
Abstract
This article highlights the perennial problems posed by the interdental col as well as their consequences for patients’ dental health and for many aspects of general dentistry. When the interdental col is not considered properly during restorative procedures new problems can arise instead of resolving existing ones. Dental professionals must be constantly vigilant because any oozing of inflammatory gingival crevicular fluid, or frank bleeding, from the col regions can impact adversely on adhesive bonding, pulpal health, impression accuracy, and restoration cementation. This article emphasises the importance of patients accepting their responsibilities early on for gaining and maintaining their dental health by appropriate cleaning of their col areas. In addition, this article demonstrates practical and cost-effective adjustments of interproximal restorations that promote periodontal health. It highlights that restored teeth often need to be made anatomically different to natural teeth to reduce the likelihood of perpetuating problems of the col. Careful design and precise execution of interproximal restorations are both essential to prevent reproducing problems which often necessitated those restorations in the first place.
This article also provides some practical hints on restoring teeth near the interdental col which will become ever more important in general practice following the imminent banning of dental amalgam.
Learning Objectives
To highlight the importance of the interdental col when restoring teeth, and the consequences when this is ignored
To discuss pragmatic tools which can be implemented by clinicians to motivate patients to take ownership of their periodontal problems
To describe some clinical tips for clinicians which aid patients being able to undertake more effective cleaning of their col areas
To describe the importance of modifying existing and new restorations to help to prevent periodontal problems
Introduction: the challenges of the col
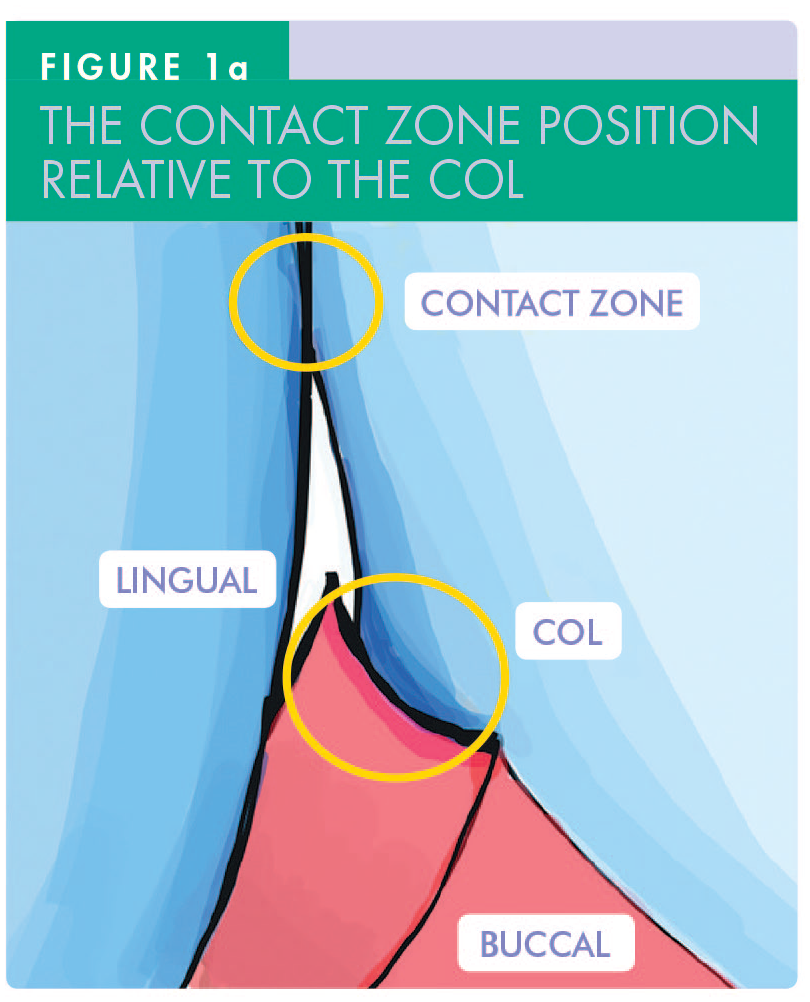
A col is a geographical term, referring to the lowest area between two hills. 1 The interdental (gingival) col refers to the interproximal concavity of gingiva which lies between the buccal and lingual papillae and beneath the contact zone of adjacent teeth (Figure 1a-b). The papillae are covered by keratinised epithelium, while the col has more vulnerable non-keratinised epithelium. The interdental col is often the first site for the development of significant periodontitis owing to the accumulation and retention of pathogenic plaque there. 2
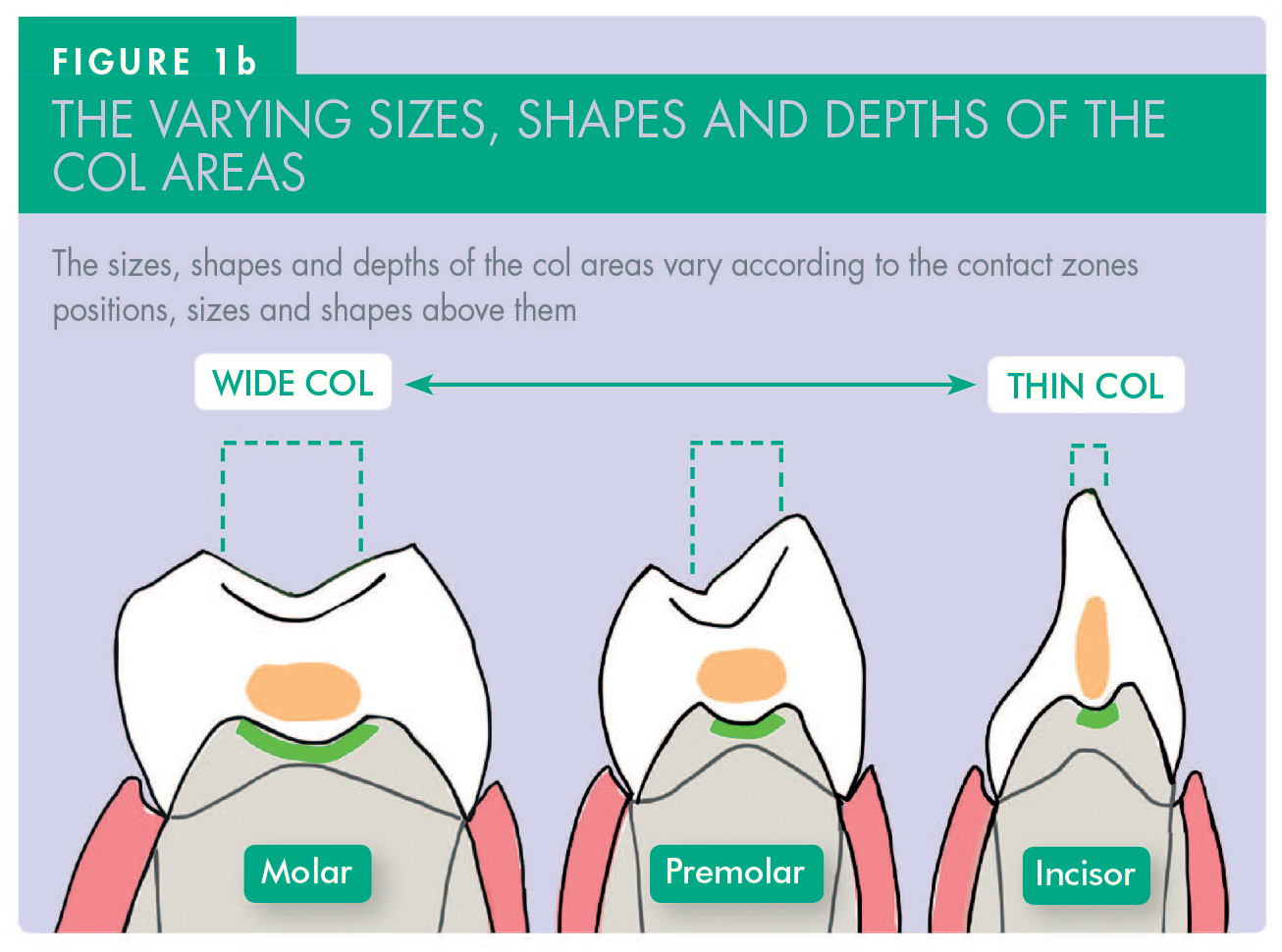
The sizes and shapes of the col areas are determined by the anatomy and positions of the teeth above them. The contact zones between incisors are narrower and taller than those between premolars, which are usually less wide than those between the much bigger molars (Figure 1b). Due to the vulnerability of those whole areas to continuing plaque-induced disease, it is prudent to reduce the size of the col areas when providing interproximal restorations – particularly when using resin composite because its surface free energy is high. Under-contouring of such restorations exposes the previous col area to much easier physical cleaning by the patient, thereby helping to prevent further diseases developing in that area.
