
Abstract
Increasing difficulties in recruitment and retention of dentists and dental care professionals in general dental practice in the UK is affecting delivery of NHS dental services. Reports of dissatisfaction among the general dental practice workforce indicate there is a significant risk to the future dental workforce supply which will affect access to dental care and worsen oral health inequalities. Understanding the factors related to job satisfaction and dissatisfaction of dental professionals would be useful in managing recruitment and retention issues and ensure a dental workforce exists which is able to meet the needs of the population. The aim of this literature review was to identify factors which contribute to job satisfaction and dissatisfaction of clinical staff in general dental practice. Database searching was conducted systematically through PubMed/Medline, Scopus, Ovid, and the National Grey Literature Collection. Part 1 of this two-part series discusses the factors relating to dentists. Twenty-two relevant articles were identified, which were qualitatively analysed using Herzberg’s motivation-hygiene theory as an analysis tool. Target-driven and restrictive contractual arrangements are a major factor contributing to dissatisfaction of dentists, as well as time pressures, poor quality equipment, and unfair remuneration. Dental contract reform should aim to minimise factors contributing to dissatisfaction and increase factors which increase satisfaction, if sufficient numbers of dentists are to be persuaded to continue to provide state-funded dentistry.
Learning Objectives
• To understand the concepts and principles of Herzberg’s motivation-hygiene theory and its application in the context of job satisfaction of dentists
• To identify existing factors that contribute to dentists’ job satisfaction according to the motivation-hygiene theory
• To synthesise the existing literature to provide a summary of factors for stakeholders to consider in contract reform
Introduction
There are widespread reports of issues in the recruitment and retention of dentists and dental care professionals (DCPs) in general dental practice in the UK, particularly affecting delivery of NHS dentistry.1-4 These issues have been exacerbated by the Covid-19 pandemic which has caused a backlog of missed dental appointments, and by Brexit which has increased barriers to overseas dental professionals practicing within the UK.2,5
Access to dental care is a determinant of oral health which enables delivery of preventative care and early intervention on dental disease, with the aim of improving health and reducing social care and wider economic costs. 6 The ageing UK population are retaining their teeth for longer, requiring more complex dental care and placing greater demands on the dental workforce and provision of care.7,8 Access to dental care has become an increasingly significant issue in the UK, due to the number of dental practices closing or becoming fully private, which is a barrier to people who are unable to afford private dental care and has a greater affect on people from lower socioeconomic backgrounds.9,10 If dental practices are unable to fill vacancies or retain dentists and DCPs in NHS practices, people will not be able to access affordable dental care. 11
The increase in unfilled vacancies in general dental practices, especially NHS practices in remote and deprived areas, and reports of dissatisfaction among dental professionals indicates there is a significant risk to the future dental workforce supply.1,12 If dentists continue to leave NHS dentistry, this will worsen the existing access to dental care and increase oral health inequalities, exacerbating what is already a significant public health problem. Understanding factors which predict job satisfaction within general dental practice in the UK would be useful in managing recruitment and retention issues and in designing acceptable dental contracts, thereby ensuring a dental workforce able to meet the needs of the population.
