
Abstract
This article details the unusual presentation of an oral squamous cell carcinoma (SCC) referred to secondary care during the COVID-19 pandemic. The patient’s chief complaints were trismus and pain from a lower left partially erupted third molar, which was assumed to be pericoronitis-related on referral. Intra-oral examination was difficult due to the patient’s symptoms, but radiographic assessment of an orthopantomogram (OPG) showed a pathological fracture and poorly defined radiolucency in the lower left third molar region. Oral SCC was diagnosed after biopsy, and surgery and radiotherapy were swiftly carried out despite COVID-19 restrictions. General dental practitioners (GDPs) remain the frontline healthcare professionals in the screening and detection of oral cancer through detailed history taking and examinations. Primary care dental practitioners should always remain vigilant with patients at risk of oral cancer. Prompt referral to secondary care for further investigations and management should be made when a suspicion of oral malignancy is raised, to ensure a better treatment outcome. Video consultations have had their merits in dentistry amid the coronavirus pandemic, but face-to-face consultations are essential to establish quality patient care.
Learning Objectives
To highlight the vigilance required from general dental practitioners in screening for and the detection of oral cancer
To understand the importance of obtaining appropriate investigations in the management of oral cancer as primary care clinician, allowing prompt referral to secondary care, thereby improving the outcome, prognosis and quality of life of a patient
Introduction
With an estimated 34 new cases of head and neck cancer (HNC) diagnosed every day, it is the eighth most common cancer in the UK, with incidence peaking between the ages of 70–74.1,2 Primary care dental professionals are on the frontline in recognising abnormalities in the oral cavity and making a swift referral to the relevant secondary care centres for further investigations and management.
Presentations of HNC vary in symptoms and clinical appearance. Squamous cell carcinoma (SCC) is the most common type of tumour affecting the head and neck region. Long-term prognosis is largely dependent on the stage of the cancer, and unfortunately many patients present with advanced forms of SCC.3,4 As treatment often requires aggressive resection of the tumour, as well as chemo- and radiotherapy, patients with advanced stages can be left with debilitating disfigurements and changes in key motor and sensory functions in the head and neck area, subsequently resulting in the deterioration of mental health and overall quality of life.5,6
Dental access and routine treatments have been vastly restricted UK-wide during the COVID-19 pandemic which will likely lead to, if it has not already, dentists seeing more patients in general dental practice with advanced dental diseases.7,8 Though dental practices may have to cope with the overwhelming stress of the ever-increasing waiting lists affected during the pandemic, every effort should be made to ensure thorough examinations and investigations are executed in determining the need for specialist referrals, especially for those with suspected HNC.
Description
A 74-year-old male presented to the Oral Surgery department at the University Dental Hospital of Manchester after a routine referral from his general dental practitioner (GDP) for what was anticipated to be a surgical extraction of a ‘painful wisdom tooth’. The GDP assessed the patient in a face-to-face appointment, described the lower left third molar (38) as mobile, and provided a prescription for antibiotics to treat the symptoms of presumed pericoronitis.
The patient’s medical history included well-controlled asthma and hypertension managed with beclometasone inhaler, amlodipine, atorvastatin, and perindopril. He was a retired press operator who had never smoked and rarely consumed alcohol.
During the patient’s appointment at the Oral Surgery department, his main complaint was an ‘erupting’ tooth on the lower left side which had caused persistent pain for the previous six weeks and prevented him from eating and opening his mouth fully. This eventually led to minor weight loss. The patient did not appear to be cachexic on presentation. He denied any altered sensation of the lip, chin or tongue.
Extra-oral clinical examination revealed no palpable lymph nodes, swellings, or significant trismus. There was a palpable step-deformity in the lower left border of the mandible with no marked tenderness. Intra-orally, tooth 38 was partially erupted with the presence of operculum. The associated soft tissue was extremely tender to palpation and appeared inflamed with slight rolled margins.
