
Abstract
Objectives:
To evaluate the feasibility of the Nintendo WiiFit™ as an adjunct to usual therapy in individuals with a lower limb amputation.
Methods:
The study was a Multiple Baseline (AB) Single Subject Research Design. Subjects were ≥19 years old, had their first unilateral transtibial or transfemoral amputation ≤12 months ago, and were participating in prosthetic training. WiiFit training was provided for 30 min, 5 times a week, for a minimum of 2 and a maximum of 6 weeks in addition to usual therapy. Feasibility indicators were safety, post-intervention fatigue and pain levels, adherence, and subject’s acceptability of the program as measured by the Short Feedback Questionnaire–modified (SFQ-M). The primary clinical outcome was walking capacity assessed by the 2 Minute Walk Test (2MWT). The secondary clinical outcomes were the Short Physical Performance Battery, L-test, and Activities-Specific Balance Confidence.
Results:
Subjects (4 transtibial; 2 transfemoral) had a median age of 48.5 years (range = 45–59 years). No adverse events associated with the intervention occurred. Median pain and fatigue levels were 1.3 (range = 0.5–3.5) and 3.1 (range = 1.4–4.1), respectively. Median adherence was 80%. Subjects found the WiiFit enjoyable and acceptable (median SFQ-M = 35). Five subjects showed statistical improvement on the 2MWT and four on the secondary outcomes (p < 0.05).
Conclusion:
The WiiFit intervention was found to be feasible in individuals with unilateral lower limb amputation. This research provides the foundation for future clinical research investigating the use of the WiiFit as a viable adjunctive therapy to improve outcomes in individuals with unilateral lower limb amputation who are participating in prosthetic training.
Keywords
Introduction
Approximately 1 million individuals were living with a lower limb amputation (LLA) in the United States in 2005. 1 This number is projected to more than double by 2050 due to the aging population and the growing incidence of diabetes-related dysvascular disease. 1 The rising number of LLAs will impose an economic burden on the health-care system as a result of the substantial costs associated with post-amputation care, including prosthesis procurement and rehabilitation. The costs of care post a LLA from surgery to follow-up post-prosthetic rehabilitation are considerable. A US study suggests that the 2-year cost for total care (surgery to 1 year post discharge from rehabilitation to follow-up) is approximately US$86,000 for those with transtibial (TT) amputation and $110,000 for those with transfemoral (TF) amputation. 2 Rehabilitation costs are also substantial with mean investments of almost $15,000 for TT and $20,000 for TF prosthetic training alone. 2
LLA is associated with significant functional limitation and disability, 3 including reduced lower limb strength, 4 poor balance, 4 and poor balance confidence, 5 all of which contribute to reduced walking. 6 Walking capacity (as measured by distance walked) has been reported as one of the strongest determinants of health-related quality of life in individuals with a LLA.7,8 The ability to walk further allows the individual to move around his/her environment more independently and safely, which in turn impacts an individual’s choice of activities and participation. 9
Following a LLA, the restoration of function and reinstatement of functional independence requires participation in a prosthetic training program. Provision of such care enables individuals to walk and remain active while abating the progression of disease and disability.1–3 A well-planned prosthetic training program incorporates balance and strength training in combination with aerobic training, all of which promote walking. 10 Regaining functional independence requires individuals to repeat specific motor tasks. Over time traditional exercises associated with most training programs may become tedious causing clients to lose motivation and adherence to the program goals may decline. 11
The use of virtual reality (VR) systems as an adjunct to usual therapy may not only contribute to improved walking, but may also motivate and promote adherence to the prosthetic program.12,13 VR allows clients to engage in interactive virtual environments that simulate real activities in a safe setting. 14 The intensity of practice can be manipulated, and therefore individualized treatments can be provided to the clients. VR offers an opportunity for a high degree of repetition which will be essential to the acquisition of the motor task.15,16 In addition, VR creates an enjoyable and engaging learning environment through providing real-time visual and auditory feedback, thereby facilitating motor learning.12,15,17 VR provides information about client’s motor movements (knowledge of performance) and outcomes of those movements (knowledge of result). Knowledge of the performance is provided through mirroring the movements of the client. Knowledge of results is provided at the end of each exercise through numerical summaries. The presence of knowledge of performance and knowledge of results is essential to learning because they provide the client with task-related information about the skill being learned and thereby enhance motor learning. 18
Due to the cost and lack of commercial availability of health-oriented VR systems, the notion of using off-the-shelf commercial VR technologies in rehabilitation has recently been embraced. The Nintendo WiiFit™ is a low-cost VR gaming system that is widely available. The WiiFit balance board has sensors that measure the user’s center of pressure and weight distribution. Users interact with the games through weight-shifting while standing on the balance board or while using a handheld remote control. The weight-shifting, gait and balance-training nature of the WiiFit games make them suitable as potential training tools to improve functional outcomes in individuals with a LLA.
