
Abstract
Objectives:
This study used validated physical performance measures to examine function, risk of adverse health outcomes, and the relationship with allocated hours of weekly caregiving assistance among older adults receiving home and community-based services through a Medicaid waiver program.
Methods:
Older adults (n = 42) completed physical performance measures including grip strength, 30-s chair rise, Timed Up and Go, and gait speed. Demographic information including age, gender, and allocated hours of weekly caregiving assistance were also collected.
Results:
A majority, 72% of females and 86% of males, had weak grip strength, 57% met criteria for fall risk based on their Timed Up and Go score, 83% had lower extremity strength impairments, and 98% were unable to ambulate more than 1.0 m/s. Frailty was prevalent in the sample with 72% of clients meeting Fried’s frailty criteria. The most significant predictors of allocated hours of weekly caregiving assistance approved for clients were race and gait speed.
Conclusion:
Based on scores on physical performance measures, clients are at risk of falls, hospitalization, and mortality, and scores indicate an urgent need to assess performance in addition to self-reported activities of daily living limitations for this population. Performance measures associated with quantifiable risk of adverse outcomes can be critical indicators for referrals and services needed to enhance the safety and improve care outcomes for homebound older adults.
Background
It is well established that the majority of older adults wish to age in place and preserve their autonomy. 1 Preservation of function in activities of daily living (ADL) will enable older adults to possess the mobility, self-care, and home management skills needed to continue to live safely in their own homes. Since increased age is associated with functional decline, 2 older adults often employ compensatory strategies or seek alternative living arrangements when the challenges of the home environment surpass their functional capabilities. One such compensatory strategy available to Medicaid-eligible older adults is home and community-based services (HCBS) financed through Medicaid waiver programs. HCBS include supportive services such as emergency response systems, adult day services, and home care aides (HCAs), who provide assistance with ADL, instrumental ADL, and home management tasks.
Home care aides are the primary supportive service provided through HCBS, and client ADL and instrumental activities of daily living (IADL) impairments are a major driver of HCBS utilization. 3 An analysis of HCBS users in Illinois found that a 1-U decline in IADL performance was associated with a 5% uptake in volume of HCA utilization. Similarly, a 1-U decline in ADL performance was associated with a 2.3% increase in volume of HCA utilization. 3 Older adults were also found to have significant numbers of self-reported ADL and IADL impairments. Many were unable to perform most or all of the components of a variety of tasks; 93% had deficiencies in meal preparation, 99% in housework, 82% in bathing, 59% in dressing, and 59% in transfers. 3
Illinois provides HCBS to older adults through its Community Care Program (CCP). The Illinois Department of Aging utilizes a Determination of Need (DON) instrument to assess CCP clients upon entry to the program and yearly thereafter. The DON assesses the functioning of older adult clients by capturing composite data on client performance using the Mini-Mental State Examination, self-reported ADL and IADL performance, and self-reported unmet ADL and IADL needs. DON scores are used to determine the allocation of weekly hours of caregiving to each individual client. Specific information on client physical performance beyond self-reported ADL and IADL functioning is not obtained.
While ADL capacity is an important marker of overall functioning, self-reported ADL performance does not capture information on gait speed, strength, or balance. These performance constructs strongly contribute to the capacity to perform ADL and IADL and also have known associations with risks for adverse outcomes including falls, hospitalizations, and mortality.4–6 For older HCBS clients, specific information on physical performance that has established associations with health outcomes could enable agencies to improve care by proactively intervening with referrals to needed services external to the HCBS program or modification of interventions to address specific areas of physical impairment.
The primary objective of this study was to examine levels of risk of adverse health outcomes, given scores on physical performance measures that are known predictors of adverse health outcomes among older adult HCBS clients in Illinois who volunteered to participate in an exercise trial. Our purpose was to assess the physical performance of these clients using measures with known predictive associations with risk of falls, hospitalization, and mortality in order to provide insights into the levels of physical performance in this population and the extent to which measured levels predict risk of adverse outcomes absent an intervention. This exploratory study was driven by the following research questions: (1) What percentage of older adult clients are at risk of falls, hospitalization, and mortality based on their scores on physical performance measures that have been validated as predictors for adverse care outcomes? (2) Do client physical performance measures correlate with the allocated hours of weekly caregiving assistance? and (3) Are there differences in hours of weekly caregiving assistance, Timed Up and Go (TUG), grip strength, and gait speed in clients who are able to rise from a chair without their upper extremities versus those who are not?