Theoretical framework
Recruitment and retention of individuals within a workforce are associated with job satisfaction.13-16 There are many different definitions of job satisfaction; the most accepted being positive or negative feelings an individual has toward their work. 17 Job satisfaction is a significant factor in a person’s intention to leave their job, which is highly predictive of this behaviour.18-20 In addition, high intention to leave also has negative effects on an individual’s engagement with their work. 21
The Herzberg motivation-hygiene theory (Table 1) suggests that job satisfaction and dissatisfaction exist on separate continuums affected by different factors.22,23 Two independent processes occur: one where people feel good or satisfied about their work and another where they feel bad or dissatisfied. The presence of “motivators” increases job satisfaction, but their absence does not increase dissatisfaction.23,24 Improving “hygiene factors” (the term used by Herzberg to describe factors that prevent job dissatisfaction) can prevent job dissatisfaction but does not contribute to job satisfaction. 23
Herzberg motivation-
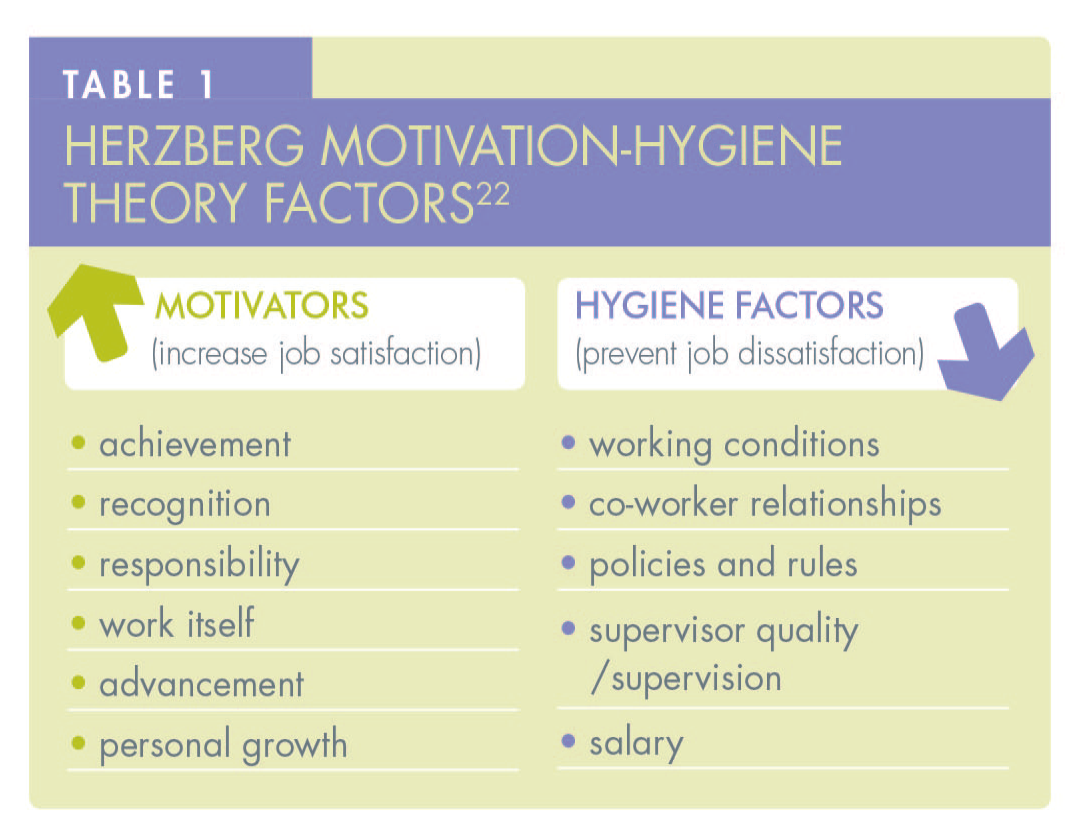
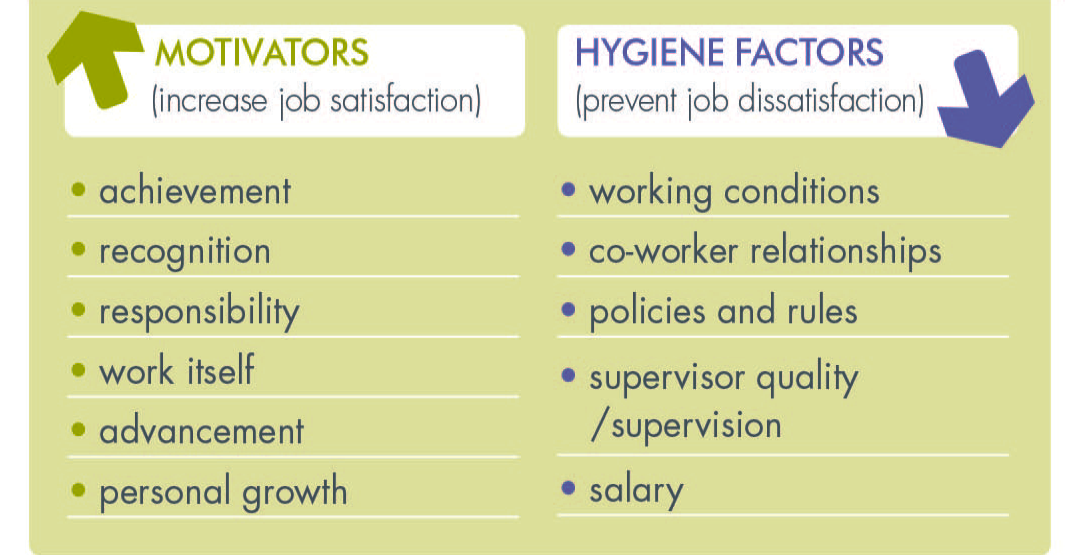
Herzberg’s motivation-hygiene theory is a useful tool in predicting job satisfaction and has previously been applied in other healthcare sectors to understand recruitment and retention of healthcare workers.14,16,25
