
Abstract
We evaluated the quality of general dental practitioner (GDP) tooth wear (TW) referrals to secondary care services in Kent, Surrey and Sussex.
Prospective consecutive referrals received via an electronic pathway were assessed from 1 June to 30 October 2019. Reasons for referral, patient demographics, quality of referral, opinion of the triaging clinician and outcome were assessed.
Of 671 referrals, 32% were for TW. Males were referred more commonly (1.7:1.0). The median age was 52. Patients were more likely to be referred from distant locations than places closer to the referral centre (p<0.001). Only 55% of referrals suggested a cause for the TW, 33% provided a clinical photograph and 1% recorded a tooth wear index of any type. Referring clinicians most commonly cited attrition as reason for referral (p<0.001). Those under 40 years were referred for erosion (p=0.001) and those over 40 years, attrition (p=0.019). The triaging clinician was more likely to allocate a tooth wear score of three for those under 40 years and a score of four for over 40 years (p<0.001). 47% of referrals were rejected. Males and referrals with photographs were more likely to be accepted for treatment (p=0.017 and p<0.001, respectively).
There is a high demand for specialist TW services. The number of referrals being rejected has not changed using the electronic referral system. We advocate the inclusion of mandatory fields for completion by GDPs as well as compulsory clinical photographs and tooth wear indices (Smith and Knight Tooth Wear Index or a basic erosive wear examination - BEWE index).
Learning Objectives
To understand better the patient population being referred for tooth wear problems from primary dental care practitioners to secondary care services
To evaluate the quality of information about tooth wear in the referrals via an electronic pathway
To identify potential areas for service improvement in the electronic pathway
Introduction
Tooth wear (TW) is defined as surface loss of dental hard tissues from causes other than dental caries, trauma or developmental disorders. 1 The causes include erosion, attrition and abrasion. It is generally understood that these processes do not occur in isolation and may be multi-factorial. 2 Unlike other common dental conditions, a degree of TW is physiological, with estimates suggesting around 20-38µm/year. 3 TW is pathological when the severity of signs or symptoms are disproportionate for the patient’s age.
In a systematic review of 186 prevalence studies, spanning three decades, severe TW increased from a prevalence of 3% at age 20 to 17% at age 70. 4 The most recent Adult Dental Health Survey also highlighted that the prevalence of TW is increasing for all ages. 5 As patients maintain their dentitions for longer, and with an increasingly ageing population, the need for management is likely to increase.
In the main, management is undertaken by general dental practitioners (GDPs) in primary care. Typically, the strategy for early tooth surface loss involves monitoring and implementing a prevention regime. If progression is apparent, additive composite techniques are recommended. 6 A proportion of patients will require referral for specialist care. Referrals may be influenced by factors such as the expertise and treatment philosophy of the referring clinician, the remuneration system being worked in making it uneconomic to treat multiple worn teeth, increasing medico-legal concerns, changes in undergraduate training and the increasing cost of treatment in primary care. Demand for secondary care services is therefore high and is likely to increase.
The majority of NHS specialist services in restorative dentistry are undertaken in teaching hospitals with some additional provision provided in local district general hospitals. Historically, referring practitioners would write a letter or complete a written proforma which was sent to the relevant department. Recently, there has been a transition to electronic referral systems which include mandatory fields for completion, allow for the attachment of clinical photographs and radiographs, the selection of referral centres and for communication with a triaging clinician. It has been suggested these systems would decrease the number of inappropriate referrals and waiting times as well as ensuring that patients are sent to the most appropriate centre. 7 There are, however, no published data on their use for restorative dentistry or for TW referrals. Only four previous studies could be found in the literature reporting on TW referrals, all of which utilised paper-based referrals.8–11 Reports on the efficacy of electronic systems within other specialities have been mixed.12,13
The aim of this study was to evaluate the electronic referral practices and quality of GDP TW referrals to secondary care services in a region within South East England.
Methods
Restorative referrals within the Kent, Surrey and Sussex (KSS) region were sent using the Dental Electronic Referral Service designed in collaboration with Vantage Ltd (London, United Kingdom). This is a centralised online electronic referral management system for GDPs.
Consecutive referrals were assessed from 1 June to 30 October 2019. Data collection included the reason(s) for the restorative referral. For TW referrals, the patient demographics were recorded (age, gender, referral postcode). Supporting information sent by referring GDPs was reviewed for inclusion of photographs, radiographs, tooth wear index, suspected cause and level of tooth wear.
The outcome was recorded as well as the reason(s) for rejection for any rejected referrals. The triaging clinician’s interpretation of the referral’s cause of TW and an estimate for severity of TW was assessed.
