
Abstract
Traumatic dental injuries (TDIs) in the paediatric population are common and frequently seen in general dental practice. The management of TDIs can be challenging and, in most cases, the General Dental Practitioner is tasked with the initial assessment and emergency treatment. Patients and their families typically attend with elevated levels of distress, which is complicated by the limited dental experience of some children. Behaviour management is essential and helps prepare patients for dental care at both their emergency and follow-up appointments. Early and accurate diagnosis in combination with appropriate treatment contributes to favourable outcomes for traumatised teeth. Early discussions with or referral to paediatric dental teams for management of complex TDIs is encouraged, however shared follow-up care is beneficial over the long-term. In specific cases, initial dental treatment can be delayed by a few days to a subsequent appointment, allowing the dental team to book sufficient time for the treatment and for the patient and their families to prepare. Education of the patients and adults with parental responsibility is essential to manage expectations, explain likely complications and encourage attendance for long-term follow-up visits. This paper discusses the management of paediatric patients to aid the primary care practitioner in providing effective immediate and long-term care.
Learning Objectives
To provide an overview of managing traumatic dental injuries in the paediatric patient
To understand the general implications of dental trauma on the paediatric patient
To recognise clinical and radiographic signs of loss of vitality in a traumatised tooth
To understand the consequences of dental trauma to the permanent dentition
Introduction
A third of all children experience a traumatic dental injury (TDI) in the primary dentition, and a quarter of all school children sustain a TDI in the permanent dentition. 1 In most cases of dental trauma, General Dental Practitioners (GDPs) are the first to assess and treat these injuries, 2 and therefore have an essential role in the overall management.
The maxillary central incisors, followed by maxillary lateral incisors, are the most likely teeth to be traumatised with a higher incidence in those with an increased overjet.1,3 Repeat TDI episodes are common, affecting just under half of patients with a history of a TDI. 1 The aetiology of dental trauma differs between dentitions, with TDI in the primary dentition often associated with falls due to transition from crawling to walking, and the permanent dentition associated with falls, accidents, and sports injuries. In the permanent dentition, males are more likely than females to sustain dental trauma, however, there is no obvious difference between genders in the primary dentition. 4 The literature identifies the environment, certain activities, and socio-economic status as a risk factor for dental trauma. 1 Teeth in the primary dentition are more likely to obtain periodontal injuries (e.g. luxation injuries) while the most common TDI in the permanent dentition are fractures to the crown. 4
In addition to the direct dental consequences, TDIs place a heavy burden of care on the child and their family and have the potential to trigger or exacerbate dental anxiety. 5 Typically, complex injuries require extensive treatment, regular attendance for monitoring of outcomes, 6 costs to the family and the health service 7 and cooperation with dental treatment. There are also psychological consequences to paediatric patients who have experienced dental trauma, with self-reported decline in social interactions and reluctance to smile and laugh.8-10 Careful, considerate, and holistic management of patients and their families is paramount to achieve positive outcomes following TDIs.
This article will outline some of the key considerations in the management of traumatic dental injuries in the paediatric population.
Safeguarding
Consideration of the possibility of non-accidental injuries when a patient presents with dental trauma is important. At least 50% of physical child abuse involves orofacial trauma, 11 therefore dental professionals are in a critical position to recognise and raise any suspicions. 12
As part of routine history taking, it is useful to determine whether there is any existing social services involvement with the family. It may be appropriate to contact the named social worker and inform them of any concerns regarding the patient. It is important to note that even if a child has no previous social services involvement, they may still be at risk of non-accidental injury.
