
Abstract
This case report outlines the effective treatment of a multifaceted orthodontic case involving multiple impacted and supernumerary teeth and complete transposition in a 10-year-old girl. She presented with missing anterior teeth, an Angle’s class I molar relation on the left, Angle’s class II molar relation on the right, and various dental anomalies. On cone-beam computed tomography (CBCT) evaluation, the patient had vertically impacted four teeth (central incisors, right lateral incisors, and canine) and four supernumerary teeth. The treatment plan included surgical extraction of impacted teeth, orthodontically guided eruption, extraction of supernumerary teeth, and atypical extraction of #12, #24, #34, and #44 due to arch length tooth material discrepancy. #12 was extracted as there was palatal fenestration and had an open root apex. The spatial position and orientation of the impacted teeth were assessed using CBCT. The orthodontic treatment employed a rigid metal framework with NiTi coil springs for guided eruption. Interdisciplinary collaboration among orthodontists, dental surgeons, and other specialists, along with meticulous planning and controlled force application, was crucial. Satisfactory aesthetics, functional occlusion, and stability were obtained at the end of the treatment, demonstrating the effectiveness of orthodontic intervention in complex cases.
Introduction
Multiple impactions of teeth refer to sequential impaction of ≥2 teeth in unison in the alveolar bone, be it in a unilateral or multisided manner.1, 2 There is no evidence in the literature regarding the incidence or prevalence of multiple impactions. 3 The prevalence rate of impacted maxillary central incisors ranges from 0.06% to 0.20%, while impacted maxillary canines are observed in approximately 0.8-3.0% of cases.4, 5 The canine impaction being relatively common often goes unnoticed and is diagnosed mostly as an incidental finding during routine dental check-ups. 6 On the other hand, central incisor impaction being relatively rare often raises concern and calls for orthodontic treatment. 7 Impaction involving maxillary anterior teeth is relatively uncommon, with significant implications on the patient’s aesthetic, functional, and psychological problems.8, 9 The etiology of the multiple impacted teeth may be due to generalized factors such as genetic influence, systemic prenatal and postnatal disorders, syndromes causing tooth impaction, and hyperdontia (cleidocranial dysplasia, Gardener syndrome, Down syndrome, Apert syndrome, Ehlers–Danlos syndrome, etc.) or localized factors such as trauma, reconstructive maxillofacial procedure, malalignment of the teeth in proximity, overlying dense mucosal tissue, tooth buds in an altered position, premature exfoliation of deciduous teeth, prolonged retention of deciduous teeth, eruption disturbances, and presence of cyst or neoplasm.10–13 Management of impacted teeth involves (a) removing the barrier and allowing spontaneous eruption, (b) orthodontically guided eruption of the teeth into occlusion, (c) extraction of the teeth if it is unfavorable movement of the adjacent teeth into their position, (d) surgical repositioning/autotransplantation, and (e) replacement of the impacted teeth. The orthodontically guided eruption is the most opted treatment option for optimal results. 6 Orthodontically guided eruption might improve the clinical crown length, alter the gingival margins, architecture and zenith level, and level osseous defects.
Sporadically, changes in the position between adjacent/nonadjacent dental units in maxillary and mandibular arches due to interference in tooth eruption and are termed as dental transposition. Dental transposition occurs with an average prevalence of 0.33%. With maxillary canine premolar being the most common followed by canine lateral incisor transposition. 14 Management of dental transposition involves either the maintenance of transposition/correction of transposition/extraction of one tooth considering various factors. 15
Supernumerary teeth are one of the most important etiologic factors contributing to both of the above-mentioned problems. Supernumerary teeth tend to occur more commonly in the premaxillary region (80%). 16 With 76-86% of cases having single supernumerary teeth, 12-23% of cases having pairs of supernumerary teeth, and <1% having multiple supernumerary teeth. 17 For their occurrence, a number of theories have been put forth, including the “phylogenetic theory,” the “dichotomy theory,” “hyperactive dental lamina” (most widely accepted), and the “combination of genetic and environmental factors‑unified etiologic explanation.” 18 Management of supernumerary teeth involves either extraction if it causes complications/interferes with orthodontic treatment and regular monitoring if no complication is associated with it. 19
The significance of an interdisciplinary approach involving orthodontists, oral surgeons, and occasionally periodontists in managing impacted teeth cannot be overstated and should be emphasized. 20 This report outlines the efficient treatment approach for a rare case of nonsyndromic multiple impactions of maxillary anterior teeth along with impacted supernumerary teeth. This involved impaction of the upper central incisors vertically, right lateral incisor, four supernumerary teeth (impacted), and complete transposition of bilateral canines and lateral incisors.