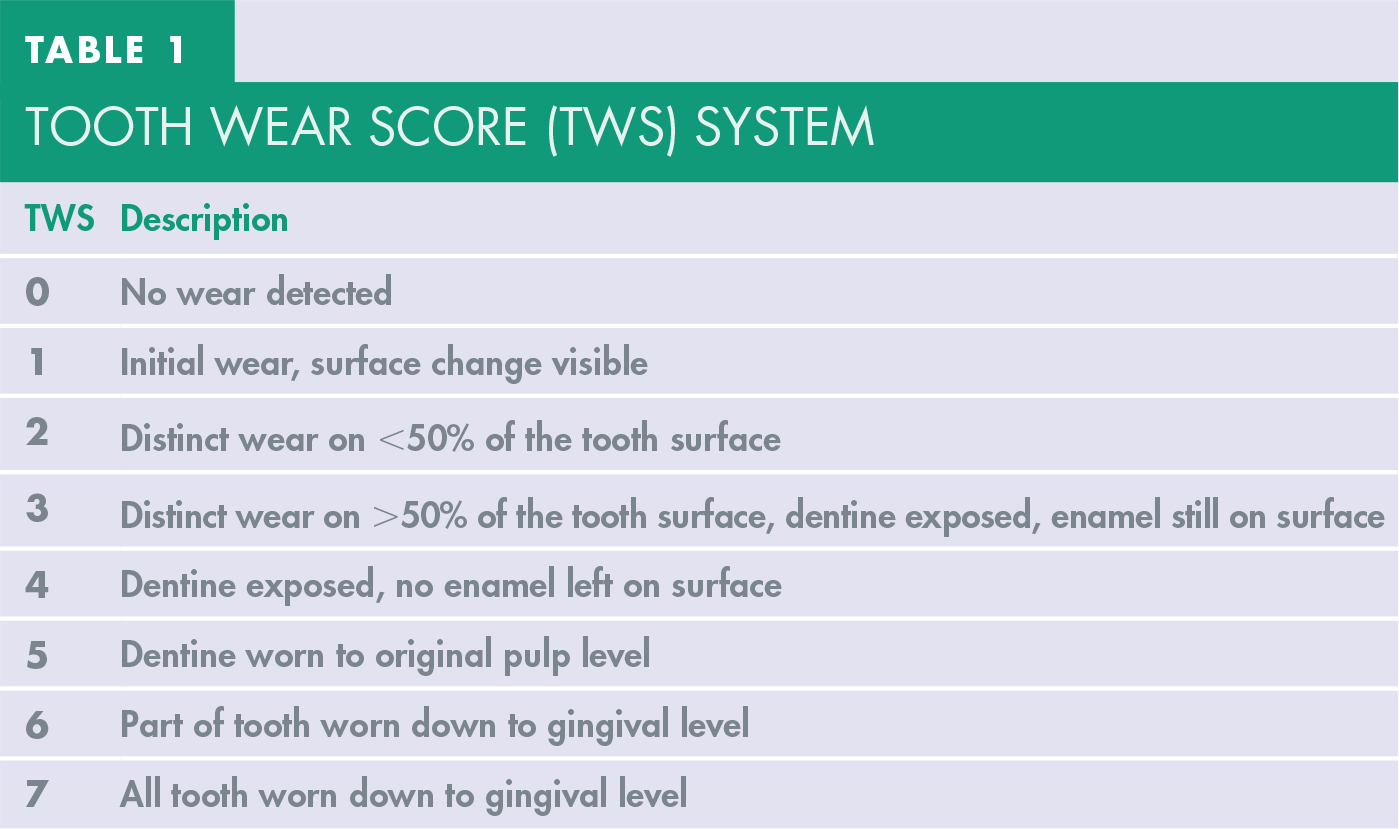
We termed this scoring system the tooth wear score (TWS). This was based on the basic erosive wear examination (BEWE) index. 14 It was formulated to estimate the severity of TW based on radiographs and photographs sent with referrals and was an extension of the BEWE index to accommodate for more severe forms of TW that might be referred.
The single most affected tooth seen on the radiographs and photographs was recorded (see Table 1).
Tooth Wear Score (TWS) system
Postcodes were classified as belonging to one of four location zones, with zone 1 representing postcodes closest to central London and therefore the tertiary hospital sites, and zone 4 those furthest. (See Table 2 and Figure 1).