Detecting and demonstrating disease in the col areas
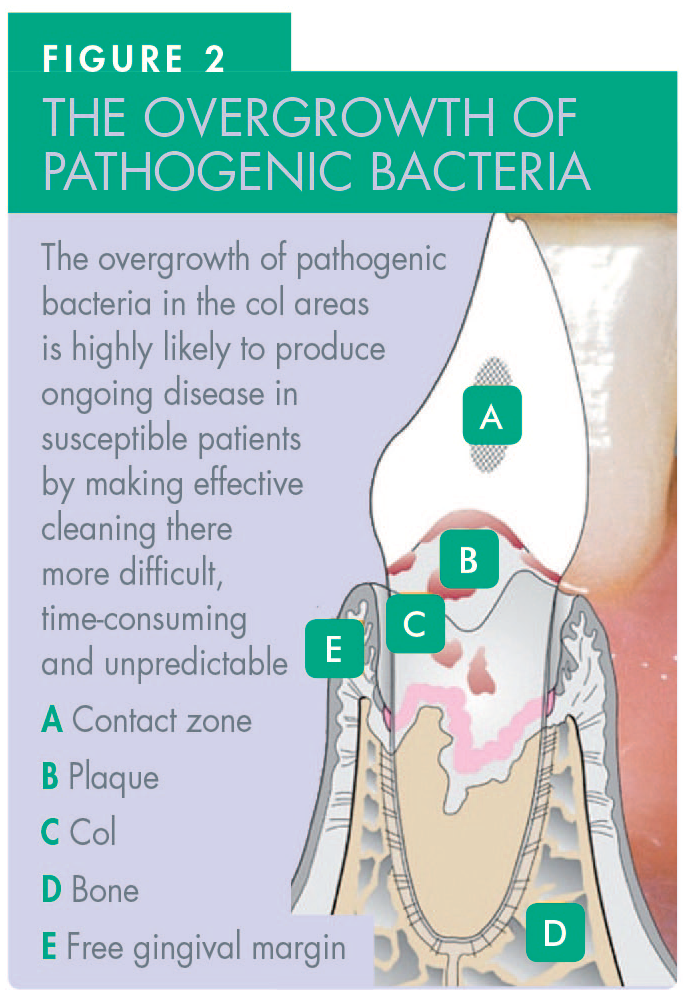
The type of dental disease that develops in the interdental col regions is related to a bewildering array of factors. The factors that cause periodontal disease to start, or that cause it to continue, include genetic susceptibility, 3 lack of effective interdental cleaning, smoking, poorly-controlled diabetes, stress, and various drugs, among other risks.3,4 The development of interproximal caries is largely dependent on the patient’s frequency of sugar intake, which influences the accumulation of cariogenic bacteria at or below the contact zones which lie directly above the col areas (Figure 2).
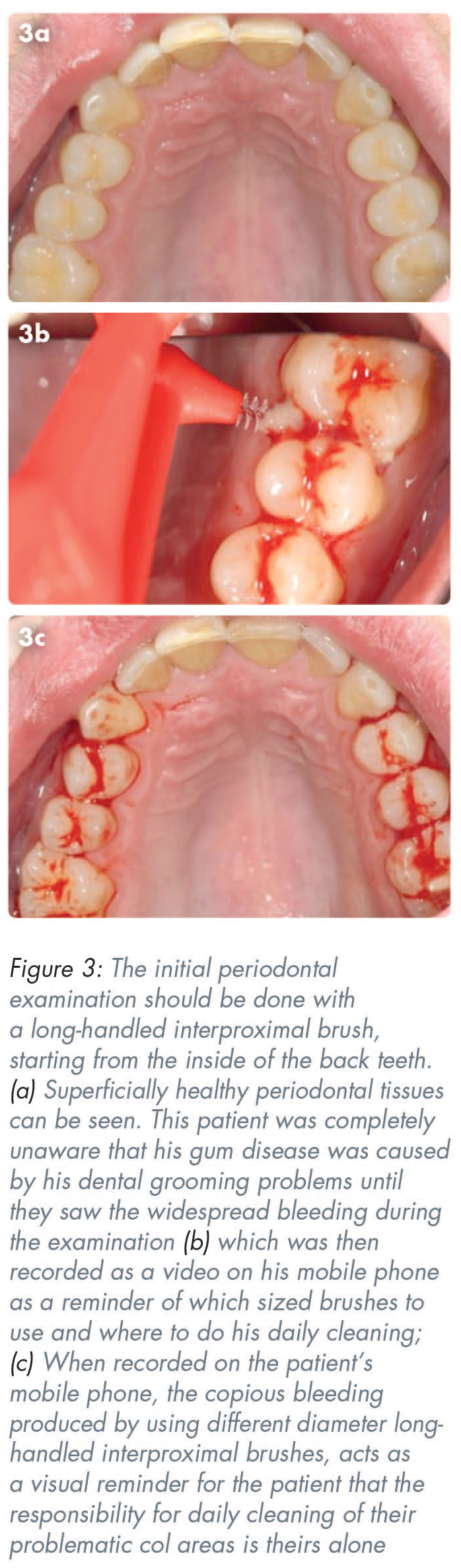
The recording of periodontal pocket depths is notoriously subjective and influenced by numerous variables such as the clinician’s skill, training, probe design, the force and angle at which the probe is used, as well as the severity of existing periodontal inflammation. Bleeding is a much better indicator of existing periodontal problems. 5 Bleeding is visually apparent to patients and can be demonstrated to patients using long-handled tapered interproximal brushes. Interdental brushes are more effective at biofilm reduction than floss, especially when appropriate sizes and shapes of interdental brushes are used. 6
Cleaning of the col by the patient
Once it has been confirmed from the patient’s history and the initial clinical examination that periodontal problems are present, permission should be sought from the patient to show them where their gum disease problems are. A slim, tapered
Doing this gently, while the patient observes the results with a hand-held mirror, or on a screen linked to an intraoral camera, will usually demonstrate bleeding from the
Making an illuminated video on the patient’s personal mobile phone using all their cleaning aids can be a highly effective tool, and readily retrievable record of what the patient needs to do to maintain their periodontal health when doing their daily home cleaning (Figure 3). 7 These videos can also be useful as medico-legal records to prove that patients had been counselled correctly about what to do about their periodontal problems.