Diagnosis and Etiology
A 10-year-old girl presented with the complaint of an unattractive appearance caused by missing front teeth in the maxillary anterior region. Her past medical history and dental history revealed nothing significant.
Family History
During the initial visit, the patient and her accompanying family members were inquired about any instances of supernumerary teeth among them or their relatives. They reported no known cases of extra teeth within their family or extended relatives.
The clinical extraoral examination of the patient revealed an apparently symmetrical face, a mesoprosopic facial form with a convex profile, and an unesthetic smile. There was no obvious mandibular deviation. Intraorally, the patient presented with clinically missing upper anterior teeth (central incisors, right lateral, and canine). The primary maxillary right canine was retained without mobility. There was the transposition of upper left lateral incisor and canine. Posterior bilateral crossbite was present in the premolar region. The maxillary left first premolar was in buccoversion and rotated mesiobuccally. She had a class I molar relationship on the left side and a class II molar relationship on the right side because of the mesial migration of the maxillary right first molar. The mandibular dental midline was coincident with the facial midline. The lower arch displayed a discrepancy in tooth size relative to the available arch length. A referral was made to a physician for the evaluation of possible syndromes, and after assessment, the physician excluded the presence of any syndrome (Figure 1).

In this case, multiple impaction and transposition could be due to thickened overlying mucosal tissue, multiple supernumerary teeth, and tooth buds in altered position, genetic factors could also be involved but the patient was not willing to genetic evaluation due to the increased cost for performing the genetic analysis.
A cone-beam computed tomography (CBCT) scan of the maxilla was performed [imaging cone beam tomography (iCAT), field of view (FOV) = 8 × 8 cm, voxel size 0.3 mm, high resolution] to obtain a more precise assessment of the supernumerary and impacted teeth, as conventional radiographs did not provide sufficient details. The scan revealed four supernumerary teeth located in various areas. 21
CBCT Assessments
CBCT images were processed to produce cross-sectional, axial, coronal, and 3D views. Findings revealed vertically impacted upper central incisors (maxillary central incisor on the first quadrant was positioned in a vertical alignment and completely impacted within the bone, root development completed with closed apex, the tooth crown was located approximately 12.6 mm from the alveolar crest, and the buccal and palatal cortices were uninvolved), right lateral incisor (positioned in a vertical alignment, completely impacted within the bone, incomplete root development with open apex, and the whole tooth appears to be positioned involving the palatal cortical plate, causing its obliteration at the alveolar crest region, the root apex appears to be clear of the nasal floor with no follicular enlargement noted) and canine (positioned in a vertical alignment, above #14, complete root formation with closed apex, impacted within the bone. The tooth crown can be located approximately 11.5 mm from the alveolar crest, and palatal cortices are uninvolved, the root apex appears to be closely involving the nasal floor as well as the sinus floor). No breach is noted in multiple cross sections, and four supernumerary teeth (one supernumerary located just buccal to 12, rotated with open apex, two supernumerary teeth positioned palatal to 11, spear-shaped crown with open apex, and one supernumerary teeth positioned palatal to 21, spear-shaped crown with open apex) are in the maxillary anterior region with complete transposition of upper canines and lateral incisors. All the teeth showed completed roots, and no bony ankylosis was found [i.e., the periodontal ligament (PDL) space was visible around all the supernumerary teeth]. The presence of supernumerary teeth had not caused any resorption or fusion of normal teeth. The presence of supernumerary teeth resulted in thinning of the palatal and lingual cortical bones without affecting the vital structures. All the supernumerary teeth were impacted and unerupted. The morphology of two supernumerary teeth was close to that of normal teeth (supplementary supernumerary teeth). Two of them appeared rudimentary. No signs of cystic formations or pathological alterations were observed in the vicinity of the supernumerary teeth (Figure 2).
