
Abstract
Background:
Care of young adults with life-limiting illnesses can often be complex due to the fact that they are growing and developing within the continuing presence of their illness. There is little research conducted nationally and internationally, which has examined the life issues of young adults or taken a longitudinal approach to understand such issues over a period of time.
Aim:
To gain clear understanding of one particular and pertinent life issue—relationship transition—occurring in the context of being a young adult with a life-limiting illness and the clinical needs arising from this.
Design:
This was a triangulated, longitudinal, qualitative study involving young adults with life-limiting illnesses and their significant others, namely, family members and healthcare professionals. Semi-structured interviews were conducted with participants and analysed using thematic analysis. Clinical case note reviews were also carried out.
Setting/participants:
A total of 12 young adults (aged between 17 and 23 years) from 2 hospices and 22 nominated significant others participated in a total of 58 interviews.
Results:
Thematic analysis revealed 4 main themes and 11 subthemes. The main themes were ‘Dependence dichotomy’, ‘In it together’, ‘Biographical uncertainty’, and ‘Conserving integrity’. These themes helped to establish the nature of relationship transitions that the young adult participants from the study experienced and additionally allowed insight into their possible needs at their end of life.
Conclusion:
This study has identified the nature of relationship transitions pertinent to young adults and has highlighted associated end of life clinical needs. This study can influence further research into the transitions and end of life needs of this particular patient group receiving palliative care, while informing the lacking evidence base which exists internationally.
Keywords
Introduction
Young adults with life-limiting illnesses
There is increasing emphasis on the needs of young adults with life-limiting conditions. 1 Much of this has been due to the fact that many children are surviving longer with conditions that were previously unique to childhood. 2 However, the needs of young adults are different from younger children and adults, particularly in relation to their physical and psychological development. 3 Moreover, the care of young adults with life-limiting illnesses can be more complex because they are growing and developing within the continuing presence of their illness. The needs of these young adults are of particular concern when they leave the care of children’s services and move to adult services. 4 Adult services are particularly challenged since they are now being expected to provide services for a group that were not expected to survive to adulthood. 5 This is also the case for adult hospice services. 1 All health and other professionals need to understand the nature of issues faced by young adults with life-limiting illnesses, to help inform the provision of appropriate care and support as they reach this stage in their development. These issues often involve multiple transitions that in the context of being a young adult with a life-limiting illness make their clinical needs more complex.
Transitions
Transitions refer to situations which represent change and development,
6
may cause anxiety, but can also be exciting periods by enabling new opportunities and progression.
7
Transitions have been defined most commonly in the context of the young adult moving from child-oriented services to adult ones.
8
As such, transition can be defined as follows:
… a purposeful, planned process that addresses the medical, psychosocial and educational/vocational needs of adolescents and young adults with chronic physical and medical conditions as they move from child-centred to adult-oriented health care system.
9
However, the literature also recognises that as well as movement between services, developing from a young child into adolescence and young adulthood is recognised as a key transition point for the young person. This is underpinned by shifting emotional attachments, pursuit of autonomy, and endorsement of self-reliance. 10 There is recognition that young adults experience a variety of transitions. 8 In addition, regardless of having a life-limiting illness, young adults undergoing this transition period share the common concerns that afflict their peers in terms of aspiring for a ‘normal life’. 1 One key aspect of this transition point that is highly relevant for young adults is relationships.1,8 Relationship dynamics are likely to be changing as young adults come to enter adulthood. 10 Part of those changes involves the adaptation from the adult–child relationship between parent and child, to an adult–adult relationship, 10 and the desire for intimate relationships with partners. 8 As such, this article focuses on this aspect of transitioning and we have termed this ‘relationship transitions’ to highlight these changing dynamics. Although this term is not specifically named in the literature, it is an appropriate way to describe this aspect in the context of this article, to take into account how relationships account for a large part of young adults’ experiences during the recognised transition point that occurs at this stage of their lives.1,8
Relationship transitions need attention
In the pursuit of development, ambitions and concerns about relationships have been highlighted as a relevant issue for young adults. 1 In particular, relationship needs revolve around socialisation issues, with socialisation being recognised as a key milestone for this age group10–12 and includes increased desire for peer interaction and permanent relationships, and more time away from families. 8 In addition, young adults seek to find ways of maintaining current relationships, guard against isolation and establish independence.1,13,14 Being a young adult also denotes a complex period where reliance on parental care decreases and peer attachment increases, but at the same time, assuming full adult responsibilities is not appropriate.