To our knowledge, this is the first study to report prevalence data on levels of physical performance among HCBS waiver clients using measures with known associations for adverse health outcomes such as fall risk, hospitalization, and mortality. We hypothesized that a substantial number of clients would be categorized as at risk of falls, hospitalizations, and all-cause mortality based on validated physical performance measures with established thresholds to predict risk of adverse health outcomes, given known levels of self-reported ADL and IADL impairment in this population.
Methods
Design and sample
This study employed an exploratory and descriptive design. A convenience sample of 42 older adults who enrolled in a concurrent exercise study and were living in the Chicagoland area and receiving HCBS through Community Care System, Inc., a licensed CCP vendor, participated in this study. Inclusion criteria were age >65 years, primarily English-speaking, not currently participating in regular exercise as defined as 30 min for ⩾3 days/week, receiving services through the Community Care System, Inc.’s Cook County office, and no health problems that contraindicate participation in physical activity as determined by the Exercise And Screening for You (EASY). 7 Participants received US$10 for participation in testing. The study protocol was approved by the University of Illinois at Chicago Institutional Review Board (2013-1152).
Data collection
Data collection occurred during a 1-week period in September 2014. Two trained research assistants who were Masters of Public Health students visited clients’ homes for testing. All clients signed informed consent prior to participation. Although the environment varied because testing took place in clients’ homes, research staff used the same test conditions across all participants. The same scripted instructions and equipment were employed to standardize testing across participants, despite changes across test settings.
Measures
Demographics
We collected client demographic information including age, gender, and weekly hours of caregiving assistance. The weekly hours of caregiving assistance are determined by the client’s DON score and represent the number of hours each week that a home care aide provides caregiving services in the client’s home.
Grip strength
Grip strength is an important marker of frailty and is associated with other performance measures, as well as self-reported measures of health.8–11 While a number of cut-point scores for classification of weak grip strength in older adults have been suggested, the most commonly reported range for weak grip is 16–21 kg in females and 30–37 kg for males.12–14 For analysis, we used cut-points of 20 kg for females and 30 kg for males, as those values have been associated with risk of poor mobility. 12
Participants completed two trials of grip strength on each hand with a Jamar Hand Hydraulic Dynamometer following standardized procedures. 15 The average value over two trials for each hand was calculated, and the higher value regardless of hand dominance was used for analysis.
The 30-s chair rise test
The 30-s chair rise test assesses the number of times an individual can rise from a chair in 30 s providing a measure of lower extremity strength. Normative values exist for this test, 16 which has excellent test–retest reliability (r = .89) and inter-rater reliability (r = .95). 17 Scores less than eight unassisted repetitions are associated with lower levels of functional ability. 18
Clients completed the 30-s chair rise using a standard height chair with arms crossed over their chests. Research staff instructed clients to fully stand and sit down as many times as possible within 30 s. If clients were unable to stand from the chair without upper extremity (UE) support, research staff noted the modification and had the client complete the test with the use of the UEs. We analyzed clients performing the 30-s chair rise with and without UE assistance separately.
TUG
Developed by Podsiadlo and Richardson 19 in 1991, the TUG is one of the most commonly used outcome measures to assess fall risk in older adults. TUG scores greater than 15 s predict fall risk at a rate of 87%. 5 The TUG has excellent test–retest, inter-rater, and intra-rater reliability.5,20 TUG specificity and sensitivity are high with values of 93.3% and 80%, respectively. 5 The TUG has also been shown to predict global all-cause mortality in ambulatory older males. 21
All clients completed two trials of the TUG with the average of the two trials used for the analysis. All clients completed the measure using a standard height chair with armrests. Clients began in a seated position, stood when instructed, walked around a small object placed 10 ft away, and then returned to a seated position in the chair. Research staff provided standardized instructions to all clients to complete the test as quickly as possible.