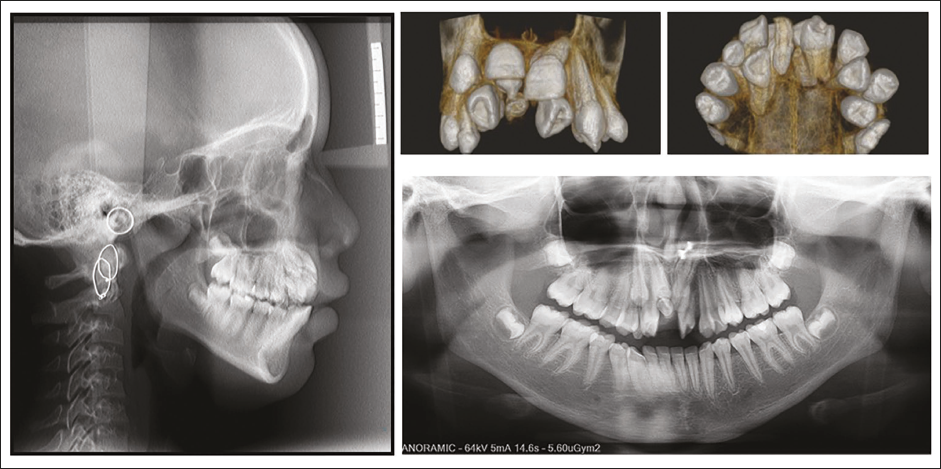
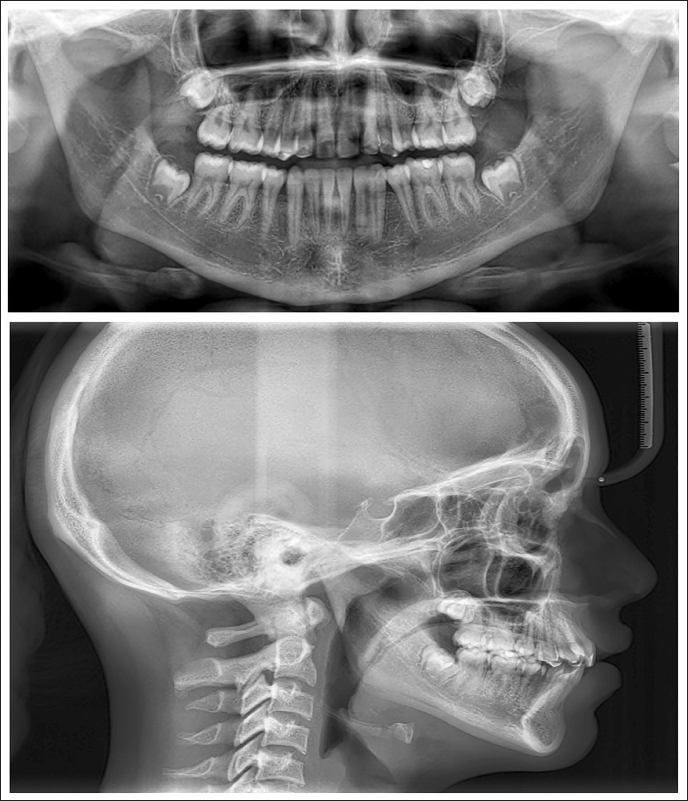
Lateral Cephalogram Assessment
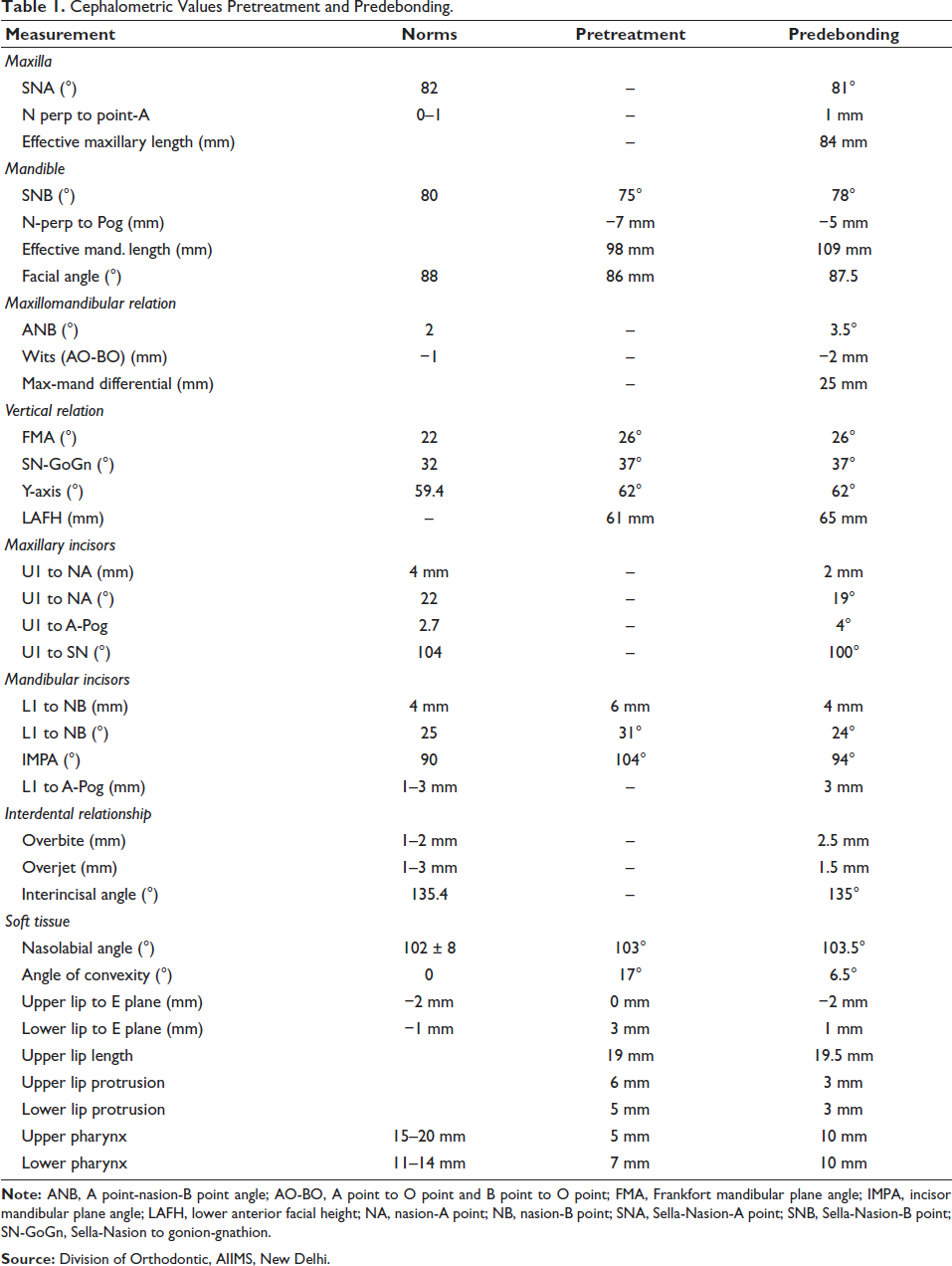
Lateral cephalometric analysis indicated an average growth pattern [Frankfort mandibular plane angle (FMA) 26°]. Multiple radio-opaque tooth-shaped structures were found in the maxillary anterior region; the mandibular incisors exhibited a slight forward inclination [lower incisor to nasion-B point (L1-NB), 31°; incisor mandibular plane angle (IMPA), 104°]. Due to the presence of impacted maxillary anterior teeth, point A could not be accurately identified (Figure 3 and Table 1).
Cephalometric Values Pretreatment and Predebonding.
Treatment Objectives
The main goal was to enhance smile aesthetics while ensuring a stable and functional bite. The treatment objectives were to (a) improve the self-esteem and quality of life of the patient, (b) facilitate the orthodontically guided eruption of impacted teeth, (c) extract multiple supernumerary teeth, (d) align maxillary and mandibular dentition, (e) achieve optimal overjet and overbite, (f) achieve functional occlusion with class I canine and class I molar relation bilaterally, and (g) achieve coinciding midlines.