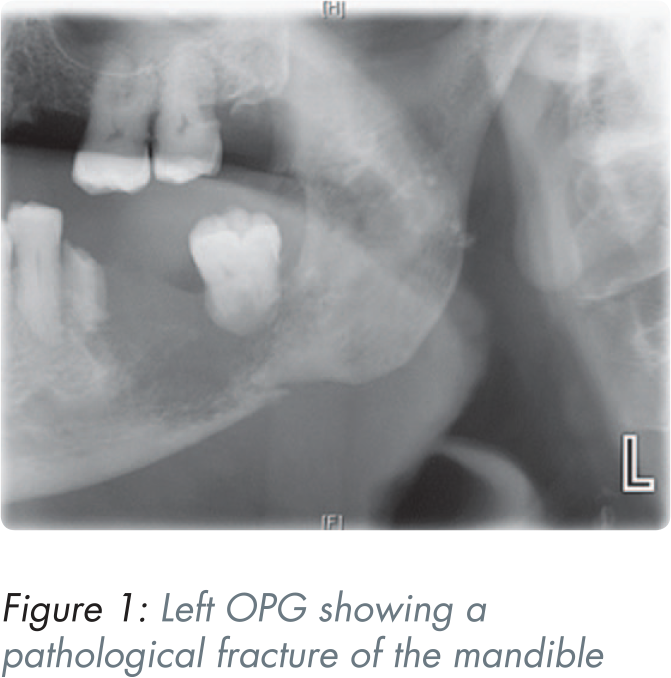
A left orthopantomogram (OPG) taken during the consultation appointment showed an incidental finding of a large area of poorly defined radiolucency extending from the lower left first molar (36) retained root to the distal region of the impacted 38 with an associated pathological fracture (Figure 1).
The patient denied the use of bisphosphonates, anti-resorptive, and anti-angiogenic drugs as well as previous radiotherapy, ruling out the diagnoses of medication-related osteonecrosis of the jaw (MRONJ) or osteoradionecrosis (ORN).
Suspecting a malignant process, incisional biopsies of the soft tissue adjacent to tooth 38 and curettage of the cavity within the left mandible were carried out urgently at the consultation appointment. The patient was then referred to the Oral and Maxillofacial Surgery (OMFS) department under the ‘two-week wait’ pathway for suspected oral cancer.
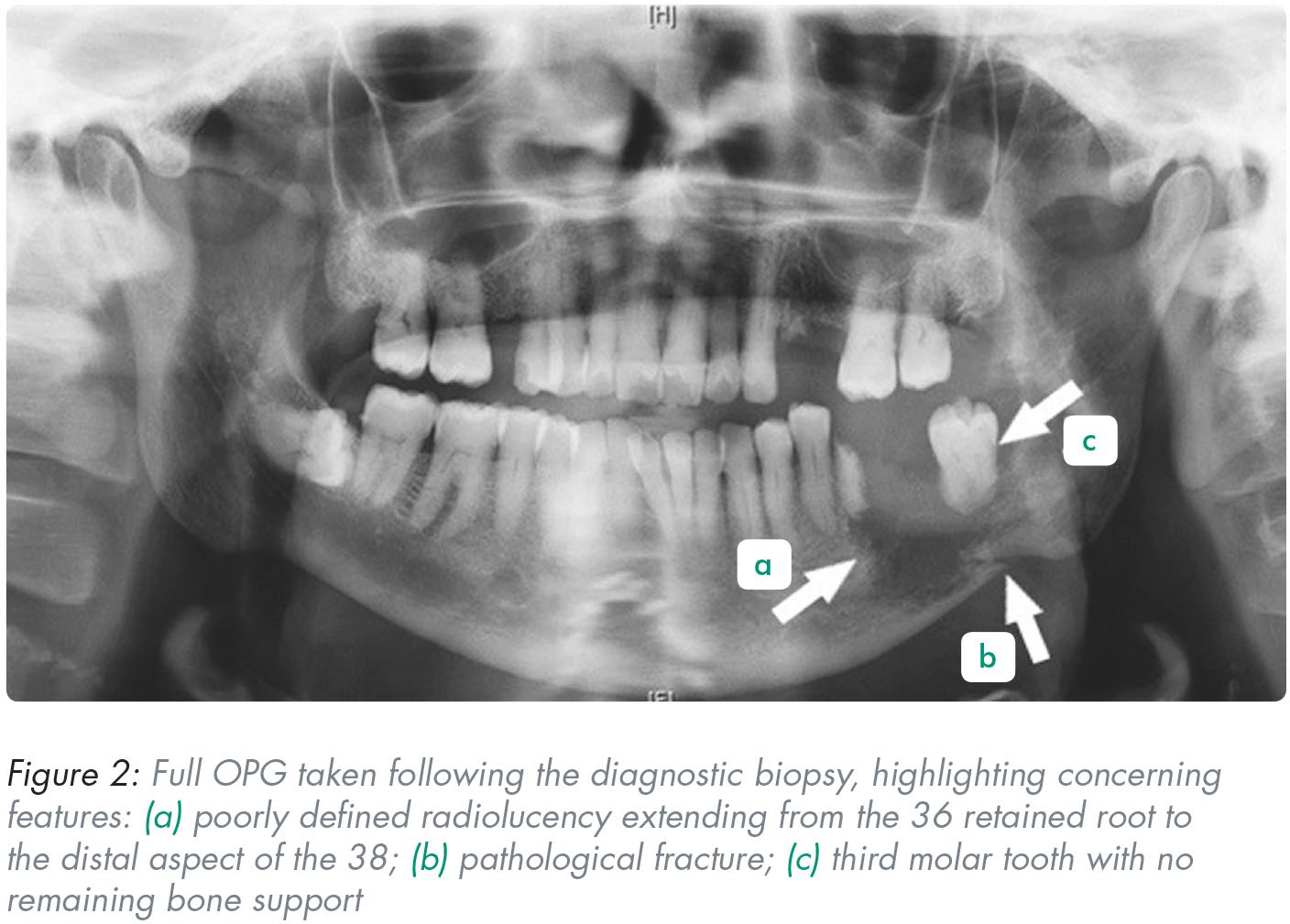
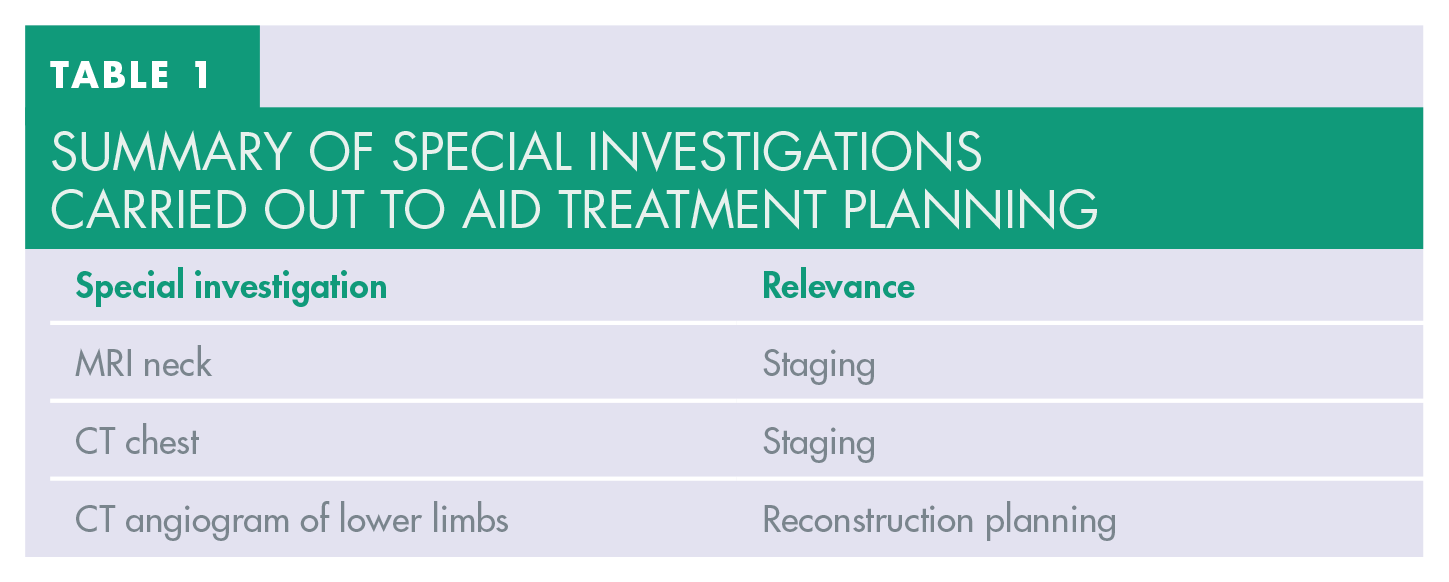
Histopathological analysis and clinical staging confirmed a poorly differentiated and invasive SCC of the left mandible, with no involvement of the nodes or further metastases. A full OPG (Figure 2) along with further necessary investigation (Table 1) were carried out within ten days from the biopsy-proven diagnosis of oral SCC. The patient received his cancer treatment thereafter thus conforming to the Trust’s commitment in keeping in-line with the NHS cancer treatment care pathway, despite COVID-19. 9
Summary of special investigations carried out to aid treatment planning