The aim of this literature review is to identify specific factors which currently contribute to job satisfaction and job dissatisfaction of dentists in general dental practice.
Methods
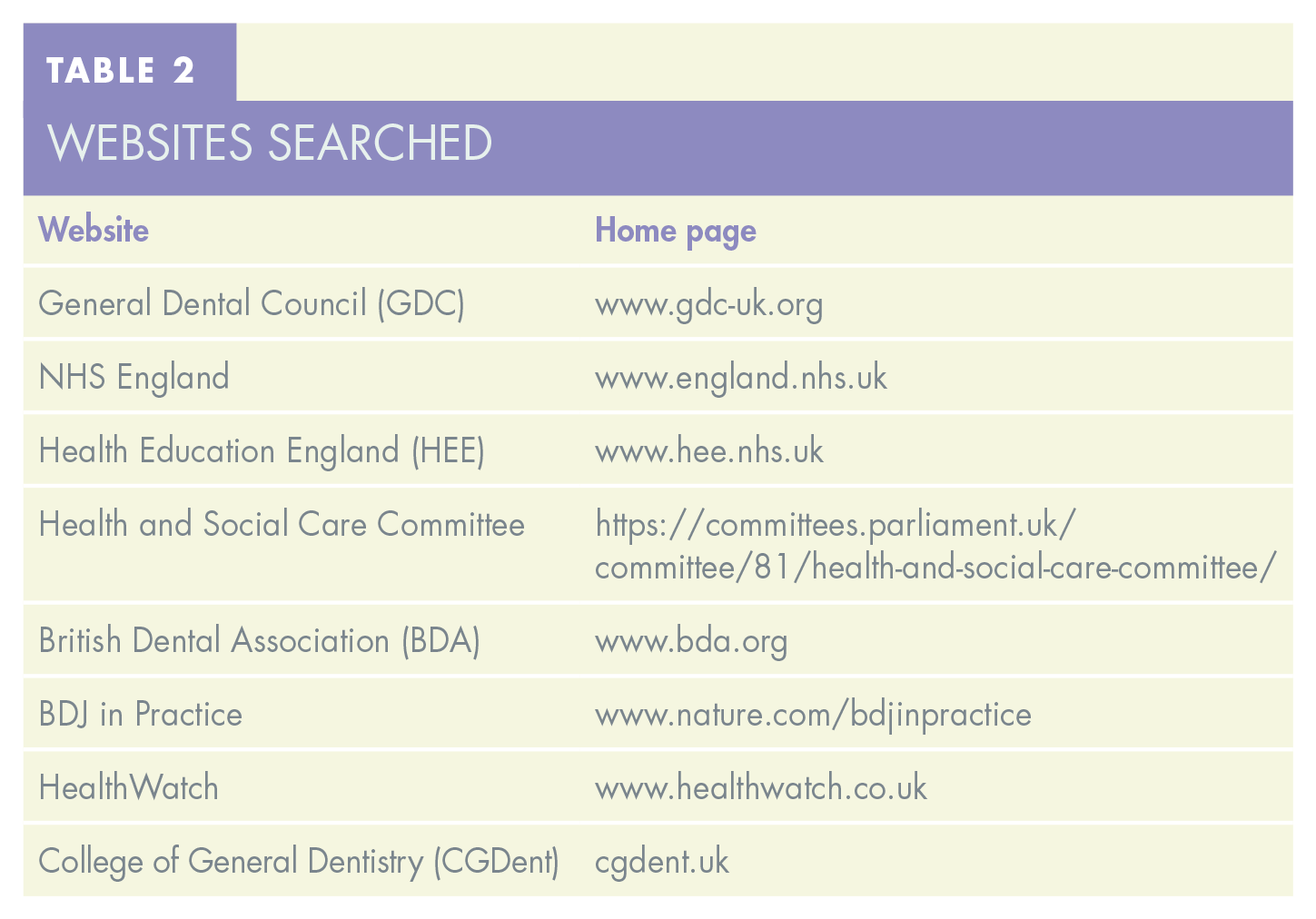
This research was conducted in a narrative literature review format. 26 Multiple sources of literature were searched to better understand the issue through a broad range of experiences, values, and perceptions. Electronic searches of databases (PubMed, Scopus, Ovid and National Grey Literature Collection) and website searches (see Table 2) were conducted to identify relevant literature. Inclusion criteria comprised any published or grey literature discussing job satisfaction, dissatisfaction, retention or recruitment of dentists in general dental practice/primary dental care after 1st April 2006. Systematic searches were carried out in June 2022 and updated in May 2023. The full search strategy can be found in Appendix 1, at the end of this paper.
Websites searched
Eligibility
To determine eligibility of records, inclusion and exclusion criteria were developed using the Sample, Phenomenon of Interest, Design, Evaluation, Research type (SPIDER) tool (see Appendix 2). 27
Study selection and data extraction
Studies identified through the search strategy were screened by the lead author (JAH) and assessed against the eligibility criteria. Selected reports were retrieved and reviewed independently by both authors. A data extraction template was designed using the Herzberg motivation-hygiene theory as a framework to ensure a consistent approach to data extraction, ensure transparency, and enable ease of synthesis of findings. The following data were extracted from each article: author, year, type of article/study, short description of study, dental professional group, motivation factors mentioned, hygiene factors mentioned, and any other factors discussed.
Risk of bias assessment
This review included a diverse range of study methodologies, opinion and grey literature, therefore distinct appraisal instruments were used to critically appraise each record. 26
For cross-sectional studies, the Joanna Briggs Institute (JBI) checklist was used. 28 Cohort studies were appraised using the Critical Appraisal Skills Programme (CASP) checklist for cohort studies. 29 For qualitative reports, the NICE quality appraisal checklist for qualitative studies was used. 30 Grey literature and opinion articles were appraised using the AACODS (Accuracy, Authority, Coverage, Objectivity, Date, Significance) checklist. 31
These tools were used to produce summary evidence quality judgements of low, moderate or high risk of bias for each included article.
