
Abstract
Patients with tooth wear are commonly encountered in general dental practice. When indicated, restorative rehabilitation is often accompanied by a request from the patient for an aesthetic, tooth-coloured outcome. This article seeks to provide an evidence-based approach, focussing on the longevity of the materials which can be used for the restorative treatment of tooth wear, as well as their modes of failure and observed performance.
Prim Dent J. 2023;12(3):1-11
Learning Objectives
To identify the materials commonly used for the aesthetic rehabilitation of the worn dentition
To differentiate between the longevity of the materials
To analyse the effectiveness of the materials, to fulfil the objectives of restorative rehabilitation
To predict the consequences, following failure of the material used
Introduction
In 2018, an estimated mean global prevalence of erosive tooth wear in the permanent dentition between 20% and 45% was described. 1 Patients with signs of tooth wear are likely to be routinely encountered in primary dental care. Where the presenting tooth wear is pathological, 2 in the absence of any concerns expressed by the patient and/or the clinician, the condition may be effectively managed by the prescription of appropriate preventive measures with periodic reinforcement, accompanied by careful counselling and monitoring. 3 However, at an individual level, restorative rehabilitation may sometimes be indicated, especially when the severity of the presenting tooth wear may culminate in symptoms and the reporting of concerns.2,3
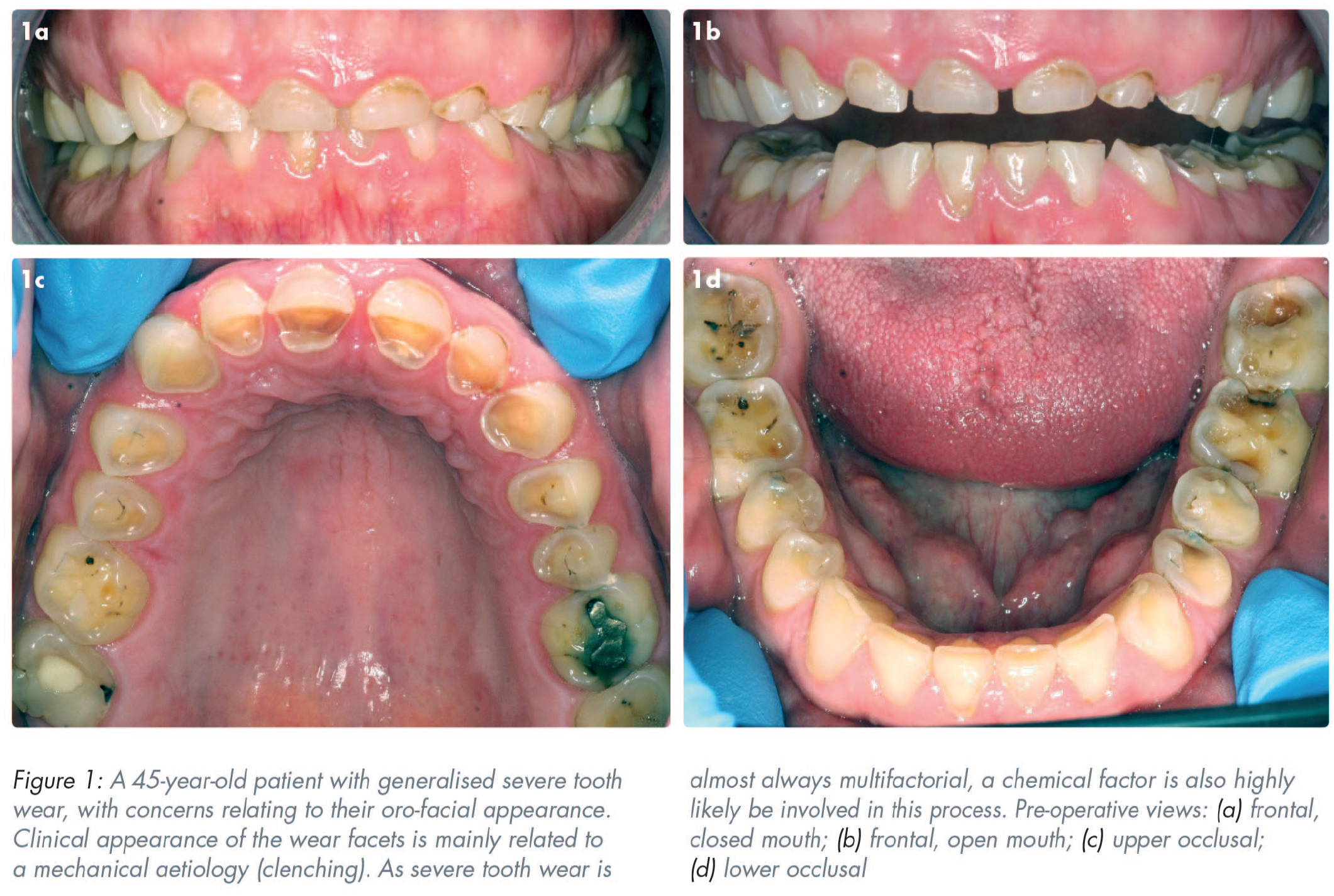
Dissatisfaction with appearance and aesthetics are concerns that have been reported by two separate studies, as the most common forms of complaint expressed by patients referred to hospital-based consultant clinics with tooth wear related problems (59% and 54% respectively).4,5 The rehabilitation of tooth wear patients may, therefore, include the use of tooth-coloured restorative dental materials as a means of addressing any aesthetically related concerns. Restoration of the worn dentition has, however, been reported to be technically challenging, time consuming, complex, and costly, frequently involving inter-disciplinary planning, 6 with accompanying high maintenance requirements. Thus, it would seem prudent to prescribe care that is supported by evidence-based protocols that offer cost-effective outcomes, acceptable longevity, and appropriate patient satisfaction. 7 A plethora of dental materials and treatment techniques have been documented for the restoration of the worn dentition. 8 Presently, however, there is a lack of clear evidence to favour the use of one type of dental material or a specific application technique (direct or indirect) for the treatment of generalised tooth wear.7,9 Figure 1 is an example of a patient with tooth wear, with concerns relating to their orofacial appearance.
