
Abstract
Transposition of teeth may present to the general dental practitioner and in some circumstances transposed teeth may present with other dental anomalies. Although dental transpositions are rare anomalies, management of transposed teeth can often be complex, requiring multidisciplinary management. It is therefore important for dentists to be familiar with the clinical and radiographic presentation of transpositions and understand the aetiology to aid early diagnosis and appropriate management.
Learning Objectives
To present an overview of the aetiology, clinical and radiographic presentation, classification and management of transpositions
To improve awareness of transpositions to facilitate early diagnosis and subsequent management
Introduction
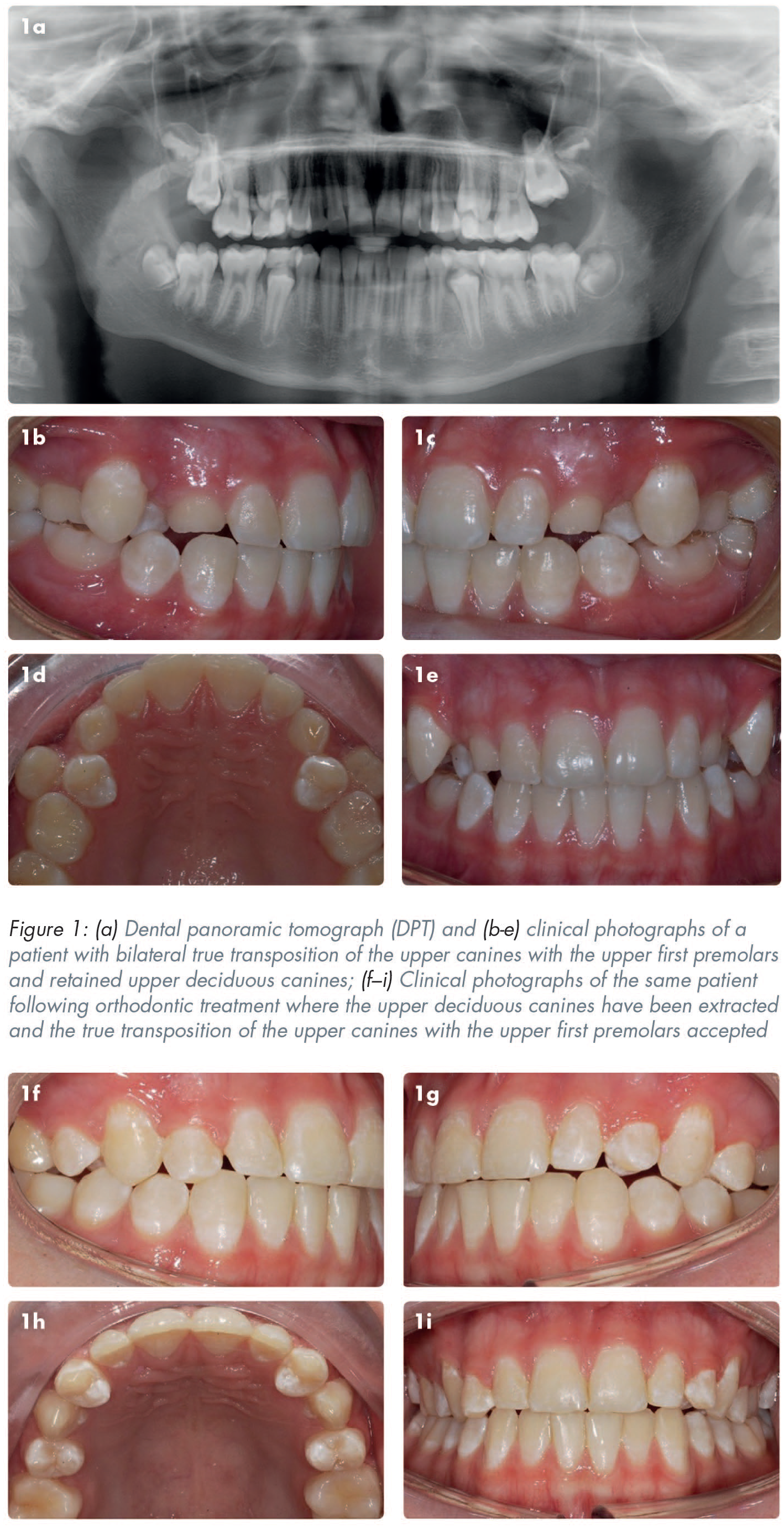
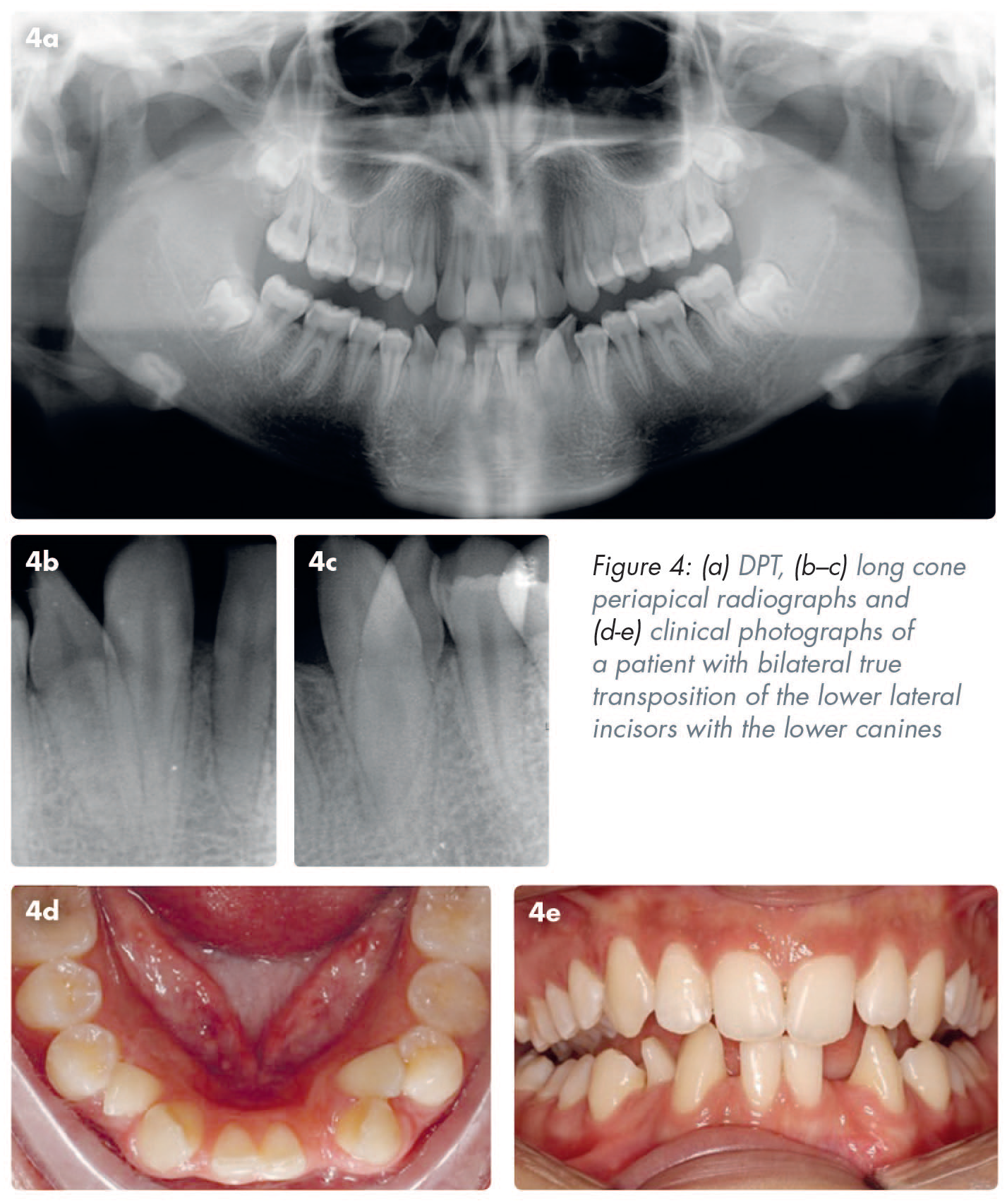
A transposition is defined as a positional interchange of two teeth located in the same quadrant of the dental arch or the eruption of a tooth in a position normally occupied by a non-adjacent tooth.1-4 Transpositions can occur in the deciduous or the permanent dentition, but more commonly affect the permanent dentition. The overall incidence of transpositions is estimated to be between 0.2% and 0.38%.3,5,6 Transpositions