The context of having a life-limiting illness
With regard to having a life-limiting illness, young adults’ experiences of transitioning to adulthood has mainly been understood in the context of them moving from children to adult services. However, when there is recognition that this should also take into account the move to adulthood, there are several issues that are noted.1,5,8,10 One such identified need is supporting the young adult in managing social opportunities, in addition to providing good coordinated health care that addresses medical deterioration and psychological distress. Although socialisation is accepted as a key milestone for young adults, 11 in the context of having a life-limiting illness, this can be challenging to achieve.11,12 For instance, young adults with cystic fibrosis in Palmer and Boisen’s 14 study found that in order to have an active social life that equated well to peers without illness, they had to input careful organisation. In addition, there were restrictions dictated by the nature of their illness, such as not being able to go to smoke-filled environments. Changing relationship dynamics are also identified as young adults begin to focus on distancing themselves from parents and focus on future intimate relationships.14,15 However, this may be compromised by parents being protective,16,17 the young adult not being listened to, 14 fewer opportunities to form social networks, 18 the young adult not believing independence can be achieved to the same levels as peers, 14 and the young adult not wanting to burden someone with their illness. 15
A report conducted by Marsh et al. 1 looked at the experiences of transitioning to adulthood for young people with life-limiting illnesses. They highlighted that such young adults aspire to make friends and live independently, but noted that the demands of care can put a strain on family relationships. Moreover, these young adults also worried about the impact that care responsibilities was having on their parents. This report also explored the perspectives of the parents of the young adults and acknowledged that the former undergo their own transition, which revolves around the challenges of watching their child grow up and seeking autonomy while also accepting the latter’s’ impending death. In addition, issues are being experienced at a time when chronic progressive conditions may be reaching a crisis. 5
The Together for Short Lives report 8 also highlights that for young adults with life-limiting illnesses, there are notable impacts on socialisation since hospitalisation and absenteeism from school compromises development of social relationship and also progression of social skills. Moreover, these young adults strive to not be defined by their illness, and instead be recognised as young people, with key priorities including achieving independence, friendships, intimate relationships, and leisure time. 8 However, there may also be aspects of the life-limiting illness that means that some aspirations such as achieving independence are unrealistic. 8 This may need handling sensitively by formal and informal carers.
Hospice services
Hospices, as with all palliative care services should endeavour to provide care that is appropriate for the recipients of care. 8 The Marie Curie Cancer Care report 5 into supporting the transition of young people with palliative care needs suggests that hospice services may need to reconfigure their services in order to provide appropriate care for young adults. Nevertheless, hospices have been criticised for not sufficiently meeting young adults’ needs. 1 Marsh et al. 1 recognise that hospices do make arrangements for social events, but concede that this is restricted to occasional gatherings and therefore do not support the normality that young adults desire.
Based on these reported issues, priorities, and concerns around the relationship aspects of transitions1,5,8 which are ultimately age-specific, 10 young adults with life-limiting illnesses can therefore be regarded as a unique palliative care group, with additional needs beyond the immediate health issues. Therefore, by highlighting the nature of relationship transitions and related end of life needs, this study seeks to recommend ways in which key providers of palliative and end of life care, such as hospices, can better support these young adults. Understanding the needs of these young adults is crucial for services to provide holistic care, catering for the psychological, physical, educational, and developmental needs of these young adults. It is important, therefore, to consider the effect of these transitions and related needs on those closely involved with them.
Our use of ‘life-limiting illness’ is based on the definition used by the UK charity Together for Short Lives:
19
… conditions are those for which there is no reasonable hope of cure and from which children or young people will die. Some of these conditions cause progressive deterioration rendering the child increasingly dependent on parents and carers.
Therefore, the young adults included in this study had illnesses that were understood to be likely to shorten their lives. The term ‘clinical needs’ refers to any need or problem identified by the patient or family member in the context of their illness and any needs that impinge the quality of their life. Within this study, ‘significant others’ denote key people that are part of the young adults’ lives, including family members and care staff. This idea draws upon Bronfenbrenner’s 20 Ecological Systems Theory, which considers hierarchical systems ranging from those proximal to the person to those most remote. This has been applied to understanding transitions in the past 21 and allows complex inter-related factors, pertaining to the young person and their environment, to be captured. Bronfenbrenner’s 20 theory is organised around three main structures which propose that all aspects and levels of a child’s environment are influential in how they grow and develop. This includes the immediate relationships and organisations, which are present in the child’s life (microsystem); the interactions between the different members of the child’s microsystem (mesosystem); the wider agencies and organisations that do not have direct contact/interactions with child, but still impact his or her life (exosystem); and finally the widest system that although remote, has a great influence over the child, for example, the economy, cultural values, and attitudes (the macrosystem). With this theory in mind, the significant others of the young adults in this study represent the microsystem since their interactions with the young adult are part of immediate relationships.
A systematic review carried out as a precursor to this study was conducted by the researchers and confirmed that there has been very little research examining the issues of young adults with a range of life-limiting illnesses. 22 Existing research has neglected young adults as a distinct group and has not acknowledged that they may have needs that are different from younger children and/or adults. The precursor review identified studies across six different countries, but found very little research that has taken a longitudinal approach by interacting with young adults over a period of time. This suggests that although there is international research interest in expanding understanding into young adults’ end of life needs, there is lack of dedicated insight into young adults’ perspectives. Thus, healthcare services across the world may not be adequately informed to deal with this patient group and their palliative care needs. This is a dire situation given that palliative care is highlighted as a critical part of all healthcare systems, 23 and that it is a global endeavour to strive for high-quality palliative care for young people. 24 The hospice and palliative care movement for younger people is expanding globally, but still requires extensive support 25 and research plays a role in informing this development.
Aims
The overall aim was to gain a clear understanding of the relationship transitions occurring in the context of being a young adult with a life-limiting illness and to identify the clinical needs arising from this. Specifically the study objectives were (1) to identify the nature of relationship transitions experienced by young adults with life-limiting illnesses, (2) to understand how these transitions inform the end of life clinical needs of young adults, and (3) to establish how palliative care providers may respond to these needs.
Methods
The study is a triangulated, longitudinal, qualitative study, taking an exploratory approach. The study adopted triangulation using data from different sources to help understand the phenomenon of interest. The two data sources used were semi-structured interviews and case note review. Data were triangulated by incorporating the case note reviews, reflective notes from interviews, and the interview transcripts into the analysis. The study can be considered exploratory since it sought to understand more about experiences 26 —specifically those of young adults and their significant others regarding relationship transitions in the context of having a life-limiting illness.
