
Abstract
Background:
Acromegaly and endocrine tumors are uncommon morbidities that are currently treated with different drugs.
Objective:
To determine the prescription patterns of somatostatin analogues in patients affiliated with the Health System of Colombia.
Methods:
Retrospective cohort study of patients of any age and sex treated with octreotide or lanreotide between January 2011 and August 2015. Socio-demographic, clinical (indications) and pharmacological (comedications) variables were considered. Multivariate analysis was performed with SPSS 23.0.
Results:
We identified 289 patients, with a mean age of 56.6 ± 14.0 years and female predominance (59.5%), who underwent treatment during the 56 months of monitoring. Octreotide was used in 56.1% of cases, followed by lanreotide (43.9%), both at approved doses. We found that 4.5% of subjects changed from one drug to another over the course of therapy, which was associated with being diabetic and receiving insulin (odds ratio: 4.27; 95% confidence interval: 1.23–14.84; p = 0.014). The most common indications were acromegaly (52.2% of cases) followed by neuroendocrine tumors (15.9%). The most common comorbidities were hypertension (39.4% of cases), depression (27.3%), dyslipidemia (23.3%), diabetes mellitus (23.5%) and hypothyroidism (23.5%). Being male (odds ratio: 0.57; 95% confidence interval: 0.35–0.94; p = 0.029) and belonging to the age group between 45 and 65 years (odds ratio: 0.44; 95% confidence interval: 0.21–0.90; p = 0.024) were significantly associated with a lower risk of receiving comedications.
Conclusion:
Somatostatin analogues are being used at recommended doses, especially in patients with acromegaly and neuroendocrine tumors. Variables associated with change in therapy were identified.
Introduction
Acromegaly is a relatively uncommon disease, with an estimated global prevalence of 40–50 cases per million inhabitants.1,2 Its primary cause is the hypersecretion of growth hormone (GH) from a benign pituitary adenoma that leads to disproportionate tissue growth.1–3 As a result, patients suffer body deformations and even cardiovascular and neuroendocrine complications that can alter their quality of life and life expectancy in addition to the increased costs from medical and surgical therapy.4,5
Neuroendocrine tumors are rare neoplasms that originate from neuroendocrine cell localized in numerous different organ systems. Most frequently, these tumors are found in the gastrointestinal tract and the bronchopulmonary system. These cells are characterized by amine and neuropeptide hormone production and dense core vesicles. Despite the diversity in tissue origin, all these tumors share common features, including pattern of growth and expression of neuroendocrine markers. They can be present in all organs and tissues where there are neuroendocrine cells.6,7 Their annual incidence is approximately 40 cases per million, of which 1%–2% are gastrointestinal malignancies. 8 Given the diversity of manifestations and the difficulty in diagnosis, neuroendocrine tumors can affect the life expectancy of those that suffer from them and require costly treatments. 9
Somatostatin analogues play an important role in the treatment of acromegaly and neuroendocrine tumors and are considered the medical therapy of choice in those patients who are not managed surgically. 10 They control clinical symptoms caused by the excessive secretion of hormones and tissue differentiation, in addition to inhibiting the secretion of pancreatic and gastrointestinal hormones and reducing the blood flow to visceral vessels. 10 This group of drugs exerts their biological functions by binding with varying affinity to the five somatostatin receptors present in the hypophysis and in tumor cell membranes.4,10,11 Currently, octreotide and lanreotide, semisynthetic derivatives with long elimination half-lives that bind to somatostatin receptors, SST2 and SST5, are used. In their current presentations of prolonged action, they are able to be administered every 4 weeks.8–15
The Health System of Colombia (General System of Social Security in Health (SGSSS)) covers the entire population of the country through two care regimens, one that is paid and the other that is subsidized by the State, that include benefit plans that include medications and access to health technologies. Given that somatostatin analogues are available and because there is a lack of information on their use in this population, we intended to determine the prescription patterns of somatostatin analogues in patients affiliated with the SGSSS between the years 2011 and 2015.
Methods
A retrospective cohort study was conducted to learn about the prescription patterns and use of somatostatin analogues (octreotide long-acting release (LAR) and lanreotide Autogel) by monitoring dispensed monthly medications. This study considered the consumption trends between January 2011 and August 2015 from the population database of approximately 6.5 million people affiliated with the contributive or paid regimen of the SGSSS belonging to different insurance companies (Health Promoting Entities–EPS) and health provider institutions -(Institución Prestadora de Salud, (IPS)) in 22 cities in Colombia.