Patient reported outcome measures (PROMs)
Clinically, restorative outcomes have been assessed on reported rates of success and survival. However, it is also pertinent to consider the patients’ overall experience and the improvement in their oral health-related quality of life (OHRQoL) following the application of the treatment intervention. Higher levels of tooth wear have recently been shown to have a significant impact on the OHRQoL. 10 A patient’s experience with any type of restorative rehabilitation may be appraised using patient reported outcome measures (PROMs). Significant improvements in the OHRQoL orofacial appearance and the self-perception in the quality of speech function have been reported where full mouth rehabilitation for tooth wear was provided using direct and indirect composite resin restorations.11,12 Self-reported improvements in the ability to eat and chew following the application of direct, full-mouth composite resin restorations for the treatment of generalised tooth wear, have also been described in a separate investigation; however, significant improvements in masticatory performance in the short term were not observed in this study. 13
Restorative management of tooth wear
The restorative rehabilitation of moderate to severely worn dentition may include the use of conventional (mechanically) retained indirect restorations, or the use of adhesively retained restorations, often applied using minimal intervention. As per the 2017 European Consensus Statement on Management Guidelines for Severe Tooth Wear, 2 where possible, restorative treatment strategies should favour the use of minimally invasive, additive techniques, enabling further options for contingency planning. Tooth-coloured restorative materials and techniques prescribed for the treatment of more severe forms of tooth wear include:
direct (chairside) composite resin restorations
indirect (laboratory fabricated) composite resin restorations
polymer-infiltrated ceramic network (PICN), computer-aided design and manufacturing (CAD-CAM) restorations
all ceramic restorations
conventionally retained tooth-coloured crowns
The aim of this paper is to review the available evidence relating to the performance of the above dental restorations for the treatment of tooth wear.
