
Abstract
Dementia has been described as the biggest health and social care challenge of this century; its impact on dental care cannot be ignored. Dementia affects cognitive ability and decision making, so it is important that oral healthcare professionals are conversant with current mental capacity legislation and issues that may be raised when treatment planning for patients living with the condition. This second article in the series considers the impact of dementia on dental care provision and covers a range of issues which are relevant to both general and specialist practice. These include assessment of capacity, use of different treatment modalities, such as sedation and general anaesthesia, and the factors that may be relevant when deciding to offer treatment or to refer to a secondary care setting for dental treatment. Advanced care planning is detailed to support general dental practitioners considering the longer-term wishes of their patients with an early diagnosis of dementia.
Keywords
Learning Objectives
To gain an understanding of legislation related to Mental Capacity Assessment and the impact of this on clinical decision making
To consider the impact of dementia, at various stages, on the process or appropriateness of providing dental treatment
To review the implications of conscious sedation and general anaesthesia in the care of people living with dementia
Introduction
The symptoms of dementia may fluctuate in intensity and presentation on a day to day basis, yet a general progressive decline is expected, varying depending on the type of dementia involved. 1 People with Alzheimer’s disease live, on average, eight to ten years after symptoms begin, whilst those with vascular dementia typically live around five years after the onset of symptoms, 2 generally due to the underlying and persistent risk factors that led to a primary stroke. These factors and the variability they produce will impact on treatment planning and the consent process. This article discusses treatment options for providing dental care for patients with dementia and how to take into account their personal wishes when planning treatment either with them or in their best interests if they are assessed to lack capacity to consent. The aim of this second article is to help oral healthcare professionals to care for individuals living with dementia by offering treatment that is appropriate to their needs and the stage of their disease.
Mental capacity
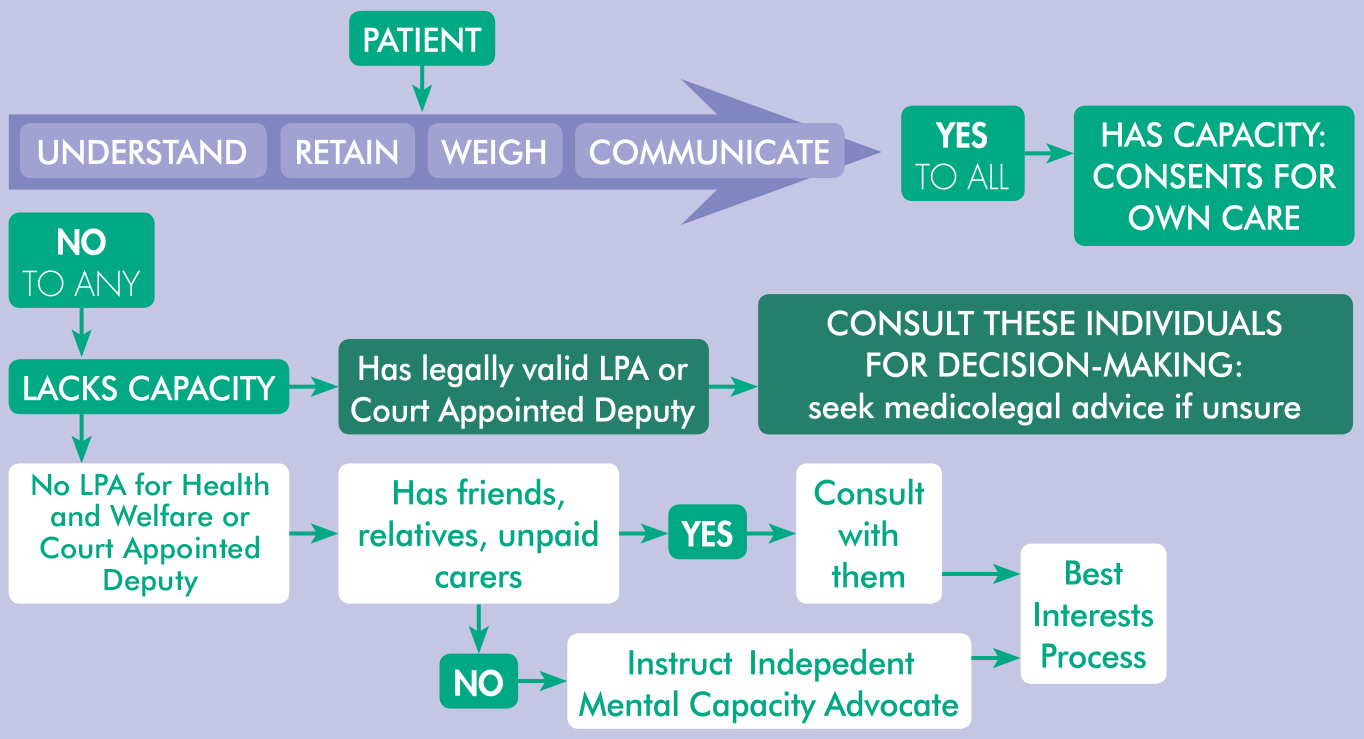
Mental capacity legislation differs depending on which region of the UK is involved. There are key similarities and common principles between the differing legislations, but also subtle differences that can impact who ultimately decides on or consents for any treatment proposed. A comprehensive review, specific to dental care, is available elsewhere3,4 and details the specific impacts of legislation in each of the devolved nations of the UK. A requirement of the Mental Capacity Act, 5 (England and Wales), is the need to assess capacity. If it is identified that the person has a known disturbance in functioning of the ‘mind or brain’, a capacity assessment is undertaken (as shown in Figure 1) and a person is assessed to lack capacity if they are unable to undertake one or more of the following four components:
Understand the information, including the risks and benefits
Retain the information for long enough to make a decision
Weigh up the factors relating to the decision
Communicate the decision by verbal or non-verbal means
A person with dementia may struggle to make sense of information about proposed treatments due to difficulty with cognition or an inability to focus or concentrate. They may have communication issues that make it difficult to understand words or to be able to express themselves verbally. Their lack of memory may make it hard to put the proposed procedure into context or understand what is happening. Alongside this, an increased anxiety may produce a powerful emotional response.