Gait speed
Suggested as the “sixth vital sign,” self-selected gait speed predicts future functional status, hospitalizations, health care utilization, functional decline, and falls.4,22 Walking speed declines with age with noticeable decreases between the ages of 70 and 80 years, especially in males. 23 Older adults able to walk more than 1 m/s are more likely to be independent of ADL, less likely to be hospitalized, more likely to be community ambulators, and able to cross a street safely. 4 Speeds less than 0.6 m/s are associated with ADL and IADL dependency, as well as increased hospitalization risk. 4 Conversely, hospitalization risk decreases by 40% for every 0.2 m/s increase in gait speed. 24 A speed of 0.6 m/s is suggestive of further functional decline in older adults with some level of existing impairment. 25 Finally, gait speed has been shown to be an independent predictor of 5-year all-cause mortality in older adults. Specifically, gait speeds less than 0.5 m/s are associated with higher all-cause mortality. 26
Research staff measured gait speed as the time required to complete a 10-ft walking distance at a self-selected, comfortable, usual pace with a 5-ft acceleration and deceleration length. All clients performed this measure twice with the average speed of the two tests used for the analysis.
Data analysis
We used SPSS 22.0 software to analyze data. Descriptive statistics including percentages were used to describe the sample. Bivariate analyses were conducted among the independent variables and between the independent and dependent variables (hours of weekly care) through correlation matrices using Pearson’s correlation coefficients. We partitioned the sample into two groups based on ability to rise from a chair with or without using upper extremities. We analyzed between-group differences using an independent t test. Finally, we modeled the hours of care received using hierarchical regression in order to investigate the ability of demographic characteristics and physical performance measures to predict hours of weekly care received. Demographic characteristics were entered at step 1, grip strength was entered at step 2, and mobility measures (TUG and gait speed) were entered at step 2. An alpha level of p < .05 was used in all tests of statistical significance.
Results
Demographics