A database designed was reviewed and validated by a physician (doctor in pharmacology), allowed for the collection of groups of variables associated with the use and modification of therapy of the patients prescribed with somatostatin analogues during the observation period, which is described below:
Socio-demographic variables: age, sex and city of residence.
Clinical variables: clinical diagnosis identified in the medical formula and modification of the dose or medication; recorded adherence to treatment is estimated by continuity of periodic drug dispensations (delivered to the patient each month uninterrupted).
Use of long-acting somatostatin analogues (patterns and consumption trends): the number of patients during the monitoring years with a monthly prescription of octreotide LAR (Sandostatin LAR®) and lanreotide Autogel (Somatuline Autogel®) and the prescribed dose were recorded. For quantification of dispensation, the daily defined dose (DDD) recommended by the World Health Organization (WHO) as the international standard was used as a technical measurement unit for carrying out pharmacoepidemiological studies, in addition to the dose recommended by the manufacturers of the molecules.
Concomitant use of other medications for the underlying disease, for example, cabergoline and everolimus.
Comedications were considered as substitutive variables of the following most common comorbidities: (a) diabetes mellitus, (b) depressive disorder, (c) dyslipidemia, (d) hypothyroidism, (e) ischemic heart disease, (f) hypertension, (g) chronic osteoarthropathies and (j) cancer.
The protocol received approval from the bioethics committee of the Universidad Tecnológica de Pereira in the without risk research category, according to resolution 8430/1993 of the Ministry of Health of Colombia according to the Declaration of Helsinki, and principles of beneficence, nonmaleficence and patient confidentiality were respected.
For data analysis, the statistical package SPSS Statistics, version 23.0 (IBM, EE. UU.) for Windows was used. Student’s t-test or analysis of variance (ANOVA) was used for the comparison of quantitative variables, and the chi-square test was used for categorical variables. Logistic regression models were used where the dependent variable was change of therapy (yes/no) and use of comedications (yes/no) and the independent variables were those that were statistically associated in the bivariate analyses. A statistical significance level of p < 0.05 was used.
Results
A total of 289 patients who underwent treatment with somatostatin analogues were identified during the 56 monitoring months. The average age of the studied population was 56.6 ± 14.0 years (range: 12–89 years), and there was female predominance, with 172 (59.5%) cases. Continuous prescription of two drugs was found in 220 subjects (76.1% of cases), and in those where breaks in dispensation occurred and interruption lasted a median of 7 months, with a mode of 3 months (range: 2–35 months).
The most prescribed somatostatin analogue was octreotide LAR (56.1%) followed by lanreotide Autogel (43.9%). The prescription patterns of the somatostatin analogues used as well as time of usage (adherence to continuous prescription) of each drug are summarized in Table 1.
Prescription patterns and time of use of long-acting somatostatin analogues in Colombia (2011–2015).

nDDD: relationship between mean dose and daily defined dose; SD: standard deviation; LAR: long-acting release.
It is interesting to observe that only 4.5% of patients changed from one molecule to another; 1.4% changed from octreotide LAR to lanreotide Autogel, and 3.1% changed from lanreotide Autogel to octreotide LAR. When determining variables that could be related to the change in therapy, a statistically significant association was found with being a diabetic treated with insulin (odds ratio (OR): 4.27; 95% confidence interval (CI): 1.23–14.84; p = 0.014). Of the group of patients using octreotide LAR, 19 (11.7%) modified the dose during the monitoring period, with scaling from 20 to 30 mg being the most common (n = 12; 7.4%), followed by 30–40 mg (n = 4; 2.6%), but there were three cases (1.7%) with reduction from 30 to 20 mg, with an mean time until dosage change of 13.4 ± 12.9 months. Regarding lanreotide Autogel users, a larger proportion of dosage changes (n = 27; 21.2%) was observed, with a change from 90 to 120 mg being most common (n = 15; 11.8%), followed by 60–90 mg and 60–120 mg, both with the same frequency (n = 5; 3.9%). However, there were also cases of reductions from 90 to 60 mg (n = 2; 1.6%), with an mean time until change of 15.5 ± 10.7 months.