Promising results have been reported regarding safety, feasibility, and efficacy of the WiiFit in a number of other rehabilitation populations such as with older adults, and individuals with mild Alzheimer’s and Parkinson’s disease.19–23 WiiFit has been associated with improvement in balance in older adults, 20 balance and gait in individuals with Alzheimer’s, 21 and walking, mobility, lower limb strength, balance,22,23 and independent performance of activities of daily living in individuals with Parkinson’s disease. 23 It seems plausible that given similar challenges with multiple co-morbidities, deconditioning, decreased walking capacity, and physical activity, individuals with LLA may also benefit from WiiFit treatment. D’Angelo et al. 24 recommend that the use of VR treatments should be investigated in individuals with LLA based on the outcomes from gait rehabilitation using VR systems in other populations. Recently WiiFit was assessed using two descriptive uncontrolled case-studies. The participants in the study showed improvement in balance, balance confidence, and spatial–temporal parameters of their gait. 25
Although case-studies provide useful foundational information, they have important limitations including a lack of experimental control. Single subject research design (SSRD) uses within-subject control, thereby increasing the internal validity of the results. In this study, we used a SSRD to evaluate the feasibility of the WiiFit as an adjunct to usual therapy to improve walking capacity in individuals with a first unilateral TT or TF amputation. We hypothesized that the WiiFit would be feasible as an adjunct treatment in terms of safety, post-intervention fatigue and pain levels, acceptability, and level of adherence. Our primary clinical hypothesis was that the WiiFit would improve walking capacity. Our secondary hypotheses were that the WiiFit would result in improved basic functional mobility, lower limb functioning (balance, gait speed, and strength), and balance confidence.
Materials and methods
Design
We used a non-concurrent multiple baseline (AB) SSRD. This design is particularly robust for controlling threats to internal validity related to maturation and history that evolve when the investigator expects to see improvement upon introduction of the intervention. Furthermore, because each subject serves as his or her own control, the investigator develops a better understanding of individual differences, thereby allowing the researcher to determine the characteristics of individuals who might benefit from the intervention for a future randomized controlled trial (case-finding). An AB design includes a baseline (A) phase with repeated measurements during a period of no experimental intervention followed by the introduction of the intervention of interest (B phase), while continuing with systematic measurements. Non-concurrent multiple baseline implies that the intervention is introduced at different time points (e.g. subject 1 has 2 weeks of baseline vs subject 2 receives 3 weeks of baseline) for each of the subjects. In our study, a total 24 data points were collected for each subject over 8 weeks with at least 6 baseline measurements and at most 18 intervention data points. Subjects were randomly assigned to a progressively longer baseline period accompanied by a progressively shorter intervention period (Table 1). This study was approved by the Clinical Research Ethics Board of the University of British Columbia and performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. Participants provided their informed written consent prior to their inclusion in the study.
Allocation groups.

Note: M = Monday; W = Wednesday; F = Friday.
Setting
Subjects were recruited from the outpatient amputee rehabilitation program at GF Strong Rehabilitation Centre, Vancouver, British Columbia.