Treatment Plan
Treatment planning and biomechanics were particularly challenging due to the complexities of the maxillary arch. Based on the overall analysis of the patient’s clinical examination, CBCT, and cephalometric findings, the orthodontic treatment plan was the best approach. In this case interdisciplinary treatment approach was planned to meet the above-mentioned treatment objectives, which involved the orthodontic guided eruption of the impacted upper anterior using a rigid metal framework attachment to anchor the NiTi coil spring bonded on surgically exposed impacted teeth, followed by fixed mechanotherapy to align the upper and lower arch. This plan involved extraction of the four supernumerary teeth, and arch length tooth material discrepancy required extraction in all the quadrants. In the first quadrant lateral incisor was extracted (#12 was extracted as there was palatal fenestration and it had an open root apex), and other than that, the first premolars were extracted in all the other three quadrants. The extraction of the right lateral and left first premolar in the maxillary arch teeth was delayed till the impacted teeth responded to the orthodontic force and was planned to be extracted before the fixed appliance placement. Maintenance of the teeth in transposition was planned as they were in true transposition and towards the end of finishing and detailing, alternating the morphology of maxillary right first premolar, left lateral incisor, and bilateral canines to substitute the morphology of maxillary right and left canine and bilateral lateral incisors respectively, were planned. Since the transposition was maintained in the upper arch and a lateral incisor was missing, the patient was planned to be provided with group function occlusion in eccentric movements.
During the consultation for treatment planning, the patient received comprehensive information about the case and treatment plan, including the potential risk that the canines might not respond to orthodontic eruption. In this event, the recommended course of action would involve extractions, followed by prosthetic rehabilitation using implants or a bridge. After discussing the options, the patient and her parents chose to proceed with orthodontic eruption and provided informed consent for the treatment. Additionally, it was agreed to monitor the development of the third molars during the treatment and retention phases, with surgical removal suggested if deemed necessary.
Treatment Progress
After the initial visit and treatment planning appointment on January 24, 2020, the patient reported again after 9 months due to the COVID-19 crisis on October 15, 2020. At this stage, there was an eruption of two supernumerary teeth and a right lateral incisor. We proceeded with orthodontic treatment as per our initial plan.
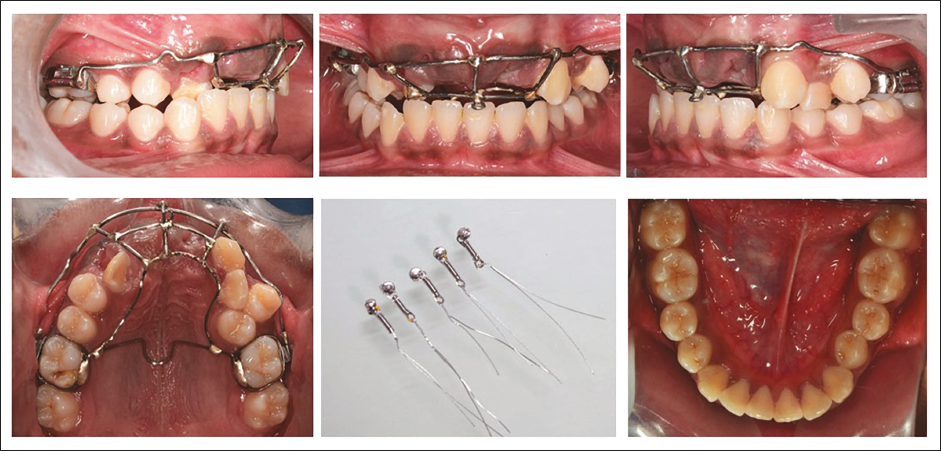
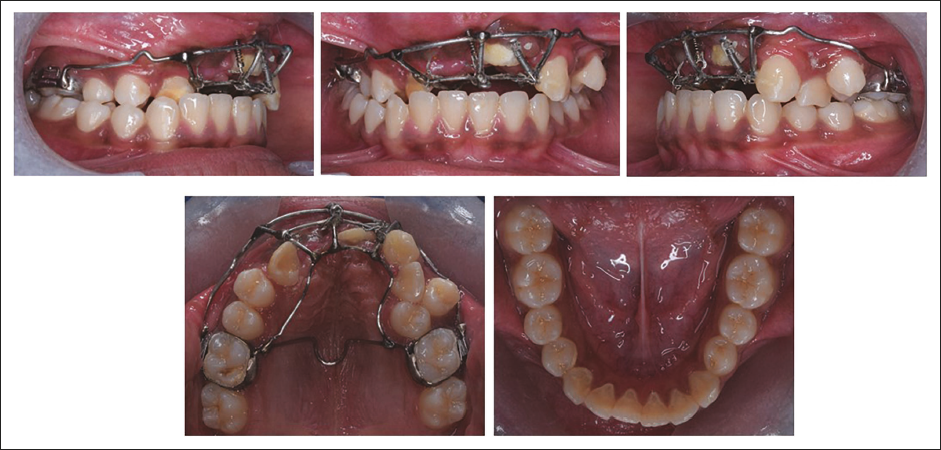
A rigid metal framework was fabricated using 40 mil stainless steel (SS) wire to provide attachments to facilitate orthodontically guided eruption. Exposure of impacted teeth was done through the crestal incisions and by raising full-thickness mucoperiosteal flaps. Extraction of two remaining supernumerary teeth was done simultaneously. Lingual buttons with NiTi coil springs were bonded to the impacted teeth after achieving a moisture-free environment. The flaps were repositioned, and suturing was done with the attachments extending orally