are more common in females than males and more frequently occur in the maxilla (76%) than the mandible.3,7 It has been reported that the most commonly occurring transposition is that of the maxillary canine and the maxillary first premolar (71%), as shown in Figures 1, 2 and 3, followed by the maxillary canine with the maxillary lateral incisor (20%). 3 Although not as common, the most frequently occurring transposition in the mandible is that of the canine and the lateral incisor, 7 as shown in Figure 4.

Aetiology
Transpositions have a multifactorial aetiology with both genetic and environmental factors playing a role,7,8 with the following factors all having been cited as having causative roles in transpositions: genetics, ectopic position of tooth bud, crowding, mechanical interference, early loss of deciduous tooth, over retention of deciduous teeth, trauma to deciduous teeth and cysts or local pathology.2,5,8-11
An increased incidence of transpositions has been reported in patients with other dental anomalies, which supports genetics having a role in the aetiology of transpositions.2,3,7 Compared to the general population, a four- to ten-fold increase in transpositions has been reported in patients with hypodontia, illustrated in Figure 2, and an eight- to sixteen-fold increase in patients with peg-shaped lateral incisors. 2 Further support for the genetic role in transpositions comes from reports of transpositions occurring in the same arch bilaterally,8,12 as shown in Figures 1 and 3.
Environmental factors, such as trauma to the maxillary incisors, have been reported to be a possible cause of transpositions due to the trauma potentially causing a disturbance in the position of the developing tooth buds of the permanent dentition.3,13 Opportunistic eruption of a permanent tooth into a transposed position has also been reported to have occurred in cases where a permanent tooth in the same quadrant has been extracted and an unerupted permanent tooth then erupts into the position of the extracted tooth. This has been reported to have occurred in cases of extraction of a maxillary central incisor with the maxillary canine erupting into the incisor position, and also in a case of eruption of a maxillary canine into the position of a previously extracted maxillary first permanent molar.3,13
Overall, the precise aetiology of transpositions for individual patients is unknown and it is most likely that there are multiple contributory factors in the aetiology of transpositions. 14
Classification