Assessing Mental Capacity in Dementia
For people with dementia it is important to remember:
It is the decision in question to which the issue of capacity relates; this is time and situation specific
Some decisions may be straightforward (such as consenting for a radiograph), others more complex (such as surgical extractions) and a person may be able to consent for one and not the other
A patient’s capacity may fluctuate both as time progresses and within any given day
A patient may lack capacity at one stage, but regain it later stage, or vice versa
If a patient is assessed to have capacity to consent for treatment, the usual processes of informed consent should be followed. Reassessment may be required at subsequent dental visits. When patients are formally assessed to be lacking capacity, dental teams should consider patients’ previous wishes as well as relevant cultural and social factors.5,6 The key principle of all legislation in the UK is that actions made must be in the ‘best interests’ of the patient. The challenge here is that in the absence of evidence on implications of dental intervention or leaving disease untreated, best interests can be difficult to ascertain. For example, a retained root left in situ may cause pain in coming years, meaning one could argue it is ‘best’ for the patient to remove it. We do not know, for each patient, however, whether a retained root, for example, would cause pain and if this pain would be more significantly impactful than the process of its removal. Consulting a colleague for a second opinion may be useful to enable debate and deliberation on this and similar treatment planning dilemmas. Patients’ perspectives and preferences are harder to determine as dementia progresses and it is therefore useful to involve those who know the patient in order to clarify what would be important to that individual. The Code of Practice that accompanies the Mental Capacity Act is a valuable read for any healthcare professional who may encounter people with issues relating to capacity. 7
The input of those with an interest in a patient’s wellbeing is invaluable in the determination of best interests. Those who can contribute include family members, unpaid carers and friends. There is a potential for conflicts of interests if paid care staff are consulted; their views can illuminate factors relevant to the decision making process but if no family, friends or unpaid carers exist or cannot be reached then the support of an Independent Mental Capacity Advocate (IMCA) must be sought. The terms ‘Next of Kin’ and ‘Lasting Power of Attorney’ or their variations are used informally, but their legal status must be considered.
Though a ‘next of kin’ may be the most appropriate person to consult, the patient’s nearest relative my also know little about the person and be poorly placed to advocate, (e.g. a distant relative who lives overseas and does not visit). Lasting Power of Attorney (LPA) is a legally binding process under the Mental Capacity Act, and must be formally registered through a solicitor with the Office of the Public Guardian. There are two types of LPA, ‘Property and Finance’ or ‘Health and Welfare’; somebody formally assigned to the former role may not be assigned to the latter and it cannot be assumed that somebody stating they have LPA actually does have the correct LPA to make a decision regarding healthcare interventions. The Office of the Public Guardian allows their records of LPA to be searched by healthcare professionals; this can be valuable to ensure that a decision is made either by a valid LPA, who is then the decision-maker, or through a best interests route in which the clinician is the ultimate decision maker. Figure 1 clarifies some of these processes.
