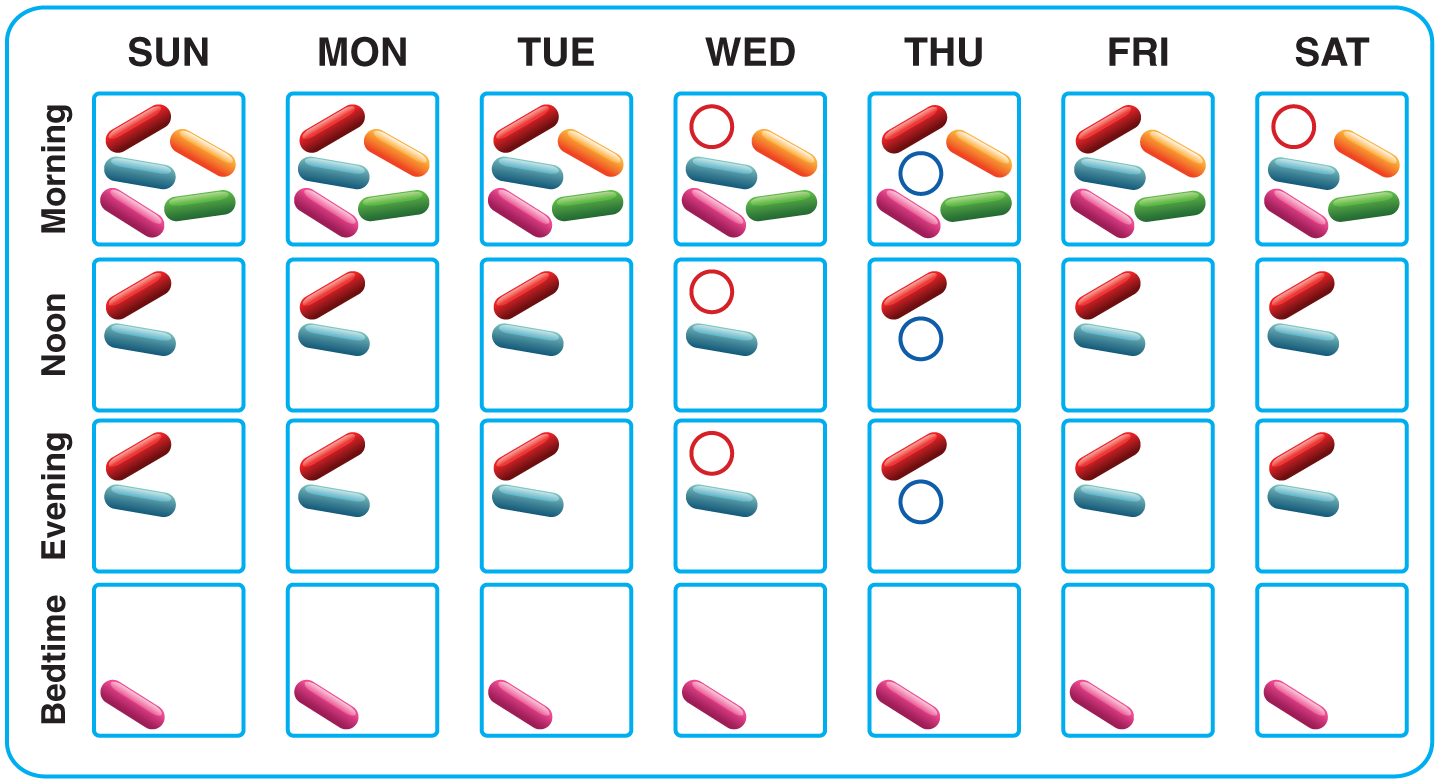
Medication self-management skills were assessed using three sequential tasks. The first task was to read a label on a pill bottle, the second task was to open a standard pill bottle safety cap, which requires pushing cap down and turning to open, and the third task was to allocate pills from the five pill bottles to the weekly pill box (Figure 1). Correct pill allocation involved placing a total of 70 different pills into the above-mentioned 4 × 7 pill box. Varying patterns could represent correct filling (an example and further discussion is shown in Figure 1) because the pill labels did not state the time of day that a pill should be taken (e.g. “Take in the morning”) nor the interval between two intakes (e.g. “Take 12 h apart”). Patients were not given the opportunity to familiarize themselves with pill bottles before testing; however, these are standard pill bottles used at all Cleveland Clinic outpatient pharmacies, making it likely that patients had used similar ones in the past. The first two tasks were assessed as pass or fail, and the third task was assessed both quantitatively and qualitatively, as described below.

