
Abstract
Objectives:
The telehealth project EQUI-ResHuS (in French, Les TIC pour un accès Équitable aux Ressources Humaines en Santé) aimed to contribute to more equitable access to care and support practice in remote regions in Mali. This study explored the evolution of perceptions concerning telehealth among healthcare professionals in the four district health centres that participated in the EQUI-ResHus project and identified variables influencing their perceptions of telehealth impact on recruitment and retention of health professionals.
Methods:
One year after a first survey (T1), a second data collection (T2) was carried out among healthcare professionals using a 91-item questionnaire. Questions assessing telehealth use and perceptions and perceived impact on recruitment and retention of healthcare professionals were rated on a 5-point Likert scale. A total of 10 independent variables were considered for the analyses. A Wilcoxon signed-rank test was performed to detect differences between T1 and T2, and a bivariate linear regression model for repeated measures was carried out to assess the impact of independent variables on dependent variables.
Results:
There were no noticeable changes in perceptions related to telehealth influence on recruitment and retention. Only access to information and communication technology significantly differed between T1 and T2 according the Wilcoxon rank test (p = 0.001). Perceived influence of telehealth on recruitment and retention was mostly explained by attitude towards telehealth, perceived effect on recruitment and retention and barriers to recruitment and retention.
Conclusion:
Based on our results, telehealth was perceived as having a positive influence but mostly indirect influence on healthcare professional recruitment and retention. Also, there were no major changes after 1 year of telehealth use.
Keywords
Introduction
Telehealth (TH) is an information and communication technology (ICT) application that has been recognized by the World Health Organization (WHO) as a means to meet the challenges facing health systems in developing countries. 1 This application has the potential to address diverse problems in modern healthcare by increasing the quality, accessibility, utilization, efficiency and effectiveness of healthcare, with the added advantage of cost reduction. 2
For instance, some studies have shown that TH could have a positive effect on organizational, professional and educational factors that influence the recruitment and retention of healthcare professionals in rural and remote areas.3,4 Recruitment and retention are two interlinked aspects of workforce supply. 5 However, the decision to take up practice in rural or remote areas considers different factors from those associated with the decision to relocate. 6 Moreover, the measurement of retention is most used to evaluate strategies to solve shortage of healthcare professionals in rural and remote areas.7,8
On one hand, some previous studies on the impact of TH or telemedicine on recruitment and retention of healthcare workforce conducted in developed countries have not shown a direct effect on these two aspects.9–11 On the other hand, a systematic review conducted by Gagnon et al., 12 found that 9 of 13 included studies have reported a possible positive impact of ICT on the recruitment and retention of healthcare professionals in rural and remote areas. Although the studies mentioned above on the impact of TH on recruitment and retention of healthcare professionals show promising results, little is known in the context of sub-Saharan Africa. A recent study conducted by Bagayoko et al. 13 showed that ICT can contribute to the balance of health systems in developing countries and equitable access to human resources and quality healthcare and services. However, there is very little knowledge concerning the influence of TH on healthcare professional recruitment and retention on the long term, particularly in the context of sub-Saharan Africa.