Advanced care planning
Oral healthcare professionals are uniquely placed to establish long-term relationships with their patients. A clinician may see patients both as they age and as they progress through acute or chronic illnesses. The signs and symptoms of some types of dementia can be subtle in the early stages, meaning regular dental attenders may still attend for examinations and treatment either before or after a diagnosis of dementia. All types of dementia have variable and potentially unpredictable trajectories 8 and so seeing a regular attender early after a diagnosis of dementia creates an excellent opportunity to have a valuable yet challenging discussion about dental care for the future.
Those with a formal diagnosis should be aware of the progressive and degenerative nature of their condition and may have begun considering the impact of this on their general health, finances and relationships. Advanced care planning is a process of recording patient’s wishes to preserve their autonomy for when they may lose capacity to consent for their own decisions.9,10 Though health decisions may be discussed with somebody formally acting as a Lasting Power of Attorney (LPA) for Health and Welfare, dental care needs and wishes are less likely to have been specifically discussed. The benefit of formally recording patients’ preferences for future care may increase substantially as the prevalence of dementia increases and as people retain increasingly restored and complex dentitions.
Whilst dental conditions are unlikely to be life-limiting, orofacial pain and infections, sudden loss of oral function, and altered appearance can certainly be life altering.11-13 This is particularly likely when patients’ risk factors, or cooperation with treatment, may mean that fixed or even removable prosthetic rehabilitation may not be possible. This can occur when extensive dental diseases in uncooperative patients mean that more radical treatment under general anaesthetic or sedation is required. With best interest discussions, prior knowledge of patients’ preferences and priorities can ensure a decision made for their care aligns with their values and wishes as specified in legislation.5,7 Only by formally planning for the future can patients’ wishes be established.
Questions that might be valuable as part of an advanced care plan may include:
What matters most to them for their dental care?
If they had pain, would they prefer an extraction or to retain a tooth?
Is freedom from pain a higher priority than tooth retention?
Would they prefer to sit through or avoid more complex procedures?
Would they rather be made less likely to have pain, even if it was at the expense of function or appearance?
A definitive decision cannot realistically be specified in the absence of all appropriate information, and though highly valuable, a patient’s past views are only one aspect of this. Despite the benefit of eliciting patient’s preferences for their future, it is worth considering that patients may wish for those involved in their care to make this decision for them based on the future facts and circumstances. It is also worth noting that a diagnosis or the presence of dementia may mean that a person’s wishes changes from those they previously expressed. 14
Advanced care plans are not legally binding. If patients express particularly strong preferences, especially if these do not align with professional recommendations or what is perceived to be in their best interests, patients can use legal routes to specify their wishes. Under the Mental Capacity Act, a patient cannot legally demand treatment be delivered, yet they can specify an advanced decision (to refuse treatment). 5 Additionally, as discussed, a patient may have a formal Lasting Power of Attorney (LPA) for Health and Welfare and have informed this individual of preferences, some of which may be relevant to dentistry. When an LPA was not produced, a court appointed deputy may exist who, like an LPA for health and wellbeing, can inform treatment decisions. 5 Those acting in either of these roles will likely have knowledge far beyond the dental team of a person’s preferences; if a person is unwilling to discuss their future wishes with dental professionals, it could be wise to encourage them to have this discussion with those in such roles or who may contribute to future care decisions.
How do we plan treatment?