1. Direct composite resin restorations
Dental composite resin materials may be classified by the distribution and average particle size of the inorganic filler phase. The direct application of composite resin offers a minimally invasive means of achieving a potentially aesthetically acceptable outcome for the treatment of tooth wear. Most composite resin materials are also well tolerated by the pulpal tissues, cost effective and the restorations fabricated in this way are readily amenable to adjustment, repair, and refurbishment. 14 The potential merits may account for the popularity of this treatment modality, and for most of the available evidence concerning the performance of restorations for tooth wear relating to the use of direct composite resin.15 -29 Figure 2 is an example of tooth wear rehabilitation using direct composite resin.

Two systematic reviews have reported the performance of direct composite resin for the treatment of tooth wear.7,30 Typical causes of failure include bulk fracture, chipping, the total loss of the restoration, caries, staining, discolouration, the presence of a marginal step, the loss of vitality and tooth fracture. The earlier systematic review by Mesko et al. (2016), 7 alluded to mean annual failure rates for the performance of direct composite resin restorations for the treatment of tooth wear to range from 0.7% (‘good’) to 26.3% (‘unacceptable’) and the worst clinical behaviour was associated with the use of microfilled materials compared to microhybrid composite resins. The more recent systematic review of the interventions after restoring worn occluding surfaces of anterior and posterior teeth with composite resin, by Kassardjian et al. (2020), 30 reported an overall intervention rate of 11.7% (range of 0% to 51.6%) and annual intervention rates of between 0.8% and 17.8%. Annual intervention rates cannot, however, be directly compared to annual failure rates, as the need for intervention may not always constitute a failure.
Fractures have been described as the most common type of failure encountered with the restoration of the worn dentition, using direct composite resin. 23 The types of fracture commonly observed include cohesive failure at the restoration margin and chipping; bulk fractures are less frequently observed. The fracture resistance of a bonded resin composite-based material may be influenced by the material composition and strength, the layer thickness, a disparity in the elastic modulus between the restorative material and the bonding substrate, the characteristics of the residual tooth tissue and how meticulously the bonding protocol is followed.31-33
Performance of direct resin composite restorations for the treatment of tooth wear
The available longevity studies often distinguish between the direct application of resin composite for the treatment of localised tooth wear (where restorations are frequently placed in the supra-occlusal location, utilising the concept of relative axial movement – the ‘Dahl’ concept),34,35,36 or for the treatment of generalised tooth wear. However, many of the available longevity studies include shorter observation periods and/or smaller samples sizes. Furthermore, comparing the outcomes of the individual investigations is often compounded by variations in the treatment protocols and the criteria applied for the assessment of failure. In Table 1, a summary has been provided of the outcomes of some clinical investigations into the performance of different tooth-coloured restorations for the treatment of tooth wear, with a focus on longer term investigations and/or where relatively larger numbers of restorations have been included in the study sample. There then follows information from a selection of investigations, to include some case series/prospective studies and the outcomes of some randomised controlled trials.