Classification of postcodes
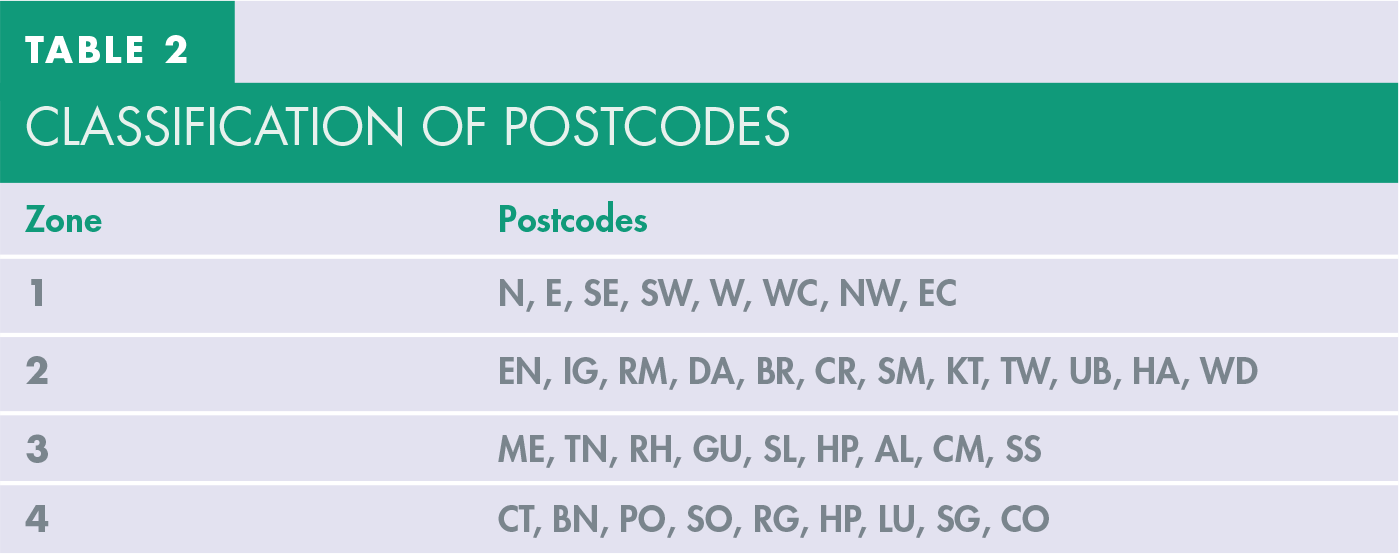
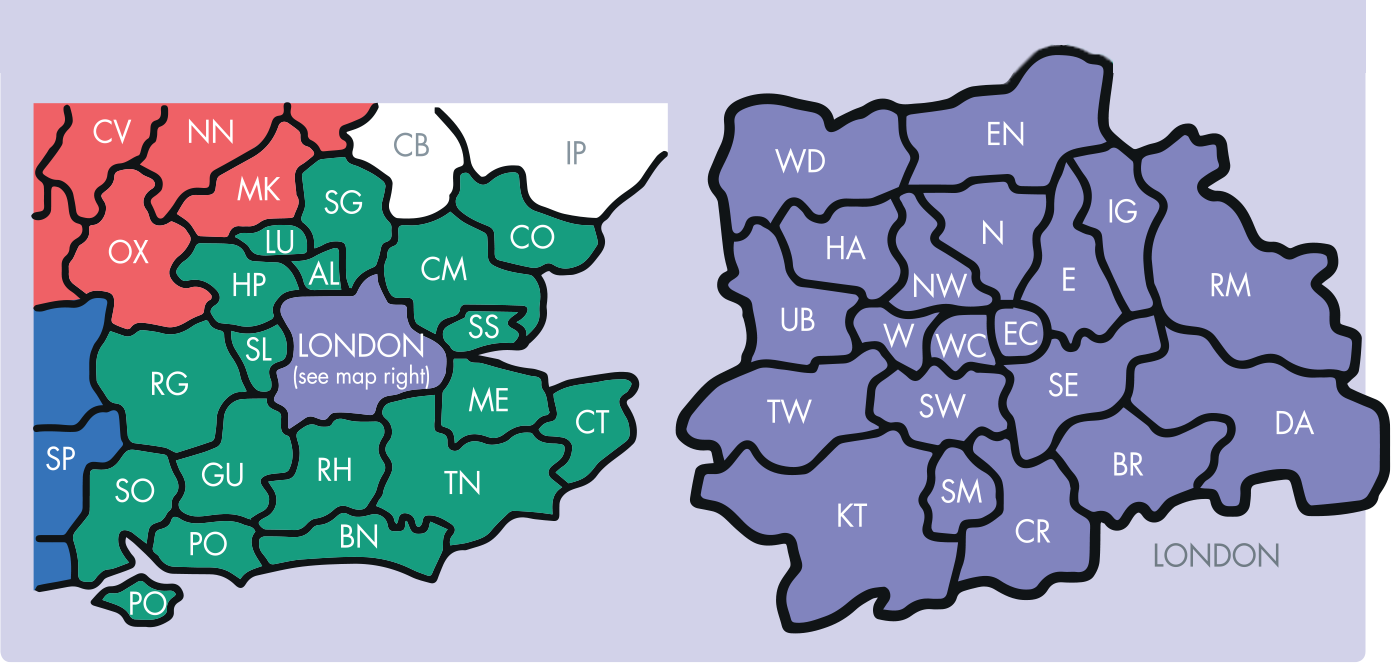
Location zones
Data analysis
Statistical analysis was undertaken using IBM SPSS Statistics software (version 25). A chi-squared (X 2 ) test was used to investigate whether categorical distributions differed significantly from one another, and an unpaired t-test was used for parametric continuous data. The level of statistical significance was set at α=0.05.