Subjects
A study letter of information was provided to all eligible individuals upon initiation of their rehabilitation at the center by the treating physiotherapist. Individuals were included if they were 19 years or older and had their first unilateral TT or TF amputation ≤ 12 months ago. Individuals who had wound(s) on their residual limb that would prevent wearing a prosthesis, had complex medical problems (e.g. congestive heart failure), or previous experience with the WiiFit or other VR games were excluded.
Intervention
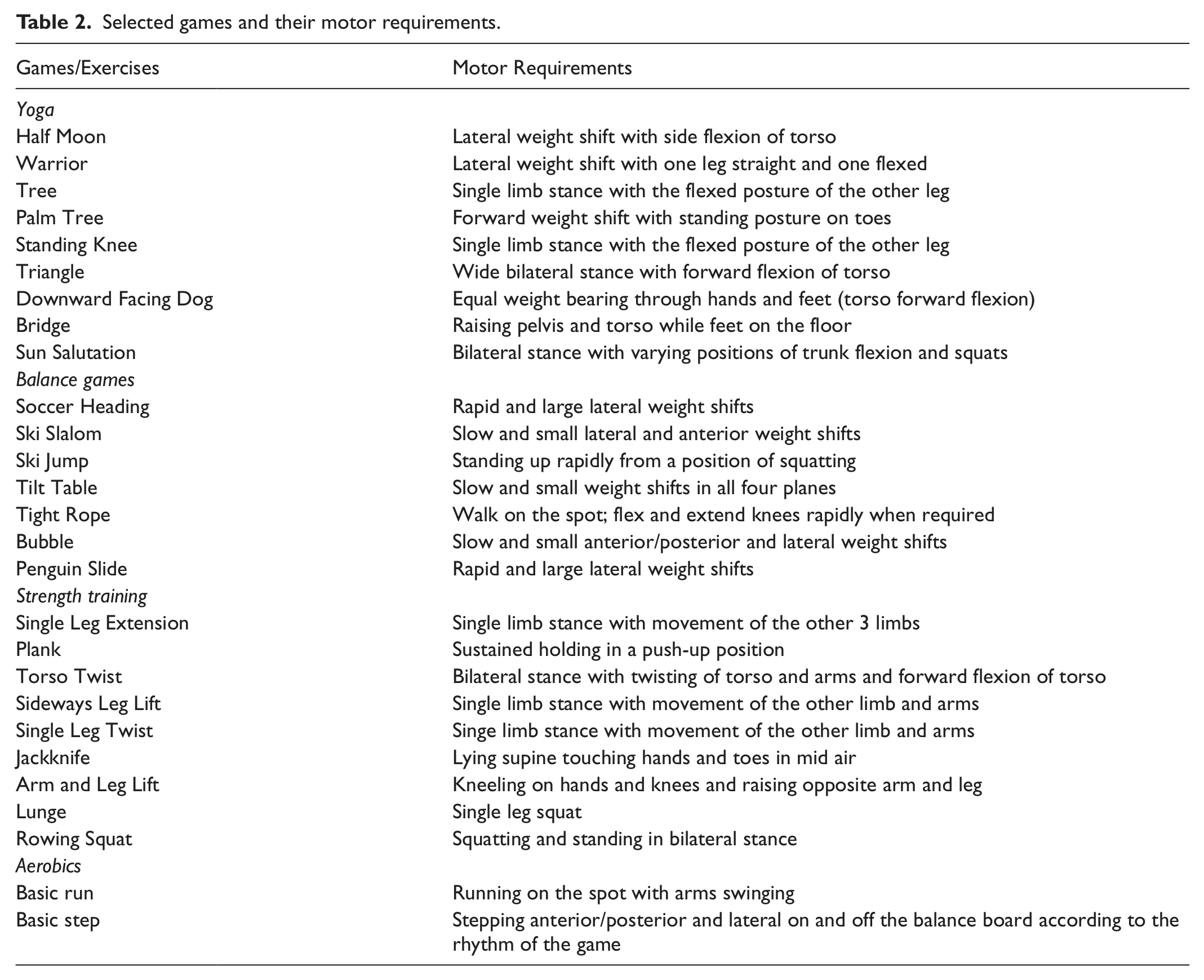
The intervention consisted of training using the WiiFit program for 30 min, 5 times a week for a minimum of 2 weeks (10 sessions) and a maximum of 6 weeks (30 sessions). Subjects also continued to receive their usual therapy which included physiotherapy provided by a single physiotherapist. The WiiFit intervention required subjects to weight shift while standing on the WiiFit balance board or while using a handheld remote control. The intervention included the following: (1) yoga: static standing both single and double leg, and static mat exercises, (2) balance games: lateral and posterior/anterior weight-shifting exercises in standing, (3) aerobics: running on spot and step class, and (4) strength training: dynamic standing both single and double leg, and dynamic mat exercises. Each intervention session included selected exercises/games from all the four categories. Table 2 summarizes the list of exercises/games and their motor requirements. The exercises/games were selected carefully by a trained research assistant based on the physiotherapist’s assessment of the subject’s abilities. Depending on their performance, participants were allowed 2–4 trials per exercise/game at each session. For example, participants were asked to repeat the exercise/game for 4 trials if they did not obtain a good score in the previous trials or if they used an incorrect posture/technique for the game. Progression to more difficult and longer activities was guided by a manual which was developed by the physiotherapist and based on the WiiFit program. In the manual, the exercise positions were modified by adding unilateral or bilateral external hand support if required by the subject. The exercises were modified if the subject was unable to do the exercise or to use the prosthesis for the exercise. For subjects with a TF amputation, the exercise was modified if the prosthesis was not structurally capable of assuming the exercise position (e.g. some of the exercises required a stance phase flexion of the prosthetic knee). Cueing and correction of the positioning was given by the research assistant if the subject used poor posture or unsafe technique. Please visit http://millerresearch.osot.ubc.ca/resources/ for a copy of the manual.