The treatment included a temporary tracheostomy, left selective neck dissection for the removal of lymph nodes, resection of the tumour and reconstruction of the mandible. After the Trust’s essential 14-day isolation period in line with the COVID-19 regulation prior to an operation, the surgery was executed as planned.
Histopathological analysis of the tumour revealed a poorly differentiated SCC with aggressive and highly infiltrating features. The pathological staging confirmed the involvement of three lymph nodes with metastatic SCC, but no further distant metastases. To reduce the risk of tumour recurrence, the patient was referred for adjuvant radiotherapy.
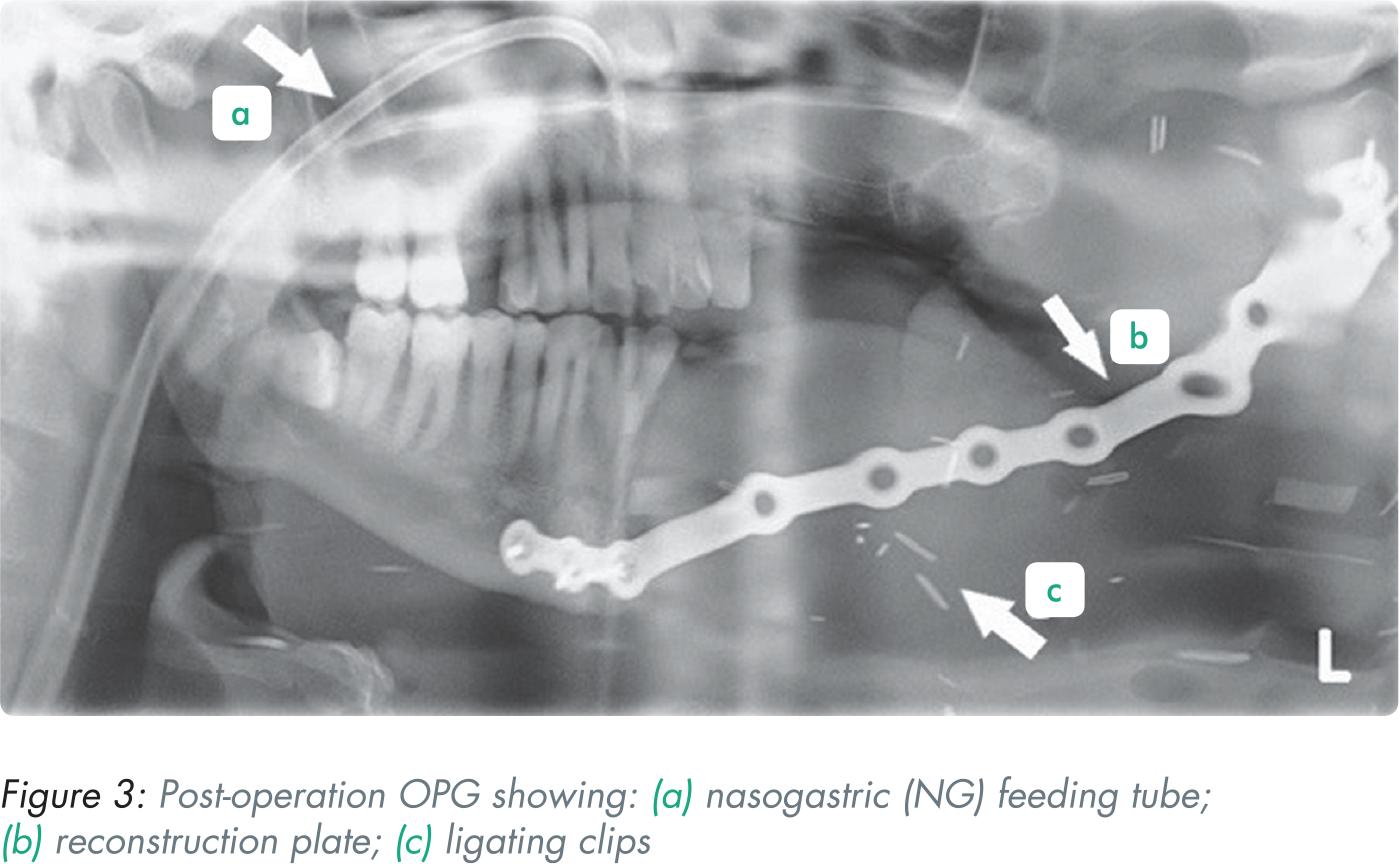
Figure 3 shows a post-operative OPG taken nine days after surgery. The radiograph revealed reconstruction of the mandible following tumour resection, with the multitude of ligating clips on blood vessels appearing as clusters of radiopaque lines.
Discussion
Taking the impact of COVID-19 into account resulting in the North West Tier 3 restrictions and subsequent UK national lockdown in late 2020, the patient still experienced timely and appropriate care provision for SCC despite the profound health service disruption. The patient was assessed by his GDP following the national re-opening of general dental practices in the summer of 2020. The GDP saw the patient presenting with pain in a timely manner and subsequently referred him to Manchester Dental Hospital where he was seen three weeks after the initial referral despite a backlog of referred patients. The vital information provided by the GDP in the referral, including severe pain which had affected the patient’s quality of