
Abstract
Background:
Conflicting reports exist on the effect of sildenafil on ophthalmic artery blood flow; many visual disturbances due to vascular insult were reported with the use of sildenafil in diabetic patients like nonarteritic ischemic optic neuropathy.
Objectives:
The present work aimed to investigate whether sildenafil modulates ophthalmic artery vasoreactivity in patients with type 2 diabetes mellitus. Literature reports on this aspect are lacking.
Methods:
A total of 35 male subjects were enrolled in this study, 18 with type 2 diabetes mellitus matched with 17 normal individuals. Ophthalmic artery was insonated through a transorbital window using colored Doppler equipment with transcranial Doppler facility. Ophthalmic artery reactivity was assessed using breath holding/hyperventilation test, before and after giving 50 mg oral sildenafil.
Results:
It was found that in both normal subjects and diabetic patients, sildenafil increased baseline control of mean flow velocity of ophthalmic artery significantly (p < 0.05), breath holding caused a decrease of MFVopa (p < 0.05), and subsequent hyperventilation caused increase of MFVopa (p < 0.05). There was no statistically significant change in breath holding index and full range of vasodilatation of ophthalmic artery (p > 0.05) after sildenafil, in normal and diabetic groups. There was a significant increase of resistive index of ophthalmic artery flow in diabetic patients compared with that of normal subject (p < 0.05). Sildenafil decreased resistive index of ophthalmic artery flow significantly only in diabetic patients (p < 0.05).
Conclusion:
Sildenafil increased MFVopa, but had no significant effect on vasoreactivity of ophthalmic artery; sildenafil decreased resistive index only in type 2 diabetic patients.
Introduction
Cumulative research data have demonstrated that sildenafil prevents the inactivation of cyclic guanosine monophosphate (cGMP) in vascular and visceral smooth muscles by inhibiting phosphodiesterase type 5 (PDE-5) and increases the concentration of cGMP. As a result, the potent effect of nitric oxide (NO) produced by the neurons innervating ocular blood vessels, as a smooth muscle relaxant, becomes greater.1–3
Furthermore, in many experimental studies, it is shown that NO plays a pivotal role in the local regulation of ocular blood flow. 4 A drug donating NO such as nitroglycerin has been reported to increase systolic and diastolic retinal artery blood flow velocities, based upon Doppler sonographyical measurements. 5 Likewise, using laser Doppler flowmetry, isosorbide mononitrate was reported to significantly increase optic nerve blood flow, 6 and cilostazol, a selective cyclic adenosine monophosphate (c-AMP)–PDE inhibitor, was shown to increase the diameter of retinal arterioles and the rate of blood flow in anesthetized rats, independent of changes in mean arterial pressure. 7
In view of the background of the relaxant effect that sildenafil exerts on smooth muscles at the sinusoids of the penile corpus cavernosum, thereby increasing the blood flow into sinusoids,2,8,9 an analogy has been assumed to exist between the penile corpus cavernosum and the human choroid, which is also an erectile tissue, and serves in supporting the metabolic function of the outer retina. 10 Thus, sildenafil may also have a similar vasodilator effect on the choroidal vascular bed and may decrease arterial resistance and increase the volume of choroidal blood flow. However, nonunanimity exists on the available literature reports on this aspect. In a double-blind randomized, crossover study performed in 15 healthy male volunteers with a mean age of 39 ± 8 years who received a 100-mg dose of sildenafil, Grunwald et al.11,12 neither observed any significant difference in the optic nerve head or foveolar choroidal blood flow and ocular perfusion pressure nor any statistical difference between the diameters of retinal blood vessels. Conversely, Pache et al. 13 detected a significant increase in the diameter of the superior temporal artery and vein after giving sildenafil.