Furthermore, a longitudinal approach was used by engaging in interviews with young adults over a period of time. This was deemed appropriate to allow sensitive and personal issues to be discussed, as facilitated by an on-going relationship between researcher and participant. 27 In their study looking at the experiences of people with chronic obstructive pulmonary disease (COPD), Pinnock et al. 28 favoured a longitudinal approach to enable key insights to materialise around patients’ experiences over the period of illness, including how their perspectives changed. Similarly, we sought to understand how relationship transitions and related end of life needs changed and developed over the course of illness for our participants. In addition, we also wanted to see the effects of these on significant others. Three time points, which were approximately 2 months apart, was deemed a realistic approach to conducting a longitudinal study, bearing in mind that the young adult participants were seriously ill.
The study was carried out between April and September 2013 and involved the collection of serial data over three time points, which were approximately 2 months apart.
Sample
For the purpose of this study, ‘young adults’ were identified as those aged between 15 and 25 years, encompassing the periods of middle and late adolescence, and early adulthood. A total of 12 young adults recruited through children’s hospice services in Scotland participated in the study (9 males and 3 females). The setting was two children’s hospices which cater for young people and their families. The ages of the young adults ranged from 17 to 23 years. A total of 10 young adults participated in the first round of interviews. A further two young adults had initially consented to participate but were unable to proceed due to ill health. However, these young adults were able to take part in the second round. Therefore, the sample of young adults came to a total of 12. Figure 1 shows the primary diagnoses that the young adult participants had. Details of rare conditions are not disclosed since this might compromise anonymity. Participants came from rural locations and cities areas across a wide area of Scotland.

Life-limiting illnesses of the young adult participants.
At the first round of interviews, the young adult participants were offered the chance to nominate other potential participants, which could include family members, professional staff, volunteers, or friends. This led to 21 significant others participating (family members n = 10; professional staff n = 11), yielding a total of 58 interviews. Figure 2 provides details of how the interviews were spread across the three time points. As can be seen, there were participants who withdrew from the study at some time points: two young adults interviewed for Time Point 1 withdrew at Time Point 2; one young adult from Time Point 2 was too unwell to participate at Time Point 3; one young adult from Time Point 2 was not contactable at Time Point 3. In total, eight young adults, four family members, and four health/social care staff did serial interviews. Family member and professional staff who did not take part at Time Point 3 were not contactable and/or had moved jobs.

Details of data collection at each Time Point.
Recruitment
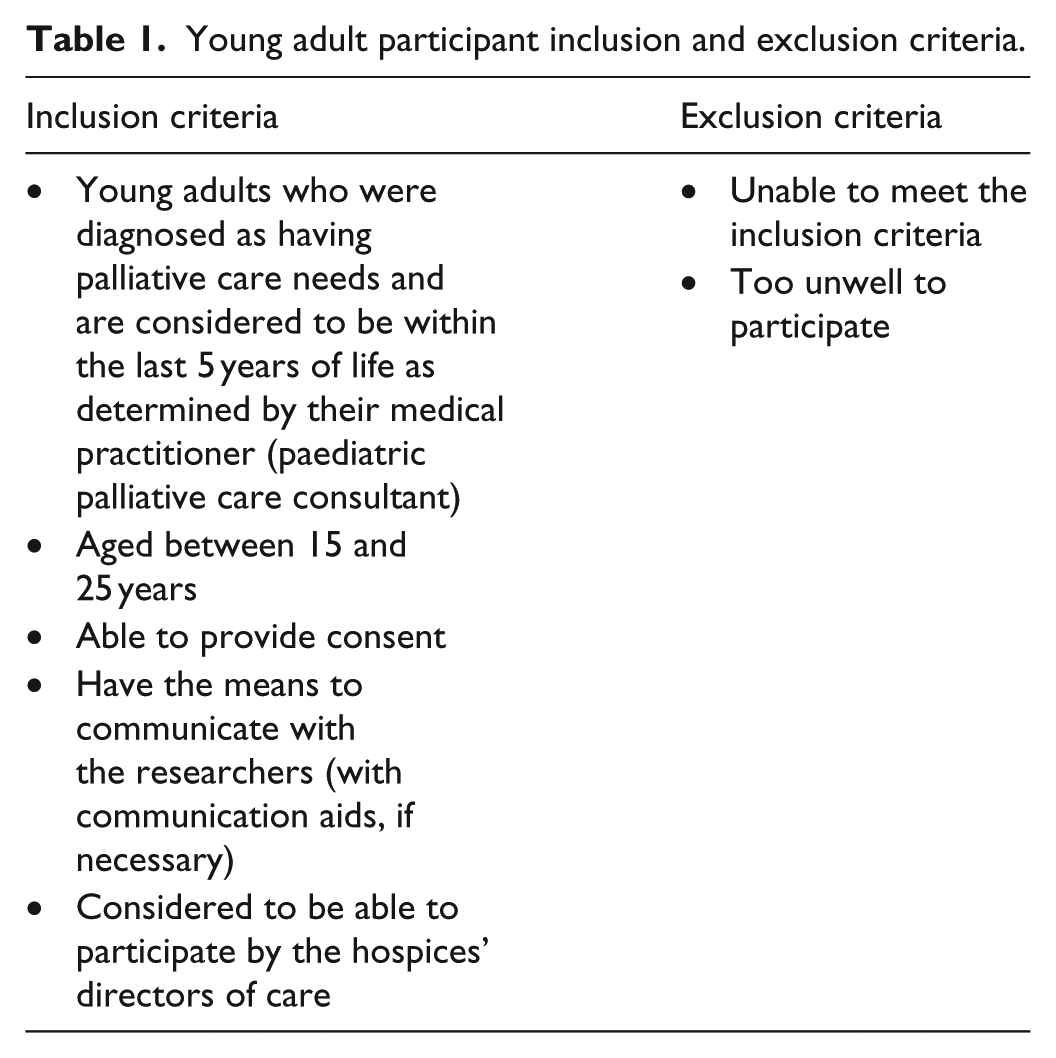
Two senior members of hospice staff approached young adults who met the study inclusion criteria (see Table 1) and gave them verbal information and study information sheets. If after a period of 24–48 h they indicated that they were willing to take part, their names were given to the researcher (subject to permission from the young adults). The researcher contacted them and gained their assent and consent. The young adult participants were invited to nominate family members and professional staff. Family members and professional staff who were approached following these nominations were given information sheets and their consent was sought before they participated.