Selected games and their motor requirements.
Outcome measures
Relevant demographic (age, sex, employment status, and education level) and clinical variables (cause and level of amputation, months since amputation, prosthetic fit stage, and type of assistive device used for walking) were recorded at enrollment. Outcome measures were administered in random order 3 times a week (Monday, Wednesday, and Friday) throughout the baseline and intervention phases.
Feasibility indicators were WiiFit program’s safety, post-intervention pain and fatigue levels, adherence level, and acceptability. Safety was determined by recording the incidence of adverse events (e.g. falls and injuries) during the intervention. Subject’s pain and fatigue levels were measured at the end of each intervention session on a scale of 0 to 10 (0 = no pain; 10 = extreme pain and 0 = no fatigue; 10 = extreme fatigue). Scores above 6 were considered high levels of pain or fatigue. Missed intervention appointments and the reasons for the missed sessions were recorded to evaluate program adherence. The percentage of intervention adherence was calculated as follows: (the number of completed intervention sessions/the total number of potential sessions) × 100. Values ≥80% were considered high adherence levels. The Short Feedback Questionnaire–modified (SFQ-M) was administered on the last day of intervention to inquire about subject’s acceptability of the WiiFit program. 26 The SFQ-M has 10 items to assess the subjects: (1) feeling of enjoyment, (2) sense of being in the environment, (3) sense of success, (4) sense of control, (5) perception of the environment as being realistic, (6) perceptions of whether the feedback from the computer was understandable, (7) indication of whether any discomfort was experienced during the intervention, (8) thoughts on whether they would engage in this experience again, (9) thoughts on whether they think they would be able to exercise at home, and (10) perception of difficulty with performing the task. The first nine items were ranked from 1 (not all) to 5 (a lot), whereas the anchors for item 10 were ranked from 1 (very difficult) to 5 (very easy). The total scores for the SFQ-M ranged from 10 to 50, with higher scores representing higher levels of positive experience with the WiiFit program.