TOOTH-COLOURED RESTORATION MATERIALS: SUMMARY OF Clinical STUDIES
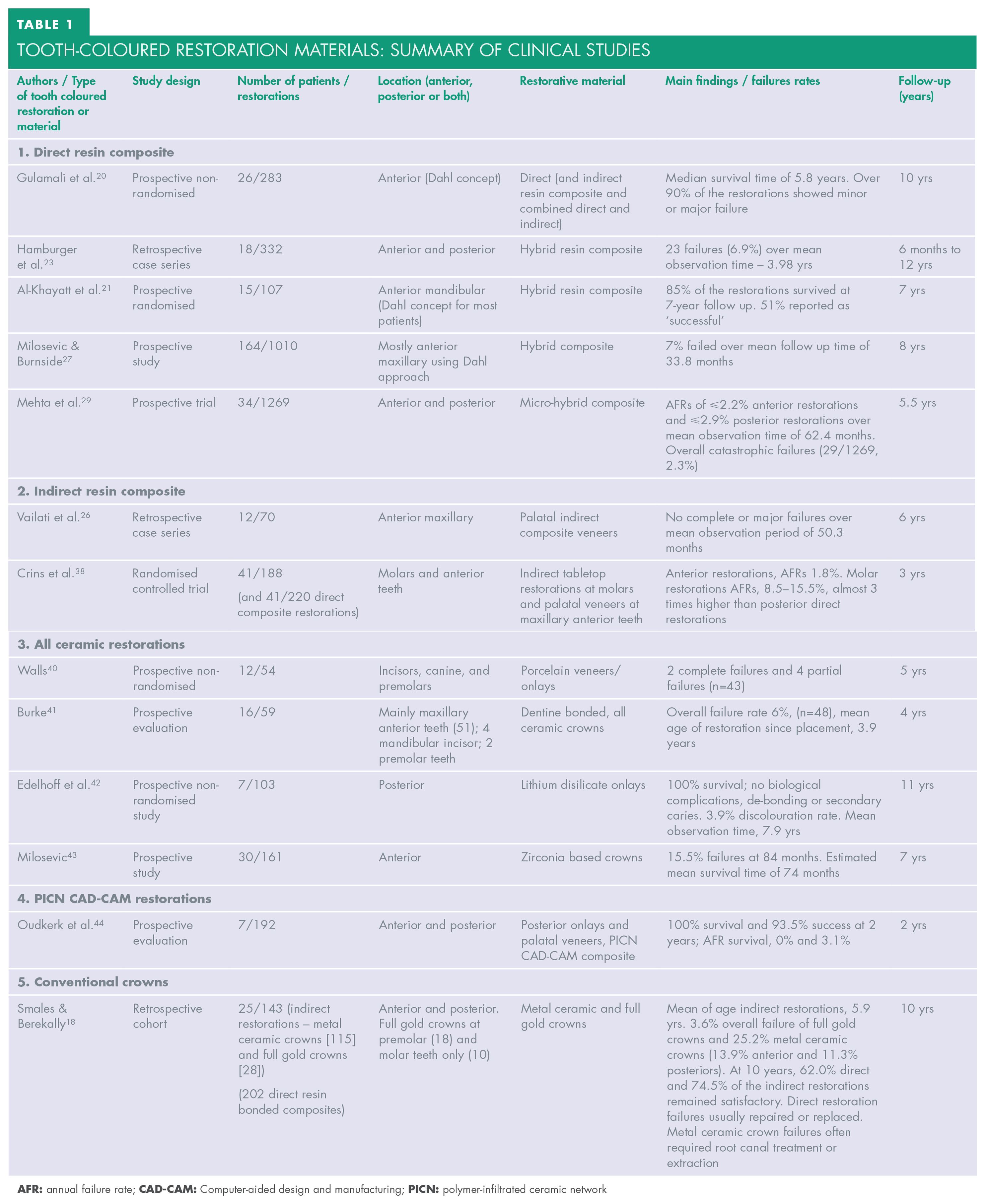
Gulamali et al. (2011) 20 documented the ten-year survival of 283 localised supra-occlusal anterior maxillary (Dahl) restorations prescribed for the treatment of tooth wear; direct and indirect composite resin restorations were included in this study. A median survival time of 5.8 years was reported, however, over 90% of the restorations displayed signs of major or minor failure, usually due to wear, fracture, and marginal discolouration. Factors that significantly impacted on the survival of the restorations included the aetiology of the tooth wear, the incisal relationship, the materials used and the nature of the antagonistic dentition. A separate, eight-year prospective study into the survival of 1,010 direct composite resin restorations (most of which had been placed at the anterior maxillary teeth using the Dahl approach) with a mean follow up time of 33.8 months, reported an overall failure of 7% of the total restorations; failure was defined by the presence of a total de-bond or a chip. The lack of posterior support was identified as a major factor associated with failure. 27
Unfortunately, only limited data is available for the performance of localised posterior direct composite resin restorations for the treatment of tooth wear.17,36 A three-year randomised clinical study comparing the performance of direct composite resin for the restoration of worn posterior teeth, reported an overall failure rate of 21%; the use of direct composite resin restorations for this application was contraindicated by the authors. 17 In the latter study, the prescription of a microfilled resin composite material was suggested to have been a factor that may have influenced the observed outcomes. However, recently, high levels of success have been described by Hoekstra-van Hout et al. (2023) 36 relating to the use of direct posterior composite restorations placed using the Dahl concept for the treatment of localised tooth wear, with high levels of patient satisfaction.