Results
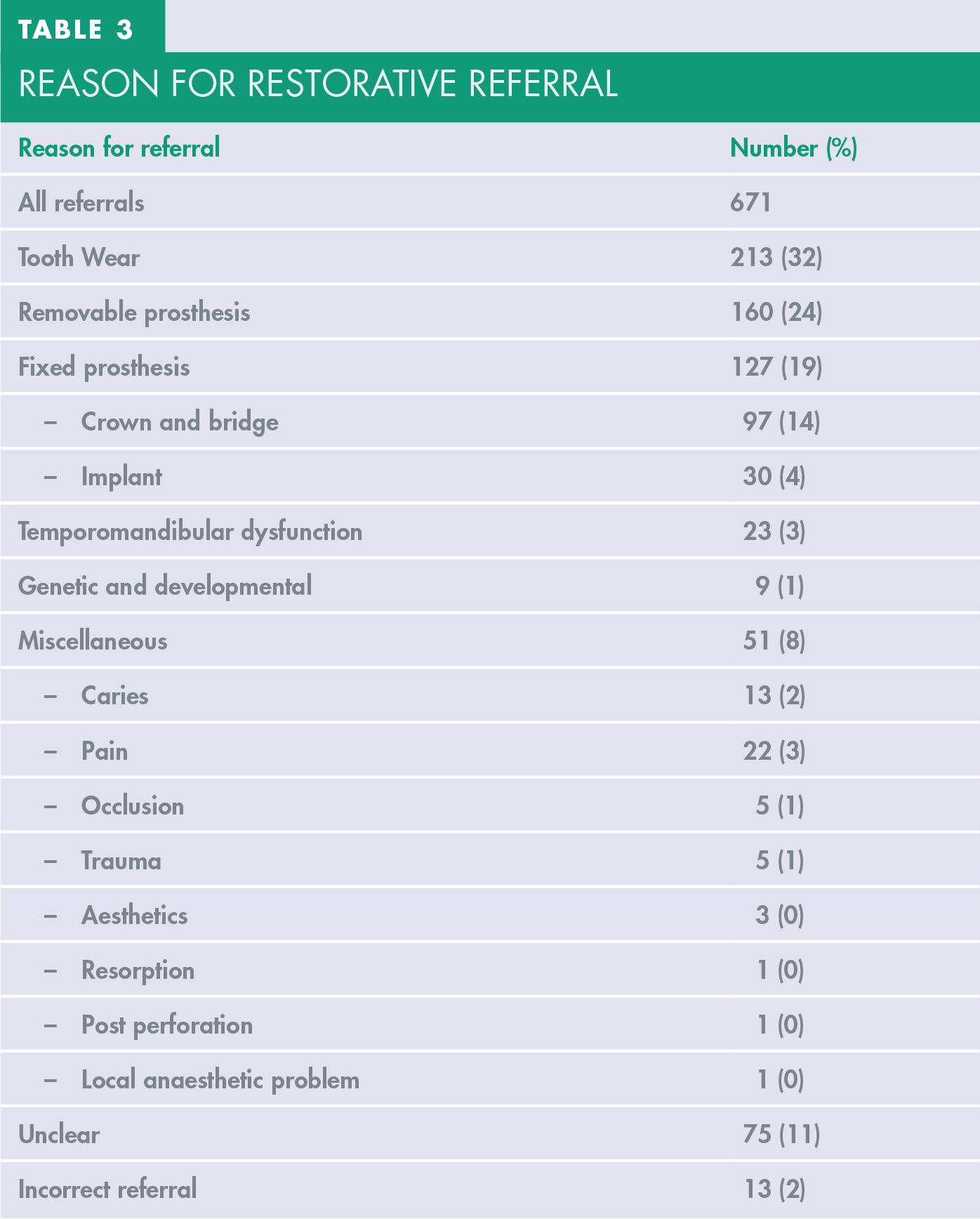
A total of 671 consecutive referrals were assessed over six months (1 June to 31 October 2019). All referral reasons are outlined in Table 3. The majority of referrals (32%, 213) were for TW.
Reason for restorative referral
Demographics
The age distribution of referrals is shown in Figure 2. Of 213 TW referrals, 63% (135) were males and 37% (78) females, with a male: female of 1.7:1.0.