Sildenafil was shown to cause a significant increase in blood flow in ophthalmic, central retinal, and short posterior ciliary arteries; a possible role of inhibition of phosphodiesterase-5 in vascular smooth muscles by sildenafil was implicated. In a study conducted on 14 healthy subjects, 14 using color Doppler ultrasound imaging, 1 h after a 50-mg dose of oral sildenafil, a significant increase of mean flow velocity (MFV) was observed in the ophthalmic artery (OPA) but not in the central artery or short temporal posterior ciliary artery; no significant changes were found regarding intraocular pressure, color vision, or visual acuity in this study. However, Laties and Zrenner 15 reported that optic nerve head blood flow was maintained or possibly enhanced after treatment with sildenafil, even in the face of a reduction in perfusion pressure or systemic blood pressure. They favored a beneficial effect of using sildenafil under certain circumstances.
In view of the conflicting reports cited above, along with the paucity of attempts to investigate the impact of sildenafil on OPA vasoreactivity in type 2 diabetic patients, this study is therefore devoted to clarify this issue, using colored Doppler technique, which is safe and cost-effective.
Materials and methods
The exclusion and inclusion criteria 16 for diabetic patients and normal volunteers recruited in this study are listed in Table 1(a) and (b). Of note, this study is an extension to our previous article published in this journal where modulatory effect of sildenafil on middle cerebral artery (MCA) was investigated in the same subjects. 17
Inclusion and exclusion criteria for diabetic patients and normal volunteers enrolled in the study. 16

TIA: transient ischemic attack; MI: myocardial infarction; BP: blood pressure; COPD: chronic obstructive pulmonary disease; TCD: transcranial Doppler.
A total of 35 subjects participated in this study, after obtaining their signed consent and formal approval of the Ethical Committee of the Faculty of Medicine of Kufa University (No. 151 in 28/Sep/2008). They were divided into two groups: 17 healthy male volunteers with mean age of 45 ± 2.17 years (range = 33–58 years) and 18 male type 2 diabetic patients with mean age of 50 ± 1.35 years (range = 42–57 years). The mean duration of diabetes from the time of diagnosis was 11.3 ± 6.35 years (range = 3–24 years). The study commenced from 26 October 2008 and ended on 7 March 2009. The diabetic patients were selected from a diabetic clinic center, and were previously diagnosed according to World Health Organization definition of diabetes as fasting plasma glucose ≥7.0 mmol/L (126 mg/dL) or 2-h postload plasma glucose ≥11.1 mmol/L (200 mg/dL). 18 The selection of diabetic patients and normal subjects was according to certain inclusion and exclusion criteria (Table 1(a) and (b)). All participants were sent for detailed ophthalmological examinations, including intraocular pressure measurement and funduscopical and retinoscopical examinations. The diabetic patients were also sent for urine albumin, blood urea, and serum creatinine to exclude diabetic nephropathy. Full history and autonomic examination were undertaken to exclude diabetic neuropathy. Liver function tests were also performed for each participant to exclude liver disease. All patients underwent a full physical examination, which included blood pressure, a 12-lead electrocardiogram, and heart rate recordings. All participants were subjected to fasting biochemical laboratory tests, including blood sugar, lipid profile, and serum uric acid.