General observations of the child, their behaviour, and the nature of interactions between the patient and accompanying adult should be recorded in the clinical notes. While taking the history, clinicians should consider any inconsistencies between the patient and accompanying adult and whether the clinical presentation is consistent with the reported mechanism of injury. Presentations of facial injuries that are symmetrical or within the “triangle of safety” between the ears, neck and top of the shoulder are rarely caused by accidental injuries and should raise suspicion. 13
Photographs, with permission, can provide helpful records of the injuries sustained. Further features of concern may be delayed presentation, repeated dental trauma, lack of supervision, or failure to attend future appointments for management of the dental trauma. 13 Any concerns should be documented in the patient’s notes and reported as per local safeguarding procedures. This subject is already well covered in broader literature and can be referred to for more detailed guidance. 13
Diagnosis
An accurate diagnosis of each injured tooth is paramount to ensure correct treatment is provided. Each tooth should be assessed for periodontal and hard tissue injuries. Both types of TDI (e.g. an enamel dentine fracture in conjunction with a subluxation injury) can occur in combination and have an important impact on pulpal survival. The dental trauma guide
14
(
Tooth and patient management
A unique challenge in paediatric dental trauma is the high level of anxiety and distress from both patients and their guardians at first presentation. 15 This can often be complicated by a patient that may be new to the practice, with limited previous dental experience, and a brief urgent appointment in an already busy day for the dental practitioner. The combination of these challenges can mean that a previously cooperative patient can have reduced capacity for managing extensive and invasive treatment in the chair, and their accompanying adult may not be able to effectively support them.
Before embarking on treatment, patients should be considered holistically: their level of distress and cooperation in the initial visit, previous dental history, and access to follow-up care. It is noted that reduced ability to cope with treatment is often related to fear sustained from a previous dental visit,16,17 therefore a positive initial experience will prepare patients for future appointments and help them acclimatise to the long-term care they may require.
Primary tooth management
Primary tooth management tends to favour observation or conservative treatment unless there is an impact to the occlusion or risk of ingestion or aspiration. 18 The new IADT guidance for management of the intruded and laterally luxated primary tooth reflects this, by allowing time to monitor for re-eruption/re-alignment rather than immediate extraction which can have a negative impact on future cooperation for the patient. 18 Clinicians should consult with or refer to specialist paediatric dental teams promptly in cases of severe luxation, crown or root fractures with pulpal exposure, or alveolar fractures to the primary dentition.
Permanent tooth management
Emphasis should be given to obtaining an accurate diagnosis in the first appointment, as this will determine the urgency of the required dental treatment. In an immature permanent tooth, prompt and appropriate treatment could preserve vitality and allow continued root development. Generally, injuries requiring repositioning and splinting are deemed the most urgent and this should be completed in the emergency appointment to avoid unnecessary delays and give the tooth or teeth the best possible chance of success. With the use of behaviour management techniques, detailed below, a large proportion of paediatric patients will allow dental treatment at the initial appointment and where this is possible, it is encouraged. In cases where there are complex injuries, significant anxieties or complete lack of cooperation, an urgent referral to paediatric dental teams is essential.
Some acute treatments, such as Cvek pulpotomies, definitive build up fractured teeth (assuming placement of a composite bandage at time of injury) or extirpations, can be delayed by a few days until a follow up appointment. This allows appropriate preparation, treatment time, and patient acclimatisation without significantly impacting the prognosis of the injured tooth.19,20
It may also be prudent to discuss the long-term prognosis at the follow-up appointment, where the patient and supporting adults are more likely to be in a better position to process the information being presented. Other situations that would warrant delayed dental treatment would be in cases of suspected head injury and the immediate requirement for a medical assessment.
Splinting in the mixed dentition
Flexible splints that are passive and short term are recommended in the IADT guidelines for luxated, avulsed and root fractured teeth.21,22 There are a variety of splints available commercially with differing costs. Splinting in the mixed dentition or where teeth are poorly aligned can present additional challenges with the need to span between teeth. In such cases composite resin splints are not suitable. Titanium trauma splints (Figure 1), despite their expense are simple to place and remove for the clinician and comfortable for the patient. 23 A composite wire splint is an inexpensive alternative; however, the wire should have a diameter no greater than 0.4mm. 24 Composite should be limited to the labial surfaces and care should be taken to not involve the embrasure spaces to aid oral hygiene. In cases of missing or mobile primary teeth, clinicians should extend the span of the splint to include the primary molars. Choosing a composite shade different to the tooth will facilitate clinicians when removing the splint. Clinicians should familiarise themselves with what materials they have available and how to use them prior to an emergency appointment.

