
Abstract
Across the globe the population is ageing. In addition, older patients are retaining increasing numbers of natural teeth into old age. Therefore, clinicians are faced with the challenges of managing chronic dental diseases, including caries and periodontal disease, alongside replacing missing units. A number of treatment options are available to replace missing teeth for such patients with large numbers currently receiving removable partial dentures. Alternative approaches to treatment should be considered for this population group, including functionally orientated tooth replacement according to the principles of the shortened dental arch concept. In correctly chosen cases, this approach can provide patients with an acceptable, functional and aesthetic reduced dentition. Additionally, evidence suggests that such an approach can significantly reduce the maintenance burden for patients and clinicians which can ultimately deliver a more cost effective solution compared to removable alternatives.
Keywords
Learning Objectives
Appreciate that functionally orientated treatment planning is applicable for partially dentate older adults
Understand that functionally orientated tooth replacement has a number of advantages over more conventional forms of treatment, including removable partial dentures
Appreciate the need for careful case selection when considering functionally orientated tooth replacement in older adults
Introduction
Despite significant changes in the oral health of older patients, many still require prosthodontic intervention to replace missing teeth. If prosthodontic replacement of teeth is required, the majority of patients currently receive removable partial dentures (RPD) to meet functional and aesthetic demands. However, there is always a biological price associated with RPD provision, with longitudinal studies indicating an increased incidence of caries and periodontal breakdown when removable partial dentures are worn.1,2 This is particularly important for older adults as evidence suggests that this group is particularly at risk of developing root caries in the presence of a RPD. 3 Given patients’ dislike of removable dentures, their biological cost and high levels of non-compliance, other treatment options should be considered when planning tooth replacement for older, partially dentate patients, including functionally orientated tooth replacement.
Principles of the shortened dental arch
Some researchers have suggested that older adults have different functional needs to younger patients and therefore do not need a complete natural dentition. 4 The shortened dental arch (SDA) concept has been successfully implemented in older patients by preserving anterior teeth in preference to molars which are more difficult to maintain. Furthermore, the World Health Organisation (WHO) suggested that a goal for oral health in the year 2000 should be that adults retain for life a healthy, functioning dentition of at least twenty teeth and do not require the use of a removable prosthesis to replace missing teeth. 5 Käyser first described the SDA as ‘a dentition where the most posterior teeth are missing’. 4 The molar regions play important roles in mastication and stabilisation, however, they are high-risk teeth for caries and periodontal disease, and possibilities for restorative treatment are often limited. In practical terms, however, it is impossible to maintain a natural shortened dental arch for all patients as some will have suffered trauma or extensive disease to their anterior teeth, resulting in tooth loss and the need for prosthetic replacement. Others may be congenitally missing teeth and some teeth, particularly upper canines, do not erupt; potentially resulting in spacing.
Käyser found sufficient oral function in SDA when at least four occlusal units remain, preferably in a symmetrical position. 4 Sarita and co-workers found that chewing ability decreased as occluding pairs of teeth decreased. 6 They found that a SDA with intact premolar regions and at least one occluding pair of molars provided sufficient chewing ability, and that a SDA comprising 20 teeth (intact anterior region and four pairs of occluding posterior teeth) can provide satisfactory chewing ability for most foods. 6
In a review of studies of the SDA concept, Kanno and Carlsson found that, although it was accepted by the majority of dentists, the concept was not widely practiced. 7 It remains controversial for some dentists, and examples of criticism are that loss of molars is associated with reduced masticatory performance, and that a SDA could cause functional overloading of the teeth and temporomandibular joints. However, Hattori et al., found no evidence of this, and the literature indicates that the SDA can provide oral functionality and comfort. 8 Routinely extending shortened dental arches with prosthetic devices, with the sole aim of preventing temporomandibular joint dysfunction (TMD) should be discouraged due to the possibility of further iatrogenic damage to existing teeth. Further evidence from studies in the Netherlands and Tanzania proved that use of the SDA did not have any measurable negative impact on temporomandibular joint health.9,10 According to Käyser and Witter, when missing teeth do not cause chewing or aesthetic problems, their replacement may constitute overtreatment. 11 The SDA may avoid the risk of overtreatment while still providing a high standard of care and minimising cost.