The most commonly identified diagnoses in these patients were acromegaly, with 151 (52.2%) cases, followed by neuroendocrine tumors in 46 subjects (15.9%). The incidence rates of each diagnosis and the number of patients treated with each molecule can be seen in Table 2. In 93 (31.8%) cases, it was not possible to identify the diagnosis. It is interesting to observe the difference in the mean ages between patients with acromegaly (54.6 ± 12.9 years) and neuroendocrine tumors (64.0 ± 14.0 years). The most used somatostatin analogue in acromegaly was lanreotide Autogel (57.6% of cases), while the most used somatostatin analogue in neuroendocrine tumors was octreotide LAR (78.2% of cases).
Distribution of cases and incidence rates of acromegaly and neuroendocrine tumors in patients from a population database of Colombia, years 2011–2015.
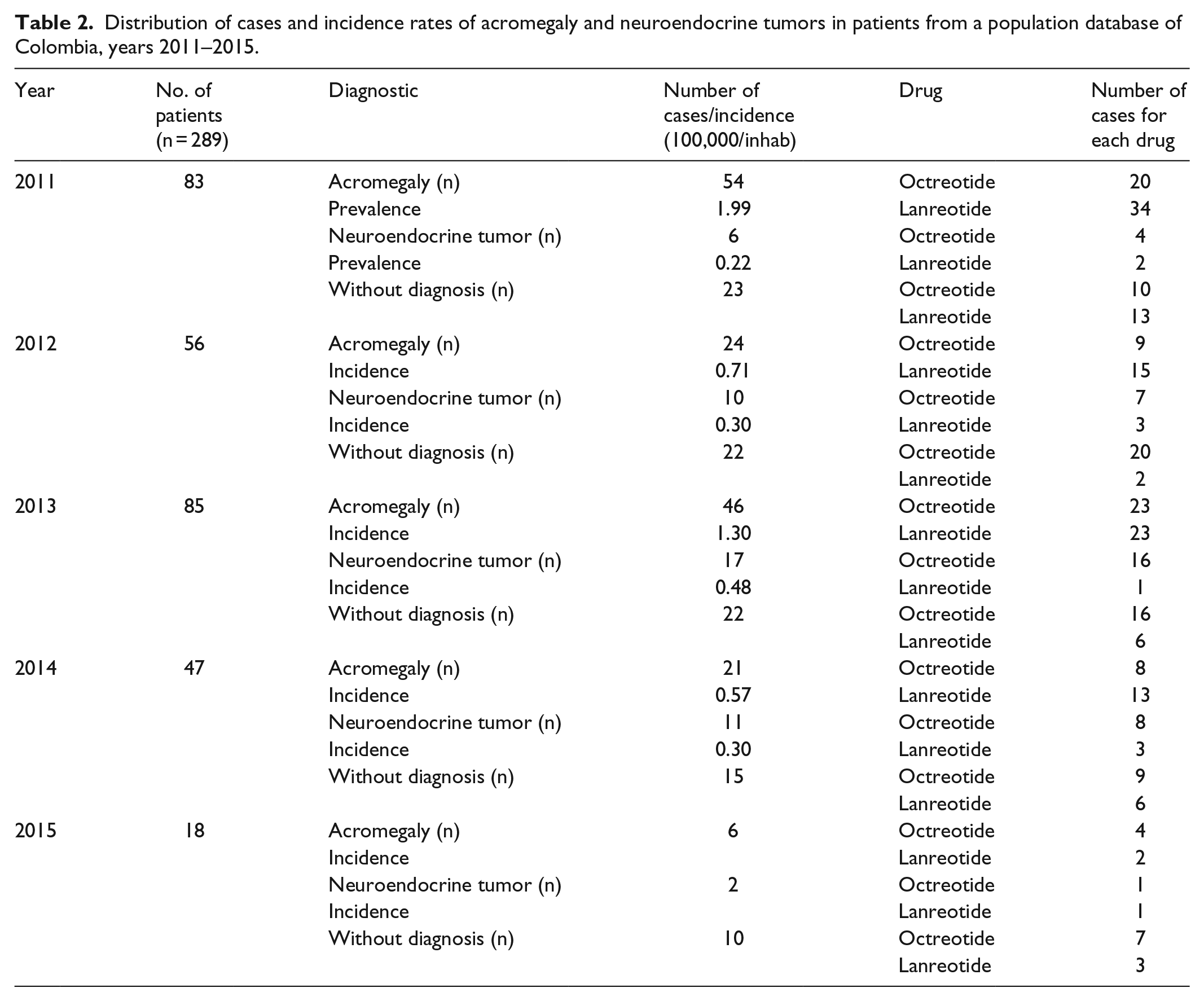
Differences were also found in the mean DDD of octreotide LAR used in patients with a diagnosis of acromegaly (DDD = 1.13 ± 0.218) versus those with neuroendocrine tumors (DDD = 1.27 ± 0.212; p = 0.0019). Regarding the lanreotide Autogel doses used, no differences were found between the groups of pathologies (p = 0.77).