Young adult participant inclusion and exclusion criteria.
Interview process and case review
The interviews were semi-structured and carried out at a time and place that was suitable for the participants. In the most part, this was in the participants’ home, but for some participants, this was a place of care, such as a hospice or day centre. All participants were interviewed in person, alone, with the exception of two young adults, who required communication support. For the two participants with communication difficulties, they were still interviewed in person, but participation was facilitated by additional input from parents and carers, and the use of gestures and picture cards where relevant. Pre-interview, introductions took place, along with consent processes and general familiarisation. Where permission to digitally record interviews was granted by participants, a digital recorder was used. When this type of recording was not an option due to participants not granting approval, written notes were taken instead. In this case, the interviewer was careful to ensure that as many verbatim responses were included as possible. Opdenakker 29 suggests that digital recording should only ever be an accompaniment to written notes, rather than being considered a replacement. Therefore, we do not feel that data fidelity was compromised by the lack of digital recording for some participants (based on their wishes), since we took detailed notes, which are also able to capture interview content.
Duration of initial interviews ranged from 19 to 41 min, with subsequent interviews taking a shorter length of time (ranging from 10 to 35 min). The duration of family member and professional staff interviews was much longer and took between 20 and 95 min. Interview questions were kept broad to allow participants to lead the interview and encourage them to divulge their experiences. Generally young adult participants were initially asked to tell the researcher about their lives up to that particular point. Family member participants were initially asked to describe their lives and experiences from the point that their child first became diagnosed with a life-limiting illness. Professional staff participants were initially asked about how they first became involved with the young adult. The researcher interviewing participants then picked up on issues that were disclosed, which gave some insight into transitions and further explored these areas if participants were willing to discuss them. Tables 2 and 3 provide some demographic information about family member and professional participants.
Demographic information about family members.

Demographic information about professional staff.

In addition to interviews, two senior members of staff working at the children’s hospice provided case note reviews to offer background clinical information at each stage of data collection. These reviews provided details around the clinical, social, and psychological needs and contributed to the data analysis. Insight into these diverse needs was relevant to understand both the clinical needs associated with having a life-limiting illness and the transition point young adults experience at this stage of their lives.
Ethics
The East of Scotland Research Ethics Committee granted ethical approval for this study (ref. 14/ES/0025) on 10th March 2014. One young adult advisor and two parent advisors (all with experience of young adults with life-limiting illness) reviewed all study documents and approved them prior to seeking approval from the Ethics Committee. The research team strictly adhered to all aspects of research ethics and data protection. Due attention was given to risk management of the sole researcher working in participants’ homes throughout the data collection period.
The study was overseen by a research steering group, who met regularly throughout the period of the study. This group was chaired by a clinician at a children’s hospice and comprised a specialist in children’s palliative care, senior nurses, a consultant psychologist, a palliative care researcher, the academic staff, and a young adult and parent representative.
Analysis
Qualitative interview data were recorded (with permission), transcribed, and analysed using mind mapping30,31 and a thematic analysis approach. 32 These processes were reviewed and agreed by members of the research team. Interview transcripts were looked at as a whole to enable an overall global impression of the data to be elicited. Interview transcripts were initially read as a whole to give an overall ‘global’ impression of the data. Detailed notes from each individual interview were then taken, and main points inserted on a mind map, to enable connections, commonalities, and differences to be highlighted. Items from the mind map and the more detailed notes were then able to inform the production of subthemes, which were grouped into main themes, according to the evident connections. Verbatim extracts from the transcripts were matched to each subtheme to verify the links between the interview data and the themes and subthemes. This process was reviewed and agreed by three members of the research team.
A mind map was then developed, which involved slotting notes and ideas from each interview and case note review on the chart/mindmap and charting connections and commonalities. Mind mapping is a procedure that can be used in qualitative research to help researchers to take an unbiased approach towards analysing the data. 31 A central idea is put at the centre of the page and then ideas branch off from this, with associations made through linking connected ideas with colour codes and words. 30
In this study, the mind map and content helped to develop the subthemes and themes. Subthemes were studied and categorised into logical main themes, based on evident connections. Eventually verbatim extracts from the interview transcripts and insights drawn from the case note reviews were linked to relevant subthemes to ensure that all subthemes were derived from evidence in the interview data. This helped verify links between the data, themes, and subthemes. We provide a pictorial of one stage of mind mapping in Appendix 1.