Behaviour management
The child’s age and ability to communicate can help guide which are the most suitable treatment options, and clinicians are likely to be aware of which techniques work best for them. Patients without previous dental experience may benefit from a tell–show–do approach, minimising the time between showing and doing to help them progress with stages of treatment and reduce anticipatory anxiety. 25 Distraction techniques are also reported to be effective during procedures like local anaesthetic administration. This can be achieved verbally through a clinician talking during the procedure or alternatively with distracting sensations like lip pulling. 26 Effective analgesia is also important in obtaining continued cooperation, and efforts should be made to use topical anaesthetic prior to a slow steady delivery of local anaesthetic to maximise comfort and compliance. During treatment, inclusion of a stop signal in the form of a hand gesture can create a feeling of control for the patient and help alleviate anxiety. 27 Other general techniques like using the patient’s name and age-appropriate language during communication can help to build rapport. Recognising and verbalising positive actions from the patient will reinforce and shape behaviour for future appointments. 26
When appropriate, delaying treatment to a follow-up appointment and giving information to the patient and guardian allows them to prepare for the treatment and improves future cooperation.26,28 Signposting to helpful images and explaining sensations and expectations may help to mitigate the fear of the unknown. Despite best efforts, some patients may not be suitable for extensive dental treatment without the support of pharmacological techniques such as inhalation sedation or general anaesthetic. Recognising these patients early will allow a prompt referral to paediatric dental teams and focus can then be given to acclimatisation, monitoring, and preventative advice in practice.
Clinical and radiographic review
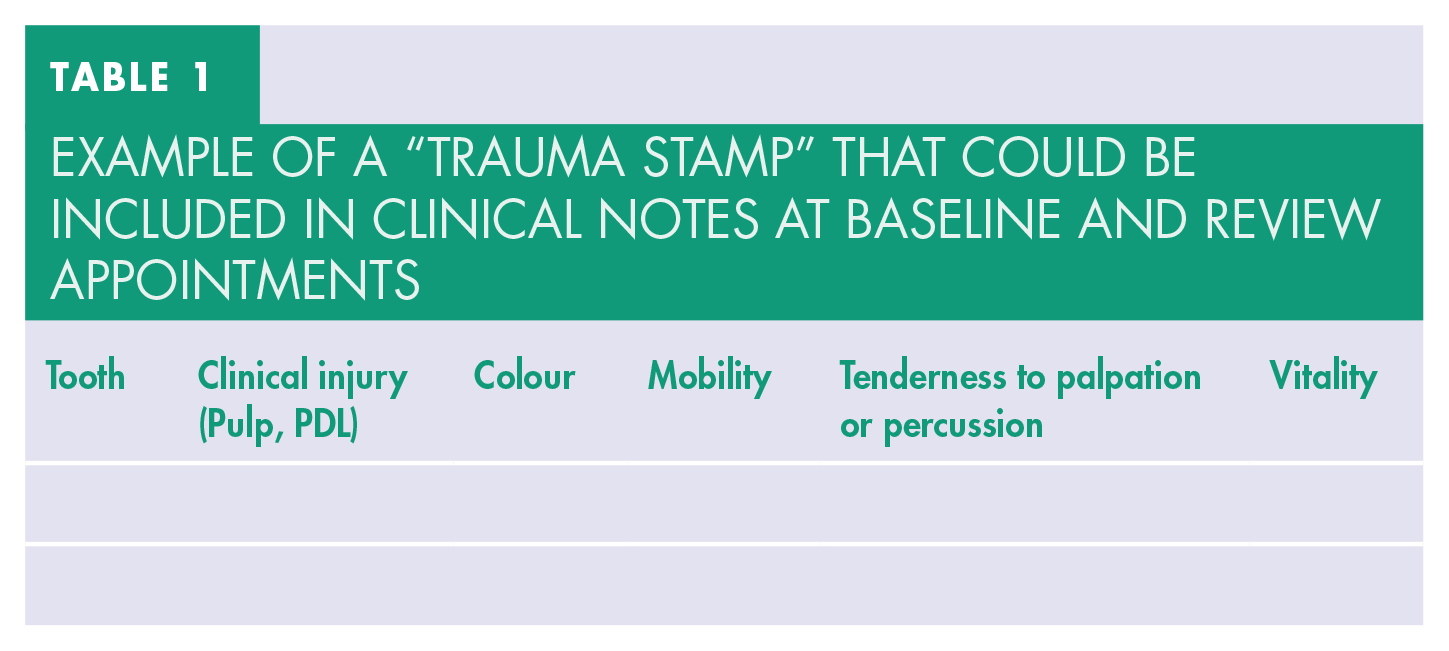
The IADT 2020 guidelines outline the frequency of clinical and radiographic reviews for traumatised teeth.18,21,22 Careful monitoring and clear documentation are important to identify sequelae of trauma at the earliest opportunity allowing prompt and appropriate management. Clinicians may find the use of a “trauma stamp” template for their clinical notes helpful (for example, Table 1). This can be created to include key headings such as “mobility”, “tenderness to percussion”, “colour”, “response to sensibility tests”. Baseline records at initial visit can be shared with specialist services at referral and allows comparison at future review appointments for evidence of change.