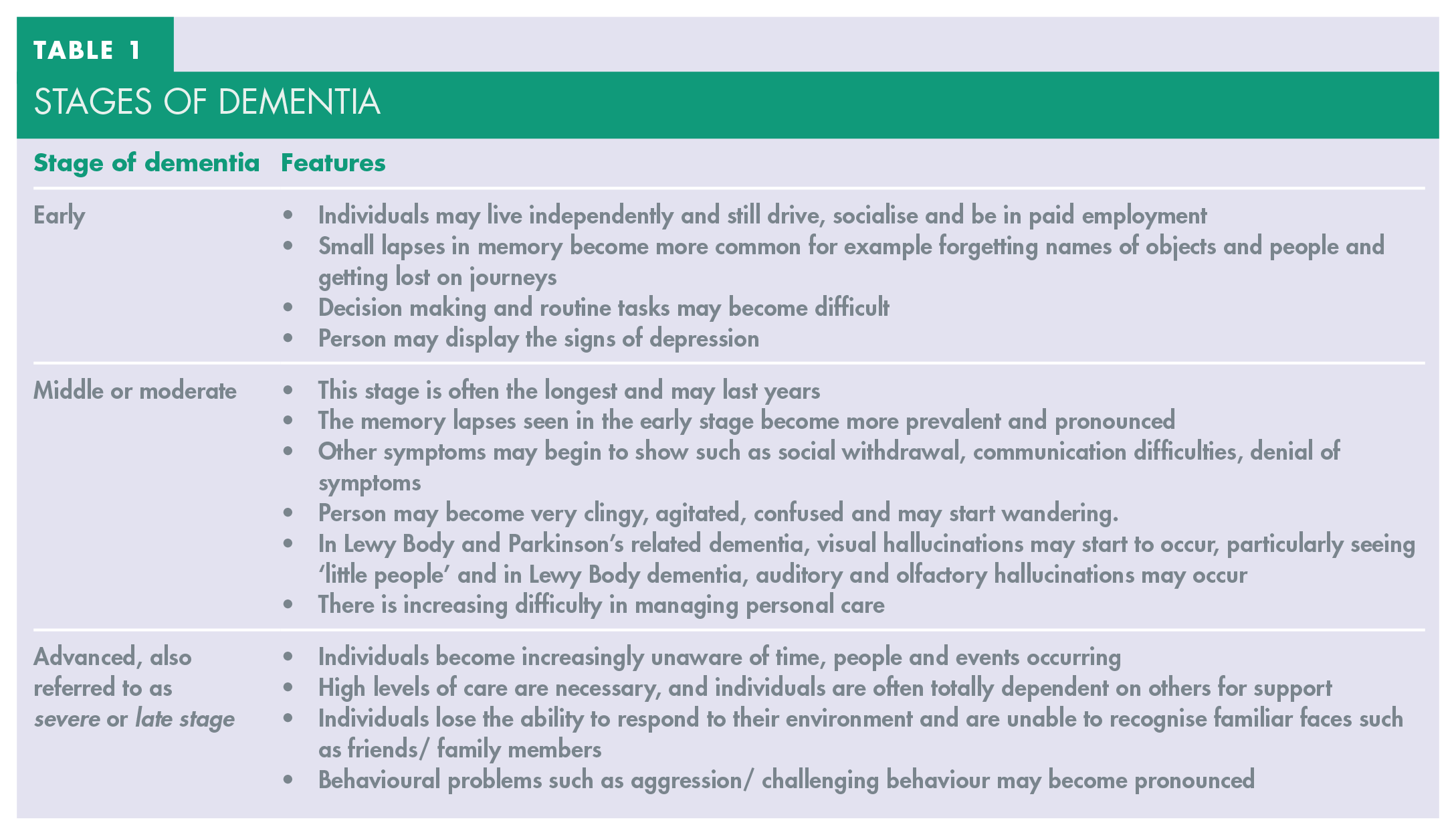
An essential step in all treatment planning is to establish the aim of the overall treatment process. This will vary depending on whether care is elective or urgent, the patient’s wishes and what can be realistically achieved based on the combination of patient, medical, social and dental factors. Crucially, the stage of dementia must be considered as this relates to patients’ symptoms, capacity, ability to cope with procedures, the safety of treatment delivery, the ability to provide oral self-care and the overall prognosis. When planning treatment, it can be helpful to classify a patient into a stage of dementia as described by the World Alzheimer Report. 15 Table 1 summarises this in three stages; early, middle and advanced.
Stages of dementia
Treatment in early dementia
Due to the degenerative nature of dementia, for those with early dementia there can be a benefit in anticipating a decline in oral and general health and proactively managing oral diseases at an earlier stage. This would aim to prevent pain, infection and the need to provide complex treatment in later stages of dementia when risk may increase. It is here that a dental specific advanced care plan, as discussed above, could be valuable. With time, a larger volume of treatment or treatment which is more complex or more invasive may be required which can be associated with substantial distress and post-operatively morbidity, especially in the advanced stages of dementia.16,17 Figure 2 shows the oral presentation of an individual living with early dementia. This is one example of how complex treatment planning can be when trying to balance the competing aims of reducing pain, managing active disease and maintaining function with long-term considerations in mind.