The primary clinical outcome of interest, walking capacity, was assessed using the 2 Minute Walk Test (2MWT). 27 Starting from a standing position, subjects were asked to walk as far as they could in a safe manner for 2 min over an 80-m, indoor course with one turn to the left. The distance traveled to the nearest meter was recorded. Evidence of intrarater reliability (ICC = 0.96), interrater reliability (ICC = 0.98), 27 validity, 28 and responsiveness to change has been demonstrated in individuals with a LLA. 28
A number of secondary outcome measures were used. The Short Physical Performance Battery (SPPB) measures the ability to perform three basic functional tasks: standing balance (ability to stand with the feet either together, semi-tandem, tandem, or in a single leg stance position for 10 s each), gait speed to the nearest second (over 4 m using a standing start), and lower limb strength (the time to the nearest second taken to complete rising 5 times from a sitting position in a chair without using hand support). 29 Each of the tasks was scored separately on a scale ranging from 0 (poor) to 4 (excellent). A total score, ranging from 0 to 16, was derived by adding scores from the individual tasks. There is support for test–retest reliability (ICC = 0.92), validity, and responsiveness of the SPPB for older adults with disability. 30
The L-test was used to measure basic functional mobility. 31 This test consists of a sit-to-stand component and requires turns to both the left and the right (in the shape of an L) over a distance of 20 m. Participants were instructed to complete the test as fast as they could in a safe manner. The time to the nearest second to complete the course was recorded. The psychometrics are reported for individuals with a LLA with respect to interrater (ICC = 0.96) and test–retest (ICC = 0.97) reliability, and validity. 31
The 16 item Activities-Specific Balance Confidence (ABC) scale was used to measure the subjects’ perceived balance confidence. 32 Each item is scored on a scale that ranges from 0 (no confidence) to 100 (completely confident), and a mean summary score is calculated to represent overall confidence. Evidence for validity and test–retest reliability (ICC = 0.91) for individuals with a LLA has been reported. 33
Analyses
Medians were calculated for the continuous descriptive variables, and percentages were calculated for the categorical variables. Median pain and fatigue scores and percentage adherence were derived for the entire group. Total SFQ-M scores were calculated for each subject as well as median SFQ-M scores for the entire group.
To address our primary and secondary hypotheses, the scores at all data collection time points were graphed for each subject for visual inspection. To determine whether there was a statistical difference between the phases, we used the 2 standard deviation (2SD) band method. 34 In this procedure, bands are created 2SDs above and below the mean of the baseline data points and were extended into the intervention phase. If at least two consecutive data points in the intervention phase fall outside of the 2SD band, the difference from baseline to intervention was considered statistically significant. The probability of two successive data points occurring outside the 2SD band is less than 5% (p < 0.05). 35 The advantage of the 2SD method is that it is robust to the variability in the data that may naturally occur across the phases of a SSRD.
Results
In total, 8 subjects were enrolled. Two subjects dropped out: one due to a prosthetic fit issue and the other due to having a symptomatic neuroma on his residual limb that required surgery. The remaining 6 subjects who completed the study were predominately male (n = 5) and had a median age of 48.5 years (range = 45–59 years) (Table 3).
Descriptive and clinical characteristics of the sample and significance of outcomes (n = 6).