As part of a large prospective study, Mehta et al. (2021) 29 reported the performance of 1,269 direct composite resin restorations, prescribed for patients with severe (generalised) tooth wear, requiring full-mouth rehabilitation. Restorations were placed by experienced operators. Over a mean observation time of 62.4 months, overall annual failure rates of ⩽ 2.2% (anterior restorations) and ⩽ 2.9% (posterior restorations) were reported. Only 2.3% (29/1,269) of the overall restorations displayed catastrophic failures, with the observation period clipped to 5.5 years. In this investigation, molar tooth restorations (versus premolar tooth restorations), posterior mandibular restorations (versus posterior maxillary restorations) and anterior restorations requiring two further sessions for completion, were associated with significantly higher risks of failure.
In summary, the application of direct composite resin restorations for the treatment of worn teeth may offer an appropriate option, where at least survival data into the medium–longer term is available. However, factors such as operator skill, the type of tooth restored (molar versus other teeth), the aetiology of the tooth wear, the treatment technique, 37 the nature and quantity of tissues for bonding and the selection of appropriate types of dental materials may influence the outcomes. Further research is required to properly understand the importance of all the factors that may influence the prognosis of restorations provided using this modality. Patients must, however, be made aware of the need for routine maintenance when prescribing direct resin restorations as part of the process of attaining informed consent.
2. Indirect composite resin restorations
Compared with direct application, indirect (extra-orally fabricated) composite resin restorations have the scope to offer superior occlusal and inter-proximal form, with the possibility of reduced chair-side time, especially when multiple restorations are indicated. However, the additional costs, the possible need to remove hard tissue undercuts, risk of the display of the cementation line and wear/breakdown of the cementation material, should be carefully discussed while seeking informed consent. Nevertheless, indirect composite resin restorations are more amenable to intra-oral repair and adjustment and less abrasive to the antagonistic surfaces, than ceramic and zirconium-based materials.