The reason for using an interdental brush for this demonstration, rather than using a sterile periodontal probe, is that the periodontal probe is a surgical instrument to which a patient does not have access.
When a probe is used extensively during the initial periodontal examination, many patients can get the erroneous impression that their periodontal disease problems are primarily surgical in nature. This can lead some patients to assume that their gum problems need to be addressed with a surgical approach – or at least by another person such as by a hygienist, a dental practitioner, or periodontist – rather than by them. This is sometimes referred to as patients relying on an ‘external locus of control’ approach. An ‘external locus of control’ refers to the belief that the outcomes are largely determined by others rather than by the patient. By contrast, an ‘internal locus of control’ means that the person with the problems takes primary responsibility for resolving them. Unfortunately, not all dental professionals wish to challenge this common initial misperception in many patients, perhaps because of mixed emotions and understandable conflicts of interests.
Nevertheless, the patient needs to be made aware very early on, that it is their lack of effective cleaning of their col areas that is causing their problems, rather than it being primarily a surgical problem or one that is likely to be cured predictably by another person disrupting their biofilm every few months.
Histology and architecture of the col
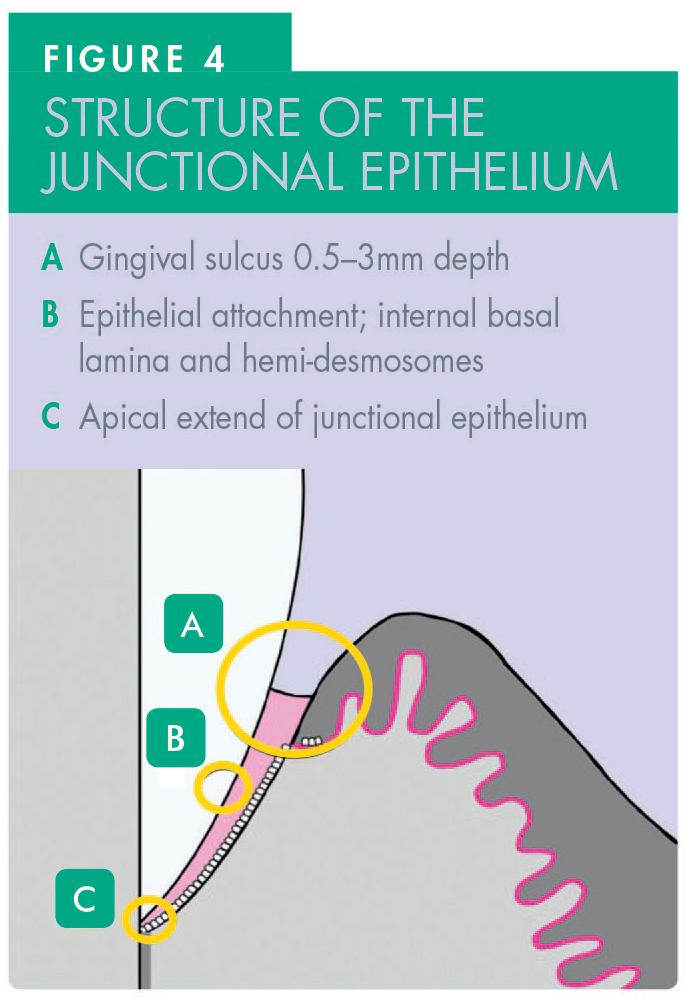
Schroeder and Listgarten 8 reported that the junctional epithelium is a non-keratinised, high-turnover epithelium characterised by expandable intercellular spaces (Figure 4). The fragile nature of this epithelium renders the col highly susceptible to invasion by bacteria, and their products produce varying amounts of inflammation and disease progression, depending on a variety of factors including patient susceptibility.3,4 Complex inflammatory processes in the highly vascular tissue below the epithelium release inflammatory exudate which can then pose major problems, particularly when dental professionals are trying to bond resin composite in that area.
Historically, what is now called the supracrestal tissue attachment (STA) was known as the ‘biological width’. The STA is composed of approximately 1mm of junctional epithelium and 1mm of connective tissue attachment coronal to the alveolar crest. 9 Depending on the periodontal phenotype, if restorations impinge on the STA, it can trigger a variable host response to recreate a distance between the restoration margin and the alveolar bone crest which can result in the loss of periodontal attachment. 9 This reaction can manifest as either gingival recession (in individuals with thin gingival phenotypes) or proliferative inflammation in those with thick gingival phenotypes. This makes the STA clinically relevant when positioning the margins of any dental restorations which should be kept supra-gingival, if at all feasible to do so.
Colonisation of the col area by various bacteria
Pathogenic plaque tends to accumulate in the col area because access for mechanical disturbance with routine cleaning aids is difficult. The contact zone forms the roof over the col area and that entire area can become colonised by different microorganisms depending on various factors (Figure 5).
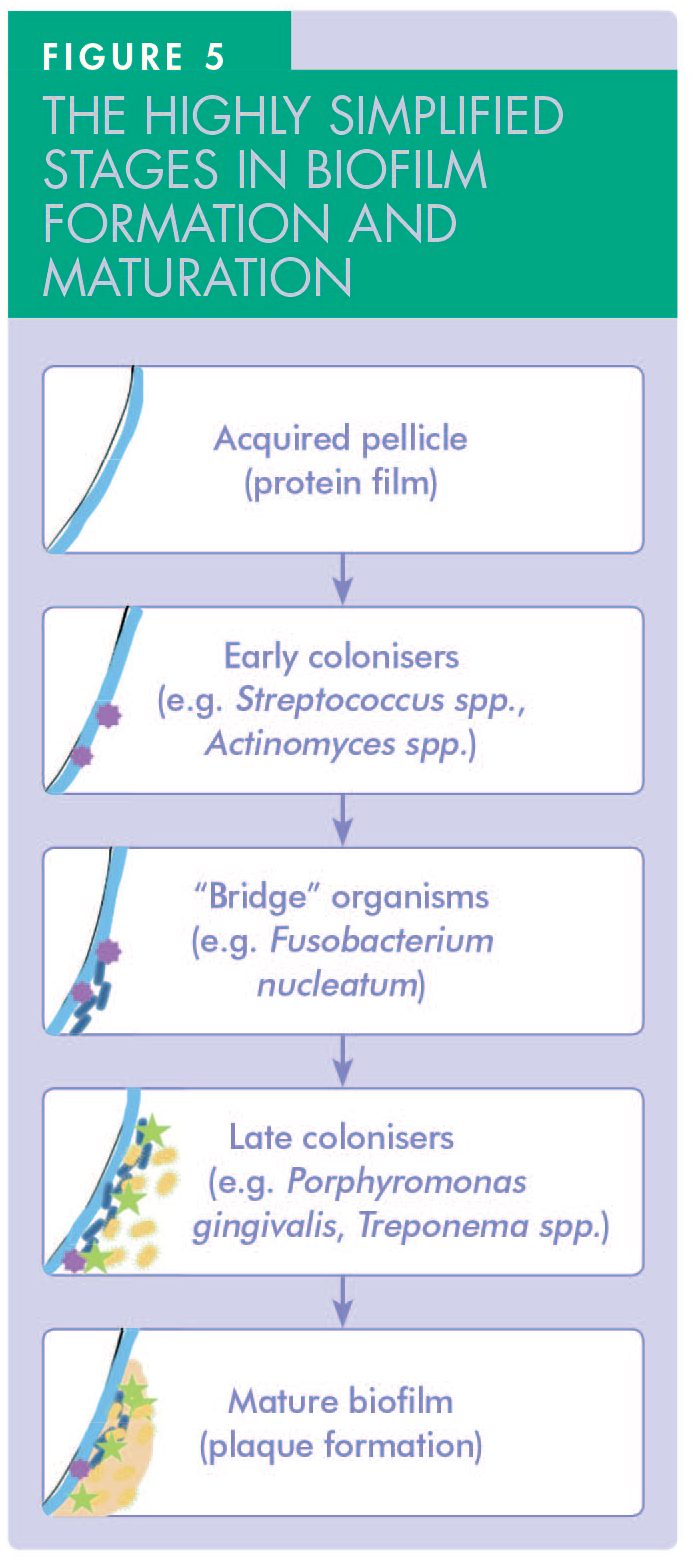
Initially, dental plaque is formed by Gram-positive cocci and rods, such as Streptococcus sanguinis and Streptococcus mitis. These early colonisers consume available oxygen, thereby lowering the redox potential of the environment and favouring the growth of more anaerobic rods and filaments such as Fusobacterium nucleatum, a Gram-negative rod known as the ‘bridge organism’, which facilitates the attachment of more fastidious Gram-negative anaerobes such as Porphyromonas gingivalis.