Planning for a shortened dental arch
The prognosis of all remaining teeth should be considered before prescribing a SDA (Figure 1). If the restorative status of these teeth is such that the increased occlusal forces associated with a SDA may hasten their failure (such as in the patient with periodontitis), this is not an appropriate treatment plan. Excessive occlusal pressure can generate inflammatory changes and resorption of alveolar bone in localised pressure-tension zones and in a periodontal disease-active patient, plaque associated areas of breakdown may coalesce with these localised zones and bone loss can be accelerated. Such alveolar breakdown may occur in periodontally unstable individuals and the result loss of support may be permanent.12,13 As such, if patients have reduced alveolar bone loss from periodontal disease and are not stabilised, posterior support should be considered if this can be provided according to hygienic principles.
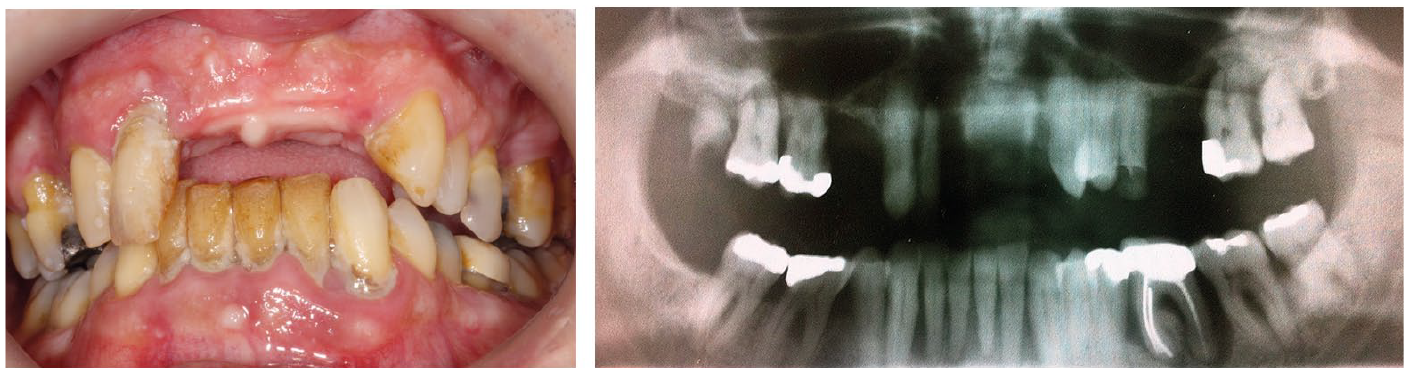
A partially dentate patient with teeth of very poor prognosis: unsuitable for a SDA approach
The prognosis of individual teeth as well as the mouth as a whole should be taken into account. Any teeth that are or will become guiding teeth in a SDA model should be assessed for their durability to perform this role. The presence of extensive restorations should alert the clinician to the possibility of failure under both static and dynamic loading. Guidance should be planned upon sound teeth with good periodontal support, and if this is not possible, serious consideration should be given to restoration of posterior units, both as an intermediate measure and long term.
As previously discussed, the SDA concept has not been shown to be linked to an increased incidence of TMD.9,10 The Käyser study did, however, find that patients without posterior teeth tend to chew more on their anterior teeth. 4 Although this is normal function, not parafunction, it is likely to accelerate the wear on the remaining teeth. This is obviously of importance in a patient who already exhibits signs of tooth wear at presentation.
However, in patients who are known to have parafunctional habits, excessive loading of teeth will compromise their future prognosis. When posterior support is reduced or absent, this process may be faster and more destructive, although the evidence for this is scarce. If this appears to be the situation, then provision of posterior support should be considered. Restorative treatment does not halt bruxism, thus the remaining dentition may well benefit from protection with splint therapy. 14
Distal migration of premolar units has been demonstrated in patients with a SDA to varying extents. 15 The resulting spacing may compromise aesthetics and permit food trapping that may in return result in an increased risk for localised periodontal disease. The loss of an occlusal stop may occur as a result of extracting a posterior tooth. This has been linked with tooth movement and over eruption in as many as 83.9% of cases. 16 If teeth are going to over erupt, it has been shown to occur within 12 months in most cases, and of those teeth that move, 24% move over 2mm. 17 Furthermore, the movement of teeth may have horizontal and rotational components as well. Such movement may be of no consequence but it could generate an occlusal interference or a retruded contact prematurity. More significantly, such over eruption can be so severe as to prevent restoration of the opposing space. Prevention of over eruption per se does not provide a mandate for restoration of edentulous spaces but it must be factored into the decision making and consent process.
Restoration to a shortened dental arch: replacement of missing teeth
In practical terms, it is impossible to maintain a completely natural shortened dental arch for all older patients as a lifetime of chronic dental diseases can result in toothloss and the need for prosthetic replacement. Patients can be restored to a SDA using a variety of options, including conventional prosthodontics, implant retained restorations and adhesive options.