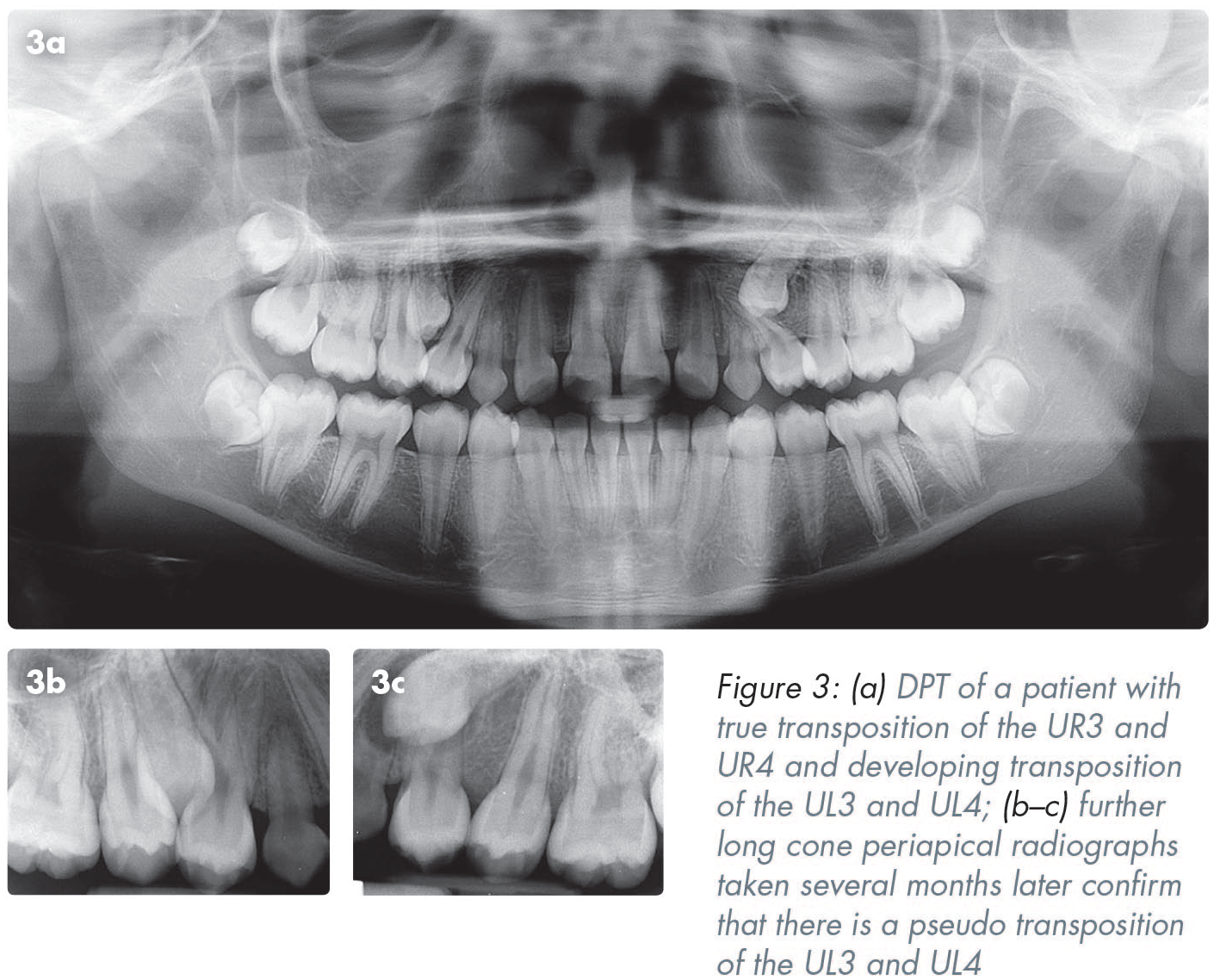
Transpositions can be classified according to whether the root and the crown have interchanged position, or just the crown. Transpositions are classified as being “complete/true” when both the crowns and the roots of the affected teeth have changed position, whereas an “incomplete/pseudo” transposition is when the crowns have changed position but the roots remain in their normal position. 1 Figure 3 illustrates a case where the patient has a true transposition of the UR3 and UR4 and a developing transposition of the UL3 and UL4. Further long cone periapical radiographs taken several months later, confirm that there is a pseudo transposition of the UL3 and UL4.
Peck and Peck developed a notation system for transpositions according to the teeth affected. 2 The notation consists of a three-part code, separated by full stops, which specifies:
the arch the transposition is in: Mx for maxilla and Mn for mandible
the tooth which is transposed: I for incisor, C for canine, P for premolar, M for molar
the second tooth involved in the transposition: described as above
the components of this three-part code are separated by full stops
For example, the transposition of a maxillary canine with a first premolar would be denoted as: Mx.C.P1.