Weekly pill box with one possibility of correctly allocated pills. Medications represented are as follows: Furosemide, take one capsule by mouth daily (green); Lisinopril, take one capsule by mouth daily (orange); Carvedilol, take one capsule twice daily (pink); Hydralazine, take one capsule by mouth three times daily (red); and Isosorbide Dinitrate, take one capsule by mouth three times daily (blue). The following minor variations were counted as correct (i.e. neither an error of omission nor an error commission): placement of once daily medication (Furosemide and Lisinopril) in any one of the four daily slots, placement of twice daily medication (Carvedilol) in any two of the four daily slots, and placement of three times daily medication (Hydralazine and Isosorbide Dinitrate) in any three of the four daily slots. An example of an error of omission related to Lisinopril would be if an orange pill did not appear at all in any of the four slots of an individual column (e.g. none of the “Monday” column 4 slots contain an orange pill). An example of an error of commission related to Lisinopril would be if two orange pills, in any combination, would appear in any individual column (e.g. both the “morning” and “afternoon” slots in the “Monday” column contain one pill in each). An example of a single pill-allocation error resulting in both an error of commission and an error of omission related to Carvedilol would be if two pink pills would appear in only one slot of any individual column (e.g. the “morning” slot on “Sunday” has two pink pills, while the “bedtime” slot on “Sunday” has no pink pill).
Two categories of quantitative pill-allocation errors were derived as follows: (1) errors of omission: a mistake of not putting correct pill into correct pill box slot and (2) errors of commission: a mistake of putting pill into wrong pill box slot. It was possible for a single pill-allocation error to result simultaneously in both an error of omission and an error of commission; this is discussed further in Figure 1 legend.
In addition, pill-allocation errors were classified into qualitative categories according to Reason’s three previously described categories of human error.25,26 Each error could only be attributed to one qualitative category. These consisted of the following:
Knowledge-based mistakes. Mistakes are errors in performance and may be related to failures in perception, judgment, inference, and interpretation. Knowledge-based mistakes occur when current knowledge or previously learned routines are not sufficient to specify what to do next. They can occur when an individual encounters a new situation that is outside his or her usual problem-solving routines. Based on this, we categorized patterns of pills allocated in no meaningful manner in relation to pill bottle directions or pill box organization as knowledge-based mistakes (examples are shown in Figure 2).
Rule-based mistakes. These types of errors occur from incorrect application of a rule or procedure, which may be caused by misinterpretation of the challenge at hand. We categorized patterns of repeating errors in pill allocation as rule-based mistakes (examples are shown in Figure 3);
Skill-based slips. These types of errors occur during routine activities, when attention is diverted from a task either by inattention or external distracting factors. A slip is an unintentional action occurring at the point of task execution. Based on this, we categorized patterns of minor/occasional errors appearing likely related to temporary diversion of attention as skill-based slips (an example is shown in Figure 4).

Examples of qualitative allocation errors categorized as knowledge-based mistakes (pills allocated in no meaningful manner in relation to pill bottle directions or pill box organization): (a) a pill box with 67 errors of omission and 27 errors of commission, (b) 2 errors of omission and 63 errors of commission, and (c) 57 errors of omission and 11 errors of commission.