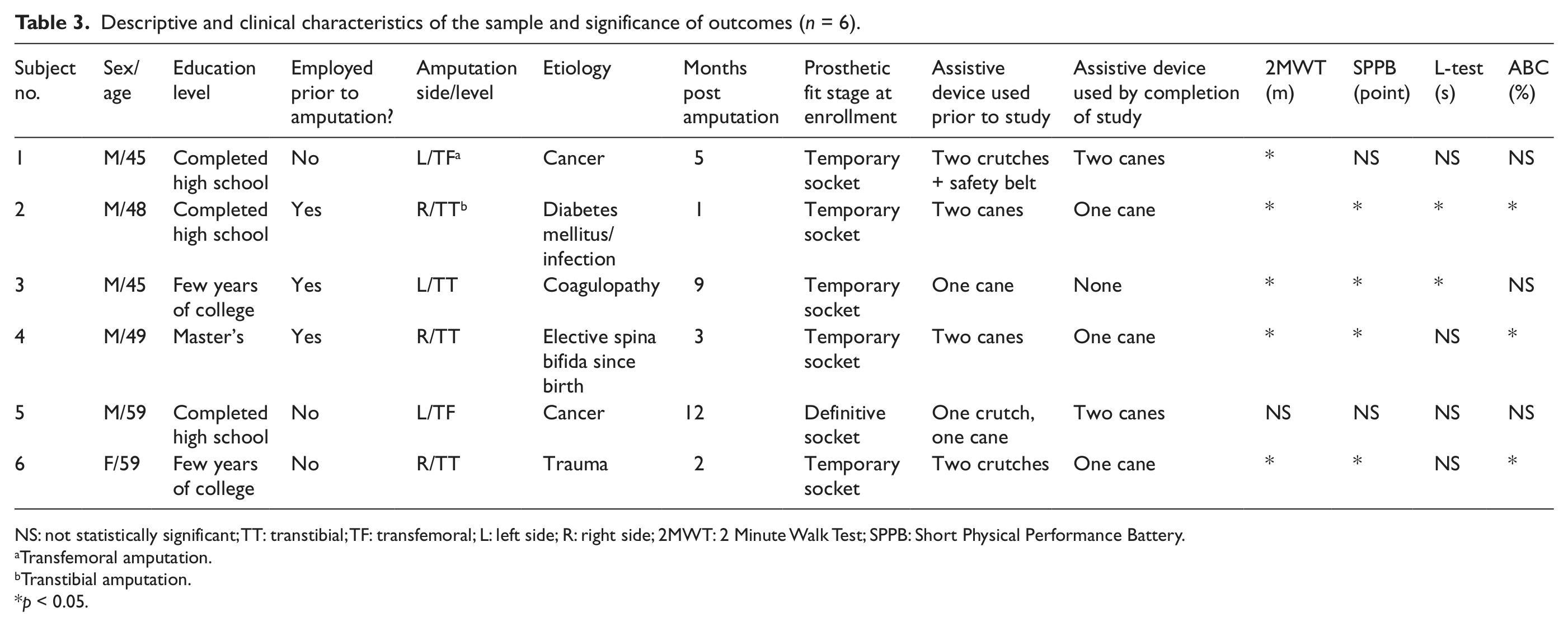
NS: not statistically significant; TT: transtibial; TF: transfemoral; L: left side; R: right side; 2MWT: 2 Minute Walk Test; SPPB: Short Physical Performance Battery.
Transfemoral amputation.
Transtibial amputation.
p < 0.05.
Feasibility indicator outcomes
No adverse events occurred due to participating in the intervention. Median post-intervention pain and fatigue scores for the entire group were 1.3 (range = 0.5–3.5) and 3.1 (range = 1.4–4.1), respectively. Median intervention adherence for the entire group was 80% (range = 60%–100%). Two subjects had adherence levels of <70%; however, the reasons for low adherence were related to prosthetic and general health (Table 4). Subject 3 had the poorest program adherence as well as the lowest SFQ-M score; however, he showed statistical improvement on three clinical outcomes (discussed below). The median SFQ-M score for the entire group was 35 (range = 19–45). Four subjects reported positive experiences with using the program and indicated that they found it enjoyable (median score for item 1 = 4) (Table 4).
Participants’ intervention adherence (%) and SFQ-M scores. a

SFQ-M: Short Feedback Questionnaire–modified.
SFQ-M items 1–9 are scored from 1 (not at all) to 5 (a lot). Item 10 is scored from 1 (very difficult) to 5 (very easy). Higher SFQ-M scores indicate a more positive experience with the WiiFitTM program.