Table 1 displays client demographics. Overall, the sample was 83% females, 75 years old, 50% African-American, and received over 13 h of HCA care weekly. Varied educational attainment was present with 52% having a high school degree or beyond, 21% attending but not completing high school, and 17% had only a grade school–level education. In comparison with the Illinois CCP population statewide, this sample had a greater percentage of female participants, was slightly younger, and had a larger representation of African-American clients (Table 2). Male participants were on average 82.6 years old and received on average 10 h of HCA care per week.
Client participant baseline demographics.

Baseline demographic characteristics of sample and statewide Illinois Community Care Program population.

Performance measures
Client characteristics on performance measures are shown in Table 3. Overall, a majority of participants had weak grip strength. Using a cut-off score of 20 kg for females and 30 kg for males, 25 out of 35 females (71.4%) were had weak grip strength. For males, six out of seven (86%) clients had weak grip strength.
Characteristics of sample on performance measures: total and by gender.

TUG: Timed Up and Go.
Clients exhibited substantial variability on the 30-s chair rise test. Only 31% of participants were able to rise from a chair without using their UE to assist. Furthermore, only 17% of participants met the threshold of eight repetitions indicating that 83% of the sample should be categorized as having lower levels of functional ability due to their lower extremity strength impairment. Nearly 10% of the sample was unable to rise from a chair even with the use of their UE and required physical assistance from another person to stand.
Overall, TUG scores ranged from 5.49 s to 2 min and 27 s with three clients unable to complete the test due to mobility impairments. Based on TUG performance, 57% of clients were classified as at risk of falls with TUG performance scores greater than 15 s.
Slow gait speed was prevalent throughout the sample. Only one client could ambulate more than the 1.0 m/s standard required for community ambulation. 4 In the sample, 64% of clients were at risk of hospitalization and further functional decline based on their inability to ambulate more than 0.6 m/s.4,25 Finally, 52% of participants were at increased risk of all-cause mortality due to an inability to ambulate faster than 0.5 m/s. 26
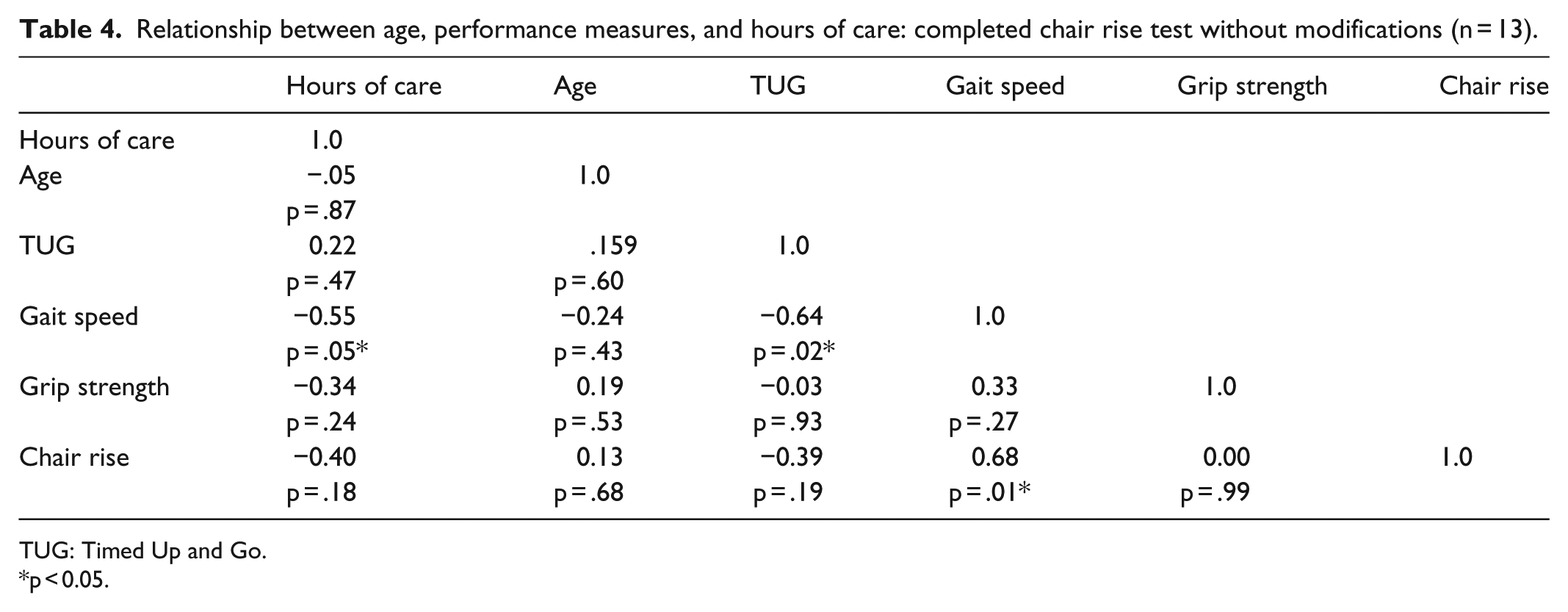
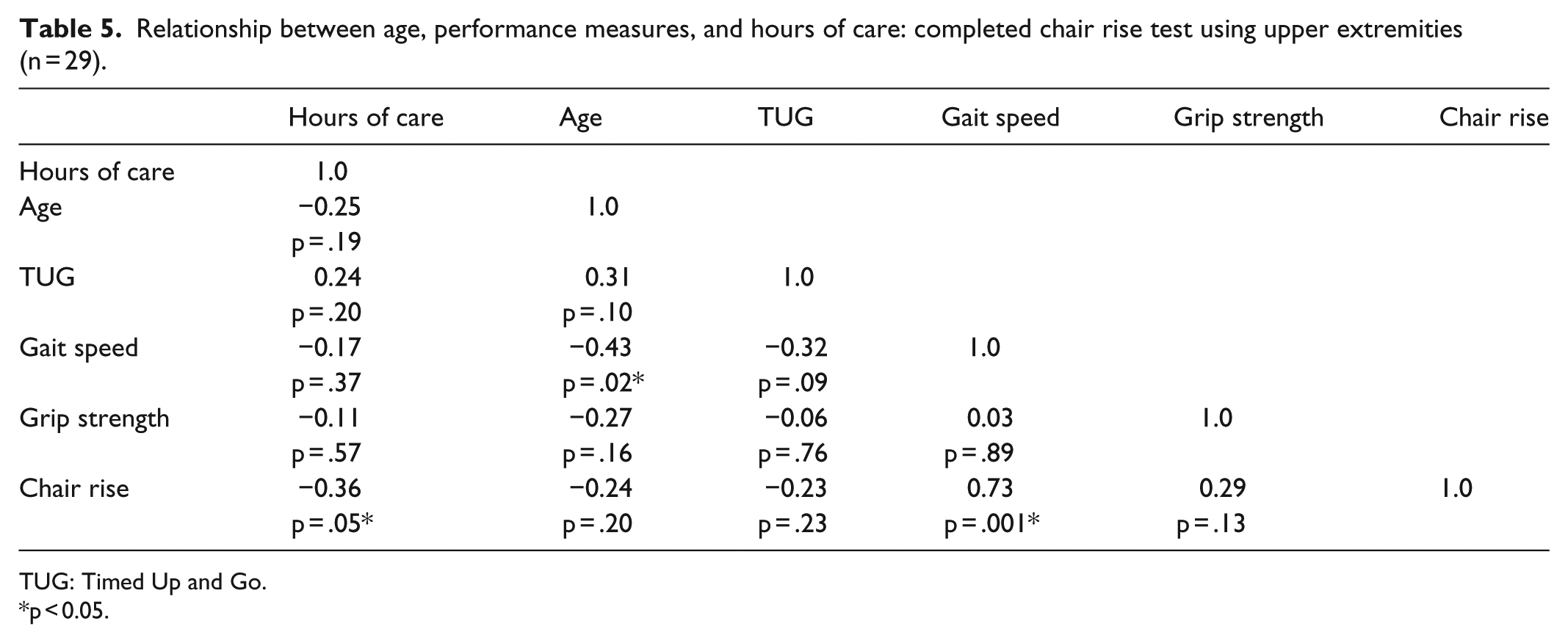
We investigated the relationship between physical performance measures, demographic characteristics, and hours of weekly caregiving assistance received. Due to the modification required by clients on the 30-s chair rise test, we analyzed groups separately: those able to complete the test following standardized procedures versus those completing the modified version using UE. Results are shown in Tables 4 and 5.