Protocol of transorbital Doppler examination
Doppler studies were conducted at 9:00 am after an overnight fasting, using Siemens Versa Plus Sonoline equipment (230 PAL version, Germany) with color flow and transcranial Doppler (TCD) facilities; a linear probe of 7.5–10 MHz 19 was used to insonate the OPA through a transorbital window. All subjects were allowed to rest quietly and examined in supine position. Before proceeding to the definitive recording, subjects were trained to perform the procedure of breath holding (BH) and hyperventilation (HV) correctly. Blood pressure, using Accoson mercurial sphygmomanometer (Accuson BP apparatus mercury, England, kochi.olx.in/accuson), and heart rate, using digital infra-red pulse-oximeter (Nonin pulse oximetry, Nonin Medical Inc., made in USA), were also recorded. To study the OPA blood flow velocities, in the first place, history was taken to rule out previous eye disease, for example, glaucoma, retinopathy, or eye surgery concerning intraocular lens implantation. A transorbital window was utilized, by placing the probe directly on the eye ball, keeping the head and neck straight. Care was taken to minimize the power of the equipment at the lowest level consistent with satisfactory recordings. A stretcher was used to support the handheld probe so that the probe just touched the closed eye lid. The subject was asked to breathe normally, and a sufficient length of OPA segment was then identified by color flow. To obtain baseline control OPA spectral wave form, pulsed wave (PW) Doppler sample volume was placed in the middle of the artery, at an angle of 0°&0x44; and the means of peak systolic velocity (PSV), diastolic velocity (DV), and resistive index (RI) of 10 cardiac cycles were recorded. To demonstrate the response of OPA flow to hypercapnia, the subject was asked to hold breath, as long as possible, after mild to moderate deep inspiration to avoid suffocation. The changes of blood flow of OPA to BH (BHopa) were calculated as the means of the above cited parameters during the last 5 s. To demonstrate the response of OPA to hypocapnia, the subject was asked to perform moderate HV for 1.5 min. Doppler spectral parameters of changes in OPA flow and the MFV of OPA to HV (HVopa) were calculated in the same manner as above.
A 50-mg sildenafil tablet (Sildenafil citrate, Sandoz product, Sandoz Canada Inc.) was then given orally, and a 45-min period was allowed to elapse to ensure optimal effect of sildenafil. Doppler examination was then repeated to record OPA blood flow changes regarding baseline control, and vasoreactivity responses, including BH and subsequent HV.
Calculation of Doppler indices
Doppler indices, including RI, MFV, breath holding index (BHI) and MFV, were calculated in the same manner described in our previous publication. 17
Statistical analysis
The data were expressed as mean ±SEM. Paired t-test was used to compare the difference between pre- and post-treatment of each group. Independent t-test was used to compare the difference between diabetic and normal groups. Statistical analysis was done by using computer program (SPSS) version 12. In all tests, p value < 0.05 was considered to be statistically significant.
Results
Effect of sildenafil on MFV of OPA in normal and diabetic persons
Before giving sildenafil, in both normal subjects and diabetic patients, the MFV of OPA was significantly decreased during BH (p < 0.05) and significantly increased during HV (p < 0.05).
After sildenafil, in both normal subjects and diabetic patients, there was statistically significant increase in MFV level (during baseline control, BH, and HV in comparison to those before sildenafil) (p < 0.05), as shown in Table 2 and Figures 1–3.
Effect of sildenafil on MFV (cm/s) of OPA in normal and diabetic groups.

MFV: mean flow velocity; OPA: ophthalmic artery; DM: diabetes mellitus.
p < 0.05.

Effect of sildenafil on MFV of OPA in normal and diabetic groups.

Doppler spectral wave form images of the OPA of diabetic patient showing the effect of giving sildenafil on OPA flow velocity during breath holding and subsequent hyperventilation. Top panel: (a) baseline control, (b) breath holding and (c) hyperventilation, before giving sildenafil. Bottom panel: after giving sildenafil (d) baseline control, (e) breath holding, and (f) hyperventilation. An increase of PSV and EDV with decrease of RI after giving sildenafil was evident.

Doppler spectral wave form images of the ophthalmic artery of healthy subject showing increased PSV and EDV, after sildenafil. (a) Baseline recording, (b) after giving sildenafil, (c) breath holding before sildenafil, (d) breath holding after sildenafil, (e) hyperventilation before sildenafil, and (f) hyperventilation after sildenafil.
Effect of sildenafil on breath-hold index and full range of vasodilatation (%) of OPA in normal and diabetic groups
There was no statistically significant change in BHI and full range of vasodilatation (FVD) of OPA (p > 0.05) after sildenafil in normal and diabetic groups (Figures 4 and 5).

Effect of sildenafil on BHI of OPA in normal and diabetic persons.