Conventional and implant-retained prosthodontics
Conventional prosthodontics can deliver excellent longevity but at a high biological cost (Figure 2). Care must be taken to ensure a minimally invasive approach without compromising pulpal vitality. Similarly, dental implants (Figure 3) can be utilised but this treatment modality would necessitate an invasive surgical procedure, which many older patients view negatively. 18 Treatment may be complicated in the mandible by the presence of the inferior dental canal, and in the maxilla by the maxillary sinuses. This may complicate potential placement, and may necessitate more complex surgery and/or grafting. Furthermore, compared to the alternative implant treatment, it is costly and more time consuming.
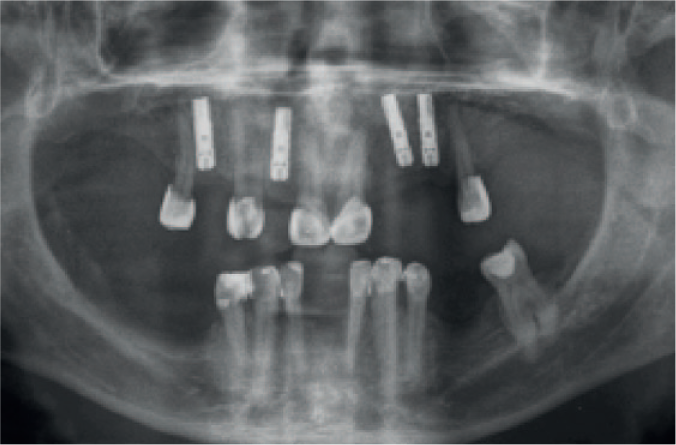
Patient restored to a SDA using conventional prosthodontics

Patient restored to a SDA using implant retained restorations
Adhesive bridgework
Resin bonded bridgework (RBB) can offer a simple yet effective option when considering the replacement of missing teeth. Evidence shows that it can provide a successful, predictable outcome with high levels of patient satisfaction.19,20 However, many practitioners appear to be reluctant to utilise RBB, instead often choosing conventional designs which are more destructive of sound tooth tissue. Since RBB evolved from the rochette bridge described in 1973, there have been significant changes in bridge design, materials used and in abutment tooth preparation. Current bridge designs use sandblasted, non precious metal cemented with chemically active resin. As with conventional bridgework, a cantilever design is favoured to reduce the amount of tooth preparation and to produce a more retrievable restoration. Evidence illustrates that RBB placed using current techniques can achieve high success rates with survival of up to 87.7% reported after 5 years. 21
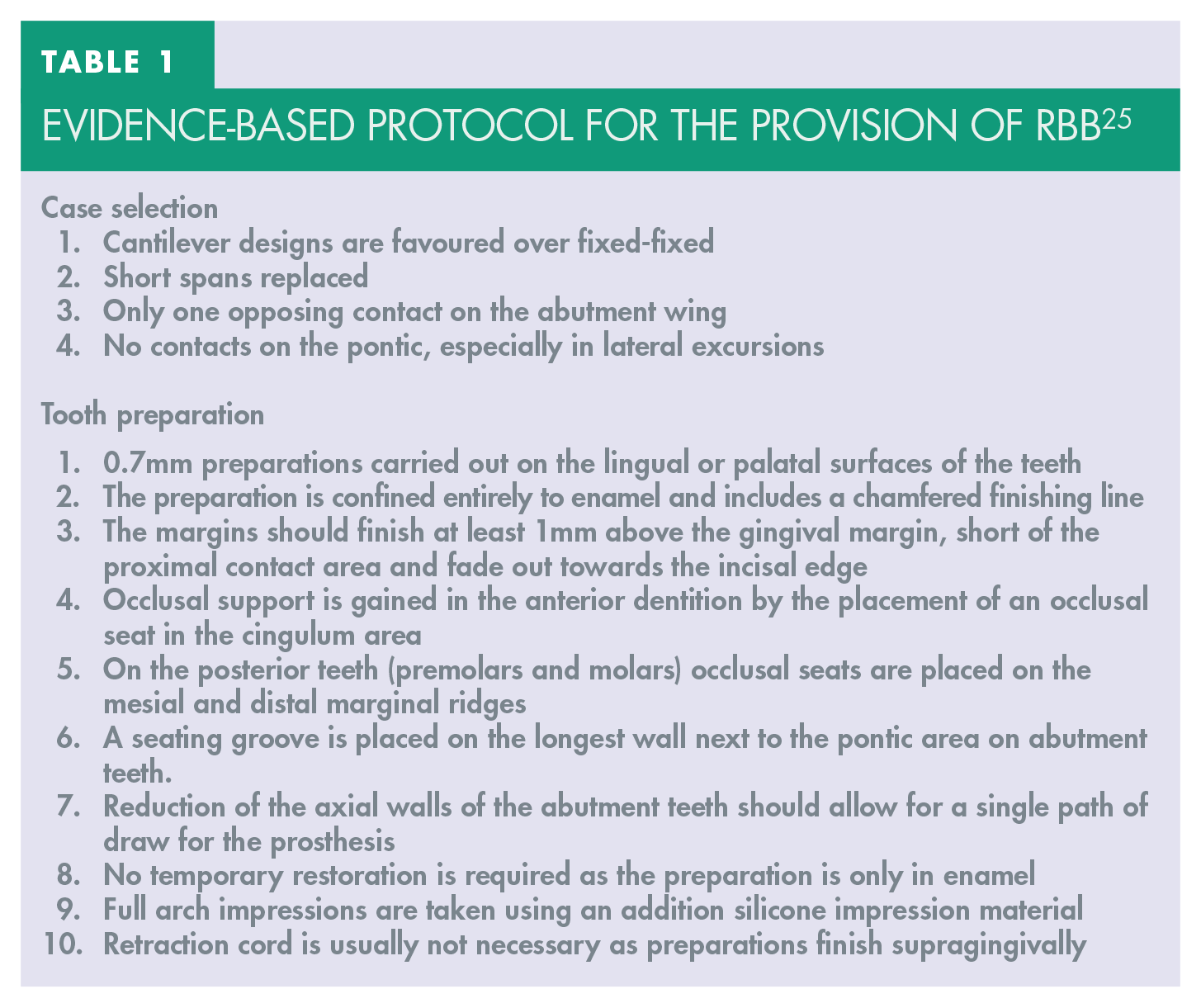
Whilst some authors argue that preparation of the abutment teeth is unnecessary, evidence shows that tooth preparation increases retention and resistance. 22 Preparations are used to produce retentive forms and to simply increase the surface area for bonding. Fundamentally, all preparations must remain within enamel to take advantage of significantly better bonding conditions. Preparing the palatal/lingual surfaces of the abutment teeth allows an adequate framework thickness to be incorporated into the RBB. The framework should be as rigid as possible, thus preventing flexure. It has been shown that an increase in thickness has a corresponding increase in resistance to dislodgement. 23 A thickness of a least 0.7mm metal work is now recommended by many authors. 24 An evidence based protocol for the use of RBB is shown in Table 1. 25