Findings and discussion
From the data analysis, a total of 11 subthemes were identified and grouped into 4 main themes: ‘Dependence dichotomy’, ‘In it together’, ‘Biographical uncertainty’, and ‘Conserving integrity’. These themes help provide insight into the nature of relationship transitions experienced by the young adult participants (Table 4) and draw attention to the clinical needs they face in the context of palliative and end of life care.
Main themes, subthemes, and life transitions.

All four main themes and related subthemes enable insight into the relationship transitions experienced by young adults with life-limiting illnesses.
‘Dependence dichotomy’
This theme encapsulated the way in which young adults experienced unwanted dependency upon others due to their illnesses, yet equally attempted to assert independence. This was challenging for the young adult participants and their significant others, as present relationships came under strain, while new ones were being pursued. Three related subthemes are presented below.
Autonomy and power dynamics
The fact that young adults were reaching or had reached adulthood created interesting power dynamics, especially with care staff, as the former attempted to assert their independence, within the limitations of their physical ability. However, parents and care staff sometimes considered these young adults to be ill-prepared emotionally and socially for the adult world:
Self and sense of identity is delayed in some young people with disabilities because of the parents’ need to nurture and protect. (Social Worker, SW for YA 6; Time Point 1)
This highlights the unique position of these young adults as entering a period in their life where they wish to express a new identity. This is challenging, first, because they may be restricted by their palliative care needs and, second, because parents may feel enhanced obligation to protect them. Parents’ reservations were often due to the young adults’ prolonged childhoods. The nature of life-limiting illness often means that these young adults do not experience adolescent ‘norms’, such as gradual separation from parents, 33 which may mean that they have prolonged childhoods.
Mutual respect
Mutual respect was often challenging for all involved. Parents and care staff struggled to accept the young adult as someone who could make their own decisions:
(Young adult) hasn’t had that life experience to understand you know, well what’s acceptable to say to a (member of the opposite sex). (Care manager, CM YA 9; Time Point 2)
This led to frustration for young adults and some responded disrespectfully, as captured in a revelation by one young adult:
(Carer) drove me to frustration, and it got to the point where I actually hit him with my chair. (Young adult, YA 2; Time Point 2)
Care staff may have perceived young adults to be inexperienced in certain social interactions, based on their age and/or prolonged childhood. This might have made care staff cautious about encouraging independent decision-making. In addition, family members may struggle to accept and support young adults’ goals around engaging in independent decision-making. Some young adults’ lack of respect for care staff may have been due to lack of experience or in frustration (as highlighted above).
Protection
Some parents and professionals reported that due to the protected and prolonged childhoods, young adults were sometimes naïve about the risks that they might be exposing themselves to (e.g. online) and required guidance from family/professionals:
(Young adult) still very childlike because (young adult) been wrapped in cotton wool and not been out there exposed to life’s elements. (Parent (mother), YA 4; Time Point 1)
This suggests that being a young adult with a life-limiting illness leads to possible overprotection by parents, which could leave the former ill-prepared for potential dangers. Entering adulthood does not necessarily equate to full responsibility because in the context of having a life-limiting illness, the young adult has, up to this point, been protected from many life elements. For these young adults, life elements included dangers associated with the pursuit of new relationships, possibly online:
(Young adult) is still vulnerable with regard to giving out personal details, especially on-line (Social Worker, SW YA 7; Time Point 3)
Thus, professionals have a role to play in protecting the young adult from danger in their endeavours, when the young adult is under their care, particularly if the latter is at risk of divulging personal information that could put them in danger.
‘Dependence dichotomy’ highlights the complexities of young adults seeking autonomy, which then impacted the relationship with family members. The young adults in this study have a complex status, in which they sit between childhood and adulthood. They may resent the dependence that they have on others since they seek to assert themselves in adulthood. The literature confirms that this period of life is reported to involve the gradual separation from parents and the development of independence. 33 However, young adults with life-limiting illnesses may not be able to fully achieve autonomy, due to vulnerabilities caused by illness and the possible prolonged childhoods that they have undergone, resulting from having a life-limiting illness. 34 Healthcare professionals, such as hospice staff, can assist young adults by accepting (and helping families to accept) that pursuit of autonomy is often a developmental norm for people within this age group. 33 Therefore, despite the presence of a life-limiting illness, this endeavour to be more autonomous and independent still remains. Therefore, changing relationship dynamics between parents and the young adults are pertinent.
Healthcare professionals could consider that some family members may struggle to accept this, particularly if they are overprotective of their children. Making time to discuss this issue with family members could open up the opportunity for concerns to be disclosed, and strategies to be collaboratively developed, which support the young adult’s autonomy, and that are of mutual benefit to both the young adult and their family members. Long-term illnesses can exert a centripetal pull on family systems, with this inward focus possibly being contrary to some family members’ needs. 35 Such illnesses may require a period of adjustment and socialisation as the person affected and their family adapt to illness onset and/or progression. Healthcare professionals may facilitate the necessary adjustments by giving time for discussion and support to all concern. In addition, healthcare staff themselves may not be considering these developmental ‘norms’ of young adults, as reflected in earlier quotes where staff highlight the vulnerabilities and child-like qualities of the latter. This may mean training sessions for staff working with young adults should possibly incorporate some content on the relevant development goals of young adults, should explore ways in which young adults can be supported in pursuing such goals, and should cover how such support can take into account the vulnerabilities that they perceive such young adults to have.