through the incision (on November 27, 2020). The rigid metal framework was cemented to the molars, and force application was started after 10 days (Figures 3 and 4). On #11 the force was applied vertically and mesially, on #21 the force was applied vertically and distally, on #13 a vertical downward force was applied with the help of the custom-made rigid framework to provide an unobstructed path of eruption to all three teeth and to get them to erupt into the proper position in the arch, requiring minimal movement during orthodontics. After 1 month, the left central incisor crown was visible clinically. After 13 months into treatment crown of the upper central incisors and upper right canine were clinically visible. At this stage, the metal framework was removed, and extraction of the upper right lateral incisor and left first premolar were performed. Fixed mechanotherapy was started in the upper arch with MBT prescriptions (0.022” × 0.028”) with 0.014” NiTi wire as the first alignment archwire. Posterior crossbite was addressed by placing expanded SS archwires. Sixteen months into treatment extraction of the lower first premolar was done for en-masse retraction of the lower anterior using a continuous “T” loop in 0.018” × 0.025” titanium molybdenum alloy (TMA) archwire. Twenty-three months into treatment results in the alignment and space closure of the upper and lower arches. Complete orthodontic records were taken to evaluate for finishing and detailing (Figure 5). The patient was referred to an endodontist for cosmetic modification of the maxillary canines, involving the contouring of the labial ridge and the refinement of cuspal slopes with fine-grit diamond burs in an air-rotor handpiece. Functional hindrance caused by the premolar’s palatal cusp on the right side during lateral and protrusive mandibular movements was of concern. The premolar’s central fossa and palatal cusps were reshaped to enable occlusal clearance, reduce interferences with centric occlusion, and ease mandibular movements. The maxillary left lateral incisor was restored to replicate the anatomical structure of a canine and support functional movements. The fixed appliance was deboned after achieving the desired optimal occlusion and smile aesthetics in 27 months of total treatment duration (Figures 6 and 7). Clear thermoformed retainers were delivered as retention devices in the upper and lower arches.


Treatment Results
Following 27 months of treatment, significant enhancement in smile aesthetics was achieved, with the impacted maxillary anterior teeth successfully aligned into a functional occlusion. The maxillary and mandibular arches were aligned, resulting in a bilateral full-cusp class I molar relationship. Morphology of maxillary right first premolar left lateral incisor and bilateral canines were altered to substitute the morphology of maxillary right and left canine and bilateral lateral incisors respectively. Coincidence of upper and lower dental arch midlines was also achieved. This led to a marked improvement in smile aesthetics and overall appearance. The periodontal health of the teeth was not compromised and maxillary anterior teeth were aligned with an adequate width of the attached gingiva. There were caries concerning the maxillary right first molar that required restoration, and the gingival zenith of the upper anterior was significantly altered and required surgical correction to improve smile esthetics.