life, expedited the triage process in this case, resulting in a prompt face-to-face consultation appointment at the Oral Surgery department. The University Dental Hospital of Manchester was the main secondary care institute with the availability of face-to-face consultation facilities for referred dento-alveolar cases in Greater Manchester in late 2020. Therefore this case was picked up swiftly and managed in a timely manner. Should the GDP opt for the extraction of tooth 38 in general dental practice due to its mobility, the patient would be likely to return to his GDP at a later stage presenting with pain from the non-healing socket with possible displacement of the pathological fracture, ultimately resulting in delayed cancer diagnosis.
Should there be no face-to-face consultations available in primary or secondary care settings, a video consultation could be utilised to ascertain and establish a patient’s presenting complaint. The emergence of video consultations during the COVID-19 pandemic has revolutinised the patient consultation process in medicine and dentistry to keep in-line with social distancing policies. Studies have shown that video consultation is a useful, and beneficial tool in managing patients remotely.10,11 In fact, some patients found this mode of consultation more convenient as they could avoid travelling long distances for a face-to-face consultation. Remote video consultation is also beneficial to medically-vulnerable patients or members of staff who are isolating and able to work from home. 12 However there are also downsides to remote video consultation, especially in the field of dentistry. Dentistry deals with pathologies surrounding the oral cavity and dentitions. The oral cavity is a confined space where visualising the presenting complaint through a video camera is challenging, placing the clinician in a difficult position and subsequently delaying the diagnosis. Additionally, this consultation method could potentially omit sinister lesions like oral cancer. A face-to-face appointment becomes mandatory when a suspicion of cancer is raised during a video consultation. This has presented a new challenge to clinicians where a critical judgement would have to be made whether a face-to-face consultation is required. This is fundamental in determining the treatment modality and outcome of a patient. 13 With the reduction of COVID-19 restrictions, there will be a large backlog of patients awaiting assessment and treatment in both primary and secondary care. The combination of video and face-to-face consultations in dentistry has thrived throughout the pandemic: it has a role to play in reducing the backlog of patients, is cost-effective to the service, and also supports social-distancing policy. This approach also exercises a clinician’s ability to triage cases according to their urgency, refining skills in prioritising patients who need acute attention. Additionally, where a multidisciplinary team is involved in head and neck oncology treatment, it allows for a proportion of the appointments with supporting medical staff to be carried out remotely to reduce travel needs for patients, for example the provision of smoking cessation advice or mental health support for patients undergoing oral cancer treatment.