Support can be given to asserting independence where reasonable, but negotiations may be required if particular endeavours would be further damaging to the young adult’s health and safety. For example, hospices could strive to accommodate Internet facilities to facilitate online social networking for young adults. This sort of social activity may be more amenable to a range of life-limiting illnesses than a day trip out, since the young adults could potentially engage in this from their beds. Negotiation could include agreement between the young adult and hospice staff that such use of social networking sites could be monitored by staff, with Internet safety settings being activated. However, this would be subject to adequate funds to facilitate this and staff time. In addition, monitoring may be perceived to be impinging on the young adult’s autonomy. Nevertheless, if such facilities could be accommodated, it may help young adults who have not been exposed to particular life elements, to learn more about appropriate social etiquette by giving them a way of increasing their interactions. Moreover, it may be manageable way of helping them to seek out more independence in creating new social networks.
‘In it together’
This particular theme highlighted the ways in which young adults’ bonds with family members developed and modified during the course of illness. Unity was a strong element in participants’ accounts, but tensions and emotional challenges were also present. Two related subthemes were revealed.
Family bonds
Close family bonds were often in place and a sense of putting on a united front was present, as reflected in the following quote:
We were in it together, so we all felt the same way. (Young adult, YA 1; Time Point 3)
This implies that the illness is a shared experience and so this would need to be considered by palliative care professionals.
Family dynamics
There were interesting insights from young adults who described how the nature of their relationships with family members changed during the course of illness:
I found that the relationship was becoming, like it was almost like I was seeing my mum as a carer … you want your mum to be your mum, you don’t want her to be your carer all the time. (Young adult, YA 2; Time Point 2)
This highlighted that the young adult desired their mother to revert to a parental role as opposed to a carer’s one. The change in the nature of this relationship appears to be the result of the illness trajectory. Thus, healthcare professionals may need to step in to provide more comprehensive care, in order to relieve families of caring duties and allow young adults to salvage the child–parent bond that they desire. This might include, for example, hospice staff finding out what main care duties the parents carry out, and offering to do these instead. This might then allow parents and the young adults to return to and focus on the preferred dynamics of the relationship, even for a temporary period of time. This could be achieved by offering extended respite breaks for the young adults, if resources allowed.
Generally, ‘In it together’ highlighted strongly that family members are integral to young adults’ relationships, and therefore the illness trajectory has implication for the whole family unit. This has been recognised in previous work, suggesting that as part of clinical needs, young adults require services and professionals to attend to the wellbeing of the whole family unit. 1 This could be achieved by identifying significant others of young adults and enabling all to express their worries and concerns. Kehl 36 advises that in the context of hospice services, staff can support families through listening, engendering trust, and providing preparatory information.
‘Biographical uncertainty’
Illness onset and the subsequent trajectory had a notable impact on both young adults and families. Like ‘In it together’, the theme of ‘Biographical uncertainty’ captured the effects of illness on the whole family unit and brought attention to the effects of diagnosis. The impact of illness was felt upon emotions and future endeavours. Three subthemes materialised.
Diagnostic shock
There were often difficulties in obtaining a diagnosis, but once this was received, it frequently resulted in a strong shock reaction for everybody concerned:
We were told then that it was terminal and that they didn’t give (young adult) any much more hope than 18 years … So obviously it, it sort of blew us, we really, we all fell to pieces. (Parent (mother), YA 12; Time Point 3)
The effects of diagnosis and prognosis, therefore, have implications for the family as well as the young adult. Further insight was provided by the next subtheme.
Grief/living loss
Following diagnosis, family members displayed grief reactions:
I was grief-stricken, whatever, I was too tired, it was like my crap life, that’s it, it’s like, you know, there was times when I just didn’t want to be here. (Parent (mother), YA 2; Time Point 2)
Clearly the emergence of grief post-diagnosis was difficult to deal with for parents as outlined above. This may have implications for their relationship with the young adult.
Future purpose
The impact of health and physical problems upon young adults was evident in planning endeavours for the future. One parent listed the various prospects that had now been marred by the life-limiting illness:
When they get to this age there’s nothing for them … there’s nothing, there’s no job prospects, there’s no future prospects, there’s no, like marriage, there’s none, there’s none of that in front of them. (Parent (mother), YA 12; Time Point 3)
This subtheme draws attention to the uncertain future that arises, including settling down in future relationships. Some of the young adults in this study had refocused goals and ambitions, in light of their illness, and for one young adult this involved part-time voluntary work:
It’s been really nice to do that (volunteering), I’ve been really enjoying it … it’s helped me build my confidence a little bit. (Young adult, YA 1; Time Point 3)
Such endeavours may be viable in the context of living with certain life-limiting illnesses. However, renewing goals, and the element of sacrifice that accompanies halting former ambitions, may be difficult for the young adult and their family. This may be something that healthcare professionals should be aware of and consider how such sacrifices may affect the young adult mentally and emotionally. This is recognised by Craig and Lidstone
37
who claim that transitioning from child to autonomous adult is restricted in the context of ill health and render them back to being a dependent child. Moreover, these authors highlight that
… the psychological perspectives on which adulthood is established are very different to those of their healthy peers. (p. 98)
Craig and Lidstone 37 recommend that supporting the typical age-appropriate goals of these young adults necessitates professionals to be organised, flexible, and responsive. Moreover, there should be an awareness of the difficulties already inherent in healthy adolescents and an understanding of how a life-limiting illness can exacerbate and complicate these. 37 Care requires preparing the young adult for what they may not be able to achieve, while also nurturing their individuality and planning for the future. 37
‘Biographical uncertainty’ revealed much about the implications of the illness on present relationships and the potential for future ones. Diagnosis produced varied reactions for young adults and family members, including uncertainty, guilt, and grief. Losses resulting from illness, even without death, can affect the whole family, with a need to ‘grieve for the loss of the pre-illness family identity’ before moving forward in a more certain manner. 35 This theme links with Bury’s 38 notion of chronic illness causing ‘biographical disruption’, where serious illness disrupts the life course. According to Bury’s 38 sociological standpoint, chronic illness transforms distant events such as pain, suffering, and death, into closer possibilities, which destabilises the individual’s everyday structures. Our theme of ‘Biographical uncertainty’ also accommodates this idea of disruption, but focuses more specifically on the uncertainties brought about by life-limiting illnesses for not only the individual with the illness but also their family and friends. This is reflected strongly in the subtheme of grief/living loss, which captures a situation where parents are grieving for their child, when the latter is still alive. This idea of living loss is recognised in the literature 39 as an effect of the uncertainty of illness. The young adult’s life is still unfolding, but in a terrain of uncertainty, that makes it difficult for those close to them to deal with. This manifests as grief, as a sense of loss is experienced.