According to the WHO, 1 Mali is one of the 57 countries identified as having a severe health workforce crisis. There is a ratio of 0.27 physicians, nurses and midwives per 1000 inhabitants and an unequal distribution of healthcare professionals between urban and rural areas. 14 This inequality of access to healthcare is more seriously accentuated in the case of medical specialties, which are almost nonexistent in rural areas. For instance, in Mali, there is only one radiologist outside Bamako, the capital, and no cardiologist within the country. 15 This uneven distribution of the healthcare workforce between urban and rural areas remains worrisome despite an improvement in the availability of qualified healthcare professionals in recent years. 16 This also explains the presence of inappropriate or untrained personnel at the head of some health facilities in rural areas. 17
Mali is among the first sub-Saharan African countries that implemented ICT projects to address health system quality and efficiency. 18 Since 2000, the Geneva University Hospitals have been involved in coordinating the development of a network for e-health in Africa (the RAFT, Réseau en Afrique Francophone pour la Télémédecine). This network started in Mali and now extends to 15 French-speaking African countries and others such as Nepal and Bolivia (web pages in Geneva: http://raft.hcuge.ch/; web pages in Mali: www.certesmali.org). Its main goal is to motivate talented medical professionals in developing countries to practise in rural and remote areas where they are most needed. 19 Indeed, accessibility of Internet in these regions, access to continuing medical education (CME) and contact between colleagues via e-mail are seen as potential incentives for healthcare professionals to work in rural areas.19,20
The TH project EQUI-ResHuS (in French, Les TIC pour un accès Équitable aux Ressources Humaines en Santé) implemented in Mali in May 2011 with support from the Canadian International Development Research Centre (IDRC) aimed to demonstrate how ICT applied to the health sector could contribute to making the health system more equitable. 21 This project encompassed two main activities: task shifting of medical imaging in obstetrics and cardiology to remote locations and the provision of CME through distance learning. These activities were chosen since they constitute national priorities to address the shortage of medical specialists in rural Mali and professional isolation. 22 This project was conducted in four district health centres: Dioila, Kolokani, Djenné and Bankass. The two first sites, Dioila and Kolokani, are close to the capital and are more accessible by road, while the two others, located in the northern part of the country, are more difficult to reach by road. 21 Although these sites differ due to the size of their population, all four sites have the same needs regarding deficits in infrastructure and shortage of skilled healthcare personnel.
To carry out these activities, 10 healthcare professionals (doctors and midwives) from each participating centre were trained, for a total of 40 for the entire project. CME sessions were provided every 2 weeks and lasted between 1 and 1¼ h. TH instructors were African and foreign experts. They used the platform ‘Dudal’ and a low-speed Internet connection to provide distance CME that could be followed both in real-time and in asynchronous mode.
This longitudinal study was based on lessons learned from the EQUI-ResHuS project in Mali. The first phase of this research showed that healthcare professionals in remote areas have very positive perceptions of TH in general, and this application could represent a mechanism for recruiting and retaining these healthcare professionals in remote areas. 21 The aim of our study was to explore the evolution of perceptions related to recruitment and retention of healthcare professionals in the four district health centres in Mali that implemented TH in the context of the EQUI-ResHus project and to identify variables influencing the perceived impact of TH on recruitment and retention of healthcare professionals in this context.
Methods
Study setting and participants
All participants in this study were healthcare professionals working in the four rural health centres participating in the EQUI-ResHus project. A first assessment of their perceptions was carried out at the onset of the project (T1). 21 For data collection at T2, conducted about 1 year after T1, a self-administered questionnaire was distributed to all participants who completed the questionnaire at T1 (n = 39). The study questionnaire provided a definition of concepts such as information and communication technologies, TH and distance training and was distributed together with the consent form. Two follow-up telephone reminders were made to the manager of each health centre. Other additional information about the project was collected from the project coordinator.
Instrument
The questionnaire used in this study was the same as the one used at T1. 21 This questionnaire was developed in a study conducted in Québec, Canada 23 and adapted to the Malian context. It was inspired by the diffusion of innovations theory 24 and contains a total of 91 items. All items were measured on a 5-point Likert scale, except sociodemographic data that were open and multiple choice questions. Nine open-ended questions provided narrative data. Based on a previous validation of the instrument, it was estimated that it could be completed in 30 min. 23 Another validation of the instrument was conducted in our study before data analysis. Internal consistency of all constructs was assessed using Cronbach’s alpha.
This study received approval from the research ethics committee of Université Laval, on 30 September 2014 (approval number: 2014-191/30-09-2014) and the ‘Réseau Informatique Malien d’Information et de Communication Médicale, REIMICOM’ ethics committee, which approved the project since its implementation (Figure 1).

Description of the variables used in the analysis.