Diagnosis
If the teeth in question are erupted, transpositions can usually be identified through intra-oral examination, where a positional interchange of two teeth will be noted (Figures 1, 2 and 4). In patients who are in the developing dentition, radiographs can often identify a transposition, or the possibility of a transposition occurring with further dental development. Transpositions may be an incidental radiographic finding in the developing dentition or radiographs may be used to confirm the presence or absence of a suspected transposition where there is abnormal dental development clinically, as was the case in Figure 3.
To ascertain whether a transposition is a true or pseudo transposition, it is often necessary to undertake a radiographic examination. This will allow the clinician to assess if, as well as the crowns, there has also been a positional interchange of the roots of the affected teeth.
If sufficient information cannot be established from conventional, routine radiographic imaging, a cone beam computed tomography (CBCT) scan may be indicated. 15 A CBCT may be advisable in situations where the roots of the affected teeth are in close proximity and cannot be clearly seen on standard radiographs and also in situations where there is possible pathology associated with the transposition which cannot be assessed in sufficient detail with those views. 16 In such situations, discerning the exact nature of the transposition and any associated pathology may affect subsequent patient management and therefore the increased radiation associated with a CBCT would be indicated if the benefits of the CBCT outweigh the risks. 16
Management
A multidisciplinary approach to managing transpositions is beneficial to allow input from all relevant specialties including Orthodontics, Restorative Dentistry, Oral Surgery and Paediatric Dentistry.
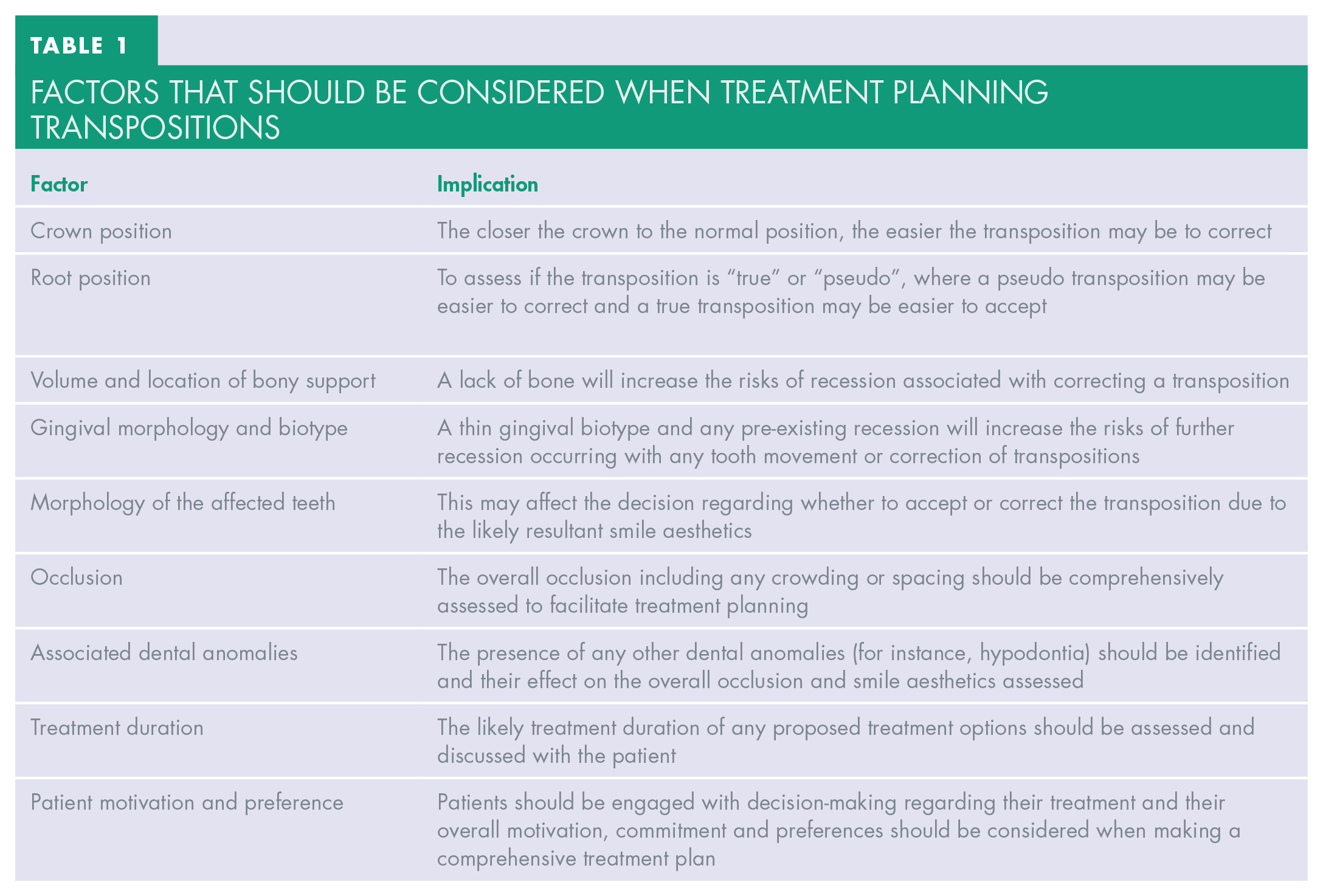
When considering the treatment options for transpositions several factors should be considered as well as the risks and benefits of undertaking treatment or accepting the current situation. The factors that should be considered when treatment planning for transpositions 17 are shown in Table 1.
Factors that should be considered when treatment planning transpositions
Treatment options
Following a comprehensive clinical and radiographic assessment, a range of treatment options are possible.
Interceptive treatment to try and prevent the development of a transposition
If a possible transposition is noted early enough, deciduous teeth can be extracted during the mixed dentition to try and guide the development and eruption of the permanent dentition to prevent a transposition developing. 18 This is usually only successful with pseudo transpositions. Patients may need a space maintainer if deciduous teeth are extracted early, to prevent space loss and the subsequent development of crowding.