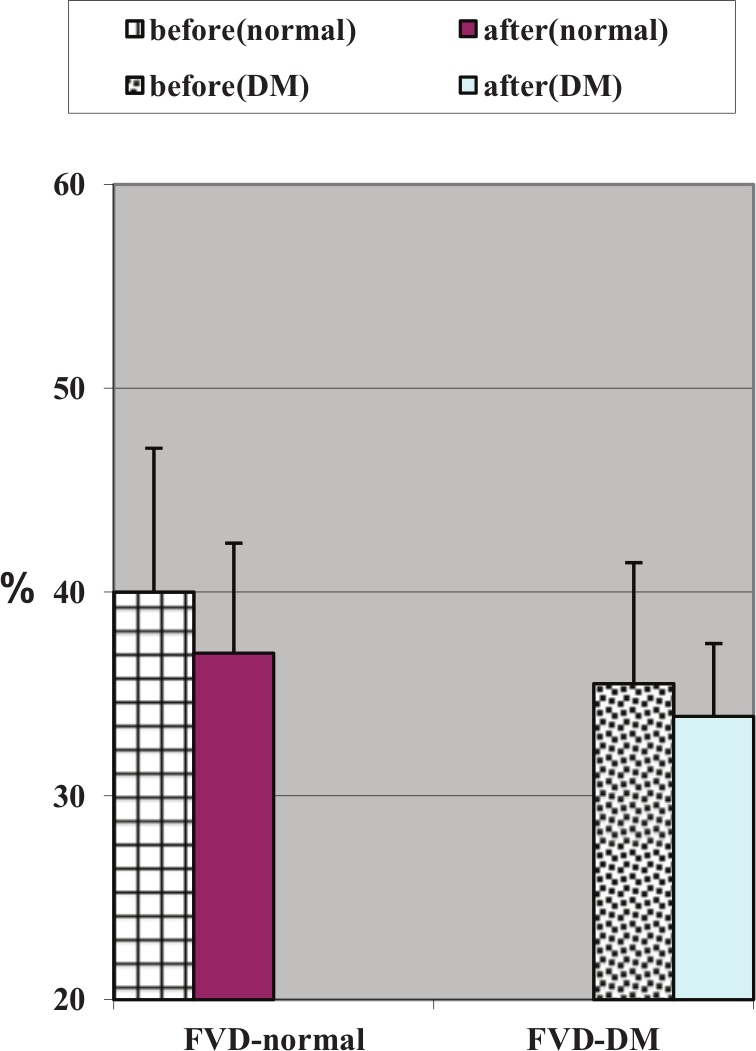
Effect of sildenafil on FVD of OPA in normal and diabetic persons.
Effect of sildenafil on RI of OPA
Before sildenafil, in diabetic group, during BH and subsequent HV, RI was found to be significantly higher than that in normal individuals (p < 0.05). After giving sildenafil, in normal individuals, no significant change of RI was found, whereas a significant decrease of RI occurred in diabetic patients (p < 0.05) (Table 3 and Figure 6).
Effect of sildenafil on RI of OPA in normal subjects and diabetic patients.

RI: resistive index; OPA: ophthalmic artery; DM: diabetes mellitus.
p < 0.05 (comparisons between normal individuals and diabetic patients before sildenafil) and *p < 0.05 (between normal individuals and diabetic patients before and after sildenafil).

Effect of sildenafil on RI of OPA in normal and diabetic persons.