Primary colonisers bind to specific receptors in the tooth pellicle and each adherent bacterium then serves as a scaffold for secondary colonisers. If left undisturbed when interdental cleaning is inadequate for long periods, those micro-colonies develop into mature and pathogenic biofilms, often including Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans and Treponema denticola, a Gram-negative spirochete.4,10
Practical adjustments to existing restorations that aid patient cleaning of their col areas
The key objectives of re-shaping the existing interproximal surfaces and contact zones include:
The contact zone area should be on the buccal half of the tooth only. In other words, the interproximal restoration should be narrowed dramatically on its palatal/lingual aspect so that lingual papilla is not evicted, thereby leaving it enough space and reducing the size of the col area significantly.
The contact zones should be adjusted to be sited 1mm below the marginal ridges (Figure 6).
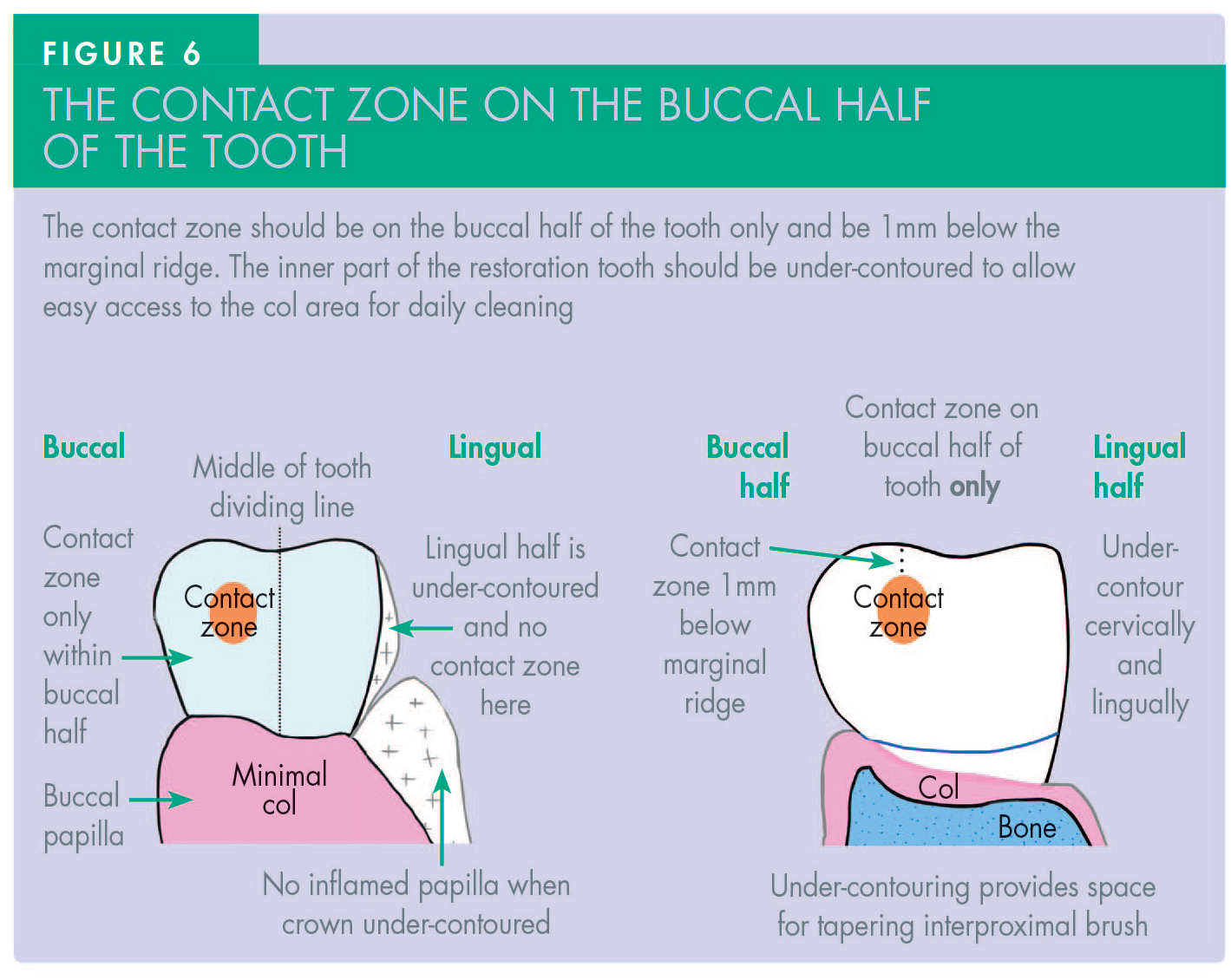
Doing this early on creates sufficient space for long-handled interdental brushes to be readily introduced from the palatal/lingual aspects of teeth, while allowing easier cleaning with single-tufted brushes being directed vertically into the inflamed gingival crevices. This restoration modification is particularly important when a material such as resin composite, whose surface has high free energy, is present. If the lingual or palatal papilla is very bulky/fibrotic it should be removed, following valid consent being granted by the patient. For this ‘papillectomy’, one can use the tip of a diamond bur run at very high speed, or a scalpel tip, laser, or electro-surgery.
Helpful tips and burs for re-contouring restorations and removing overhangs:
For smoother finishing of surfaces, use multibladed tungsten carbide burs, rather than diamond burs. However, tapered diamond burs are usually necessary to cut back any bulky ceramic present near the col areas.
A multibladed, needled-shaped, friction grip tungsten carbide bur (such as a Jet FG 7901 [Kerr™ Corporation, Kloten, Switzerland], Figure 7) is very useful for subgingival finishing of margins and for removal of any obvious overhangs to allow interproximal brushes to clean the col areas more easily. Extend the bur down into the free gingiva by about 1mm, while holding it at 45 degrees to the long axis of the tooth.

Provided the patient has been informed appropriately and given their consent, and the treatment is performed under local anaesthetic, it is quite reasonable to trade a small amount of short-term gingival bleeding for a much more cleansable col and interproximal area in the longer-term.
Many substantial overhangs and over-contoured existing restorations can be modified very quickly and smoothly using a Komet H48LQ bur (Komet Dental, London, UK) (Figure 8), thereby helping patients to clean the col areas with long-handled interproximal brushes without incurring the costs of replacement restorations. Although initially expensive, these burs are very durable, recyclable and usually last for a long time. They are also suitable for initial resin composite veneer shaping.