Accept the transposition
The position of transposed teeth can be accepted and this is usually most feasible in cases of true transpositions. This is illustrated in Figure 1, where the orthodontic treatment plan was to accept the bilateral true transposition of the upper canines with the upper first premolars. The affected teeth may require modification of the incisal edge or occlusal surface to achieve an optimal aesthetic result. 11
Correct the transposition
The position of transposed teeth can be corrected using orthodontic treatment. This is usually a feasible option in cases of pseudo transpositions. However, the duration of treatment can be lengthy, and tooth movement can risk causing root resorption, bone loss, perforation through the buccal or lingual plate and gingival recession, all of which should be carefully considered prior to undertaking treatment to correct a transposition.11,14,19-22
Extraction of one of the transposed teeth
This is usually the preferred treatment option in patients who present with crowding, with insufficient space to accommodate both affected teeth or if one or more of the affected teeth are severely affected by caries or periodontal disease and have a poor long-term prognosis. 18 If appropriate, orthodontic treatment can then be undertaken to align the remaining dentition and close any residual spaces.
Extraction of the transposed tooth and replacement
Extraction of the transposed tooth with a view to replacement can be considered if the position of the transposed tooth is deemed as being detrimental to the overall occlusion or if it has a poor long-term prognosis. 11 If space closure is not feasible the patient can then consider restorative replacement of the extracted tooth.
Autotransplantation of the transposed teeth
Autotransplantation of transposed teeth has been described as a treatment option in a few case reports in the literature.23,24 However, this option should only be considered in very specific cases when patient, operator, recipient, and donor factors have all been considered.
Conclusion
Although dental transpositions are rare anomalies they can present to the general dental practitioner (GDP). It is therefore important that GDPs have knowledge and understanding of the aetiology, diagnosis, and management of transposed teeth. Management of transpositions can often be complex and require multidisciplinary management, therefore, early recognition of the clinical and radiographic features and an understanding of the aetiology and classification can be beneficial for prompt diagnosis and subsequent onwards referral in order for these patients to access the multidisciplinary management they require.
Footnotes
Declaration of conflicting interests
The Authors declare that there is no conflict of interest.