Discussion
OPA vasoreactivity
The significant decrease in the mean OPA flow, of both systolic and diastolic elements, to hypercapnia, induced by BH, is in agreement with the Harer and Thomas 20 report, where significant decrease of OPA velocity in response to increase in end-tidal CO2 pressure by 5 mmHg was demonstrated. Conversely, this result is in conflict with that obtained by other investigators who demonstrated that hypercapnia induced by CO2 resulted in either no change in OPA flow 21 or increase of OPA flow, 22 whereas acetazolamide-induced hypercapnia resulted in consistent increase of OPA flow. 23 However, hypocapnia induced by HV resulted in highly significant increase of OPA flow, which accords with other reports. 21
The results of the present investigation demonstrated that the OPA behaves in a different and opposite manner from that of MCA, in response to hypercapnia or hypocapnia induced by physiological stimuli, as reported by other investigators.17,20,23 A reasonable explanation for these modulatory effects is perhaps due to the occurrence of “steal effect” during hypercapnia induced by BH, which is known to have a significant dilatory effect on the large cerebral blood vessels, resulting in reduction of flow velocity in the OPA. Conversely, during hypocapnia induced by HV, an “inverse steal” may occur, as HV has a profound constrictor effect on large cerebral blood vessels with the result of increased flow in the OPA. Furthermore, the finding of increased flow of the OPA on HV may be explained on the basis of the following contention: it is known that HV results in an increase of cardiac output through increase of heart rate and stimulation of pulmonary stretch receptors. As a result, “retrograde” flow in OPA occurs through many anatomic connections with branches of the external carotid artery. 24
Effect of sildenafil on OPA blood flow and reactivity
In both normal individuals and diabetic patients, sildenafil had no modulatory effect on OPA vasoreactivity but had evident effect on OPA flow velocity; it significantly increased both systolic and diastolic velocities of OPA, 45 min after drug intake. Similar results were reported in ocular Doppler studies, in healthy young subjects, 1 h after respective oral dose of 100 19 or 50 mg 25 of sildenafil; no significant increase in intraocular pressure was observed.25,26 The novel result of the present investigation is that sildenafil significantly decreased RI (an index of vascular resistance), only in diabetic patients.
This relaxant vasodilatory potential effect of sildenafil on OPA can be rationalized on the bases of the following mechanisms: it has been proposed that sildenafil may counteract the enhance endothelin (ET-1) activity that has been demonstrated to arise in type 2 diabetic patients than in healthy subjects.27–29 Furthermore, cGMP was found to be reduced in diabetic patients and in those with endothelium dysfunction; sildenafil increases the bioavailability of cGMP and improves endothelial dysfunction. 30 Moreover, sildenafil may stimulate the synthesis and transcription of endothelial nitric oxide synthase (eNOS) resulting in increased NO-generated guanylate cyclase activation, yielding an enhancement of cGMP formation.31,32 Additionally, similarities in many respects to sildenafil, between penile corpus cavernosum and choroidal vascular structures, have been postulated: the presence of the endothelium-derived relaxing factor, nitric oxide in the microcirculation can modulate the tone of pericytes, which are contractile cells outside the endothelial lining of capillaries.10,32 Thus, it can be inferred that sildenafil may exert a vasodilator effect on the choroidal vascular bed and may increase the volume of choroidal blood flow through reduction of arterial resistance by relaxation of smooth muscles.8,32,33
The decrease in RI may be favorable in reducing the risk of retinopathy on the ground that early changes in diabetic retinopathy are found to be coined with increased RI of ocular blood flow. 34 On the other side of the coin, there exist reports indicating that changes in ocular hemodynamics induced by high doses of sildenafil may have hazardous outcome in patients with disturbed ocular vessels resembling that in patients with diabetic retinopathy. 35
Conclusion
In this study, it was observed that sildenafil increases OPA blood flow velocity in both normal subjects and diabetic patients. OPA in type 2 diabetic patients has higher RI than that of normal subjects; sildenafil decreases the RI of the OPA in type 2 diabetes mellitus patients only. This vasodilatory effect of sildenafil may have a clinical utility in the prevention of diabetic microangiopathy.
Footnotes
Acknowledgements
A.A.Z. was involved in the setting up the design and protocol of the study and performed all Doppler examination. F.G. conceived the study, and participated in its design and coordination. N.R.H. participated in the sequence alignment and drafted the manuscript, design, and coordination. A.M. was involved in the preliminary writing of the manuscript and carried out most of the statistical analysis. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.