Example of qualitative allocation errors categorized as rule-based mistakes (repeating errors in pill allocation): (a) a pill box with 35 errors of omission and 35 errors of commission, (b) 35 errors of omission and 37 errors of commission, and (c) 60 errors of omission and 27 errors of commission.
Example of qualitative allocation errors categorized as skill-based slips (patterns of minor/occasional errors appearing likely related to temporary diversion of attention): a pill box with 7 errors of omission.
Validation cohort
We performed a face validation of the three medication self-management tasks in a healthy non-hospitalized population (n = 30), consisting of pharmacy residents and internal medicine resident physicians. Our primary goal was to evaluate the tasks for design flaws, so we enrolled medical professionals, where any errors could be attributed to false positives and less likely related to deficits in cognition, physical disability, or poor health literacy. We collected information regarding age, sex, and personal medication use.
On average, validation cohort subjects were younger men (mean age = 29 (median = 28, range = 24–37) years, 63% male). In total, 12 subjects (40%) in the validation cohort reported taking one or more medications on a daily basis.
All 30 subjects (100%) were able to read pill bottle labels, and all (100%) were able to open at least one pill bottle. Subjects in the validation cohort made a very low number of pill-allocation errors (errors of omission averaged = 0.03, standard deviation (SD) = 0.2, with a range of 0–1 errors; errors of commission averaged = 0.1, SD = 0.3, with a range of 0–1 errors). Qualitative analysis of pill errors showed that all three subjects (10%) made skill-based slips alone.
Data variables and outcomes
We collected demographic and clinical variables based on previously published American College of Cardiology/American Heart Association (ACC/AHA) definitions. 27 Health literacy was assessed using the questionnaire from Peterson et al. and Chew et al.,13,28 which included the following three questions: “How often do you have someone help you read hospital material?”, “How often do you have problems learning about your medical condition because of difficulty reading hospital materials?”, and “How confident are you filling out forms by yourself?” In brief, a score is obtained on a 5-point Likert scale with a higher score denoting lower literacy. 13 Scores were summed and dichotomized such that a total score greater than 10 was categorized as low health literacy and a score of 10 or lower as adequate health literacy. 13 Frailty was assessed using the Fried criteria, 29 whereby presence of three or more of the following indicated frailty: unintentional weight loss, weak handgrip strength, self-reported exhaustion, slow gait speed, and low self-reported physical activity. HF with preserved ejection fraction (HFPEF) was defined as left-ventricular ejection fraction ≥50%. 30 Estimated home value was determined from Zillow (www.zillow.com) or Trulia (www.trullia.com), and median household income from the US census data based on city of residence (http://quickfacts.census.gov/qfd/states/39/3945556.html). These variables were obtained to better describe patients’ socioeconomic status.
Statistical analyses
We stratified baseline characteristics, and performance on medication self-management skills tasks, by cognitive status. We compared deficits in medication self-management skills between patients with and without CgI using the prevalence ratio (PR; 95% confidence interval (CI)) and chi-squared p-value.31,32 We compared numbers of quantitative pill-allocation errors graphically using boxplots and by calculating means and SDs.
Analyses were performed with using R, version 3.0.2 (www.r-project.org). We used Stevenson’s epiR library version 0.9-62 (https://cran.r-project.org/web/packages/epiR/epiR.pdf) for calculating PRs and p-values, and Wickham’s ggplot2 library version 0.9.3.1 (www.ggplot2.org) for graphics.