While high risk cancer patients will always require face-to-face assessments, the benefits of remote follow-ups and reviews have become evident for regular- or low-risk patients in primary and secondary care settings amid the pandemic. In order to curb the rapid spread of the COVID-19 infection, especially with the emergence and development of the COVID-19 Omicron variant, it is vital that we continue to utilise the advancement of technologies in telemedicine/teledentistry in an appropriate manner to minimise disruption in the quality of care provided to patients, while ensuring compliance to current standards. 14
As described by the GDP in this case, the unusual finding of mobility of the partially erupted tooth together with recent weight loss should raise a clinician’s suspicion at the initial assessment appointment.15,16 Detailed social, medical, and dental histories are crucial to establish the presence of risk factors, together with appropriate special investigations, thereby allowing the derivation of differential diagnoses to aid treatment planning. 17
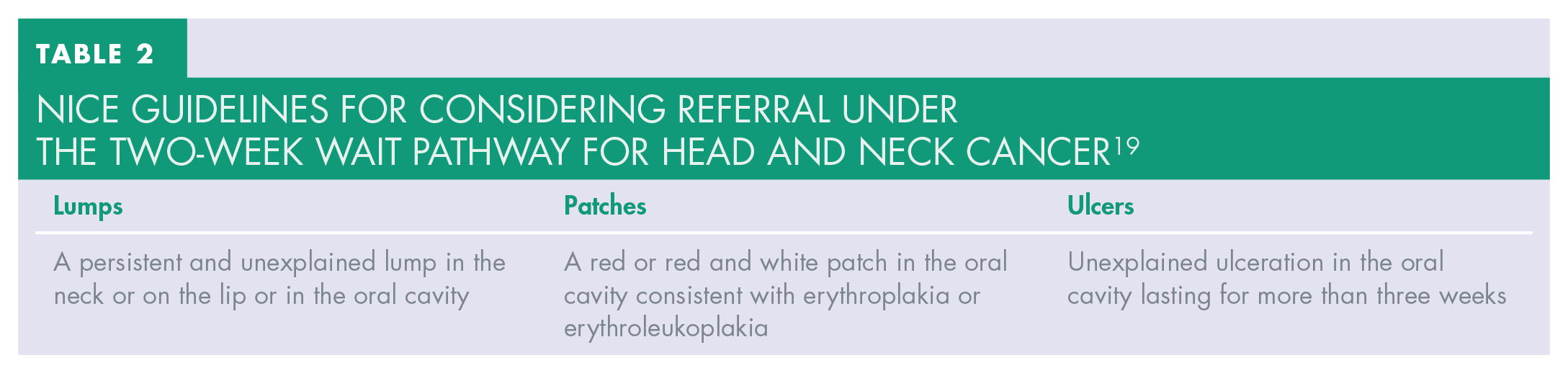
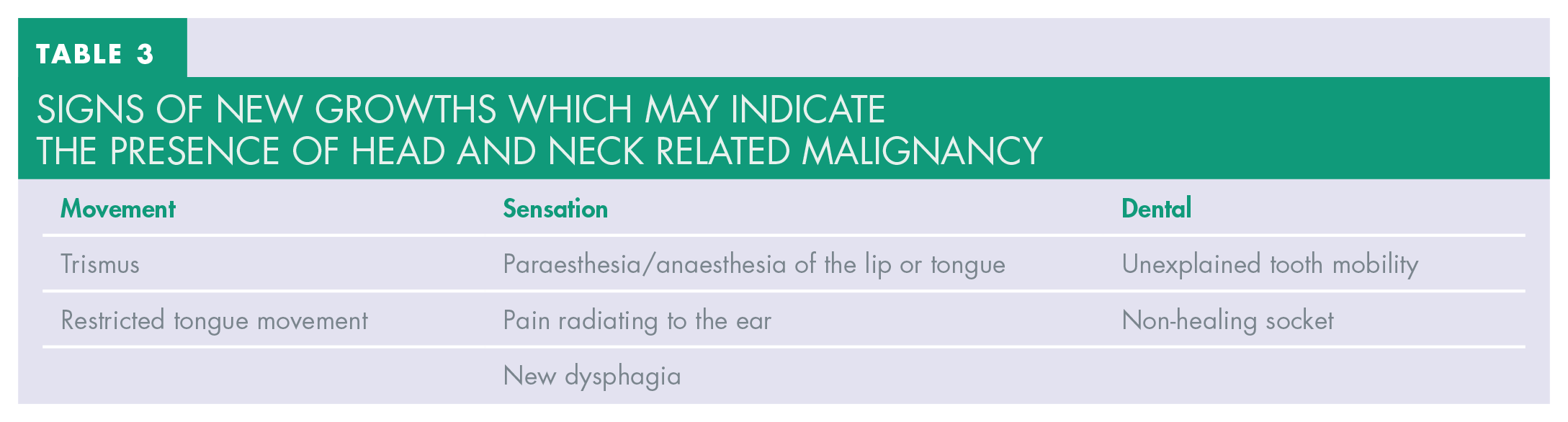
Despite the ease of COVID-19 related restrictions in dental care, there still remains a backlog of patients awaiting assessment and treatment in primary and secondary settings. In order to appropriately triage and manage potentially high risk cases, a thorough examination of the patient’s presenting complaint are pivotal, including the assessment of their social, medical, dental, and drug histories. The Oral Cancer Recognition Toolkit, developed by the British Dental Association together with Cancer Research UK, provides an excellent source of continuing professional development activities for dental clinicians in keeping up with their knowledge in oral cancer screening, detection, and prevention. 18 The National Institute for Health and Care Excellence (NICE) also provides up-to-date guidance for referring high risk oral cancer patients under the two-week wait pathway and this is outlined in Table 2. 19 Other concerning signs on examination include any new unexplained growths. These may not always be readily visible, however their presence can manifest in different forms as summarised in Table 3. 20 The most common sites for oral SCC are the tongue, followed by the floor of the mouth. 21
NICE guidelines for considering referral under the two-week wait pathway for head and neck cancer 19
Signs of new growths which may indicate the presence of head and neck related malignancy