The oral presentation of a patient living with early dementia.
Treatment in the middle stage of dementia
In the middle stage, it may still be possible for patients to access care with their general dental practitioner with support from formal or informal carers and an understanding dental team. The goal of the dental practitioner at this stage is to diagnose and manage dental pain and to maintain and support oral hygiene. Freedom from pain cannot be realistically guaranteed, but efforts should be made to minimise this risk as dementia progresses. Preventive messages must be reinforced with the patient and care team, whilst adjuncts, such as high fluoride toothpastes, and ideally, professional application of fluoride varnish on a six-monthly basis would be beneficial. 18 Carers may be given specific training in how to support oral hygiene with the use of electric toothbrushes and personalised dietary advice. 19 Periodontal disease can significantly complicate treatment planning. The radiograph shown in Figure 3 demonstrates a generalised reduction in bone levels for a 74-year-old woman living with middle stage Alzheimer’s disease. This shows many teeth, with uncertain prognosis, which may rapidly become mobile as dementia progresses; it may be essential in a case such as this to proactively manage the most mobile teeth as preventing plaque accumulation may become increasingly challenging with time. Mental capacity is often retained at this point, but it may not be consistently present and extra support may be required to ensure patients remain involved in decision-making about their care. 7

Radiograph showing a generalised reduction in bone levels for a 74-year-old woman living with middle stage Alzheimer’s disease.
Treatment in the advanced stage of dementia
The final stage of dementia presents a wider range of challenges to all those involved in a patient’s care. Generally, a person may be older, less able or unable to communicate comprehensively and therefore be likely to lack capacity to consent for treatment or to understand what treatment is happening during care delivery. Symptoms of the condition can be significant, and alongside altered pain experiences, 20 a person’s ability to swallow safely can also be affected. 21 Other illnesses and frailty may also have progressed alongside the progression of dementia. These circumstances are not conducive to delivery of complex or comprehensive dental rehabilitation or to complex surgical procedures. It is these instances in which general anaesthesia or sedation may be essential if treatment is definitely indicated yet these approaches are associated with greater short- and long term risks.
In the absence of symptoms, treatment provision can offer a lesser benefit and can adversely affect aesthetics, masticatory function and quality of life,11,12,22 potentially to a greater extent than leaving conditions untreated. For example, it may be appropriate to leave asymptomatic retained roots or suboptimal advanced restorative treatment for which management would be intrusive or complex. 23 Both referring and treating clinicians must consider what dental status a person may be left with if extensive treatment were provided. Both a restored, high maintenance dentition or an edentulous state present substantial challenges and longer-term impacts for patients’ ability to eat, chew and smile. 23 Though symptoms and infection may necessitate this end point, it must not be arrived at without consideration for its impact. Consequently, an aim and outcome for a treatment process must be determined holistically with the support of those involved in a patient’s overall care. There is no one-size-fits all approach to patient care, yet clearly the anticipated benefit to a patient from delivering treatment must outweigh the risk of treatment delivery.
When to refer
It can be difficult to determine when a patient should be referred to specialist services, particularly when a low treatment need is anticipated, or long waiting lists lead a patient to seek care in general dental services whilst waiting for specialist assessment. The NHS England Commissioning Guide for Special Care Dentistry 24 details domains of patient care relevant issues that may mean referral is required to either a Level 2 practitioner, such as a dentist with additional relevant skills and experience, or to a Level 3 practitioner, a specialist or consultant. This framework, though useful, relates to the clinician’s experience, not the setting in which care is delivered; consequently, referral to a secondary care or hospital setting may be necessary only for the delivery of treatment whilst patient assessment may be undertaken in primary care environments based on the clinician’s experience.
General dental practitioners are expected to work within their competency 25 and this will vary based on experience and prior relevant training, meaning some practitioners may feel referral is required whilst others can provide ongoing care. When a dental professional has provided long-term care, the trust and rapport established can be of immense value, 16 especially for patients who may develop anxiety or become easily confused in a less familiar setting. This dental professional may be the most able to achieve a satisfactory outcome for patients who can tolerate treatment under local anaesthesia if and when needed and who have an established relationship with that individual.