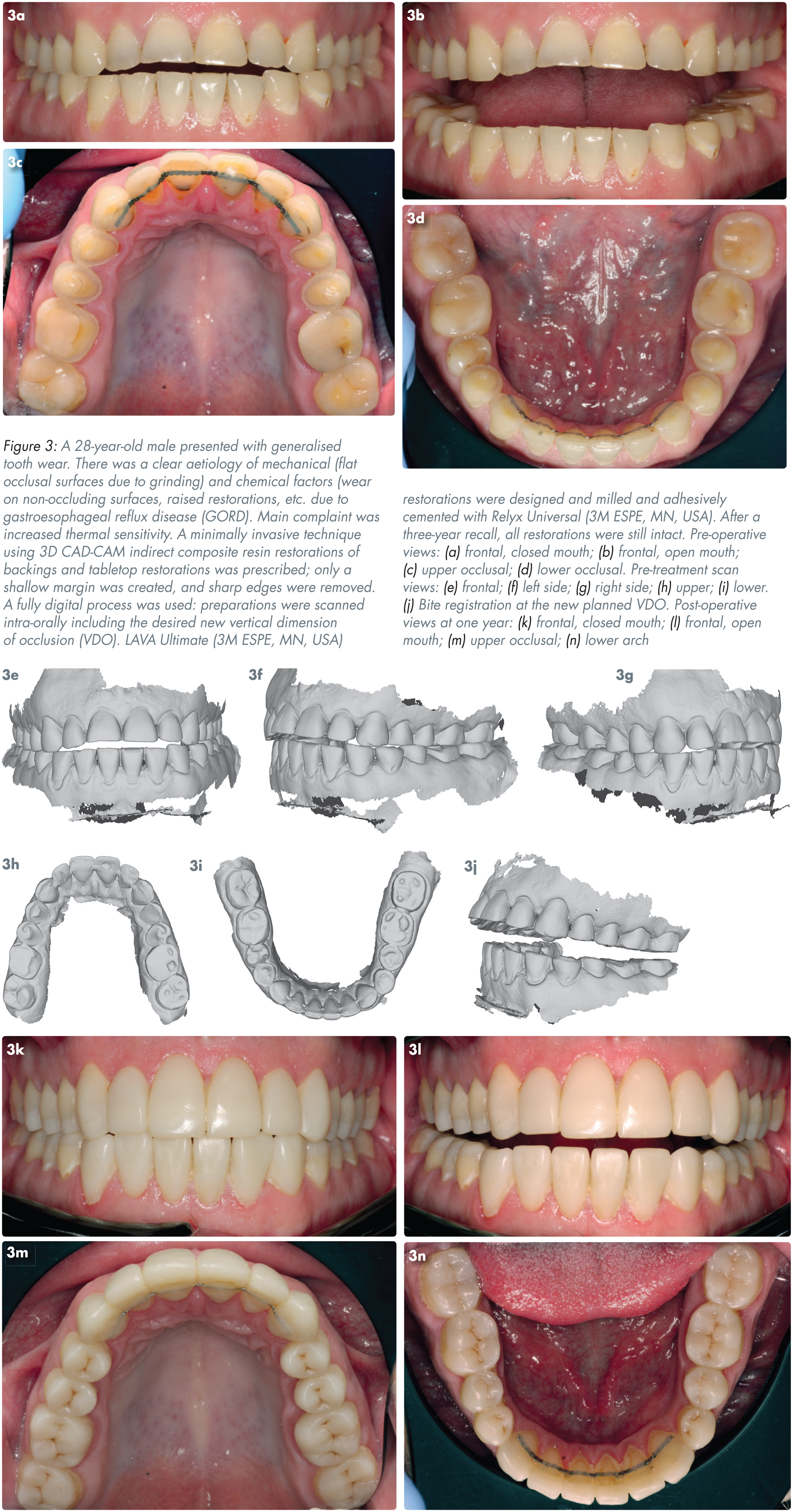
Traditionally, indirect composite resin restorations are fabricated on a die stone, with initial light curing followed by a post-curing phase, aimed at increasing the level of polymerisation conversion. Methods for post curing include the use of light, heat, pressure nitrogen or a vacuum. The latter processes may enhance the fracture toughness, tensile strength, wear resistance, and the colour stability of the restorations. More recently, pre-polymerised blocks of resin materials formed by compressing and polymerising a filler and monomer that may be used with CAD-CAM applications, are being increasingly employed. These restorations may offer better adaptation/fit and superior mechanical properties, such as improved flexural strength compared to conventional resin composite, especially given that blocks are likely to be more homogenous with the reduced risks of flaws. The rapid progression of digital dentistry will likely further support the use of indirect CAD-CAM restorations for the minimally invasive management of complex dental conditions, such as severe tooth wear. Figure 3 depicts an example of a case of tooth wear, restored using indirect composite resin restorations.
A few studies have reported the clinical performance of indirect composite resin restorations for the treatment of tooth wear.20,22,26,38,39 Table 1 includes a summary of the outcomes of a selection of these investigations. Vailati et al. (2013) 26 reported the outcomes of a prospective clinical study involving the use of an interesting “Sandwich Approach” for the restoration of severely worn anterior maxillary teeth, with the placement of two separate veneers fabricated in differing materials and dissimilar paths of insertion. This approach may alleviate the need to provide invasive crown restorations. Despite relatively small sample sizes, promising functional and aesthetic outcomes were documented for the indirect palatal surface composite veneers (70 restorations) and the labial surface porcelain veneers (64 feldspathic ceramic veneers) with no complete or major failures seen over a mean observation time of 50.3 months and 49.6 months respectively.