Evidence-based protocol for the provision of RBB 25
The use of resin bonded bridgework to restore patients to a shortened dental arch has been shown to significantly improve patient satisfaction (Figure 4). In a randomised controlled clinical trial, patients were restored to a SDA using resin bonded bridges. After treatment, patients reported significant improvements to oral health related quality of life compared to those provided with removable dentures.26,27 Other studies have demonstrated those patients restored to an SDA using resin bonded bridgework required much fewer maintenance appointments than patients treated with removable partial dentures. 28 The removable denture group also demonstrated a statistically significantly greater incidence of new and recurrent carious lesions two years after rehabilitation. 29 These results were mirrored in a similar longitudinal study which compared removable partial dentures with cantilever adhesive bridgework in an elderly population. Despite a careful professional maintenance programme, dental caries incidence was six times greater in the removable denture group. These patients also required more frequent follow up visits. 30

Patient restored to a SDA using RBB in upper and lower arch
Glass fibre-reinforced composite bridgework can also be used to restore patients to a shortened dental arch. Fibre-reinforced composite resin bonded bridges can be made both directly in the mouth by the clinician or indirectly in a dental laboratory. Moreover, both techniques may be combined by which optimal adaptation to the existing situation can be achieved. Fibre-reinforced composite resin bonded bridges in general have a somewhat less favourable prognosis than metal framework resin bonded bridges. However, for use in the management of partially reduced dentitions in elderly, this is compensated by the relative ease in which they can be repaired and extended if necessary. 31 (31).
Conclusion
A number of treatment options exist for partially dentate older patients. Whilst the majority of cases currently receive RPDs, alternative treatment options should be considered, including functionally orientated tooth replacement according to the principles of the SDA. A considerable amount of high quality evidence from clinical trials has demonstrated that this approach can provide a functional, aesthetic dentition which older patients can maintain more easily than removable alternatives.