Therefore, supporting families through grief and guilt reactions is important, particularly since the ramifications on members such as parents may impinge on their relationship with the young adults. Although it would be recommended that staff extend their care and attention to family members as well as the young adult, given possibly limited resources, another option would be for staff to offer signposting to other services, such as counselling. These other services may be better trained and equipped to attend to family needs, such as the experience of grief. 40 This would require healthcare staff to be up to date with the range of services available in the area.
‘Conserving integrity’
The final main theme revealed young adults’ and their significant others’ efforts to allow personal development to take place and thus conserve integrity in the process. Such development was enabled by supporting social, personal and structural elements within the young adults’ lives, in the context of them living with the life-limiting illness. As a result of having had a life-limiting illness from an early age, some young adults were more at ease with adults and care staff than peers. However, care staff and parents seemed to make significant efforts to preserve the social integrity of the young adults in their care, by encouraging social activities.
Moving on
Personal development in the pursuit of ‘Conserving integrity’ often involved the desire for a close personal relationship:
I’m just like hoping to meet someone, like someone, a (partner) … and start my own family … well, while I’m able to anyway. (Young adult, YA 6; Time Point 1)
Important to note is that life aspirations are not restricted by the life-limiting illness. The young adults’ significant others wanted to support this and play a part in enabling them to fulfil wishes, but realistically. This gave rise to some disagreements about the future:
(Young adult) was looking to move into an independent-living flat with (young adult’s partner), and, do you know, I was so against it. (Parent (mother), YA 4; Time Point 2)
Parents may be reticent about their children developing personal relationships regardless of illness presence. However, in the context of the young adult having a life-limiting illness, this reticence may be enhanced because of the young adult’s often prolonged childhood and possibly increased vulnerability. This reveals that young adults construct ambitions regardless of their life-limiting illness, potentially leading to unrealistic endeavours. This may be the result of not completely understanding their illness and therefore are unable to ground their ambitions realistically. Craig and Lidstone 37 suggest that young adults should be supported by staff to take more of role in their own healthcare decisions, which might enhance understanding. This could lead to the young adult accepting what might not be viable to achieve while also enabling them to construct realistic goals.
Communication
Communication was an important medium through which young adults were able to preserve their links with their peers and support their quest for social integrity:
We’re just happy (young adult’s got the computer and the Internet so (young adult) can communicate with other people, bar looking at us 24/7! (Parent (father), YA 1; Time Point 3)
Communication strategies are likely to take varied forms for young adults with life-limiting illness since many young adults are technologically oriented. 41 Having a life-limiting illness does not alter this preference and allows the young adult to extend their social network through their preferred medium.
Two young adults in the study had very limited verbal capacity and used communication aids to express themselves. However, this was often augmented by the knowledge of those who knew them well, and it was sometimes difficult for other care staff who knew them less well to interpret their needs. Being receptive to varied communication needs is crucial for services since it helps to facilitate the maintenance of social life and better care. Liaising with those who know the young adult best is likely to be useful, particularly in highlighting preferred communication methods.
Sanctuary and support
Time spent in hospices provided young adults with further opportunities to interact with peers, while also allowing family members to have respite. Therefore, hospices became a sanctuary and support system that facilitated social opportunities and helped conserve young adults’ integrity. The support gained from staff and peers had positive outcomes for not only the young adult but also the whole family:
(Hospice) was one of the best things that’s ever happened … definitely, em, that was a lifesaver, that definitely saved our lives. (Parent (mother), YA 12; Time Point 3)
‘Conserving integrity’ was an important endeavour for young adults and revolved around the pursuit of ‘normality’ and structure in spite of the chaos, restrictions, and disruption that life-limiting illnesses can bring about. Levine 13 postulates that human beings make necessary adaptations to preserve structural, personal, and social integrity. This may be down to the person’s need to feel in control over their environment despite the impact of an altered situation, which enables them to be empowered and better adaptation. 39 In this study, this manifested in the young person seeking social opportunities and leisure activities.