Clinical measure outcomes
At the end of the program, subjects achieved a median distance of 166 m (range = 65–211). On average, TF subjects walked a median distance of 73 m, while TT subjects walked a median distance of 180 m. Figures 1–6 illustrate graphical representation of the results for the 2MWT for each subject. As can be seen in Figure 1, there was an increase in walking distance upon introduction of the intervention and ≥2 consecutive data points were above the 2SD line. This result was consistent for subjects 2, 3, 4, and 6. Subject 5 demonstrated a marked decline over the study period.

Graphical representation of the 2MWT for subject 1 (baseline mean = 50.6; intervention mean = 62 m).

Graphical representation of the 2MWT for subject 2 (baseline mean = 160.8; intervention mean = 198.5 m).

Graphical representation of the 2MWT for subject 3 (baseline mean = 142; intervention mean = 172.7 m).

Graphical representation of the 2MWT for subject 4 (baseline mean = 103.7; intervention mean = 146.9 m).

Graphical representation of the 2MWT for subject 5 (baseline mean = 67.9; intervention mean = 62 m).

Graphical representation of the 2MWT for subject 6 (baseline mean = 115.4; intervention mean = 152.1 m).
For the secondary clinical outcomes, subjects 1 and 5 did not show statistical improvement in any of the secondary outcomes. Four subjects showed statistical improvement in the SPPB, whereas three subjects showed statistical improvement on the ABC scale (Table 3).
Discussion
The WiiFit program is an entertaining off-the-shelf gaming software program that has potential to offer health and retraining benefits for individuals with a LLA. In this study, we created a systematic intervention program based on the WiiFit and tested its feasibility to improve walking capacity in individuals with unilateral LLA.
The program was found to be feasible given no adverse events, low levels of reported pain and fatigue post intervention, and high adherence and acceptability levels. According to the SFQ-M scores, all but one of the subjects found the WiiFit acceptable, entertaining, and enjoyable. Others have also reported that over 70% of participants with disability enjoyed the WiiFit intervention more than their usual therapy and about 90% expressed that they would like the program to be added to their usual therapy. 13 Program enjoyment is crucial because it has been linked to increased program adherence.36–38 Our program adherence of 80% supports this notion. Only one subject (subject 3) did not enjoy the intervention and reported visual and audio discomfort that may have been related to reported migraine headaches.
The WiiFit exercises/games stimulated static and dynamic balance, and stationary gait training,23,39 all of which are critical to improve prosthetic walking. 4 The yoga games mainly targeted static balance training, whereas the balance games, strength training, and aerobics focused on dynamic balance and gait training. At the end of program, subjects walked a median distance of 166 m. As one might expect, TF subjects walked a median distance of 73 m, while TT subjects walked a median distance of 180 m. The observed difference between TT and TF subjects is not surprising, given that a higher level of amputation results in a greater loss of function and decreased walking efficiency as a result of an increased energy cost. 40 The observed walking capacity values for both our TT and TF subjects are higher than those reported in the literature where outpatient TT amputees walked for a distance of 121–141 m 27 and TF amputees at discharge walked for 35 m. 28 Although our sample was younger than those in the literature (mean age 55 years for TT and 66 years for TF), the increased distance walked in our study may be due to the WiiFit treatment effect. All but one subject showed statistical improvement in walking distance after the introduction of the WiiFit training. This finding is reassuring because improving walking capacity is one of the primary goals of prosthetic training, and it is one of the strongest determinants of health-related quality of life in individuals with a LLA.7,8,41 The lack of improvement in subject 5’s walking capacity may reflect the fact that he had the shortest intervention period (2 weeks); however, some trending toward improvement was still expected; in fact, this subject demonstrated a decline in walking capacity upon introduction of the intervention. A possible explanation is that his health deteriorated during the study due to the progression of his pulmonary metastasis.