Statistical analysis
Construct validity was estimated for each data collection (T1, T2) using confirmatory factor analysis (results not shown) and Cronbach’s alpha. All items were retained to corresponding constructs if they had at least 0.30 loadings at factor analysis and 0.60 for Cronbach’s alpha. Moreover, the intraclass correlation coefficients (ICCs) were calculated for purposes of testing the reliability of measurements using a one-way model. 25 We then performed a general descriptive analysis for paired sample at T1 and T2 for categorical data and continuous data. Some constructs were dichotomized for consistency with previous study at T1. 21 We calculated difference (T1 value minus T2 value) and carried out a descriptive analysis for two outcomes (recruitment and retention) and 10 independent variables (access to ICT, ICT training, information on ICT, attitude towards ICT, perceived effects on recruitment and perceived effects on retention, barriers to recruitment and barriers to retention, use of ICT last year and ICT usage by colleagues). Afterwards, we conducted Wilcoxon signed-rank tests to detect differences between T1 and T2 for all studied outcomes and factors. Also, items measuring the independent variable, use of ICT last year, were dichotomized and divided into two sub-constructs: users of TH and beneficiaries of continuing education (CE). Finally, we carried out a bivariate linear regression model for repeated measures. We used a generalized estimating equation (GEE) to estimate the parameters of this model using an exchangeable working correlation matrix chosen using quasi-likelihood criteria. All analyses were performed using SAS software (version 9.3; SAS Institute Inc., Cary, NC, USA) and IBM SPSS Statistics (version 22.0).
Instrument validation
The construct validity of the scale was acceptable, with almost all Cronbach’s alphas above 0.70. 26 The only exceptions were for access to ICT (Cronbach’s alpha of 0.58 at T2), barriers to retention (Cronbach’s alpha of 0.62 at T1) and barriers to recruitment (Cronbach’s alpha of 0.68 at T2) (see Table 1).
Internal consistency and reliability of the constructs.

ICT: information and communication technology; SD: standard deviation.
According to DeVellis, 27 alpha values between 0.60 and 0.70 represent an acceptable value given the exploratory nature of variables. However, for access to ICT, the moderate alpha value 28 could be due to a small number of items or to characteristics of respondents, but its value at T1 was acceptable with a Cronbach’s alpha of 0.72.
On the other hand, all ICCs were above 0 except for the variable perceived effect on retention. Overall, this showed a good reliability of measurements over the two periods. 29
Results
We first present the results of the validation of the instrument and then the results of the study. The results pertaining to the first questionnaire have been presented elsewhere. 21 The study population consisted of doctors, nurses, midwives, medical assistants and other staff involved in the delivery of healthcare in the four district health centres participating in the EQUI-ResHus project. A total of 39 participants completed the questionnaire at T1 on a possibility of 45, for a response rate of 86.7%. At T2, questionnaires were distributed to the 39 participants from T1. Despite two reminders, only 16 people out of 39 completed the questionnaire, for a response rate of 41.0%. The data analysis is based on the 16 participants who completed the questionnaire at T1 and T2.
Sociodemographic characteristics and additional information
Participants’ sociodemographic characteristics are provided in Table 2. Males represented 81.3% of participants. Almost half of participants were general practitioners and others were midwives, nurses, medical assistants and other professionals. The mean age was 34.7 years (standard deviation (SD) = 4.82 years) with a minimum of 29 years and a maximum of 46 years (Table 2). Second, we noted that the number of TH users and beneficiaries of CE remained stable. However, the number of patients benefiting TH increased significantly (Table 2). As for the number of staff in the four rural centres, only one physician left during the study period for a reason unrelated to the project.
Participants’ characteristics and additional information.

Differences in independent variables between T1 and T2
The Wilcoxon signed-rank test was performed to detect the differences in healthcare professionals’ perceptions of the influence of TH on recruitment and retention between T1 and T2 (Table 3). Access to ICT had a higher average at T2 with a mean of 2.85 (SD = 0.9) (Table 1). The difference between T1 and T2 for access to ICT considering the median was −0.33. According to the Wilcoxon test, this difference was significant, with a p value of 0.001 (Table 3). Attitude towards ICT was one of the constructs with a mean value higher at T1 than at T2 (4.46 vs 4.26) (Table 1), but the difference was not significant. The mean values of the constructs perceived effects of TH on recruitment and retention at T1 and T2 were high, as was attitude towards ICT (Table 1), but their differences of median were not significant according to the Wilcoxon signed-rank test. No significant trends were found for the other constructs (Table 3).