A recent randomised controlled trial evaluated the performance of direct and artisanal indirect hybrid composite restorations placed at the palatal surfaces of maxillary anterior teeth and on the occlusal surfaces of first molars – “tabletop restorations”. 39 Indirect restorations were fabricated using a micro-hybrid indirect resin composite material (Clearfil Estenia C&B, Kuraray Noritake Dental Inc., Japan). Following light curing, the restorations were heat treated in an oven at 110–120°C for 15–20 minutes. Restorations that were replaced and restorations that displayed material chipping were recorded as failed. Direct and indirect restorations on maxillary anterior teeth showed good performance. Annual failure rates (AFRs) of 0.7% and 1.8% were respectively reported. Direct composite restorations on first molars had an AFR of 5.4%, while the indirect composite restorations had an AFR of 15.5%, indicating that artisanal indirect hybrid composite restorations in the posterior area had a 3.2 times higher risk of failure compared to the direct composite restorations. One possible reason for the difference in the performance of the direct and indirect molar restorations may have been due to variations in layer thickness. 40 A previous randomised control trial documented an unfavourable overall failure rate of 28%, with an evaluation period of three years with the use of indirect cusp coverage (micro-filled) composite resin restorations for the treatment of localised posterior tooth wear; fracture and complete loss were the most common modes of failure observed. 17
3. All ceramic restorations
All ceramic restorations used for the treatment of tooth wear may range from minimally invasive, additive veneers to full coverage, adhesively retained crowns. Restorations fabricated in adhesive ceramic such as leucite reinforced glass ceramic (IPS Empress, Ivoclar Vivadent Inc, Liechtenstein) and more recently, lithium disilicate reinforced glass ceramics (IPS e.max, Ivoclar Vivadent Inc, Liechtenstein) offer the merits of superior aesthetics, favourable abrasion resistance, reduced susceptibility for staining (due to a lower relative surface free energy compared with resin composite) and good gingival tissue tolerance. Non-etchable ceramic materials, such as those based on alumina or zirconia, offer higher strength and fracture resistance, however, these materials have inferior optical properties. The cost, the brittle nature of some ceramic materials and reduced scope for intra-oral adjustment, may favour the use of resin-based materials, at least, at the stage of attempting to verify the patient’s acceptance of planned (and often complex) changes to their aesthetic zone and occlusal scheme.
As seen in Table 1, longevity data for the use of adhesive ceramic restorations for the management of tooth wear is sparse and/or predates the use of contemporary materials.41 -44 However, a prospective clinical study reported a highly promising 100% survival rate for a sample of 103 adhesively retained minimally invasive monolithic lithium disilicate occlusal onlays, over a mean observation time of 7.9 years. 43 It was suggested that these restorations may facilitate a safer and more stable implementation of physiological occlusion and compared to direct composite resin restorations, they may offer optimal form and aesthetics for longer periods of time. While the level of tooth preparation required to accommodate minimally invasive occlusal onlays is likely to be less than for the preparation of a tooth to receive a full coverage crown, the former approach is likely to be more invasive than the prescription of a directly bonded resin composite restoration for the same application.
All ceramic, full coverage, adhesively bonded restorations may also be prescribed following a traditional, subtractive protocol. In 2014, Milosevic 44 reported the survival of 161 zirconia based (Lava™ 3M ESPE, St. Paul, MN, USA) crowns for the management of severe anterior tooth wear, over a median follow up period of 72 months. A relatively low overall failure rate of 15.5% was observed. Failures were attributable to total de-bond or to minor delamination chips within the ceramic layer. The presence of an edge-to-edge incisor relationship as well as an underlying tendency towards developing tooth wear because of attrition or bruxism, were also linked to higher risk of failure. More recently, Hammoudi et al. (2022) 45 reported long-term success as part of a randomised clinical trial with an observation period of up to six years, when evaluating the performance of pressed lithium disilicate crowns (362 restorations) and translucent zirconia crowns (351 restorations) for the treatment of extensive tooth wear. All crowns were adhesively luted using a resin-based cement, and success rates of more than 98% were reported for both types of crowns. The crowns assessed in the latter study were applied at anterior and posterior teeth.