Example of a “trauma stamp” that could be included in clinical notes at baseline and review appointments
Clinical signs and symptoms
It is typical for traumatised teeth to present initially with transient clinical symptoms such as discolouration, mobility, and tenderness to percussion. These symptoms in isolation shortly after the injury do not indicate a loss of vitality. A thorough assessment and comprehensive records will allow the tooth to be monitored for changes at review appointments. Clinicians should consider the bigger picture and what key activities need to be accomplished for each clinical visit.
Sensibility testing
A positive response to pulpal sensibility testing at the time of acute presentation is a valuable indicator of pulpal prognosis.21,22 However, to prevent further distress, careful preparation of what sensations may be felt is essential to maintaining cooperation. Temporary loss of response to sensibility tests can occur following trauma, especially in luxation injuries. 29 A negative response may be expected for several months following injury. Sensibility testing in a paediatric patient can be unreliable for variable reasons: firstly, teeth that are immature have poorly myelinated nerve fibres so they may be poor conductors of thermal stimuli; secondly, the child may not comprehend the instructions; or thirdly, their anxiety may make it difficult for them to interpret the various sensations. Therefore, lack of response to sensibility testing in isolation is insufficient to conclude pulpal necrosis and may be best avoided at initial presentation.
Radiographs
Radiographic evidence of periapical pathology is indicative of loss of vitality.
30
An immature root which does not continue to develop in comparison to baseline or uninjured contralateral tooth, may also be an indicator of pulp necrosis. Follow-up radiographs should be taken with similar orientation to assist in identifying any resorption or periapical changes. This will also reduce the need for repeat exposures and adheres to the principle of ALARA (
In the absence of clear radiographic pathology or clinical signs, the diagnosis of pulp necrosis requires the combination of at least two clinical or radiographic features prior to embarking on endodontic treatment. Clinical signs such as tenderness to percussion, buccal tenderness or swelling, sinus, mobility, discolouration or non-response to thermal stimuli (usually a cold test such as Endo-Frost™ [Roeko GmbH, Sonthofen, Germany] over sequential long term follow-up appointments) should be considered alongside radiographic signs. 21
An exception to this approach is with avulsion and intrusion injuries involving a closed apex permanent tooth where endodontic treatment is advised within two weeks of the injury.19,22 For severe lateral luxation and extrusions, pulpal necrosis is likely. A discussion with the child and parent is encouraged to weigh up the balance between the possibility of pulpal healing versus infection related resorption. In some cases, elective extirpation may be the preferred choice, while for others, a watch and rigorous follow up is favoured.