Results
Included records
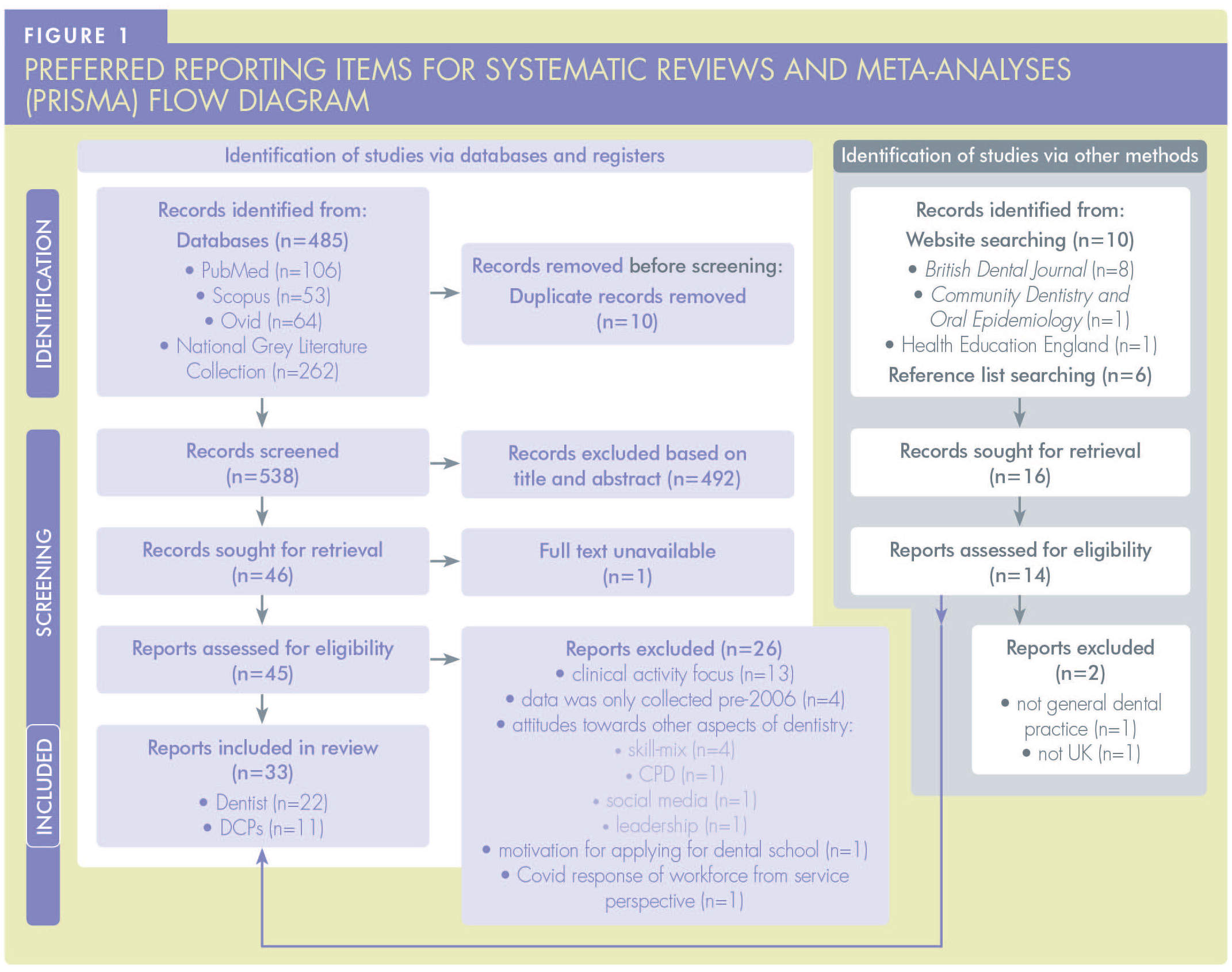
Database searches, carried out in June 2022 and repeated in May 2023, identified 548 records. Following removal of duplicates and screening of titles and abstracts to identify relevant records, a total of 46 reports were retrieved for full text screening. The full text of one record was unavailable, and therefore excluded from the review. Following review of full texts, 26 reports did not meet eligibility criteria and were excluded.