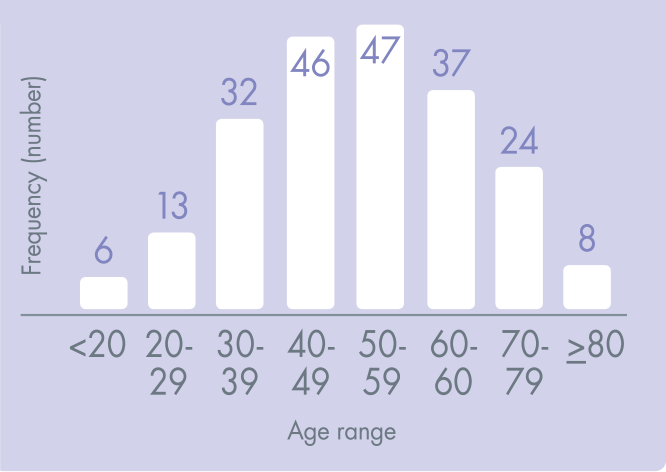
Age Distribution of TW Referrals
The median age of patients referred was 52 years (range 11-88 years).
The median age of males and females referred was 51 and 52, respectively. No referrals were seen from zone 1, 19% (41) were from zone 2. 46% (97) came from zone 3 and 35% (75) were referred from zone 4.
Patients were significantly more likely to be referred from zone 3 or 4 as opposed to zone 1 or 2 (p<0.001).
Quality of referrals
Figure 3 summarises the supporting information sent by referring GDPs. A clinical photograph was sent with 33% (71) of TW referrals and a radiograph with 78% (167). Of the 167 cases where radiographs were sent, 60% (100) included bitewings. 42% (70) included periapical radiographs and in 17% of the referrals (29) a panoramic radiograph was sent. In 15% (32) both radiographs and photographs were included. In only 1% (3) a basic tooth wear index score (BEWE) was included.
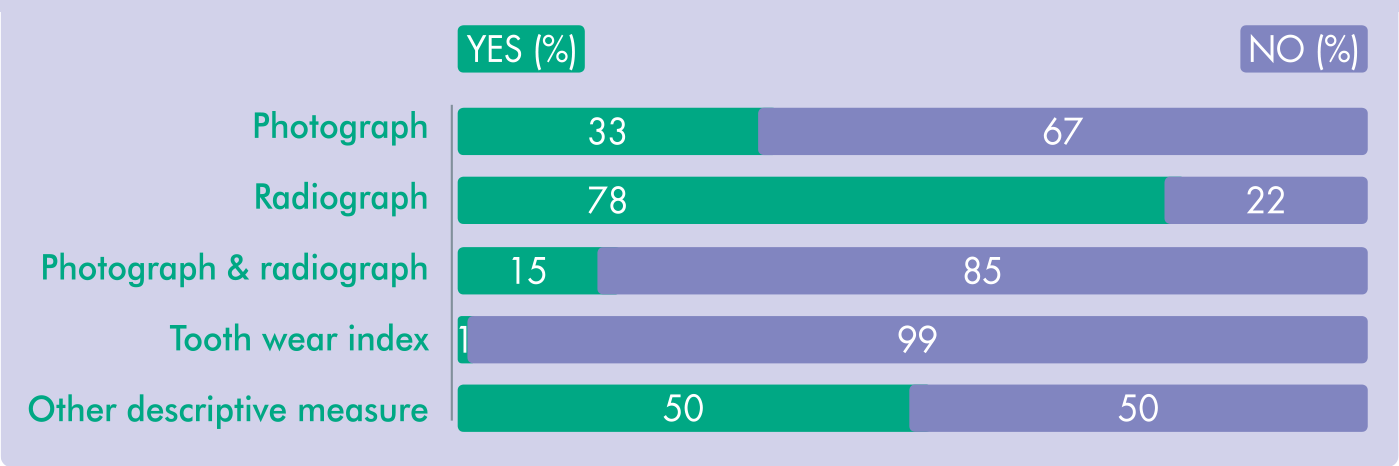
Information Sent With GDP Referrals
In three cases a percentage estimate for wear was given and in one case a measurement in millimetres. In 48% (103) the referring clinician gave a description of the severity of tooth wear. The terms used included mild, moderate, severe, into dentine, massively and significant.
Reason for TW referral
Figure 4 summarises the GPD opinion of cause of TW. 45% (90) of all referrals did not provide any cause for tooth wear.

Stated Reason For GDP TW Referral
The remaining causes included 24% (51) being due to attrition, 15% (31) being caused by erosion, 1% (2) abrasion and 16% (34) described some combination of these. When no cause given was excluded, GDPs were more likely to suggest attrition as the cause for referral (p<0.001).
Females were more likely to be referred for a combination of causes as compared to males (p=0.031).
48% (65) of the male referrals gave no reason for the referral. 25% (34) were stated to be due to attrition, 14% (19) due to erosion, one (1%) abfraction and 12% (16) described the problem being caused by a combination of causes.
In the case of female referrals, 38% (30) gave no reason, 22% (17) nominated attrition, 15% (12) were stated to be due to erosion, 1% (1) due to abfraction and 23% (18) due a combination.