Difference between T1 and T2.
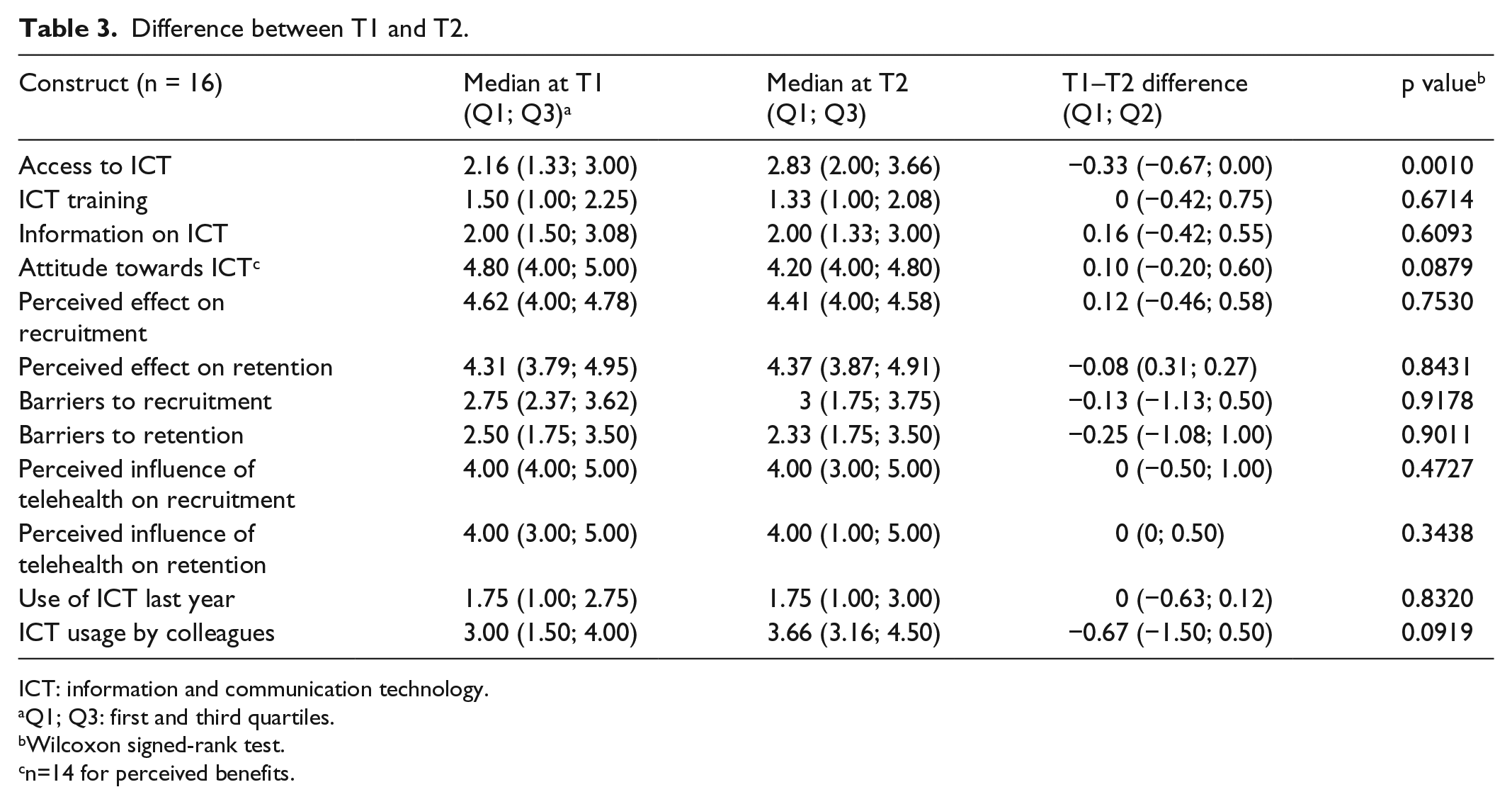
ICT: information and communication technology.