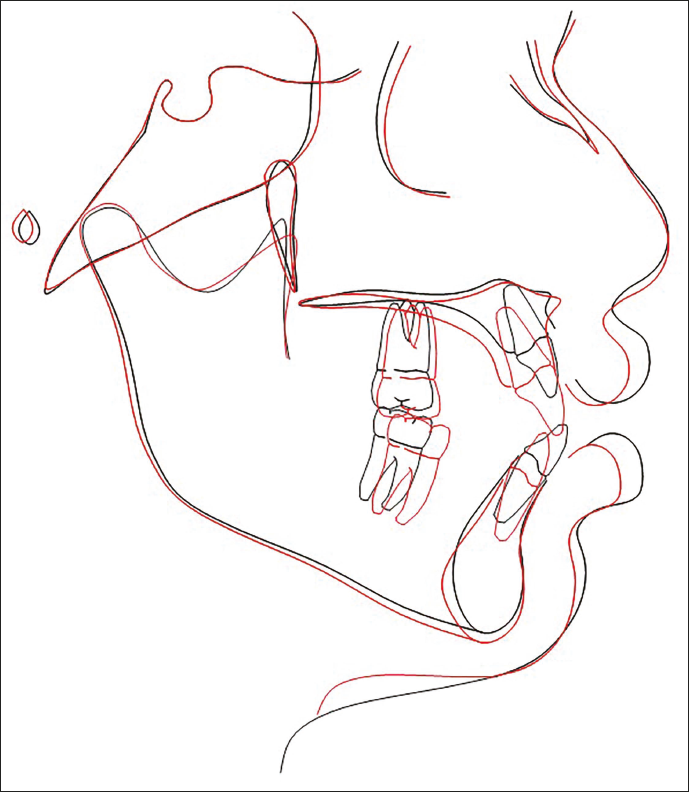
Following debonding, the panoramic view illustrated that the roots of the teeth in both arches were aligned and angulated appropriately (Figure 7a). There was no apical root resorption detected on the radiographic examination. Post-debonding lateral cephalogram (Figure 7b) showed class I skeletal bases [maxilla Sella-Nasion-A point (SNA)—to 81° and mandible Sella-Nasion-B point (SNB) 74-78°], with no change of mandible in the vertical plane (FMA, 26°). These skeletal changes might be linked to her pubertal growth phase. The maxillary [U1 to Sella-Nasion (SN)—to 100°] and mandibular (IMPA 104° to 94°) incisor inclinations were normal after the treatment (Table 1). The superimposition of the cephalogram has been presented (Figure 8). Figure 9 illustrates the changes before and after treatment.

Discussion
This case report describes the treatment of an unusual clinical scenario with multiple impacted maxillary anterior teeth supplemented with the presence of complete transposition and the presence of multiple supernumerary teeth that usually pose a hardship to the orthodontist in diagnosis, mapping out the appropriate treatment plan, and execution of the treatment progress as per plan. The existence of impacted, transposed, and supernumerary teeth is one of the most justified indications for obtaining CBCT for visualizing the accurate information on the number of impacted and supernumerary teeth, location, angulation, the spatial orientation of the individual teeth, their proximity to the other teeth, and associated structures.22, 23 This three-dimensional imaging helped in treatment planning decisions of extraction needs and deciding appropriate biomechanics for the predictable treatment outcomes.
In this specific case, the unerupted four supernumerary (2 supplementary, 2 rudimentary) teeth were situated in the premaxillary region, causing obstruction to the eruption of teeth 13, 12, 11, and 21. It is important to note that none of these teeth exhibited cystic lesions or any pathology. Hence, unerupted supernumerary teeth were the reason for the impaction of the neighboring teeth. That is why the extraction of supernumerary teeth was crucial in achieving the successful completion of the orthodontic treatment, enabling the patient to attain proper functional occlusion and an esthetic smile. The extractions were strategically planned to facilitate the appropriate eruption and subsequent alignment of the natural dentition, promoting optimal dental alignment and aesthetics for the patient. 19
The orthodontic guided eruption is the first treatment option often opted for the impacted teeth. 15 Surgical exposure followed by orthodontic traction increases the versatility of treatment techniques that can be applied to achieve desired treatment results.24, 25 Although tooth repositioning or surgical transplantation may be another option, but transplanting several teeth in the same area would not be a viable option. Also, they may have a high risk of pulp necrosis, ankylosis, and root resorption post-transplantation.24, 25 One common feature among impacted central incisors is that they often have shorter roots and are associated with dilacerations. 26 However, this was not the situation with this patient making it further possible for us to apply orthodontic traction in place of the extraction of teeth, followed by prosthetic rehabilitation. Based on this, we opted for the orthodontic-guided eruption using a rigid metal framework attached to the maxillary first molars. The rigid metal framework was made up of 1.02 mm SS wire labially with transpalatal arch (TPA) on the palatal side, along with a continuous lingual wire soldered to molar bands and a soldered buccal wire extended in a helical design to provide an attachment to the active element for orthodontic guidance of eruption of teeth. This acted as a rigid framework to facilitate the eruption of the impacted teeth and the proper execution of needful biomechanics and positioning of impacted teeth. Treatment started with the surgical phase to remove the supernumerary teeth and to bond the impacted teeth for orthodontic traction. A full-thickness mucoperiosteal flap was raised with a midcrestal incision to allow the eruption of the tooth through the crest of the alveolar ridge. It results in the naturally appearing gingiva over the erupted teeth and eliminates the reintrusion problem post-treatment. 26
When looking into the literature for optimal forces to be applied for the traction of impacted teeth, it varies greatly due to the lack of homogeneity of the patient and techniques used for aligning the impacted teeth lead to evidence-based evaluation challenges. However, one common factor may be deduced: low forces should be used during traction rather than strong forces. 2 Daskalogiannakis and McLachian demonstrated that the mean tooth movement rate was greater when the constant force was applied for a prolonged period than impulsive forces. 26 Hence light continuous forces were applied using NiTi closed coil spring. Furthermore, biomechanical considerations pertaining to guided orthodontic traction, that is, the application of accurate direction of forces for tooth eruption based on the initial position and angulation of the impacted teeth are important to achieve the desired outcome.