Results
Study flow
Recruitment and study procedures were carried out in intermittent 1-week blocks between November 2012 and March 2013. During these 1 week blocks, all patients were reviewed, approached, and consented in a consecutive manner. Of the 94 consecutive HF inpatients who were the potential candidates for the study, 74 were approached for enrollment, of which 56 consented to participate. Those who were not approached (n = 20) were discharged from the hospital prior to the investigators being able to offer them enrollment in a timely manner. Reasons patients who were offered enrollment refused or were unable to consent (n = 18) included the following: patient preferred no more testing while hospitalized (n = 8), patient refused with no reasons given (n = 6), patient had concerns about confidentiality (n = 2), patient had concerns about additional unknown costs related to research participation (n = 1), and patient expired in hospital (n = 1). Characteristics of the 38 patients who did not participate were as follows: mean age = 76 (range = 66–88) years, 50% male, 32% White, 26% with New York Heart Association (NYHA) functional class III or IV, 39% with HFPEF, 34% with ischemic cardiomyopathy, and 5% with prior diagnosis of dementia. As compared to those patients who consented, patients who refused tended more frequently to be female and of non-White race. Of the 56 patients who consented, subsequently 1 refused to complete medication self-management testing, leaving 55 patients who completed the study. For these 55 patients, all study procedures universally occurred on the day of consent and took place a median of 1.0 days (25th, 75th percentile: 0 days, 2 days) prior to hospital discharge.
Participants’ baseline characteristics
Of the 55 patients who participated in the study, 12 (22%) were found to have CgI as assessed by the Mini-Cog. Patients’ characteristics, stratified by Mini-Cog performance, are summarized in Table 1. Patients with CgI had more NYHA class III or IV symptoms (p < 0.01) and more objectively assessed frailty (p = 0.04). There were no significant associations between CgI and age, sex, race, home value, help managing medications at home, and health literacy.
Baseline characteristics.
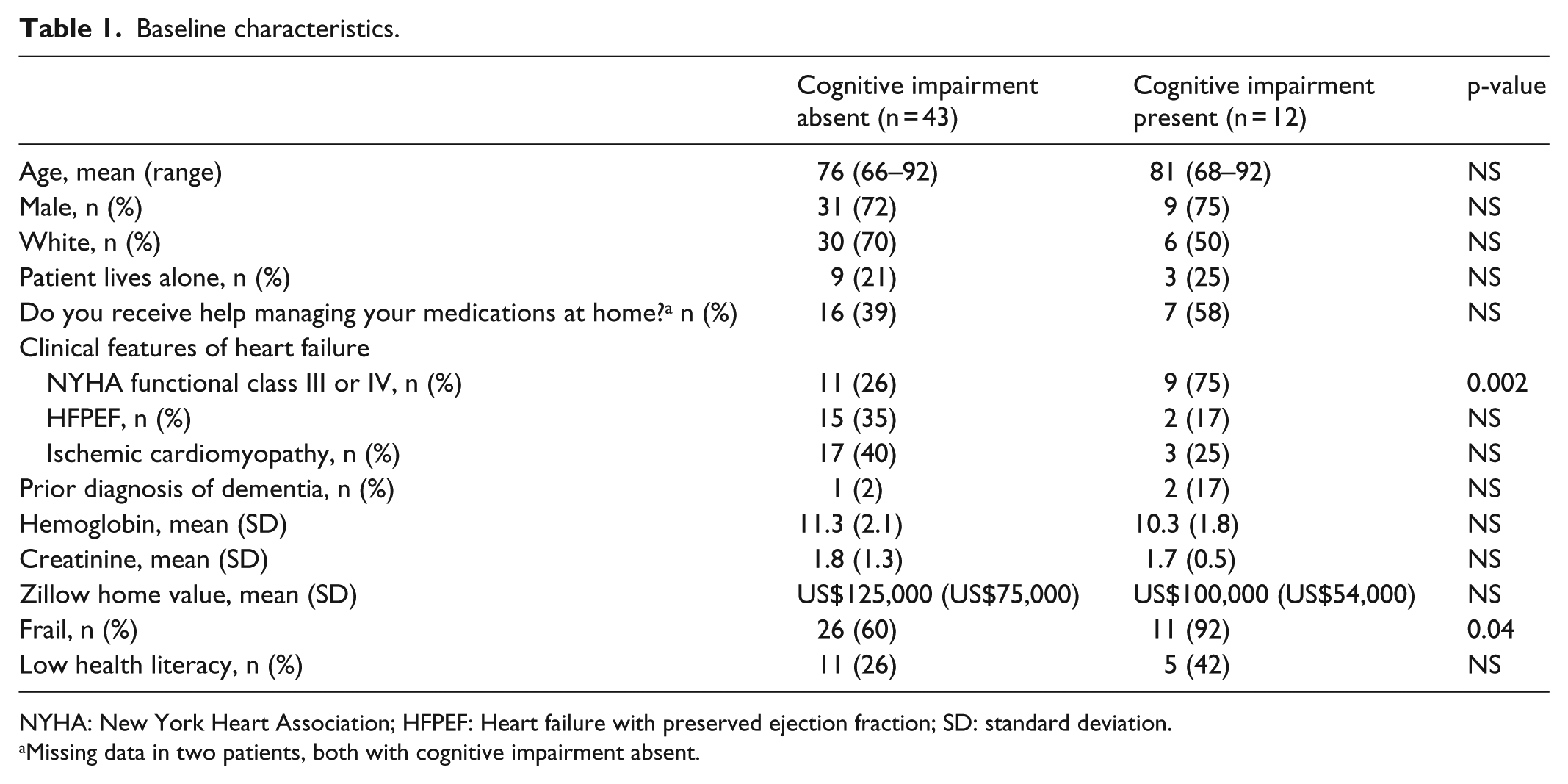
NYHA: New York Heart Association; HFPEF: Heart failure with preserved ejection fraction; SD: standard deviation.
Missing data in two patients, both with cognitive impairment absent.
Performance on medication self-management tasks