Q1; Q3: first and third quartiles.
Wilcoxon signed-rank test.
n=14 for perceived benefits.
Linear regression models for repeated measures
Finally, we carried out a linear regression model for repeated measures, using a GEE to assess the effects of the independent variables on the dependent variables at T1 and T2 (Table 4). This analysis showed that attitude towards ICT (p < .0001; p = 0.0042), perceived effect on recruitment (p = 0.0001; p = 0.041), perceived effect on retention (p < 0.0001; p = 0.0069) and barriers to retention (p = 0.0432; p = 0.0081) have a significant influence on both perceived influence of TH on recruitment and on retention of healthcare workers in rural areas at the 5% level of significance. Barriers to recruitment have an influence only on perceived influence of TH on retention (p = 0.0177). However, ICT training, information on ICT as well as the use of TH and the fact to benefit from CE have no significant influence on recruitment and retention.
Bivariate GEE linear regression models for repeated measures.

ICT: information and communication technology; GEE: generalized estimating equation.
Discussion
This longitudinal study made it possible to explore the evolution of healthcare professionals’ perceptions regarding the influence of TH on recruitment and retention in the context of the EQUI-ResHuS project conducted in four rural centres in Mali and to identify which TH-related factors could impact recruitment and retention.
According to the diffusion of innovations theory, 24 the acquisition of knowledge on innovation for some time could improve perceptions about the use of technology. The success of an innovation is determined by five attributes: relative advantage, compatibility with existing values and practices, simplicity and ease of use, trialability and observable results. A possible explanation is that in the context of the EQUI-ResHuS project, perceptions of healthcare professionals using TH could become more realistic after a year of utilization, while those who did not use TH saw fewer advantages to its use over time.
The results showed that access to ICT is the only variable for which the difference between T1 and T2 is significant. This finding supports results of the analysis conducted by the IDRC of Canada 30 on a telemedicine project in Indonesia that demonstrated the important role played by human resource development in the sustainable implementation of ICT-based telemedicine. 22 Access to ICT often means access to Internet for individual needs. In this context, outside the Internet connection at work, access is also reflected in the search for health information on the project platform and distance learning. A possible explanation for the increased perception of access is that some healthcare professionals also used their personal computers to connect to the Internet. Moreover, in line with this result, Mireskandari et al. 31 have shown that the familiarity of health professionals with ICT tools and TH applications is one of the factors that help to achieve development and sustainability of TH projects. Although access to ICT increased, the use of ICT has not followed. The study showed that the number of TH users has not changed between T1 and T2. This could be explained by the fact that the first TH users in each centre were physicians who received an initial training. These champions were responsible to train other healthcare professionals as planned in the project, but it was not the case. Furthermore, our results show that changes in perceptions of healthcare workers in rural areas with respect to influence of TH on recruitment and retention are not noticeable. This lack of change in the healthcare workers’ perceptions may be explained by the fact that healthcare workers trained in the use of TH had a more favourable perception of the importance of TH for recruitment or retention, as mentioned in the study by Bagayoko et al. 21 In this project, all the healthcare professionals were informed of the availability of TH in the centre, but few were trained in its use. Also, a number of respondents did not directly use the technology, so it is difficult for them to change their perceptions. It is reported that over time, perceptions were closer to the experience. This observation is in line with the diffusion of innovations model, 24 which suggests that awareness of TH alone is insufficient to change perceptions. Furthermore, Cameron et al. 32 concluded that negative perceptions are commonly associated with technical and training aspects of the technology. Thus, it seems important to provide regular training for healthcare professionals in the use of TH in order to favour project sustainability. However, some studies have shown the benefits of using this technology in rural and remote areas,33–36 and other studies support that ICTs, and particularly TH, may have positive effects on the recruitment and retention of healthcare professionals in rural and remote areas.12,37–39
The results of the linear regression model for repeated measures indicate that attitude towards ICT, perceived effects on recruitment and on retention and barriers to retention impact perceptions related to TH influence on recruitment and retention. These variables include several factors that can be grouped into different categories. Attitude towards ICT encompasses factors concerning which some studies have demonstrated an influence on recruitment and retention of healthcare workers in rural and remote regions. For instance, Taylor and Lee 40 have asserted that access, availability and use of ICTs play an important role in influencing occupational therapists to continue to practise in rural areas.