Consequences of dental trauma
Unerupted permanent tooth following primary tooth TDI
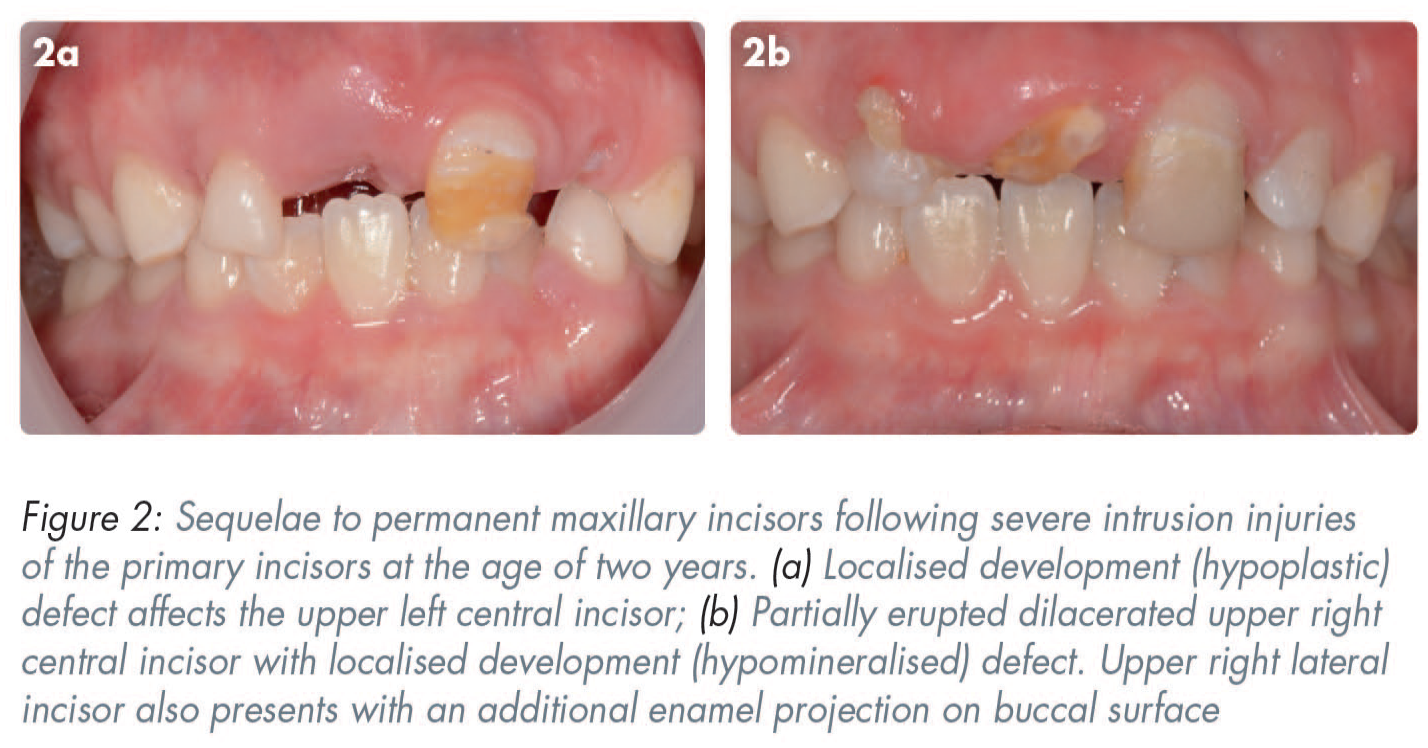
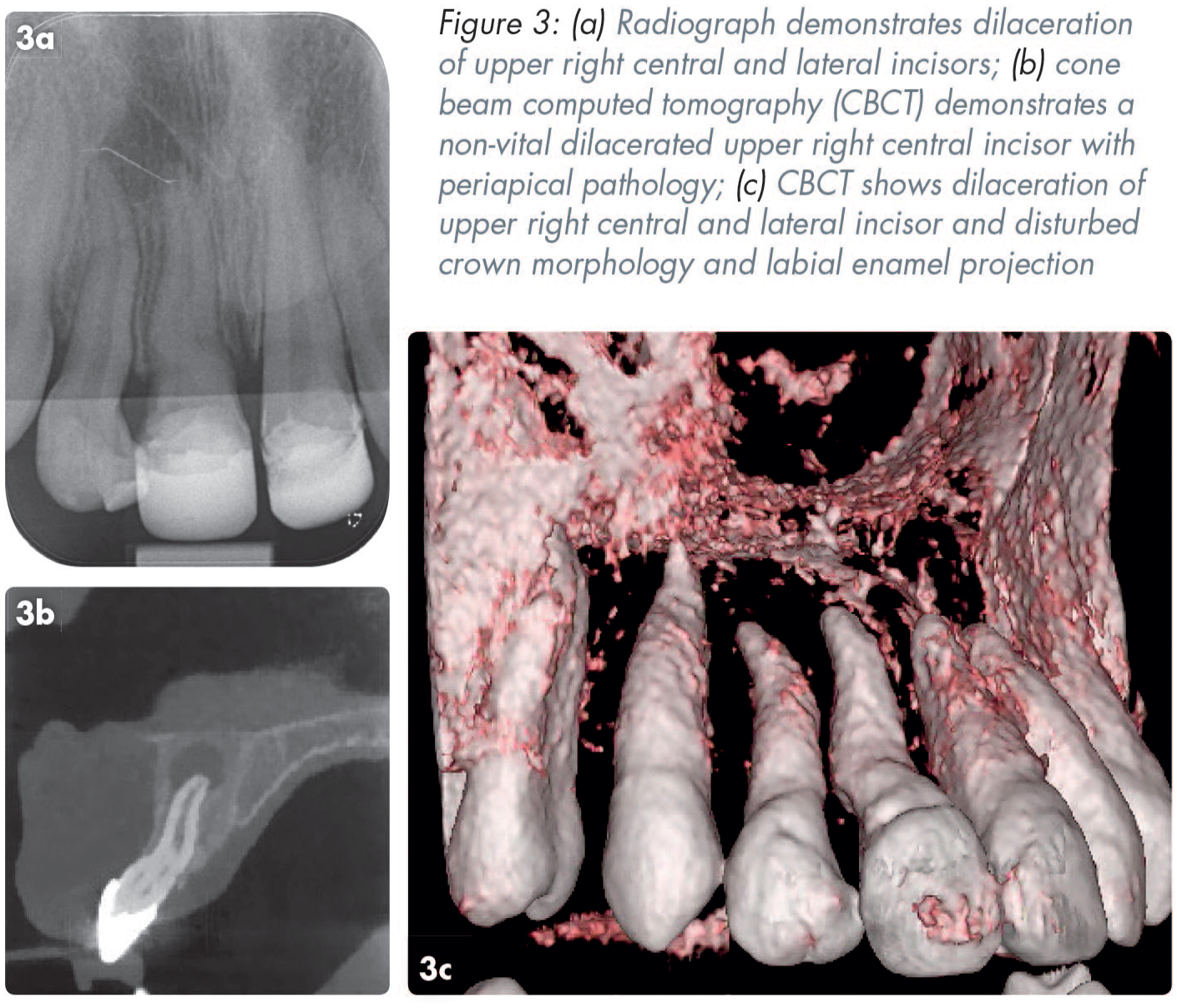
Trauma occurring in the primary dentition has the potential to impact the unerupted permanent successor. The likelihood of this is dependent on the age of the child and the type of TDI. Children under the age of two at the time of TDI as well as those with intrusion and avulsion injuries are most likely to sustain damage to the underlying tooth germ. 31 Three-quarters of the time, any damage to the permanent tooth is mild, 32 however patients and their families should routinely be informed of the risk of damage to unerupted successors. Complications include local developmental or enamel defects to the crown, changes to or delay in eruption patterns, and in more severe cases dilaceration, root duplication, cessation of root development or odontome formation of the permanent successor (Figures 2 and 3).33,34
Traumatised permanent tooth
The severity and nature of the TDI in combination with patient age and stage of root development can affect the prognosis of a traumatised permanent tooth. 30 Sequelae in the permanent dentition include discolouration, pulp canal obliteration, pulpal necrosis, and root resorption.
Discolouration
Discolouration is a potential sequela of dental trauma; it does not necessarily indicate irreversible damage but should be monitored closely alongside other clinical and radiographic features. The timing, location and hue of the discolouration may be a clue to the diagnosis and pulpal status of the traumatised tooth. Parents and guardians should be informed of the possibility of colour change at the time of trauma or at a later point.