Practical challenges when managing caries near the col
The interproximal surfaces of teeth below the contact zones and above the col are susceptible to caries developing there due to the reduced accessibility for conventional tooth brushing. Risk factors for developing caries include the frequency of the patient’s sugar intake, the anatomy of the teeth and the pathogenicity of the bacteria accumulating there. Caries-causing bacteria, such as Streptococcus mutans and Lactobacilli, metabolise fermentable carbohydrates to produce acids which lower the pH and cause demineralisation of teeth. 11 When cavitation occurs sufficiently to justify interproximal invasive operative treatment, resin composite has become the material of choice for many patients and dentists. However, even if finished tediously and carefully near the col areas, resin composite usually has microscopic surface roughness and surface high free energy, which makes effective cleaning even more difficult for the patient.
The main challenge in ‘adhesive dentistry’ is that for any material to adhere, it must have a low contact angle, a clean surface and high free energy. Put simply, it should possess the opposite characteristics to a Teflon-coated saucepan whose surface has low free energy to prevent substances sticking to it during cooking, thereby making it easy to clean afterwards.
Bonding of resin composite near the col in deep interproximal carious cavities is fraught with practical difficulties. Etching, washing and drying is required to clean the surface for bonding materials to flow and adhere reliably and predictably there. However, these technically demanding processes often start microscopic crevicular fluid movement from any inflamed col area near the cavity, which then contaminates those critical surfaces before the adhesive bonding resins can set and seal the cavity effectively from bacteria and micro-leakage.
Deep carious cavities are often situated close to a vulnerable and often already partially inflamed pulp. Any micro-leakage caused by nearby crevicular fluid, blood or other fluids can be disastrous by interfering with effective bonding in the base of the box of the interproximal cavity. Bacteria and micro-leakage products in that area can then travel straight through the small amount of residual dentine and thereby tip the pulp into irreversible pulpitis with all the associated consequences and costs.
A serious drawback of using resin composite in deep interproximal cavities is that it has residual high free energy, meaning that bacteria, stains, and dyes can adhere tenaciously to the outer surface, especially in any minor defects or cracks within the surface of the material near the col. Beyond a threshold of around one micron, bacterial adhesion increases markedly, which then causes further hypertrophic inflammatory gingival problems, thereby perpetuating the problems for periodontally susceptible patients especially. In real life, achieving such microscopic smoothness interproximally is technically impractical.
Resin composite is notoriously weak in shear and tensile stress. Due to fears of composite chipping in the marginal ridge areas, many clinicians produce very wide interproximal contact zones which are often too close to the occlusal surface and which can make effective cleaning of their col areas much more difficult for patients (Figure 9).
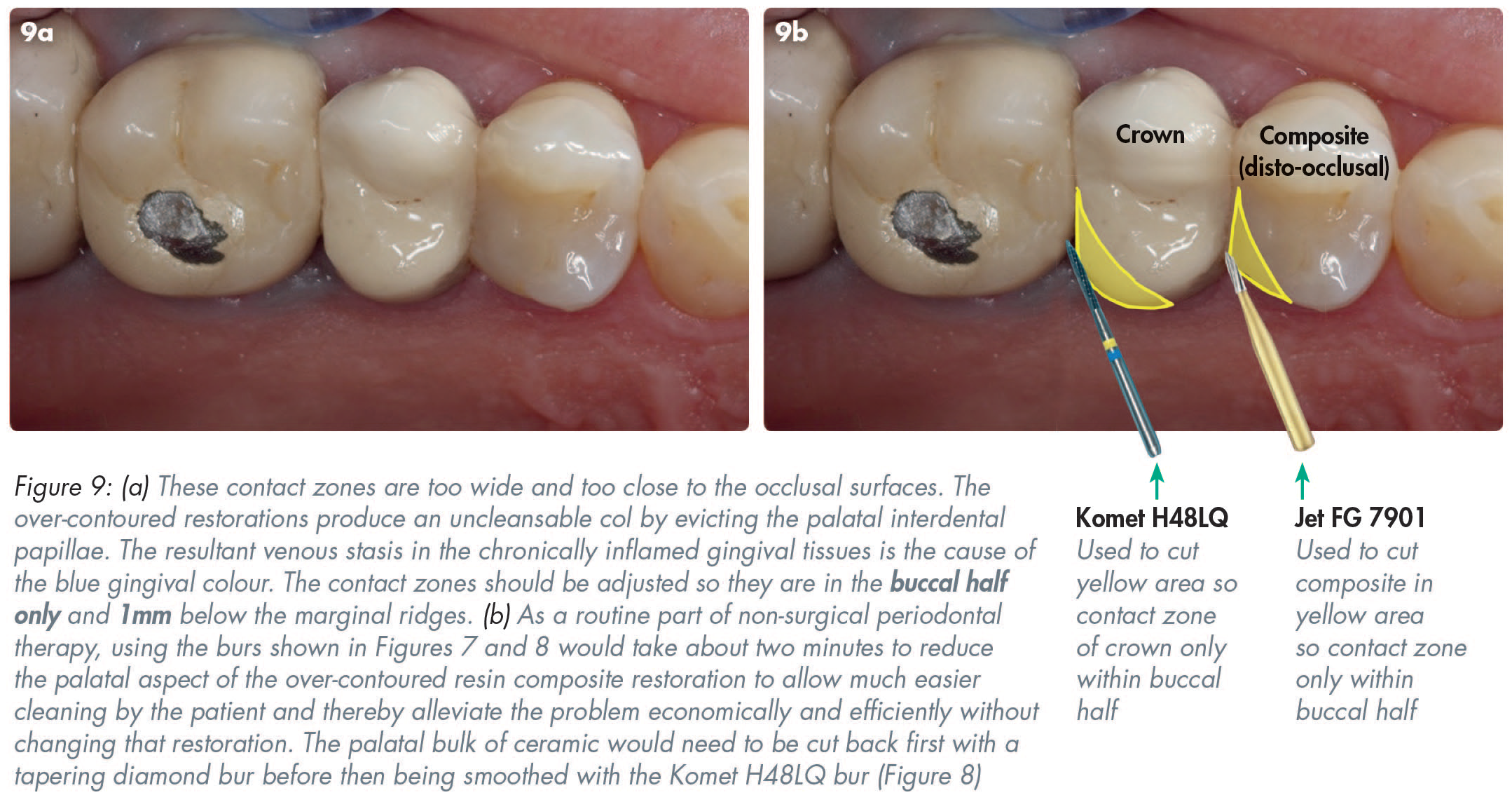
Increasing the bulk of interproximal restorations often evicts the interdental papillae laterally thereby providing sanctuary for pathogenic bacteria, fuelling inflammation there and making bacteria even more difficult to disturb with routine tooth brushing. Gradually, as acute inflammation ebbs and flows, fibroblasts appear in the inflamed granulation tissue in an attempt to promote healing and consequently the chronically inflamed gingival tissues often undergo hypertrophy. Depending on the gingival phenotype, the cyclical processes of simultaneous inflammation and attempted healing often persist, which results in noticeable gingival overgrowth with that ongoing problematic area usually being covered on the inside by bacteria of varying pathogenicity.