Alongside the complexities that can arise in maintaining a heavily restored dentition, the nature and prevalence of dementia means that significant complexities can arise both in medical assessment, mental capacity assessment, treatment planning and treatment delivery. In these instances, referral should certainly be considered. As dementia progresses, it is more likely that treatment will be associated with increased medical, surgical and potential medico-legal risk.23,26 When treatment delivery is deemed necessary and appropriate, treatment within specialist services may well be appropriate. The decision to actively not provide treatment is more complex and is justifiable when it is felt that the extreme risk in providing care is not in a patient’s best interests. A decision of this complexity requires a substantial understanding of the considered medical and surgical and psycho-social risks, applied to each individual patient; clearly this is the remit of a specialist or consultant practitioner, and this is echoed in relevant service guidelines. 24
Conscious sedation and general anaesthesia for the person living with dementia
Many people living with dementia will also experience anxiety and depression which may impact on the acceptance of treatment. 27 If anxiety is marked, conscious sedation may be required. If a patient displays anxiety, inhalation sedation with nitrous oxide may be a useful adjunct as it provides anxiolysis. Whilst inhalation sedation may be suitable in the early stages of dementia, intravenous sedation may be required with extreme caution as the condition progresses. As dementia is more commonly found in older people, it is important that the clinician is aware of the physiological changes and common diseases that more commonly occur in ageing that may affect the pharmacodynamics of drugs. 28 For example, ageing is associated with increased sensitivity to the central nervous system effects of benzodiazepines. 29 Although the exact mechanisms are unknown, sedation is induced by diazepam at lower doses and lower plasma concentrations in older subjects. 30 When considering sedation for older people with dementia, it is advisable for procedures to be carried out in a secondary care setting.
When sedating older patients with intravenous midazolam, the ‘usual’ dose is halved and the amount of time between increments is doubled compared to the usual adult schedule. 31 It is worth considering that, even with this cautious titration, the process of recovery can be unpredictable and that a prolonged period of post-operative monitoring can be required to ensure somebody returns to their ‘baseline’ function. A secondary care setting facilitates a longer period of postoperative observation by an experienced recovery team. Intranasal sedation may be considered for the un-co-operative patient prior to intravenous sedation, but great caution is required and a secondary care setting, often with an anaesthetist, may be more appropriate due to the unpredictable response to an intranasal bolus of midazolam. A secondary care setting allows use of additional sedation agents, such as a continuous infusion of propofol; the use of anaesthetic drugs in sedation are well detailed in relevant guidelines.32,33
Where sedation or general anaesthesia need to be considered within specialist services, the consequences of treatment delivery both medically and psycho-socially increase significantly and a treatment plan must, therefore, consider both the treatment and the approach by which it is delivered. Crucially, a treatment plan must be arranged that reflects the complexity and degree of risk of anaesthesia provision. A repeat general anaesthetic exposes a patient to the same or greater risk and therefore, a dental treatment plan should strive to avoid the need to expose a person to a repeat general anaesthetic in the future. This may include more radical treatment; although this could impact function, aesthetics and post-operative discomfort, these adverse effects are less significant than the potential mortality risk with a repeat anaesthetic. Where possible, alongside the compulsory anaesthetic pre-assessment process, it is advisable that frail, older or otherwise complex patients with dementia are assessed by a specialist geriatric team prior to any treatment under general anaesthesia considering medical, functional, psychological and social issues, with the aim of reducing postoperative problems and ensuring a safe and effective discharge from hospital.
Conclusion
Every person living with dementia is an individual and the course of the disease will be distinct to them. Behaviour can fluctuate from one occasion to another and treatment planning for their care will depend on their previous dental history, the risks and benefits of the treatment under consideration, the stage of the dementia and their ability to comply. It is vital to take a holistic view to planning their care by considering the broader aspects of their health and wellbeing, including social and cultural factors that are important to them. This will enable the practitioner to discern what is in the individual’s best interests at this point in time whilst taking into account the potential outcomes that providing this treatment may produce in the future. Extensive restorative treatment may not be the most appropriate option, and in certain circumstances, providing simple treatments that can be easily maintained and preserve masticatory function are more apposite. The focus should be on eliminating pain, controlling infection and preventing new disease. Irrespective of the stage of the dementia, dental practitioners should continually seek ways to help facilitate the person to exert choice, control and influence over the care they receive and to provide services designed to meet their needs.
Footnotes
Disclaimer
Andrew Geddis-Regan’s academic post is funded by the National Institute for Health Research (NIHR) Doctoral Fellowship (NIHR300149). The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.