Initial discolouration of a pinkish or grey hue is a result of intracanal haemorrhage at the time of trauma. In a tooth that maintains pulpal vitality, this colour change is transient and improves over a period of three to six months. 35 Persistent grey discolouration (for more than six months) while highly suggestive of pulpal necrosis, is not alone a justification to commence endodontics without other features of pulpal necrosis. 18
In cases of pulp canal obliteration (PCO) (see next section) a traumatised tooth will appear yellower with reduced translucency owing to new tertiary dentine being laid down in the root canal. 36 This is usually seen between three and 12 months following a TDI and is a clear sign of pulpal survival. 37
Pulp canal obliteration (PCO)
PCO occurs to some degree in 4–24% of traumatised teeth and is identified clinically as a yellowing discolouration and increased radiopacity in the canal. 36 This is caused by the calcification of the pulp canal space in response to the sustained injury. It is most frequent in immature teeth with severe luxation injuries such as lateral luxation. 21 PCO only occurs if the tooth is vital, therefore the presence of PCO is not an indication to commence endodontic treatment. Despite lack of response to sensibility tests, it is reported that less than 1% of teeth with PCO develop periapical pathology and pulpal necrosis per annum. 38 The presence of PCO does not warrant any active treatment, however if the tooth becomes symptomatic, an onward referral is reasonable due to the complexity of root treatment.