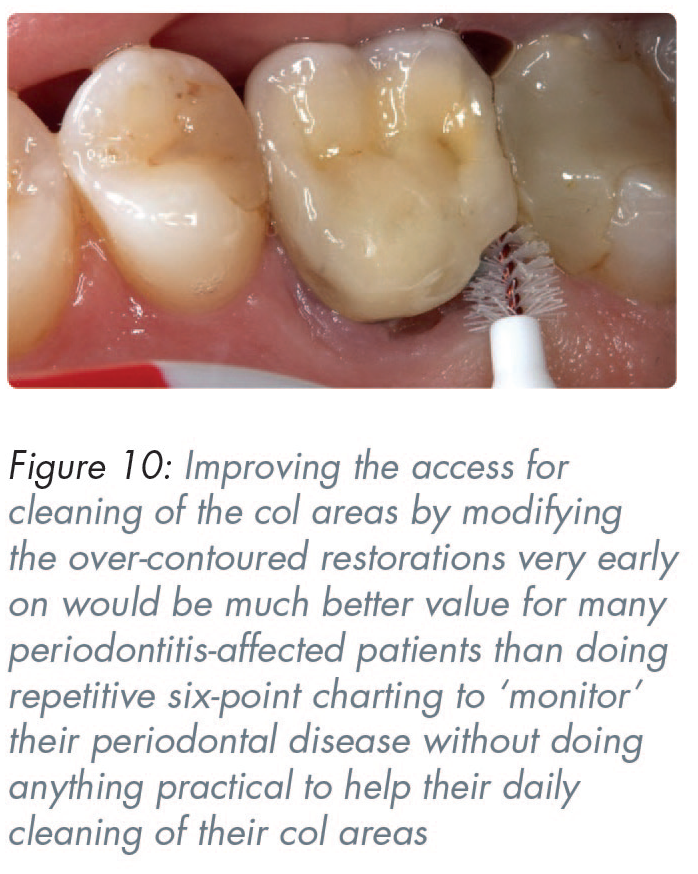
The only effective way to clean this massively over-contoured mesio-occlusal composite restoration is with a long-handled tapering interproximal brush (Figure 10). The mesio-palatal aspect should be cut back dramatically using the burs shown in Figures 7 and 8, to leave the contact zone on the buccal half of the tooth and 1mm below the marginal ridge. That would still stop food packing but would reduce the cleaning problems in the col area at minimal risk or cost. The distal ceramic of the crown could be cut back with diamond burs.
The new dangers with the imminent banning of amalgam
The imminent banning of dental amalgam means resin composite will become the default material for deep carious lesions. This is a significant new threat to many patients on low incomes, who are the most likely to have poor oral hygiene and a cariogenic diet. Amalgam, which is relatively tolerant of crevicular fluid and blood, will no longer be available to help such patients at moderate costs. Instead, they will only be able to have resin composite restorations which are technically much more difficult to place deep down interproximally. As discussed earlier in this paper, gingival crevicular fluid movement from the inflamed col and the interdental papillae area will often interfere with very technique-sensitive bonding and often create leaks directly opposite inflamed pulps, thereby resulting in pain and potentially pulpal necrosis with all those possible consequences.
In the absence of adequate subsidy in the English NHS’ Units of Dental Activity (UDA) system, it is very likely that many deeply carious teeth, which could have been restored pragmatically with amalgam, will now end up needing endodontic treatment or, much more likely, extraction. Molar endodontic treatment will not be feasible in the UDA remuneration system in most ‘NHS practices’ and consequently many deeply-carious-but-saveable-with-dental-amalgam teeth are likely to be extracted as an outcome of the probably well-intentioned amalgam ban, and produce yet another manifestation of ‘Merton’s Law of unanticipated consequences’. 12
Practical tips for minimising micro-leakage when bonding near the col
While treating deep interproximal caries, it is vital to prevent contamination of the interproximal box by gingival crevicular fluid or by blood, especially when trying to seal the very bottom of the subgingival box. These pragmatic tips can reduce pulpal sensitivity, improve marginal seal and clinical outcomes. Ideally, restorations should be kept supra-gingival and not impinge on the col in the first place, but cariogenic bacteria rarely comply with that laudable advice. The following practical tips are useful for minimising micro-leakage when bonding near the col.
Protect the adjacent tooth from acid etching by using a
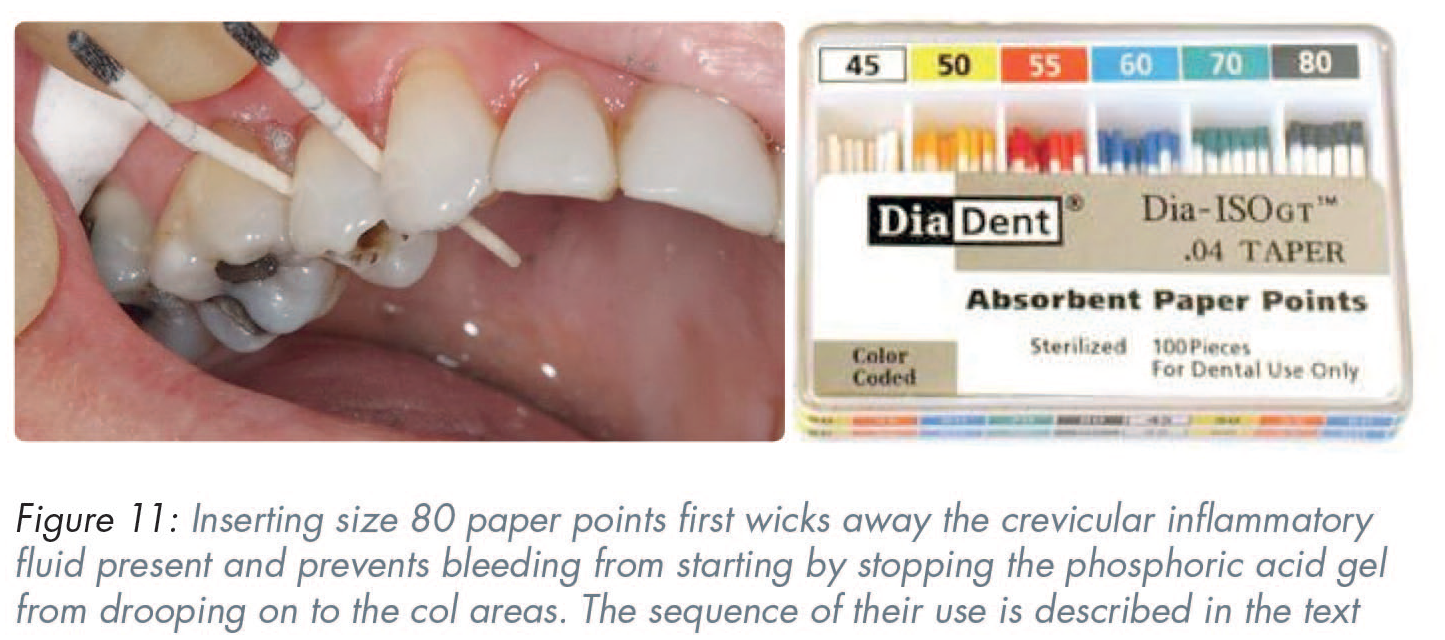
Place a large paper point (size 80–100) below the contact zone, similar to the placement of a wedge (Figure 11). The paper point will wick any crevicular fluid away sideways.
Use a fine needle and
Once the gel has been
Apply a low viscosity hydrophilic adhesive bonding agent to the clean, dried cavity which will then be wicked downwards and away by the new dry paper point.
Replace the paper point.
Apply and
Place the preferred resin composite in small increments
Build up the restoration in incremental segments to the correct shape – including having the contact zone in the
The preferred outcome should be that restorations are under-contoured on their lingual/palatal sides to minimise col size, thereby enabling the patient to clean the
Incurring worse col cleaning problems with fixed prostheses?