Patients under 40 years were more likely to be referred for erosion (p<0.001) and less likely to be referred for attrition (p=0.019) as compared to those ⩾ 40 years.
For those under 40 years, the reasons given were erosion in 31% (16), attrition in 12% (6), a combination was suspected in 18% (9), 0 abfraction and in 39% (20) no reason was given.
For those ⩾ 40 years, 28% (45) were caused by attrition, 15% (25) were due to combination, 9% (15) due to erosion, 1% (2) abfraction and in 56% (45) of the referrals the reason was not given.
Tooth wear score (TWS)
Figure 5 shows the data for TWS allocated by the triage assessor. An unknown score was designated if limited referral information was given, thus not allowing for a score to be allocated.
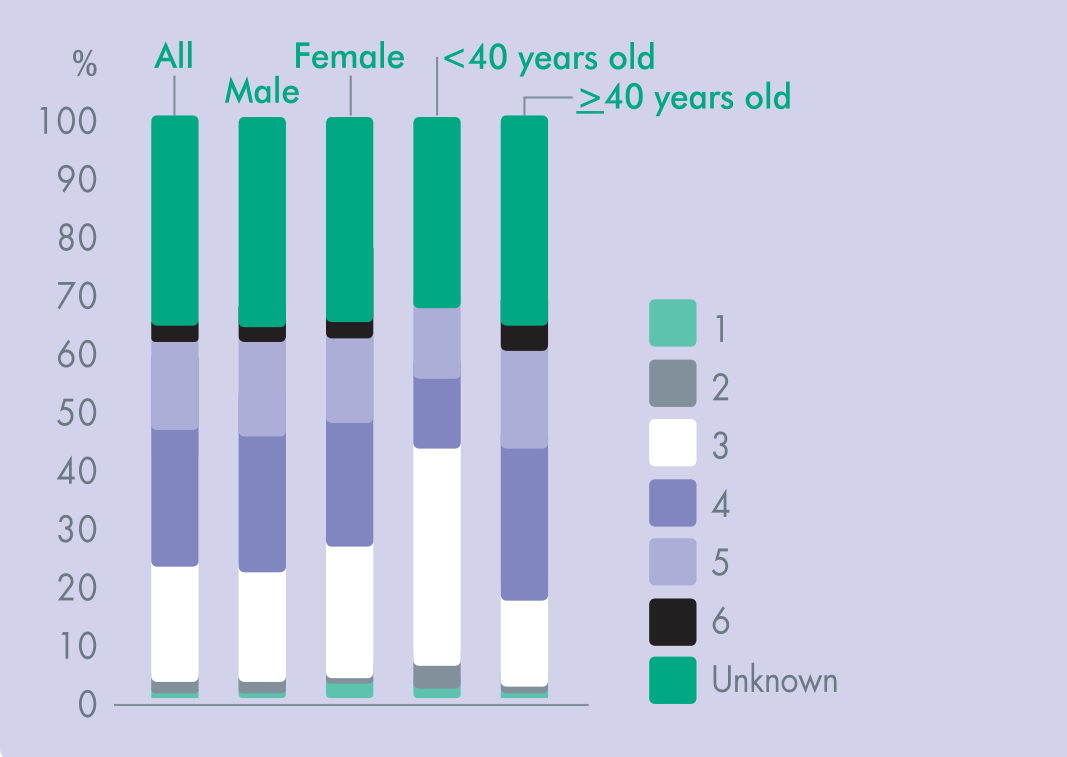
Triaging Consultant TWS Assessment
From all referrals, 36% (76) were scored as unknown. The most common TWSs were 4 (23%; 48), 3 (20%; 43) and 5 (5%; 33).
Only 1% (3) of referrals were given a 1 score, 2% (4) as 2 score and 3% (6) a 6 score. No referrals were scored 0 or 7.
When ‘unknown’ was removed from the data set, a score 3 or 4 was more likely than any other score (p<0.0001).
Of the male referrals, 36% (48) were unknown, 23% (31) scored 4, 19% (26) scored 3, 16% (22) scored 5, 3% (4) scored 6, 2% (3) scored 2 and 1% (1) scored 1.
Of the female referrals, 36% (28) were unknown, in 22% (17) a score of 3 or 4 was given, 14% (11) scored 5, 3% (2) scored 6 and 1, 1% (1) scored 2.
A difference in scores was noted between the <40 and ⩾40 years old cohorts. When unknown scores were excluded, those <40 were more likely to have a score of 3 compared to those ⩾40 and those ⩾40 were more likely to have a score of 4 compared to those <40 (p< 0.001).
The remaining score distributions were similar. For those <40 the most common score was 3 (37%; 19) followed by 4 and 5 (12%; 6), 2 (4%; 2), 1 (2%; 1) and score 6 (0). 33% (17) of referrals were classified as ‘unknown’.