Two subjects did not show statistical improvement in any of the secondary measures. Both these subjects had a TF amputation. Since a TF amputation usually results in a greater loss of function and longer rehabilitation compared to those with a TT amputation, it is plausible that a longer intervention may be required for an individual with a TF amputation to show statistical improvement. 40 Four subjects did improve related to the elements of the SPPB (balance, gait speed, and lower limb strength), suggesting some support for our secondary hypothesis that training with the WiiFit may result in improvement in balance, gait speed, and lower limb strength. This finding is consistent with other studies that have shown training with the WiiFit resulted in improvement.20–23
Only two subjects showed statistical improvement on the L-test. The L-test requires a higher level of function compared to other walk tests because it incorporates a sit-to-stand transfer as well as turns to both the left and the right. 31 It is not clear why the other subjects did not show statistical improvement on the L-test. However, the two subjects who showed statistical improvement also showed statistical improvement in all other performance-based measures (2MWT and SPPB) and progressed to higher, more complex levels on the WiiFit.
Finally, three subjects showed statistical improvement in the ABC scale, which supports the previous finding that the WiiFit training results in improvement in balance confidence in individuals with unilateral LLA. 25 This trend was not observed in the other three subjects. One of these subjects (subject 1) had a very low ABC score at baseline, which decreased throughout the study. The reason for decline is not obvious; however, this subject was diagnosed with a brain injury at an early age and as a result there was some concern by the study physiotherapist that he may have some cognitive impairment influencing his ability to comprehend the scale. This is one possible limitation of the study given that subjects were not screened for cognition. Future studies should measure cognitive impairment as a potential confounder particularly for outcome measures that use subjective responses.
Study limitations
The study had a number of limitations. First, because subjects received both their usual therapy and the WiiFit intervention, we cannot confirm that the observed improvement was the result of the intervention. Future studies should focus on evaluating the effect of the WiiFit treatment in community dwelling individuals with a LLA who are no longer in active rehabilitation. Alternatively, a full factorial design addressing each component should be considered. Second, the small and heterogeneous sample of SSRD limits our ability to generalize the findings to the broader population of individuals with a LLA. However, case-finding is a robust feature of SSRD and therefore heterogeneity is desirable for this type of design. The SSRD allows us to determine the characteristics of individuals who may most benefit from the intervention, thereby enabling us to target a more homogenous sample for a future larger randomized control trial. For example, because two subjects withdrew from the study due to residual limb/prosthetic fit issues, we concluded that for a future larger study we need to include individuals with a mature LLA who have no or minimal residual limb/prosthetic fit problems. Third, although repeated testing offers control over maturational trends and history, it may have introduced a learning bias with improvement on the test possibly being to the result of practice. Future larger trials with fewer measurements may minimize this bias. Fourth, the use of the 2SD band method of analysis for a study on an acute population may add bias because the baseline data may show improvement as a result of natural recovery. However, the 2SD band method remains the main statistical method for SSRD studies. Finally, our sample was relatively young and may not represent the majority of the LLA population. Future studies are required to investigate the use of the WiiFit in older individuals with a LLA.
Conclusion
The WiiFit intervention was found to be feasible in individuals with unilateral LLA. The results of this study suggest that the WiiFit may contribute to improved walking capacity and functional outcomes in individuals with unilateral LLA. This research provides the foundation for future clinical research investigating the use of the WiiFit as a viable adjunctive therapy to improve walking capacity and therefore health-related quality of life in individuals with unilateral LLA.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the British Columbia Rehabilitation Foundation for funding the study and the Canadian Institutes of Health Research for Masters Scholarship for Ms. Bita Imam. The study was conducted at: 2GF Strong Rehabilitation Research Lab, Vancouver, BC, Canada. Material in this manuscript has been presented at the Canadian Association of Physical Medicine & Rehabilitation (CAPM&R) Annual Scientific Meeting in Victoria in June 2011.
Clinical Trial Registration Number: NCT01131819
Declaration of conflicting interests
The authors declare that no party having a direct interest in the results of the research supporting this article has or will confer a benefit on us or on any organization with which we are associated, and we certify that all financial and material support for this research (e.g. NIH or NHS grants) and work are clearly identified in the Funding section below. The article does not contain information about medical device(s).
Funding
Operating grant from the British Columbia Rehabilitation Foundation; Canadian Institutes of Health Research Masters Scholarship (BI).