Comedications
It was identified that 67.1% of patients concomitantly received one or several medications for the management of other diseases, with the most frequently prescribed medications being for the treatment of hypertension (39.4% of cases), for example, angiotensin II receptor antagonists and calcium channel blockers (21.5%), followed by antidepressants (27.3%) and hypolipemiants (25.3%) and for the management of other endocrine pathologies, such as hypothyroidism, for example, levothyroxine (23.5%) or cabergoline (n = 41; 14.1%) was mainly used in patients treated with lanreotide Autogel (65.9% of patients with dopaminergic agonist). Only three of the patients who received cabergoline had a ceiling dose of octreotide LAR of 40 mg, while 20 subjects used the maximum dose of 120 mg lanreotide Autogel. Interestingly, no patients with neuroendocrine tumors were found to be concomitantly receiving everolimus.
In the bivariate analysis that evaluated as a dependent variable whether or not patients were receiving any comedication, it was found that being a man (OR: 0.57; 95% CI: 0.35–0.94; p = 0.029) and belonging to the age group between 45 and 65 years (OR: 0.44; 95% CI: 0.21–0.90; p = 0.024) were associated with a significantly lower risk of receiving other medications. No association was found with variables that elevated the likelihood of receiving comedications for comorbidities.
Differences by cities
The patients in this study were distributed in 22 different Colombian cities, and the majority were concentrated in Bogotá (39.8% of subjects). Table 3 shows the different variables related to the use of somatostatin analogues, comedications, average DDD used, use percentage of each analogue and diagnosis discriminated by each of the seven most represented cities, including 80% of the evaluated population and also by nationwide consolidated percentages.
Comparison of demographic variables, concomitant medications, prescription and diagnostic indicators from seven Colombian cities in patients using long-acting somatostatin analogues, in Colombia (2011–2015).

ARB-II: angiotensin receptor blockers-II; iACE: inhibitors angiotensin converting enzyme; DDD: daily defined dose; LAR: long-acting release.
Discussion
In this study, it was possible to identify the prescription patterns of long-acting somatostatin analogues for the management of acromegaly and neuroendocrine tumors between the years 2011 and 2015 in 22 Colombian cities, providing valuable information on the identification of socio-demographic profiles and the use of these drugs in poorly studied diseases. In addition, it provides data that can be used to create health system strategies for the proper and timely care of these pathologies.
The proportion of women with acromegaly who underwent treatment with somatostatin analogues was higher, as previously described by epidemiological studies.16–18 The age of patients who underwent treatment for acromegaly had a mean close to 56 years, which is within the range described for this disease; however, regarding other studies that evaluate age at the time of diagnosis, this is common in subjects in their fifth decade,1,2,5 which is evident in that this studied cohort corresponds to patients who have been undergoing treatment for some time or had a delayed diagnosis.
The age of patients with a diagnosis of neuroendocrine tumors that required management with somatostatin analogues was higher than in patients with acromegaly, which was expected, given the differences in presentation and epidemiology of both diseases. These neuroendocrine tumors are present in adults older than 60 years, especially in the case of carcinoid tumors.19,20
In general, the two somatostatin analogues were used in similar doses to those defined by WHO; however, there were significant differences between the DDD of octreotide LAR used for acromegaly and neuroendocrine tumors, with the latter being greater. These findings agree with previous reports in the literature.7,19,21 Octreotide LAR can be used in higher doses (up to 60 mg/month) because of the scaling need for adequate clinical control of tumors, compared to acromegaly where the usual maximum doses vary between 30 and 40 mg/month.1,4,7,21–23 Unlike this behavior, lanreotide Autogel is at the forefront of frequency of use for acromegaly, although with little difference, which is possibly explained by usage preferences on the part of the prescribing doctors due to no clear recommendation for one of the analogues over the other in this indication. 22 However, the behavior differs from that reported in other countries, such as the United States, where octreotide LAR is preferred.10,16
The change between molecules showed a low proportion, an expected phenomenon because clinical practice guidelines recommend increasing the dose or adding other medications that can act as adjuvants (cabergoline or pegvisomant, which is not available in Colombia) before rotation between somatostatin analogues for the treatment of acromegaly.4,22,23 Despite the low frequency of change, it is useful to observe how patients with diabetes mellitus on insulin treatment present a greater risk of changing from one drug to another (OR: 4.27; p = 0.014), which is possibly related to the difficult glycemic control of those patients with acromegaly and diabetes mellitus, which can affect the management of GH levels and may be associated with drug intolerance or therapeutic failure, but there are no specific publications that explain the reasons for the change associated with a possible therapeutic failure influenced by some other metabolic disease. This hyperglycemia has been previously reported as a potential consequence in patients with acromegaly or patients treated with octreotide LAR and lanreotide Autogel.24,25 It could also be explained by pharmacokinetic differences between the two molecules that explain different outcomes among patients.