For those ⩾40 the most common score was 4 (26%; 42) followed by 5 (17%; 27), 3 (15%; 24), 6 (4%; 6), 1 and 2 (1%; 2). 36% (59) of referrals were classified as ‘unknown’.
Outcome
A total of 47% (100) of TW referrals were rejected. Of these, 75% (75) were due to a lack of information sent by referring clinicians, 19% (19) were sent back with advice given, 3% (3) were rejected due to a lack of evidence of TW and 3% (3) due to incorrect details given.
Males referred were more likely to be accepted for treatment compared to females (p= 0.017). 59% (80) of male referrals were accepted, compared to 42% (33) of females.
A similar referral acceptance rate was seen between those <40 years (49%; 25) and those ⩾40 (54%; 88). 33% (71) of referrals included a photograph. Referrals sent with a photograph (77%; 55) were more likely to be accepted for treatment (p<0.001). This was also true for referrals sent with both radiographs and photographs (15%; 32) (p<0.001).
No referrals with a score of 1 were accepted, 100% (4) with a score of 2, 65% (28) with a 3 score, 69% (33) with a 4 score, 91% (30) with a 5 score and 83% (5) with a 6 score.
Discussion
Previous reports have investigated paper-based referral systems.8 -11 This study is the first of its kind to report on electronic TW referrals in the UK. As these systems become more ubiquitous, understanding how they are being used is critical for improving and planning future service.
Approximately half of all referrals were rejected (47%). These results are similar to previous data from non-electronic referral systems (47 8 -56% 9 ), indicating no change in rejection rate when using the electronic system.
A high proportion of referrals were of poor quality. Limited information and supporting details were common problems. Lack of information was the most cited reason for referral rejection, accounting for three-quarters of rejected referrals. Although radiographs were often sent (78%), these were generally considered to be poor discriminators for determining the extent of TW.
Referrals sent with photographs were more likely to be accepted (p<0.0001) but only one third of GDPs sent these.
The inclusion of photographs had a high positive predictive value (77%) and specificity (84%). Unlike radiography, the use of photography in general practice is not routine. TW referrals sent with photographs provide critical information such as the identification of wear facets and a more accurate assessment of the degree of wear. Multiple images can be taken without harmful exposure to the patient. Unlike a paper referral requiring a printed photograph, uploading a digital image with an electronic referral should also present less of a problem.
Most referring clinicians did not attempt to quantify the degree of wear. Less than 2% used a TW index to give a quantitative measure for the degree of wear and around half gave a vague description. In the remaining half, no attempt was made to report the degree of wear.
Qualitative descriptors pertaining to the degree of wear are subjective and therefore difficult for the triaging clinician to assess. An objective score is critical to overcome this. A number of measures have been suggested, with the BEWE score considered by its authors to be the most convenient in general practice. 14 These results highlight its poor utilisation. A lack of familiarisation of TW indices, and so GDPs not regularly utilising an index of any type as part of routine examination, may account for this.
To improve the quality of referrals, we advocate the use of mandatory fields for completion. This would include photographs, a tooth wear index and suspected aetiology of TW. Local audit data such as recurring reasons for rejection could also be disseminated via the electronic system.
In recent years, plans have been discussed for GDPs with enhanced training to undertake more complex treatment in a primary care setting. 15 If a role is developed for dentists with enhanced training, it would be prudent that expertise in TW is prioritised. Our data highlights a high demand for specialist TW services. Of 671 referrals, TW accounted for the majority, approximately a third of all referred (32%). This is a considerably higher proportion than previous reports, which range from 7-25%.16-19 Comparison with previous studies is, however, problematic as different categories for referral reason have been ascribed which are not always comparable. Service provision amongst referral centres also varies. An increasing prevalence of TW,2,5 a greater awareness amongst GDPs, the current UDA based remuneration system and increased patient demand might explain our findings.
Patients were more likely to be referred from distant locations according to postcodes as stratified in Table 2 (zones 3-4, 81% vs zones 1-2, 19%) (p<0.0001).
This finding is contrary to all previous reports, which used written referrals.16,20 Indeed, time and again, distance from referral centre has been cited by GDPs as a barrier for referral.17,21 The influence of an electronic pathway on restorative referral practices has not been studied in the literature.
It is possible that GDPs are more likely to refer from a greater distance with an understanding that these will be triaged centrally and sent to the most appropriate centre. Previously when written referrals were routinely used, GDPs might have been confined to only local referrals. Our data suggests a lack of local NHS dental services within further-out communities (zones 3-4). This may result in patients travelling a substantial distance for treatment, particularly when considering the rehabilitation of a worn dentition. Our data supports the concept of expansion of services locally.
This study also aimed to assess the referral characteristics of patients. A higher proportion of males were referred than females (1:7:1.0) with the largest proportion of referrals from 40-59 years (44%).