A majority of patients (Table 2) were able to read the pill bottle label (n = 52, 95% of patients) and open the pill bottle safety cap (n = 50, 91%). Reasons for failure to open the bottle included pain (n = 2), hand arthritis (n = 1), weakness (n = 1), and confusion (n = 1). Overall performance on the pill allocation task was poor (Table 2), with a majority of patients committing skill-based slips, knowledge-based mistakes, or rule-based mistakes.
Medication self-management tasks.

SE: standard error; SD: standard deviation.
Performance on medication self-management tasks, stratified by Mini-Cog performance
Patients with CgI had a higher prevalence of inability to read the pill bottle label (25% vs 0%; PR = 5.8, 95% CI = 3.2–10.5, p = 0.001) and inability to open the pill bottle safety cap (25% vs 5%; PR = 3.3, 95% CI = 1.3–8.4, p = 0.03), as compared to those without CgI (Table 2). Only one patient with CgI failed to both read the pill bottle label and open the pill bottle safety cap, while the other two patients in each category were independent.
Patients with CgI committed more errors of omission as compared to those without CgI (p = 0.006) and a similar number of errors of commission (p = NS) (Table 2; Figure 5). Furthermore, patients with CgI had a higher prevalence of knowledge-based mistakes (75% of patients with CgI vs 40% of patients without CgI, p = 0.03) (Table 2).

Quantitative pill-allocation errors stratified by Mini-Cog performance. Boxplots of (a) errors of omissions and (b) errors of commission. Mean values are shown with red dot.
Discussion
In this study of older adults hospitalized for HF who were to be discharged home, we found an association between CgI and poor medication self-management skills. Patients with CgI had a higher prevalence of an inability to (1) read the pill bottle label, (2) open the pill bottle safety cap, and (3) correctly allocate pills into the pill box. While most patients (65%) had pill-allocation errors regardless of cognitive status, patients with CgI had more concerning types of pill-allocation errors as compared to those without CgI. These errors included more errors of omission, as well as knowledge-based mistakes.
Previously published work in various populations including community-dwelling older adults who were outpatients,20,33–35 older outpatients with schizophrenia, 21 and mixed populations of medical and surgical inpatients 36 support the hypothesis that CgI is associated with poor medication management skills. Our findings expand on this literature by specifically evaluating a variety of medication self-management skills in older adults hospitalized for HF. Additionally, we tested pragmatic tasks including reading a pill bottle label, opening a pill bottle, and allocating pills to a pillbox, all of which are necessary components of medication self-management in a HF population.