The patient in this case, diagnosed with oral SCC, lacked the major known risk factors of tobacco smoking, betel nut chewing or alcohol drinking. In cases of oropharyngeal cancers, another major risk factor is human papillomavirus (HPV). 22 Oral HPV infections can be sexually acquired and an increased number of lifetime sexual partners has been shown to increase the risk of developing oropharyngeal cancer. 23 In recent years the incidence of oropharyngeal cancer has been on the rise amongst people in their forties and focus has been drawn especially to those who do not consume tobacco.24,25 The presence of HPV in oropharyngeal cancer has seen an increase over decades, and particularly tonsillar carcinomas have the highest prevalence of HPV DNA. 26 Studies from the US found that over 70% of oropharyngeal cancers were HPV positive between the years 2000–2004. 27 Non-smokers with SCC who are HPV positive have been shown to have a better prognosis post-treatment compared to HPV negative cases.28,29 These tumours harbour viral antigens, making them unique and attractive for targeted immunotherapies.30,31
GDPs have a duty of care to continuously monitor the routine dental and oral health of patients who have undergone cancer treatment. While regular post-cancer treatment follow-ups are arranged by OMFS colleagues, GDPs remain the pivotal front-line practitioners in recognising abnormal oral/dental pathologies and in making prompt, urgent referrals should the need arise. Provision of oral healthcare and diet advice, prescription of fluoride preparations and topical treatments for radiotherapy-induced xerostomia should be undertaken regularly for each HNC patient. 32
Good quality radiographs remain one of the significant special investigations that can aid in the derivation of an accurate diagnosis. 33 Poorly defined radiolucencies can arise from a localised malignancy, osteomyelitis, MRONJ, ORN or metastases from other primary tumour sites. 34 The patient’s medical and drug history can therefore guide a clinician to establish jaw radiolucencies induced by medication or radiation related osteonecrosis of the jaw. Upon taking an OPG in this case, a large radiolucency which extends from the 36 retained root to 38 was noted. A pathological fracture was clearly visualised radiographically as well. Figure 2 outlines the concerning features noted in the OPG. Well defined lesions and those with corticated borders usually manifest cystic lesions, the most common being a radicular cyst which develops following pulpal necrosis from advanced caries.35,36 In this case this is not a viable diagnosis considering the poorly demarcated margins of the radiolucency surrounding the otherwise healthy and intact 38 seen on the OPG in Figures 1 and 2.