Both in patients with acromegaly and those with neuroendocrine tumors, a considerable proportion of comorbidities were found that are commonly described,26,27 especially hypertension, a finding that is higher than that found in a cohort of subjects with acromegaly in the United States (21.8%), 16 but is similar to Mexico, with 37.1% of hypertensives. 18 Regarding other comorbidities of great importance for their implications in control as well as for their high influence in the mortality of patients with acromegaly, there is diabetes, found in more than 23% of cases, with a frequency higher than that of the North American study (14.2%) but considerably lower than the Mexican report (32.3%).16,18 When these pathologies are present in patients with acromegaly or neuroendocrine tumors, they have been associated with complications such as poor control of therapy with somatostatin analogues and even accelerated mortality.24,26 However, it is clear that adequate control of excess GH as well as management of hypertension, diabetes mellitus, dyslipidemia and other risk factors have been associated with better outcomes, such as return of left ventricular hypertrophy, improvement of heart function and a direct impact on mortality.25,26
The second most commonly found comorbidity, which has been poorly studied in this group, is depression. When reviewing other studies with groups of subjects with acromegaly, this comorbidity was not studied, showing the little interest or care that has been given to it. In spite of this lack of interest, an investigation conducted by Geraedts et al. 28 showed that the appropriate management of psychiatric comorbidities, such as depression or anxiety, positively impacts the quality of life of people with acromegaly.
Approximately 15% of the patients evaluated with acromegaly used cabergoline, which corresponded to more than 56% of those who received somatostatin analogues at maximum doses, most likely due to the difficulty in achieving control of the pathology.2,29,30
The differences in the behavior of the prescription of somatostatin analogues between different cities with respect to presentation of the medication, DDD and comedications used are common findings in pharmacoepidemiological studies. These differences can be explained by variability in medical care, whether by differences in prescription patterns or in clinical practice on the part of doctors, and can be influenced by different factors in continuing education and training as well as by the services and health providing institutions of each of the cities. 31
The limitations of this study include no record of a diagnosis in close to 30% of cases, which, in conjunction with the information being obtained from databases and not from the patient or clinical history, should promote the development of future studies on the use of somatostatin analogues that evaluate clinical records, effectiveness and safety of therapy. It is important to emphasize that this population has its own characteristics regarding health insurance and care, so interpretation of the results should be carried out for similar populations.
Conclusion
It can be concluded that long-acting somatostatin analogues are being used at the recommended doses, primarily in patients with a diagnosis of acromegaly and in a significant proportion of patients with neuroendocrine tumors. However, these subjects, as was expected, frequently presented comorbidities with their respective comedications, which can potentially alter control of the underlying pathologies. The need for interdisciplinary management that guarantees comprehensive treatment of all pathologies that affect the patient should therefore be considered. Additionally, it is necessary to establish channels of communication and ongoing feedback with prescribing doctors to promote the appropriate use of medications.
Footnotes
Acknowledgements
The authors thank Viviana Andrea Orozco for her role in collecting information.
Authors’ Note
J.E.M.-A. participated in the drafting, data analysis, description of results, discussion, critical revision of the article and evaluation of the final version of the manuscript. M.E.M.-D. participated in the drafting, data collection and data analysis, description of results, iscussion and critical revision of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from Comité de Bioética de la Universidad Tecnológica de Pereira, Código: CBE-SYR-162015.
Funding
This study received funding from the Universidad Tecnológica de Pereira-Audifarma S.A. and Novartis de Colombia. There was no intervention by Novartis de Colombia in any stage of processing, analyzing or publishing the data.
Informed consent
Informed consent was not sought for this study because the bioethics committee gave permissions to review the clinical records.