On the other hand, attitudes towards ICT do not translate into increased retention, despite the strong association between perceived TH impact on healthcare professionals practice and their interest in remote practice. 37 Thus, similar to what we found in a previous study, 38 our results show that the influence of positive attitude towards ICT on retention could be indirect. According to Bhattacharya and Ramachandran, 41 basic awareness and knowledge about ICT applications could influence healthcare professionals’ perceived benefits of using ICT in their work and also their acceptance of the technology. Moreover, previous studies stated that ICT applications alone cannot solve the problem of workforce distribution.37,38
Regarding the relationship between the perceived influence and real influence, previous studies have shown that there is a strong association between the perceived influence of TH on the practice of healthcare professionals and their intent to stay or leaving rural practice.37,41
With respect to perceived effects on recruitment and retention, TH influence has been shown in previous studies. For instance, a study conducted in Québec among medical residents showed that access to CME was the most important factor influencing medical resident intention to practise in a remote region. 29 Moreover, this finding is consistent with a study by Duplantie et al. 38 which highlighted that ICTs have an indirect effect on recruitment and retention by influencing related factors such as providing a second opinion in case of doubt, diminishing the feeling of isolation, supporting decision-making and maintaining natural professional networks among physicians. On the other hand, the negative effect of barriers to recruitment and/or retention was similar to perceived TH limitations identified by a study of TH to support medical practice in rural and remote regions. 42 Among the limitations reported were the following: TH could replace a doctor on site, TH limits the possibility of getting outside training and TH means a lack of staff. Furthermore, remote physicians thought that teleconferences could prevent them from socializing with their colleagues working in urban areas. 42
This study has some limitations. First, the low response rate (41%) makes it impossible to generalize these findings to all participants in the EQUI-ResHuS project. The fact that only participants from T1 were considered for T2 limited the number of potential respondents. The small sample can also explain the lack of significant change observed in most of the variables of the model. Also, due to the limited number of participants in this project, it is not possible to infer the influence of TH on retention from data on actual retention. A qualitative study may complete data from this survey and explore reasons why healthcare professionals use TH or not in rural areas. Nonetheless, the process used in this survey may be helpful for further studies on the topic. Second, the relatively short interval between T1 and T2 measures may not allow sufficient time to observe significant trends in healthcare workers’ perceptions related to TH. Furthermore, longitudinal studies with a larger sample are needed to see how healthcare professionals’ perceptions can evolve over time.
Conclusion
This study offers a longitudinal perspective regarding the potential influence of TH on recruitment and retention that could inform TH project managers. Our results show that change in healthcare providers’ perceptions is not noticeable after 1 year. Several reasons have been identified. Access to ICT was the only variable for which the difference between T1 and T2 was significant. This result will therefore be useful to policy makers to plan training on the use of TH applications. On the other hand, our study supports the argument that attitude towards ICT, perceived effect on recruitment and on retention and barriers to retention have a significant effect on perceived influence of TH on recruitment and retention of healthcare workers in rural areas. Further studies based on these findings are needed in order to identify the longer term impact of TH on healthcare workers’ practice.
Footnotes
Acknowledgements
The authors are grateful to all healthcare professionals who participated in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
This study received approval from the research ethics committee of Université Laval, on 30 September 2014 (approval number: 2014-191/30-09-2014) and the ‘Réseau Informatique Malien d’Information et de Communication Médicale, REIMICOM’ ethics committee, which approved the project since its implementation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly supported by a grant from the Global Health Research Initiative (GHRI), a research funding partnership composed of the Canadian Institutes of Health Research, the Canadian International Development Agency (CIDA) and the International Development Research Centre (IDRC).
Informed consent
Written informed consent was obtained from all participants before the study.