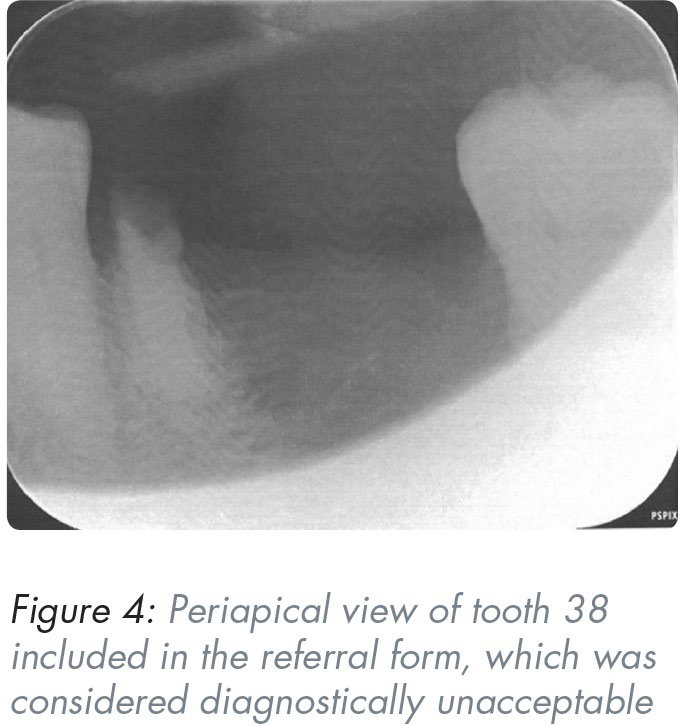
Radiographic analysis and assessment, e.g., in the evaluation of root morphology and its proximity to vital structures, are imperative in surgical planning, and pre-empting potential complications, thereby building a solid foundation for a valid consent process. 37 In this case the intra-oral periapical radiograph included in the referral letter was diagnostically unacceptable due to coning off (see Figure 4). If the patient had not been experiencing pain on initial presentation at the GDP’s appointment, this could have significantly delayed the referral process as there was “no suspicion of pathology” from the GDP’s point of view. In hindsight the suboptimal radiograph may simply have been due to the patient’s level of discomfort from the underlying pathology resulting in the inability to tolerate the film. Unfortunately, OPG facility is unavailable in many NHS-run practices and this must be taken into consideration when triaging incoming referral letters.
Conclusion
Early detection of oral cancer is crucial for the successful outcome of head and neck oncology treatment. The use of virtual consultation appointments as an adjunct to face-to-face appointments should be case selective so that the process of diagnosis and treatment is not compromised. Virtual appointments can also be used to improve follow-ups where a multidisciplinary team approach involving auxiliary healthcare staff is utilised. GDPs remain at the frontline for not only detecting and referring any dental pathologies or abnormalities not treatable in primary care settings, but they also play an important role in the provision of advice on lifestyle choices such as smoking cessation advice, alcohol consumption reduction, and adoption of a healthy diet rich in fruits and vegetables. Should a GDP encounter any concerning radiographic findings, such as poorly defined radiolucencies or unusual presentations on clinical examination as summarised in Tables 2 and 3, a swift referral to specialist units in secondary care is warranted for further investigations to ensure successful outcome in patient management and treatment.
Footnotes
Declaration of conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.