Anklyosis-related replacement resorption
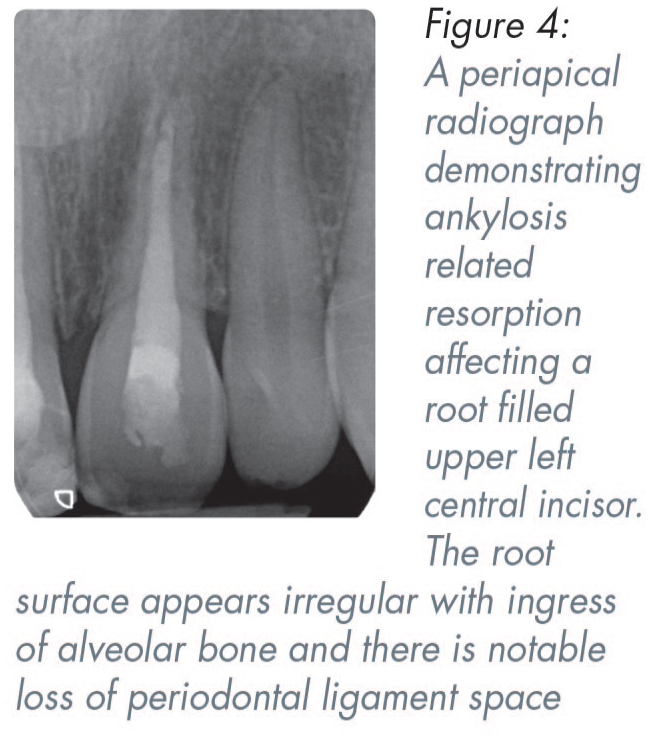
Ankylosis-related replacement resorption may occur following avulsion, intrusion and occasionally lateral luxation injuries which damage the periodontal ligament (PDL) cells adjoining the root surface. 39 The damage occurs from crushing in luxation injuries or from mishandling an avulsed tooth (incorrect storage medium or prolonged extra-oral dry time). These injuries lead to ischaemia of the PDL and cementum cells and result in the root surface being replaced by bone. 40 The process is irreversible. The speed of resorption is related to the speed of bony turnover and is more rapid before or at the time of the pubertal growth spurt. Radiographically, areas of root surface may appear to be replaced by bone with loss of lamina dura, with the resulting root appearing irregular (Figure 4). Clinically the affected tooth may have reduced mobility and a dull metallic sound on percussion. 40 In a growing patient, infraocclusion may be noted (vertical discrepancy of the crown height or gingival margins compared to the adjacent teeth) (Figure 5). In these cases, prompt referral to a specialist team is advised, and patients and their families should be prepared for the guarded prognosis with consideration given to future decoronation, root burial, and prostheses. 19

Infection related resorption
Infection related resorption (previously known as inflammatory root resorption) can occur following pulpal necrosis and is driven by bacteria in combination with damage to the root surface. Avulsion and intrusion injuries are at most risk of developing this type of resorption.39,40 It is best practice to commence root canal treatment in mature teeth seven to ten days post avulsion or intrusion injury, to prevent initiation of infection related resorption.21,22 A tooth undergoing infection related resorption will be unresponsive to sensibility testing, and radiographically appear with localised loss of root surface and associated radiolucency of the adjacent bone. 40 Endodontic therapy should be initiated as soon as resorption is identified to prevent progression.19,21 This type of resorption process can progress rapidly and render the tooth unrestorable within a few months. Therefore, referral to paediatric dental teams should not prevent the primary care clinician from initiating endodontic therapy when it is required.