‘Conserving integrity’ also appeared to be the motivator for family members and professionals in their support of young adults’ personal development. The study found that young adults were more often at ease with adults and care staff than peers. This puts care staff in an ideal position to encourage young adults pursue other social interactions, such as with peers, which may help to conserve social integrity and further personal development. This might include care staff encouraging, facilitating and monitoring social meetings online, or organising social outings and/or activities within hospice facilities. However, this would be subject to available resources, willingness from the young adult to participate, and illness permitting. Care staff may also have a role to play in providing reassurance to parents who are reticent to their children pursuing new relationships. The reassurance that any social pursuits would be overseen/monitored by care staff while the young adult is under their care may enable parents to feel more comfortable with the situation.
Having a life-limiting illness can lead to routines that disrupt the crucial experiences required to attain ideal developmental goals, resulting in social isolation and inability to function in groups beyond the family.33,34 Communication with others was a key mechanism for young adults in this study, as they maintained current relationships and sought ways to interact with peers. It took varied forms since many of them had very limited face-to-face contact with their peers. Means of communication were often social media and online gaming with peers. This seemed to preserve their links with others of a similar age and with similar interests. Therefore, as mentioned before, if resources allow, healthcare staff can facilitate appropriate opportunities for such young adults to expand their networks beyond the family. This is supported by findings which suggest that the pursuit of social activities has been recognised as an important aspect of maintaining quality of life.42,43
Young adults and significant others
This study aimed to gain a clear understanding of the life transitions of young adults with life-limiting illnesses as they move to adulthood. The life issues identified by the young adults, their family members, and nominated professional participants are related to four main themes: ‘Dependence dichotomy’, ‘In it together’, ‘Biographical uncertainty’, and ‘Conserving integrity’. Together, these themes, and their related subthemes, can be of assistance in understanding the global context of being a ‘young adult’ with a life-limiting illness. The life issues faced by these young adults include the challenges of independence, the effect of their situation on other family members, and the need to preserve personal and social integrity, within an uncertain biographical future. Such uncertainty impacted the young adults’ educational and life transitions, including their aspirations for the future, which were often unclear and without focus.
The impact of the young adult’s life transitions and choices on their family members and professionals was significant in that family were often limited in their own way in terms of employment, social life and financial situation, as well as professionals also living with emotional burden. There was also an unwillingness to ‘let go’ from some parents and to acknowledge the young adults’ evolving identity due to their care focus over several years. Sometimes this was expressed as the young adult being ‘child like’, naïve, or not ready to be independent. This came not only from parents and professionals but also from some of the young adults who seemed to be, on one hand, ready to explore their independence and, on the other hand, not sure they were ready.
Bronfenbrenner’s 20 Ecological Systems Theory provides a framework for understanding relationship dynamics and personal development. The theory postulates that influences on the immediate microsystem of the young adult (i.e. their personal and physical development and functioning) will impact the Mesosystem (family, education) and vice versa. In terms of the wider societal community, or Exosystem, there are impacts in terms of how the young adult is able to engage with their community and vice versa. For many of the young adults in this study, this engagement was sometimes reduced through choice. For others, their health condition had resulted in communication difficulties, making it more difficult for them to engage fully. In some situations, such as periods of when young adults are within hospice facilities, it is appropriate and ideal for healthcare professionals to facilitate young adults’ engagement within society. Given the challenges of this responsibility, this article has offered some initial guidance that might be feasible. This has revolved around areas of training, the use of online networking, and providing time and support for family members.
This study highlights that healthcare professionals can effectively address pertinent end of life needs of young adults with life-limiting illnesses by taking into account current key relationships that exist for the young adult, being receptive and responsive to the changing dynamics that are likely to occur with these relationships, being aware of the common developmental goals associated with this age-group, safely enabling young adults’ autonomy as they may seek new relationships, constant liaising with family members, providing information and guidance to young adults and families relating to their illness and viable prospects, and facilitating appropriate opportunities for communication and social interaction that are tailored to individual needs.
This study may influence further research around understanding relationship issues that are related to young adults’ transitions, and how these inform clinical needs. The recommendations offered here, for example, the facilitation of online social networking in hospice facilities, could be tested within a well-designed research study, to see whether such interventions improve the experiences of young adults with life-limiting illnesses.
Limitations
A few of the young adult participants were unable to engage fully in the study due to health problems. Nevertheless, a greater number than originally anticipated took part. Although serial interviews with young adults over three time points were carried out, this was a 12-month study with a small sample size and the findings need, therefore, to be taken in that context.
Conclusion
Young adults with life-limiting illnesses have been recognised as a specific and unique group with palliative care needs, but research has thus far neglected to take a longitudinal approach to their experiences. This study has identified and unpacked the complex relationship transitions that are pertinent to such individuals and has highlighted the associated end of life clinical needs. The article has dedicated space to suggest appropriate service responses to ensure that end of life needs are met. It is hoped that this study will influence further research into the transitions and end of life needs of young adults with life-limiting illnesses. Given the lack of worldwide research and longitudinal insights into young adults with life-limiting illnesses, while also acknowledging that excellence in palliative care for people of all ages remains a worldwide endeavour,23,24 it is expected that these findings will inform the sparse evidence base internationally also.
Footnotes
Appendix 1
Acknowledgements
The research team would like to acknowledge the significant and valuable contribution made by all the participants of the study. Sincere thanks also go to the young adult and parents who advised us on various aspects of this research. We would also like to thank Children’s Hospice Association Scotland for funding this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from The East of Scotland Research Ethics Committee granted ethical approval for this study (ref 14/ES/0025) on 10 March 2014.
Funding
This work was supported by a grant from the Children’s Hospice Association Scotland.
Informed consent
Written informed consent was obtained from all subjects before the study.