Searching via other methods (reference lists of included records and website searching) identified 16 reports, 14 of which were eligible for inclusion. Therefore, a total of 33 reports were included (Figure 1). Twenty-two reports were relevant to dentists (Table 2) and are discussed in this article. The 11 reports relevant to DCPs are discussed in Part 2 of this series, “It’s not just about the money: recruitment and retention of clinical staff in general dental practice – part 2: dental care professionals” (see pages 55–63).
Included reports had high methodological heterogeneity therefore it was not appropriate to attempt any quantitative synthesis or meta-analysis. The papers are presented through a narrative synthesis.
A summary of the included studies is provided in Table 3. The agreed “motivator” and “hygiene” factors influencing job satisfaction identified in reviewed literature are presented in Table 4.
Descriptive summary of included studies relating to dentists
Summary of factors relating to job satisfaction and dissatisfaction of dentists
Risk of bias
All the reports included in this review were individually assessed for risk of bias using the appropriate quality assessment tool described in the Methods, and a summary judgement made of low, moderate or high risk of bias (Appendix 3). Factors which only appeared in articles determined to be at a high risk of bias were excluded from the summary table (Table 3).
Discussion
The purpose of this literature review was to identify specific factors that contribute to job satisfaction and prevent job dissatisfaction of dentists in general dental practice. This review found that there may be factors specific to certain groups, e.g. females and those at different ages and career stages.
The most prominent overall factor associated with job dissatisfaction found in this literature review was working under target-driven, inflexible, and restrictive contractual arrangements, which was mentioned in over half of included reports. The majority of these were in relation to NHS arrangements in England and Wales. The risk of dentists leaving the NHS to go private due to the focus on targets over quality was an issue raised in an independent review of NHS dentistry in England and Wales in 2009, and there have been minimal changes in contractual arrangements since then. 54 A previous report on the motivation level of dentists by NHS Digital found that motivation level is inversely correlated with the amount of NHS work carried out. 49 However, dentists in Scotland have higher morale and provide more NHS dentistry compared to dentists in other countries of the UK. 49 There is evidence suggesting that fee-per-item payment models, such as those in Scotland, are associated with more clinical activity and less preventative advice.55,56
The present study identified that providing quality care and helping people increases job satisfaction of dentists,45,47 however it is reportedly difficult to provide good quality of care within the “framework” of the NHS.43,44 Some dissatisfaction (hygiene) factors which featured in the present review, such as unfair remuneration for work done under the NHS,44,49 inadequate time to spend with patients,35,42,43 and lack of access to/no investment in quality equipment,37,47,49 may be consequential of NHS contractual arrangements.
In July 2022, NHS England announced marginal changes to the English dental contract for 2022/2023, including introduction of a minimum Unit of Dental Activity (UDA) value and increasing the number of UDAs claimable where the course of treatment involves three or more teeth, or for complex procedures such as root canal treatment. 57 These changes may reduce dissatisfaction of dentists regarding remuneration under the NHS contract but do not increase access to dentistry.44,49
Time pressures are cited as a source of stress for dentists and can impact a dentist’s ability to provide quality care to their patients, which can lead to poorer care outcomes.58,59 In the present study, time was a factor mentioned frequently in relation to working in NHS dentistry.35,36,43 Earning potential is linked directly to the amount of time taken to complete a course of treatment. 60 Autonomy/control over work was a commonly mentioned satisfaction (motivator) factor in the literature examined in this review.35,38,44,46,47
Associate dentists have little influence over the equipment they are provided with by the owner of the practice. 47 There are many stresses faced by practice owners associated with running a dental business and the business aspect of dentistry has previously been described as a source of moral tension due to the conflict between asking patients for money and providing healthcare.41-43,61 Increasing bureaucracy and regulation has been previously cited as a barrier to investment by practice owners. 62 Dental practices with poor quality equipment are not attractive workplaces.37,47,49
Younger dentists are less satisfied and feel more restricted by contractual arrangements to be able to provide quality care.35,38 Career plans, particularly of newly qualified dentists, may be influenced by employment benefits such as annual leave, parental leave, and sick pay.33,50,51 Self-employment is the traditional status for dentists working in general practice, but the Covid-19 pandemic highlighted that associates have little protection or rights, as there were many instances of practice owners who did not pass on payments given to NHS practice owners which were intended for associates.