Relationship between age, performance measures, and hours of care: completed chair rise test without modifications (n = 13).
TUG: Timed Up and Go.
p < 0.05.
Relationship between age, performance measures, and hours of care: completed chair rise test using upper extremities (n = 29).
TUG: Timed Up and Go.
p < 0.05.
For those performing the 30-s chair rise without modifications, statistically significant correlations were found between gait speed, hours of care, TUG, and chair rise repetitions. For the clients requiring their UE to stand from a chair, statistically significant correlations were found between gait speed, age, and chair rise repetitions. Hours of caregiving assistance were significantly correlated with the number of chair rise repetitions.
We used an independent t test to further investigate group differences between those clients who were able to rise from a chair without the use of the UE and those who were unable. A two-group comparison is presented in Table 6. Across all variables, participants who were unable to stand from a chair without UE assistance had lower physical performance scores compared with those who were able to stand from a chair unassisted. Statistically significant differences were found in age, weekly hours of caregiving assistance, and gait speed between those who could stand unaided and those who could not.
Group differences in ability to stand from a chair.

TUG: Timed Up and Go.
p < 0.05.
We next examined correlations between the hours of weekly care, client demographics, mobility measures (TUG and gait speed), and strength measures (grip strength). We examined correlations among the predictor variables and found correlations were very weak to moderate ranging between r = −.08 (p = .63) and r = −.43 (p < .05). No independent variables were highly correlated, and collinearity statistics were all within accepted limits indicating no multicollinearity among independent variables.
We then used hierarchical regression to model hours of care as a function of these predictor variables (Table 7). In the first step of hierarchical regression, demographic variables were entered as predictors for weekly hours of caregiving assistance. This model was not statistically significant (F test: 2.439, p = .08). The addition of grip strength in the second step was not statistically significant (R2 change = .036, p = .20). In the final step, mobility measures (TUG and gait speed) were added into the model. This model was statistically significant (F test: 3.283, p = .01). The individual contribution of mobility measures was statistically significant (R2 change = .162, p = .02) and accounted for 16% of the variance in weekly hours of HCA care.
Summary of hierarchical regression analysis for variables predicting weekly hours of care.

TUG: Timed Up and Go.
p < .05.
Based on the associations between the performance measures tested in this study and risk of adverse outcomes, a substantial majority of participants in our sample could be classified as at-risk persons. Using Fried et al.’s 27 frailty criteria that classifies someone as frail if the person meets three of the following criteria: low physical activity, fatigue, weight loss greater than 10 pounds, weakness, and slow gait speed; 72% of clients (n = 30) are frail, given their documented grip strength, gait speed, and self-reported low physical activity levels.
Discussion
Although many studies have reported high self-reported ADL and IADL impairment in HCBS populations, this study is the first, to our knowledge, to directly measure physical performance to assess this issue. Consistent with previous research describing the pervasiveness of self-reported ADL and IADL deficits in this population,2,3 the majority of older adults in this study were found to have significant grip strength and mobility limitations when assessed using performance measures. These findings contribute important new information specifying the significant percentage of the sample at risk of falls, hospitalization, and all-cause mortality based on physical performance disability that is not captured by traditional self-reported ADL or IADL assessments. We argue that these findings contribute important new information specifying the significant percentage of the sample at risk of falls, hospitalization, and all-cause mortality based on physical performance disability that is not captured by traditional self-reported ADL or IADL assessments.