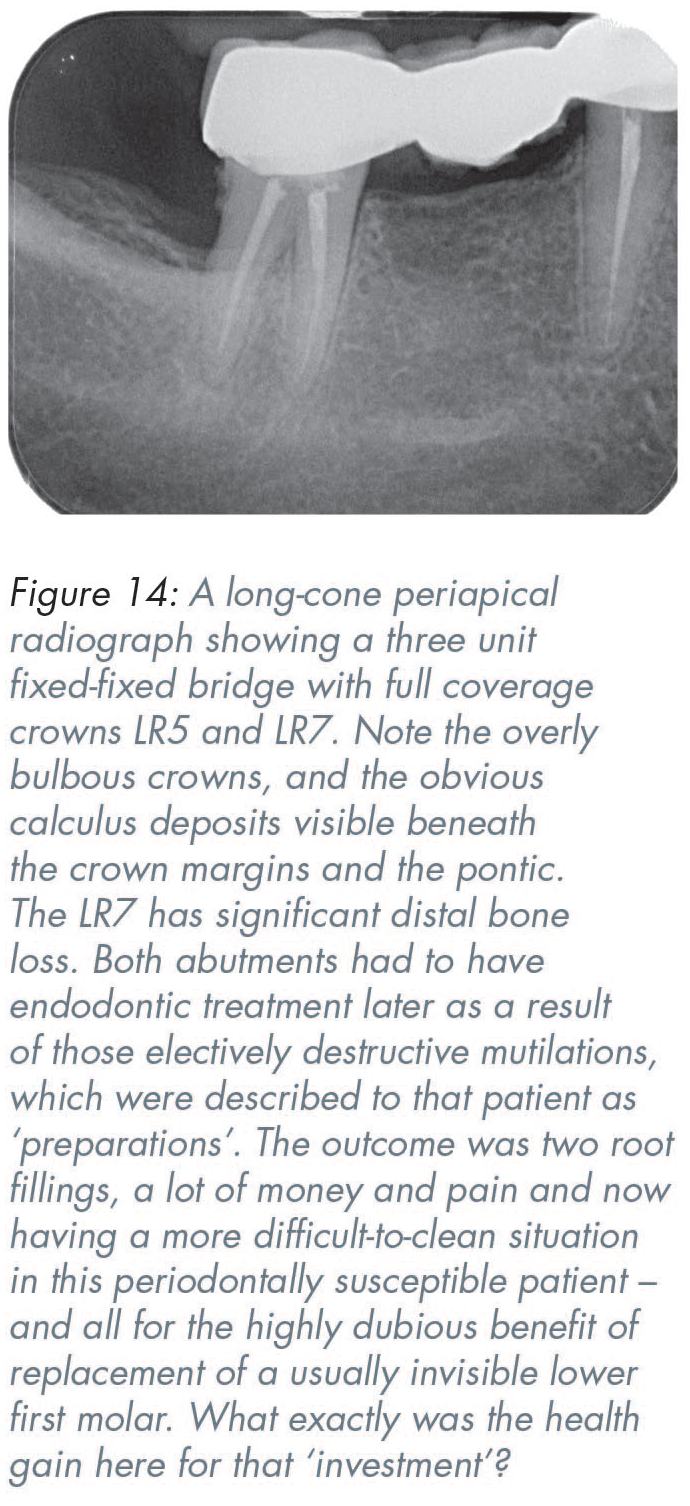
The traditional teaching is that most missing back teeth ought to be replaced to prevent drifting, tilting, overeruption and ‘disruption of the occlusion’. However widely-believed those well-meaning exhortations might have been, the sad truth is that many extensive fixed prostheses make it more difficult for patients to clean their col areas easily, thereby unintentionally favouring the growth of mature undisturbed biofilms and Gram-negative anaerobic species (Figure 14). In many such cases, patients are often missing those teeth because of a history of poor cleaning. Individual teeth are a lot easier to clean than frequently over-contoured full-coverage bonded crowns with a complicated shaped pontic between them, which can accumulate pathogenic plaque and sometimes calculus around them.
The col and ceramics in ‘cosmetic dentistry’
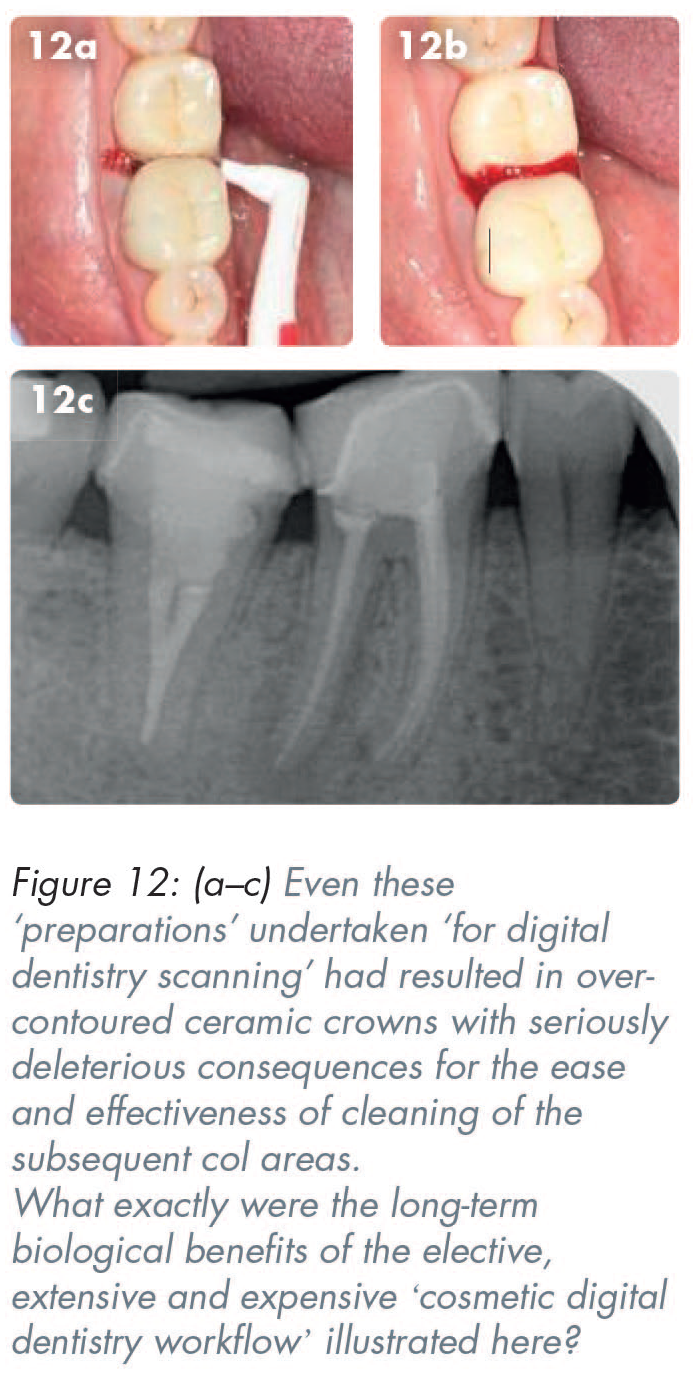
Ceramic restorations, such as veneers, crowns, and bridges, are often used in the euphemistically-termed ‘just cosmetic dentistry’, but, because of their brittle nature they all require sufficient material thickness to avoid failure in clinical service. Many enthusiastic ‘cosmetic’ dentists seem to remain blissfully unaware that if one deforms brittle ceramic by more than 0.2%, it breaks. In clinical practice, the failure to remove the required 63–72% of the tooth to provide adequate space for the bonded-ceramic restorations, including what is required for the substrate (whether that be metal, zirconia or other material) as well as enough thickness of the veneering ceramic, often leads to seriously over-contoured restorations. 13 (Figures 9, 10, 12-14).