63
There are benefits and drawbacks of employed and self-employed status and potential impacts on productivity and income, which should be considered if an employed model is adopted or offered as an option within general dental practice. The BDA conducted focus groups of associate dentists in 2021 which revealed that dentists do not believe NHS working conditions and constraints would change if associates were employed.
63
This highlights that the situation around NHS contractual arrangements is more complex than simply changing the model of remuneration, it definitely
The present review found that flexible and part-time work is desired, especially among newly qualified and female dentists.32,50 This agrees with a recent report on dentist working patterns which found an increase in part-time working for dentists. 64 The proportion of female dentists has been rising in the UK, and in 2021 the GDC register for dentists was 51.5% female and 48.5% male. 65 There has also been an increase in the number of dentists who want a “portfolio” career, where they work part-time in general practice and have one or more additional roles elsewhere, such as teaching or even a role outside of dentistry. 66 The findings of this review are reflective of this, as dentists desire a variety of work,33,51 opportunities for additional roles36,51 and opportunities to gain further qualifications and develop skills.34,36,38,42,50 These prospects are unlikely to be found within general dental practice where the work is regarded as repetitive.40,67 In addition, this review found dentists have concerns around litigation and complaints,32,46,48,49 which has previously been reported as the biggest concern of dentists up to five years post-qualification. 68
There has been an increase in the number of corporate dental bodies in the UK (multiple dental practices owned by one dentist or company), due to their ability to employ economics of scale and manage the increasing burden of bureaucracy and regulation. 68 Findings from this review suggest that there is a perception among dentists that corporate environments focus on profit over quality care.45-47 Dentists who work in corporate environments are less satisfied than non-corporate dentists. 49
The present study suggests availability of professional support networks could increase the retention of dentists.40,41,51,52 Dentists are at high risk of burnout, anxiety, and depression from the stressful demands of the job.49,51,69 A study in 2022 found that dental professionals may not understand how, or may be unwilling, to access formal help. 69
This review identified factors relating to job location. Newly qualified dentists have anxiety over securing a job in a preferred location 39 and there have been few incentives to work in rural or high-needs locations, 38 although a recently launched scheme in Wales is offering preferential terms to attract graduates to work in rural and remote localities. It has been previously reported that recruiting dentists in rural and more deprived locations is challenging 48 so without initiatives that remove the potential for this to be a factor contributing to dissatisfaction, it is unlikely these locations will become more attractive to dentists. This has the potential to further exacerbate oral health inequalities and lead to poorer outcomes for patients in rural and more deprived areas, as patients in these areas will find it challenging to access timely dental care and resort to seeking care in inappropriate places, such as the Emergency Department, putting more pressure on other areas of the healthcare system.
From the literature available, there is insufficient evidence to make any definitive conclusions about the impact of Covid-19 or Brexit on the dental workforce, but this is a topic which warrants future investigation due to the prediction that it will lead to a reduced supply of dentists and dental care professionals. A reduction in the supply of dentists and dental professionals may improve working conditions as demand increases, however there is likely to be increased competition from private practices and they may be able to offer more attractive positions compared to NHS practices.
Conclusion
Current contractual arrangements are contributing to the dissatisfaction of dental professionals, and any changes should consider minimising or removing factors identified in this review which lead to dissatisfaction, and introduction of factors which increase satisfaction, to firstly retain the existing workforce and to attract dental professionals to NHS dentistry. This is crucial to ensure there is a dental health workforce that is able to meet the needs and demands of the population.
Footnotes
Appendices
Quality Assessment of included records: summary judgement table of included articles
|
Acknowledgements
Part of this research was carried out in partial fulfilment of a Master’s in Public Health by the first author (JAH).