Significant differences in hours of care between clients who could rise from a chair without their UE and those who could not suggest that the allocation of hours of care that agencies provide based on unmeasured physical performance has some validity. The finding that decreased gait speed and inability to rise from a chair unaided are associated with increased hours of care is consistent with the allotment of client hours based on self-reported greater physical limitation. However, nearly 10% of this sample was unable to rise from a chair at all. The inability to stand without physical assistance is a significant indicator of mobility impairment and places older HCBS clients at risk of serious adverse outcomes, including falls, malnutrition, or pressure wounds, since these persons are unable to transfer on their own in order to perform basic requirements of daily life activities. The association between ability to rise from a chair and increased hours of care received suggests that a simple assessment of the ability to rise from a chair could serve as a valuable and quick screening tool to determine those at risk of functional decline.
We found that gait speed was the strongest predictor of hours of care received. Gait speeds less than 1.0 m/s indicate a need for interventions to reduce fall risk. 28 The finding that only one participant in the study was able to walk faster than this threshold supports the need for targeted interventions in this population to improve gait speed in order to improve functioning and decrease fall risk. Furthermore, the slow average gait speed seen in this sample suggests that these individuals face substantial limitations or complete inability to ambulate in the community. Since HCBS are designed to support and maintain individuals in community settings, interventions to address the mobility requirements necessary for community living are urgently needed. Finally, given the association between slow gait speed and risk of hospitalization, the prevalence of slow gait speed in this sample underscores the vulnerability of this population. Gait speed levels documented in this study indicate that 64% of clients are at a high risk of hospitalization and loss of community living. In this study, mobility measures explained 16% of the variance in hours of care received. This finding along with previous research showing that gait speed is a strong predictor of future functioning provides justification that gait speed should be considered in client assessments when prescribing hours of care.
Practical implications
To translate these study findings into practical implications, we argue that HCBS waiver programs incorporate standardized physical performance measures into their regular client assessments. The performance measures used in this study can be implemented with minimal training, time, and equipment needs and could be implemented by paraprofessionals serving HCBS clients. Utilizing existing care providers to implement this data collection is likely to be a cost-effective way to obtain important client information which could be used to facilitate referrals for additional services such as rehabilitation services, physical activity programs, or medical follow-up to complement standard care. Furthermore, results on these physical performance measures could allow for interventions to be directed to clients who are most at risk of adverse health outcomes in order to reduce health care expenditures and improve client quality of life.
Limitations
Several factors limit the generalizability of findings. This study examined physical performance in a small sample of total users of the CCP in Illinois. Sedentary participants were drawn from a single geographic location and restricted to a large provider agency in Illinois. Future studies need to explore the diverse population of older adult waiver recipients by both ethnic background and geographic region. The small number of males, 17% of our sample, further limits our findings. Further investigation into the physical performance of males who receive HCBS is needed in order to more broadly generalize findings to that population. Finally, we were unable to control for specific types of chronic health conditions faced by participants in the study. Certain conditions such as osteoarthritis or stroke have strong associations with mobility limitations, and a history of these mobility-impacting conditions could influence performance on physical outcome measures.
Conclusion
This study provides the first report, to our knowledge, of levels of physical performance using measures that are validated predictors of adverse outcomes in a sample of older adult HCBS waiver recipients. Identifying specific characteristics of this population is critical for developing appropriate health promotion efforts. Findings from this study affirm that this population has functional limitations, but for the first time highlight the significant risks for adverse health outcomes that are associated with clients’ low performance in upper and lower extremity strength, mobility, and gait speed. Despite limitations, this study obtained important new information about CCP client physical functioning that is not currently obtainable using existing assessment tools. The results of this study advance what is known about the frail, homebound population, and identify areas that are important to address in future research and practice, such as the use of these measures as part of routine client assessments. The use of these tools to classify clients relative to risk of falls, hospitalization, and mortality moves assessment beyond ADL and IADL in order to promote more coordinated care by screening clients for needed referrals to other health care providers or targeted evidence-based interventions that can improve physical function.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Grant Number P30AG022849 from the National Institute on Aging. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute on Aging or the National Institutes of Health.