‘Merton’s Law of unanticipated consequences’ 12 is often invoked and highly relevant when prescribing full coverage all-ceramic or ceramic-veneered restorations. Put simply, Merton’s Law means that in attempting to address the patients’ often understandable aesthetic concerns, the consequent over-contouring of zirconia/all-ceramic crowns frequently creates ‘unanticipated consequences’ of producing new disease in the col areas by making them very much harder to clean than their previously often reasonably intact and unprepared teeth.
Significant over-contouring of pressed ceramic, or other ceramic-veneered materials often displaces the previously healthy interdental papillae and thereby creates a wider and more difficult-to-clean col area. Even though the inside surfaces of many teeth are normally invisible, the over-contoured ceramic placed there often produces consequential gingival inflammation in the col areas and the inside of many bonded metal crowns, thereby perpetuating the cleaning problems (Figures 10, 12-14).
Thin periodontal biotypes often show their profound dislike for any adjacent restorations by receding. 14 Moderate and thick periodontal phenotypes can produce a pronounced inflammatory response, often presenting as florid, red, and bleeding erythematous tissues with intermittent flare-ups occurring alongside attempts at healing (Figures 10, 12, 13).
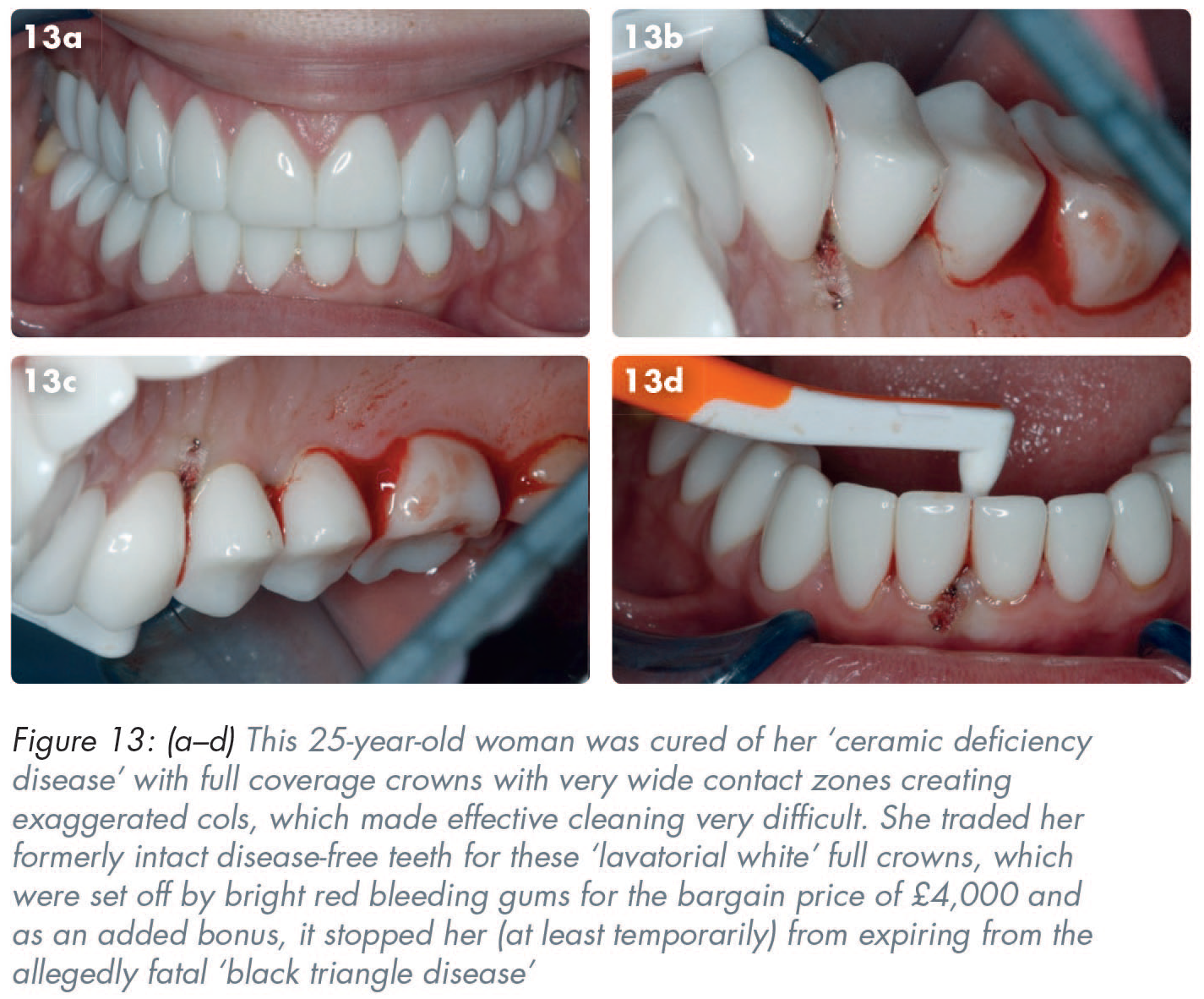
Some ‘influencers’ convince gullible or some self-absorbed narcissists to cure their perceived problems of not having a ‘perfect smile’ with a holiday in Turkey to acquire some ‘Turkey teeth’ which involves curing them of an imaginary ‘ceramic deficiency disease’ (Figure 13). 15 Those monochromatic ‘lavatorial white’ restorations are usually not all that difficult to detect because many could blind a polar bear at 40 yards, particularly as they are often framed by voluptuously filled lips and matching bright red gums as a result of the very wide interproximal contacts creating difficult-to-clean ‘bleeding cols’.
Summary of practical solutions
The col area of the interproximal gingivae is hugely important in the development and possible progression of dental diseases.
The col area is difficult to access with ordinary tooth brushing.
Long-handled brushes with a tapered design of appropriate diameters are highly effective at cleaning the col areas, provided they are used from both the lingual and buccal aspects.
Periodontally-susceptible patients should be shown how to use those brushes very early on and informed of their responsibilities for removal of their recurring biofilms in their col areas.
Over-contoured interproximal restorations ought to be modified substantially as an early and integral part of ‘non-surgical periodontal therapy’ by using the appropriate diamond and tungsten carbide burs to increase access to the col areas from the lingual/palatal aspects for daily cleaning by the patient.
New resin composite interproximal restoration should be delayed for up to a month after patients have been using the correct interproximal brushes in order to minimise gingival fluid exudate possibly contaminating composite restorations if they are anywhere near the gingival margins.
Conclusions
This article highlights some of the various challenges general dental practitioners face on a daily basis. Patients need to better understand the importance of them cleaning their own interproximal areas effectively. Adjustment of existing over-contoured restorations to improve access for easier cleaning is relatively simple, quick and very beneficial for patients in the longer-term. New posterior restorations should be under-contoured lingually/palatally and have their contact zones in the buccal half or the teeth only and be sited 1mm below the marginal ridges.
The well-intentioned banning of amalgam is likely to produce perverse outcomes and unintended consequences, particularly in patients from poorer communities who are most likely to have highly cariogenic diets, and many of whom rely on some dubious and reduced state subsidy for their dental treatment. Following the imminent banning of amalgam, it is recommended that dentists apply the clinical tips outlined above to ensure effective bonding in the col areas and help avoid perpetuation of pulpal and periodontal problems by not creating over-contoured resin-composite restorations in the difficult-to-isolate ‘bleeding col’ regions.