Guidelines regarding transitions of care for patients with HF recommend routine screening for high-risk characteristics that may be associated with poor post-discharge clinical outcomes, including cognitive difficulties. 37 These guidelines also recommend medication reconciliation, medication education, and implementation of handoff procedures that detail discharge medications. Future research should focus on how to manage these complex aspects of medication self-management among HF patients with CgI. It may be that intensive medication education will be insufficient in this population due to an inability to understand or retain information. It is unknown if other interventions such as medication education of the patient’s family or social circle, or use of pre-packaged medications 38 may be effective in improving outcomes.
Our study has several limitations. First, we defined CgI by poor performance on the Mini-Cog, which is a succinct measure of cognitive status. Perhaps, other more detailed cognitive tests, such as the Montreal Cognitive Assessment (MOCA) or Mini Mental State Exam (MMSE), would have yielded different findings in our population. 10 There is no consensus on which cognitive assessment tool should be used in HF populations. 1 Second, due to absence of a standardized approach to assessment of medication self-management skills in HF patients, we had developed a novel approach to do so. Further studies are needed to develop and validate an efficient and optimal approach to assess medication self-management skills in HF patients. Third, we used mock pills rather than the patients’ own home medications because patients acutely hospitalized for decompensated HF in our institution tended not to have their own medication bottles with them. It is possible that performance on our medication self-management test would have been better had patients had medication bottles they were more familiar with. This should be investigated in future studies. Fourth, we did not collect information about the proportion of patients who were familiar with the medication regimen used in the study. Pre-existing knowledge of the study regimen could have introduced bias which we did not account for. Fifth, we used capsules of various colors in our study rather than plain white tablets which are the more common oral solid formulation worldwide. This may have introduced bias toward improved medication self-management performance. Sixth, this was a single-center study from a tertiary referral hospital with limited sample size, which may limit generalizability. Seventh, because of a variety of reasons detailed in the “Methods” section, not all potential candidates for the study were approached. This may have introduced a selection bias, whereby sicker and more complex patients refused participation. Eighth, not all patients approached agreed to participate, which may have introduced selection bias as well.
We believe that our findings have several important implications for clinical practice. First, clinicians who care for patients hospitalized for HF should consider screening patients for CgI in a routine fashion and should be aware of the potential association between CgI and poor medication self-management. 10 Second, clinicians who prescribe medications for patients transitioning home after a hospitalization for HF should not assume that their patients can perform even the simplest tasks (reading labels, opening pill bottles, and allocating pills to pill box) required to manage these medications correctly. Clinicians should consider directly testing patients’ abilities to perform these medication self-management skills. Published HF guidelines do not currently recommended this type of evaluation, but maybe they should. Third, clinicians who routinely assess for CgI should not assume that a lack of it is sufficient in ruling out problems with patients’ ability to allocate their pills. In our study, we found a large number of pill-allocation errors even among patients who were cognitively intact.
In conclusion, we found an association between CgI and poor medication self-management skills among older adults hospitalized for HF with an intended home discharge. In addition to difficulties with reading pill bottle label, and opening pill box, patients with CgI had a higher rate of errors of omission which were qualitatively knowledge-based mistakes. Our findings, which should be considered to be preliminary due to our limited cohort size, suggest that medication taking failures due to poor medication self-management skills may be part of the pathway linking CgI to poor post-discharge outcomes among patients with HF transitioning from hospital to home.
Footnotes
Acknowledgements
The authors are grateful to four anonymous peer reviewers for their thoughtful and constructive critiques, which they believe have strengthened the presentation of this work.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:Dr Gorodeski was a consultant for Novartis in 2015.
Ethical approval
Ethical approval for this study was obtained from Cleveland Clinic’s Institutional Review Board (study number 16-524).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This study was funded by the Hunnell Research Fund.
Informed consent
Written informed consent was obtained from all subjects before the study.