Management of open apex
Although open apex teeth requiring endodontic treatment warrants onward referral to specialist paediatric teams, the initial extirpation, is suitable for primary care practitioners. Moreover, it can minimise progression of infection related resorption and morbidity associated with a non-vital infected root canal. As with endodontic treatment in a mature tooth, clinicians should provide appropriate analgesia, isolation, and an access cavity appropriate for the tooth. Apex locators can be unreliable for working length estimates in immature teeth 41 therefore careful working length confirmation can be completed with the use of radiographs. Mechanical preparation should be minimal in an immature root and focus should be given to the removal of pulpal remnants and chemical irrigation to disinfect the canal, 42 typically with sodium hypochlorite. Non-setting calcium hydroxide is the recommended intracanal dressing material due to its antibacterial and anti-resorptive qualities. 43 Glass ionomer cement provides a good coronal seal compared to other temporary restorations and are the preferred material following extirpations. 44
Orthodontics
Patients with a Class 2 Division 1 malocclusion are at increased risk for TDI. 1 Early referral for functional appliances will allow the orthodontist and patient to have an informed conversation around the merits of two-phase treatments, compared to treatment in permanent dentition. Before the appropriate time for referral, provision of a mouthguard for contact sports and discussions around preventing TDIs is prudent.
Patients that have qualifying malocclusions should be referred for orthodontic interventions at the appropriate age, although it is paramount that any history of dental trauma is indicated at the referral stage. If dental trauma occurs during orthodontic treatment, liaison with the orthodontist is essential as orthodontic teams may need to complete a period of observation before recommencing active treatment with the time frame ranging from three months to two years, depending on the nature of the injury. 45 Orthodontics plays a crucial part in the management of some dental injuries where controlled repositioning is required, such as intrusion injuries. For complex injuries, multidisciplinary teams (MDTs) will consider whether orthodontic space creation or closure is required for the long-term restorative management of poor prognosis teeth. 46
Tooth loss and replacement options
TDIs can sometimes result in the immediate or long-term loss of a permanent tooth. Some options, like implants are only available in adulthood, and therefore treatment planning should be considered in the short and long term. A further challenge is the risk of space loss in a growing patient which can reduce definitive tooth replacement options.
MDTs involving paediatric, orthodontic and restorative clinicians are in the best position to consider multiple treatment options and minimise complications in the short, medium and long term for the paediatric patient. Some options, such as autotransplants (premolar transplants), have small windows for optimum success and therefore early referral is essential in cases with significant or complex dental trauma. Clinicians should already have a good foundation of knowledge of anterior tooth replacement options including dentures, resin bonded bridges, orthodontics and implants. Literature is available to familiarise clinicians with the anticipated management options, 46 which can be useful to refer to when informing patients and their supporting guardians at the stage of referral.
Communication
Effective communication in trauma appointments is paramount in obtaining a correct diagnosis and delivering relevant and important information to patients and families. Involvement of the patient in discussions will be dependent on their age and maturity, however in most cases detailed information is likely to be tailored to the adult with parental responsibility.
Priority for communication in the initial appointment should be given to alleviating anxiety of the patient and family, provision of emergency care and delivery of oral hygiene instructions and analgesia advice. The 2020 IADT guidelines published new parental instructions for home care following traumatic dental injuries. 18 Practical advice regarding the use of cotton swabs or a soft bristled toothbrush should be included in the delivery of this information. Distributing a written copy of the advice or signposting to an electronic version is helpful as the full verbal instructions are unlikely to be retained in the high stress environment.
Managing expectations of parents/guardians is important, and they should be aware of the requirements for multiple follow up appointments and guarded prognoses as early as possible. Alongside this, identifying any risk factors for further dental trauma and mitigating this risk can also be achieved through relevant questioning. Patients that participate in contact sports are likely to benefit from a mouth guard.
Thorough conversations regarding the prognosis of teeth and long-term treatment plans should ideally be delayed to the follow up appointment where guardians may have a greater capacity to understand and retain this information. Patients should be aware of the importance of long-term follow up, and how to identify signs and symptoms that would warrant an early return. Discussions regarding this can be supported by relevant dental trauma websites and literature. 18
Conclusion
Effective management of paediatric dental trauma includes not only the clinical management of the dentition, but also ensuring the patient and their family are prepared and supported for the long-term consequences of the injury. Consideration should be given to a patient holistically regarding the best management options, with clear communication at each stage. Early involvement with multidisciplinary teams is encouraged in cases of severe dental injury. Shared care between primary and secondary care can help to optimise outcomes for children following TDIs.