4. Polymer infiltrated ceramic network (PICN) materials
PICN materials were developed with the aim of offering mechanical properties that closely mimic human enamel such as the modulus of elasticity, enabling mechanical biocompatibility. PICN materials comprise a sintered ceramic matrix infiltrated with a polymer matrix. Restorations fabricated in PICN materials are digitally designed and milled from pre-polymerised blocks of material. Compared with the use of ceramic materials for this purpose, PICN restorations may be milled to a very low thickness (up to 0.11mm at molar teeth) and intra-oral occlusal adjustments can be performed more readily.46,47 Good mechanical and adhesive properties have also been reported with these restorations.48,49
The use of pre-polymerised blocks of PICN material for the full mouth rehabilitation using a “One-step No-prep” approach was described by Mainjot (2018) 50 with the absence of the need for tooth preparation or a provisional phase. A two-year prospective evaluation of 192 PICN CAD-CAM restorations documented very good patient acceptance where a mean increase in the vertical dimension of occlusion (VDO) of 5.09 ±0.85mm was prescribed, together with the rapid adaptation to the new occlusal scheme and survival and success rates of 100% and 93.5% respectively. 46 Minor chipping of the very thin occlusal borders was the most frequently observed complication in the latter study. As a limitation, however, further performance data is currently lacking.
5. Conventional tooth-coloured crowns
The fabrication of conventionally retained full coverage metal ceramic crowns usually involves the firing of feldspathic porcelain onto a cast coping. While these restorations have been prescribed for decades, there is the notable absence of high-quality evidence relating to their performance for the treatment of tooth wear. 51 One investigation compared the survival of direct and indirect restorations for the treatment of advanced tooth wear, over the course of a ten-year assessment period. In this investigation, survival estimates of 58.9% were reported for the directly bonded anterior composite resin restorations, and 70.3% for the indirect, anterior metal ceramic crowns. Restoration fracture was observed to be the most common mode of failure for the direct resin bonded composite restorations and the failures were often amenable to repair or replacement. In contrast, failures of the crowns were generally of a catastrophic nature, typically involving the complete loss of the restoration, which frequently necessitated subsequent endodontic treatment, or the need for a dental extraction. 18
Conventionally retained crowns may, however, be considered where the placement of adhesively retained restorations may not be achievable (e.g. in the presence of multiple units of existing failed crown restorations), or where the maintenance elements associated with the placement of direct composite resin restorations may be of significant concern to the patient. 30 However, there is the absence of clear evidence to support conventional crown restorations requiring lower levels of maintenance than reasonable alternatives for the rehabilitation of the worn dentition. Limiting the extension of ceramic (for metal ceramic crowns) may help provide a more conservative type of restoration. However, it is imperative to carefully discuss the risks of these restorations, including the recognised “biological complications,” such as the copious loss of coronal volume and risks of irreversible pulp tissue pathology.52,53 In the authors’ opinion, the primary focus of restorative interventions should be the preservation of the tooth tissues, with a secondary focus on the survival of the restoration.
Conclusion
While embarking upon the restorative rehabilitation of tooth wear, the clinician must have a clear and contemporaneous understanding of the evidence-base of the performance of the available dental materials and the treatment modalities. This information will form a vital part of the discussions relating to the attainment of consent. Where possible, the least invasive option should be given primary consideration, enabling effective contingency planning.
It is paramount to consider the survival of the tooth over the survival of the restorative material, to discuss the impact of tooth wear on the OHRQoL, and for the clinician to acquire the necessary knowledge and technical skills to properly execute treatment protocols.
All patients must be carefully advised of the risks of restorative failure and the maintenance needs, especially among higher-risk tooth wear patients. Restorative intervention should only be undertaken where there is a well-defined indication for treatment.