Potential treatment options for the transposition have been beautifully outlined by Ngan et al. as (a) correcting the transposed order of the teeth, (b) maintaining the transposed order of the teeth, and (c) extracting one of the offending teeth. 15 In this case, the complete transposition of the teeth on the maxillary arch was maintained. Hence, the maxillary canines were cosmetically reshaped into lateral incisors by trimming the labial ridge, and further, reducing cuspal slopes using fine grit diamond burs in the air-rotor handpiece. Functional hindrance caused by the premolar’s palatal cusp on the right side during lateral and protrusive mandibular movements was of concern. The premolar’s central fossa and palatal cusps were reshaped to enable occlusal clearance, reduce interferences with centric occlusion, and ease mandibular movements. Restoration of the maxillary left lateral incisor was done to mimic the canine anatomically and to aid in functional movements. Yet recontouring might be associated with the sensitivity to heat and cold, other pulp and dentin reactions, this can be countered with adequate cooling with abundant water and air spray and preparation of smooth and self-cleansing surfaces without interdental steps. The interdisciplinary approach can achieve not only an optimal occlusion but also a well-balanced, natural smile that will be stable over the long term.
Good gingival contour was another significant factor in achieving successful treatment outcomes. 27 According to Vermette et al., 90% of open exposure cases exhibited gingival scarring. 28 However, the closed eruption technique is known to yield improved aesthetics, bone support, and periodontal health on a long-term basis. 29 In particular, with respect to the length of the clinical crown and the level of the crestal bone, the surgical procedure chosen to expose impacted central incisors has significant effects on the long-term outcome of orthodontic therapy. 30 The gingival zenith of the upper anterior was significantly altered and required surgical correction to improve smile esthetics. Gingival contouring was not performed in this case since the patient was very satisfied with her dentition and the gingival outcomes and improvement of her smile aesthetics and was not willing for further treatment.
The interdisciplinary collaboration of orthodontists (diagnosis and treatment planning, orthodontic alignment of the arches), oral surgeons (surgical uncovering of the impacted teeth and extraction of the supernumerary teeth), and endodontists (aesthetic recontouring of the anterior teeth) helped to deliver optimal occlusion and smile aesthetics to the patient.
The total treatment duration was 2.25 years, which is the average treatment duration for an adolescent patient.
Conclusion
The possibility of nonsyndromic multiple impactions with supernumerary teeth and complete transposition is a rare case that poses a hardship for the orthodontist. A cautious evaluation of the case and planning of appropriate treatment biomechanics, supported by three-dimensional analyses, results in successful treatment outcomes with a harmonious occlusal relationship and aesthetic smile. The orthodontically guided eruption of the impacted teeth and atypical extraction of #12 (palatal fenestration and had an open root apex), #24, #34, #44, and maintenance of transposition with esthetic recontouring gave a satisfactory outcome in this case.
Authors Contributions
Naveen K. Subbaiah: Conceptualization, methodology, investigation, resources, data curation, writing—original draft, visualization, supervision, and project administration.
Sukeshana Srivastav: Conceptualization, methodology, investigation, resources, data curation, writing—original draft, visualization, supervision, and project administration.
Prabhat Kumar Chaudhari: Conceptualization, methodology, investigation, resources, data curation, writing—original draft, visualization, supervision, and project administration.
Ritu Duggal: Conceptualization, methodology, writing—review and editing draft, visualization, supervision, and project administration.
Availability of Supporting Data
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form, the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.