Previous reports as well as epidemiological data have similarly highlighted a higher prevalence and severity of TW amongst males.5,8,9-11,22 The gender distribution for TW referrals interestingly differs from general restorative referrals in which females predominate.16-19 Various explanations for the predominance of male referrals have been offered in the literature. Burnett et al. 9 postulated that females were more likely to seek treatment for TW earlier than males and therefore would be less likely to require referral. Additionally, males are able to generate greater masticatory forces as well as more likely to have risk factors relating to diet and stress. 10 Males may delay or avoid seeking treatment until the disease process was significantly advanced.
When referrals with no suggestion for cause were excluded, attrition was the most frequent reason (p<0.001). Previous studies also found this to be the case.8-11 Only 1% of referrals were for abrasion, in line with previous studies.9,10 GDPs appear to be comfortable in managing these patients without referral.
Females were more likely to be referred for a combination cause (p=0.031), whilst attrition was only just more common for males (25% of males compared to 22% of females). Previous literature has found males to be more affected by attrition, and females by erosion.9,10 The threshold at which a clinician diagnoses a combination cause rather than just erosion or attrition is subjective. It may be that referring GDPs felt that erosion in females was often accompanied with a degree of attrition. Indeed, Bartlett suggested that it is rare for erosion to occur in isolation. 23
Younger patients (<40 years) were more likely to be referred for erosion (p<0.001) and less likely to be referred for attrition (p=0.19) compared to the older cohort (⩾40 years). The challenge of erosive wear, in particular within younger patients, has been previously reported.5,22 Modern dietary habits and the increased mobility of younger generations to move for work and study have an impact on the prevalence of erosion and the delivery of care. 2 Our data highlights an at-risk group that will likely require an increased service provision in the future.
A customised scoring system was used in this study (TWS). This was not designed as an accurate diagnostic measure, but rather a representation of how a triaging clinician would assess referrals with the limited information given. This differs from previous reports in which patients have been examined clinically.
In 36% of referrals it was not possible to allocate a TWS due to a lack of radiographs or photographs. Of those that were classifiable, a score of 3 or 4 was most likely (p<0.0001). There is no agreed strictly defined point at which TW requires operative intervention or specialist referral. Factors influencing referral include severity, patient symptoms, aesthetic or functional concerns as well as the expertise of the referring clinician. It appears clinically appropriate that the majority of referrals were for TWS of 3 and 4.
A total of 18% of referrals were seen with a TWS ⩾5. This signifies severe wear to the level of the original pulp and beyond. Of these, 51% were < 60 years old. This highlights a severely affected cohort of potentially late referrals. Explanations for this may include that these patients were late in seeking dental attention or that the current NHS remuneration system does not make it attractive for GDPs to treat these patients earlier.
Males and females had similar TWS. This differs from data in the literature where males are more severely affected than females.5,10,22 Interestingly, males were more likely to be referred in the current study as well as accepted for hospital treatment (p= 0.017). This was despite similar severity (TWS) and age distributions. Males seem to have been identified as a higher risk cohort both by the referring and triaging clinician.
Younger patients were more likely to be referred with a lower TWS (3) compared to the older cohort, who were more likely to be referred with a higher TWS of 4 (<40 years compared to ⩾40 years, p<0.001). This is consistent with the literature which has shown severity to increase with age.4,5,22 A possible explanation might be that referring GDPs appropriately required a lower threshold for referring younger patients. Alternatively, a genuine difference in the aetiology of tooth surface loss between the cohorts may exist.
Close to half (52%) of accepted referrals were aged from 40 to 59. This represents the patient cohort that the current system is predominately targeting. In this limited study, a difference in referral outcome was not noted between the younger and older cohorts. This seems appropriate as the pathway identified younger patients at a lower TWS compared to those that are older.
Limitations of the study
This study is the first of its kind to report on electronic TW referrals in the UK. There is a high demand for specialist TW services within the region that was studied. In order to evaluate the applicability of our findings this should be reproduced in other regions of the UK. A degree of pragmatic interpretation was required in the assessment of referrals when allocating a TWS based on radiographs and photographs.
In 36% of cases, a TWS was not determinable due to limited information provided. We employed a single assessor to ensure consistency, although a risk of intra-researcher bias or inconsistency was present and no attempt was made to eliminate this possibility.
Conclusions
Consistent with previous studies, a high proportion of GDP referrals were of poor quality. This had not been addressed by the electronic system. We recommend the use of mandatory fields for completion, the inclusion of photographs and a tooth wear index – either a Smith and Knight Tooth Wear Index or a BEWE index with all referrals.
The dissemination of local outcome data, such as reasons for rejection, can be sent via the electronic system and may serve to increase practitioner awareness and improve the quality of referrals.
The current referral service is most commonly identifying males and those between the ages of 40-59. Two distinct groups are referred; a younger cohort typically referred for erosive tooth surface loss with a TWS of 3 and an older cohort referred for attrition, with a TWS of 4. These findings are consistent with at risks groups identified in the national epidemiological data.