
Abstract
Background:
Discoloration of carious lesions after application of silver diamine fluoride lowers patient acceptance and limits its wider use for caries arrest.
Objective:
To assess lesion and tooth color changes from 2 novel silver fluoride (AgF) products and its relationship to caries activity (clinical visuo-tactile scores) and bacterial load (using laser fluorescence with the DIAGNOdent).
Methods:
A split-mouth design was followed, with matched smooth surface carious lesions in the same arch in adults with special needs randomized for 1-min treatments with AgF/potassium iodide (KI) (Riva Star Aqua, SDI) and AgF/stannous fluoride (SnF2) (Caries Status Disclosing Solution; Whiteley). Standardized images taken at baseline, immediately postoperatively, and at 3-mo review were subjected to digital image analysis to calculate delta-E and to track changes in luminosity of carious lesions.
Results:
Twelve participants were recruited in the study. A total of 56 teeth (28 pairs) were included. Significantly greater changes were seen in treated lesions than in the adjacent noncarious natural tooth structure, both immediately after treatment and at the 3-mo review (P < 0.0001). Color change and caries activity were not affected by tooth type, tooth location, plaque status, salivary status, or special needs condition. AgF/SnF2 caused transitory darkening immediately on application, while AgF/KI caused the immediate formation of yellow deposits (silver iodide). Both products caused significant darkening of treated lesions at 3 mo (P = 0.0009; P = 0.0361), with no differences between them (P = 0.506). Responding lesions showed larger and more perceptible color changes immediately after either AgF application (P = 0.002; P = 0.024).
Conclusions:
Both AgF products were highly effective for caries arrest in this patient population. Despite minor differences in the appearance of treated lesions at the time of application, both products lead to similar darkening of treated sites at 3 mo.
Knowledge Transfer Statement:
This study shows the usefulness of silver fluoride used in conjunction with potassium iodide or stannous fluoride for achieving caries arrest in smooth surface lesions in adults with special needs. Patients need to be informed that long-term staining of the lesion occurs with both, similar to silver diamine fluoride.
Keywords
Introduction
Individuals with special needs (i.e., intellectual disability, medical, physical, or psychiatric conditions) (SN) often have poor oral hygiene (Anders and Davis 2010) and elevated rates of untreated dental caries (Ziegler and Spivack 2018). They struggle to access timely and appropriate oral health care (Davis 2009; Anders and Davis 2010; Ziegler and Spivack 2018).
Silver diamine fluoride (SDF) and silver fluoride (AgF) offer a simple, noninvasive, and low-cost treatment to arrest carious lesions in this population, potentially eliminating the need for restorations (Rosenblatt et al. 2009; Contreras et al. 2017; Subbiah and Gopinathan 2018). Its application involves painting the solution onto dentine at the cavity base for 1 min (Rosenblatt et al. 2009; Rajendra et al. 2017). Therefore, it is ideal for patients with limited cooperation or unable to tolerate long procedures, such as adults with SN. SDF and AgF have been used for treating carious lesions in deciduous teeth and on root surfaces in older adults, including those living in residential aged care facilities (Rosenblatt et al. 2009; Lewis et al. 2015; Crystal, Marghalani, et al. 2017; Hendre et al. 2017; Crystal and Niederman 2019; Seifo et al. 2019).
While topically applied silver-based products have been shown in multiple studies to be free of systemic adverse effects (Vasquez et al. 2012; Lin et al. 2019), a particular concern with their use is staining of the treated lesion, as applied silver ions eventually become metallic silver deposits (Almuqrin et al. 2023). Staining of treated lesions limits parental acceptance of SDF for use on the anterior teeth of children (Bagher et al. 2019) and its wider use in adults (Crystal, Janal, et al. 2017; Alshammari et al. 2019; Crystal et al. 2019; Kumar et al. 2019; Huebner et al. 2020).
Several AgF products have been developed recently, with the goals of enhancing effectiveness for caries arrest while reducing staining. The first of these is Riva Star Aqua (SDI), where 38% AgF is followed by the application of potassium iodide (KI) (AgF/KI), to scavenge excess silver ions by forming a creamy yellow precipitate of silver iodide. This product lacks the 20% ammonia component of the parallel SDF product (Riva Star), which has SDF followed by KI. The other product is Caries Status Disclosing Solution (CSDS; RM Creighton Dental Pty Ltd; dental caries detecting stain, manufactured by Whiteley Corporation Pty Ltd t/a Whiteley Medical). This uses 40% AgF followed by 10% stannous fluoride (SnF2) (AgF/SnF2).
There is a strong evidence base for the clinical use of SDF for caries arrest, and its propensity to stain lesions is well known. Nevertheless, these same issues have not been explored for AgF products without ammonia. No past studies have assessed lesion discoloration over the medium term when KI or SnF2 is used after AgF. Therefore, the aim of this study was to compare AgF/KI with AgF/SnF2 in terms of the caries activity and the extent of tooth discoloration immediately after application and at 3 mo in adult patients with SN. The null hypothesis posits no difference in discoloration of the treated lesions between the 2 products. Participant attitudes toward AgF application process and discoloration were also assessed at baseline and 3-mo review.
Methods
Ethics Approval
Ethics approval for the study was granted by the Human Research Ethics Committee of Metro North Hospital and Health Services (HREC/2021/QRBW/73736) and the Human Ethics Research Committee of the University of Queensland (2021/HE002354). The study was registered with the Australian Clinical Trial Registry (ACTRN 12621001139864p).
Study Design
The present study used a split-mouth design to investigate the clinical effectiveness of these new products (AgF/KI and AgF/SnF2) in adult patients with SN.
Participants and Teeth
The study was conducted within an adult special needs dentistry (SND) clinical service operated in the public sector in Brisbane, Australia. Participants were recruited from adult SN patients attending routine dental treatment within this service who satisfied the eligibility criteria, with suitable paired teeth with similar carious lesions (Appendix Fig. 2). Participants with SN were aged at least 18 y and had at least 1 pair of similar carious lesions (cavitated or noncavitated) on smooth surfaces of the same type of teeth in the same arch and on opposing sides. The selected teeth were asymptomatic or had mild and reversible pulpal symptoms (nonlingering pain to cold, hot, and air) and no periapical pathology. All recruited participants had capacity to grant informed consent (written and verbal) for the study. Recruitment continued until the target number of participants was reached.
Interventions
Prior to clinical assessment, the selected teeth had plaque deposits disclosed using GC Tri-Plaque ID gel (GC Corporation) at both initial and review appointments and photographed.
Each site was photographed using a professional DSLR camera with a macro lens and ring flash (Canon EOS 5a; Macro Lens EF 100 mm 1:2.8; MR-14EX flash) with standardized settings (manual white balance, aperture F22, shutter speed 1/200 s, ISO 100, zoom ratio 1:1.5) after removing overlying plaque by a dental prophylaxis, immediately after treatment, and at 3-mo review appointment. An example of standardized images for 2 treated sites is shown in Figure 1.
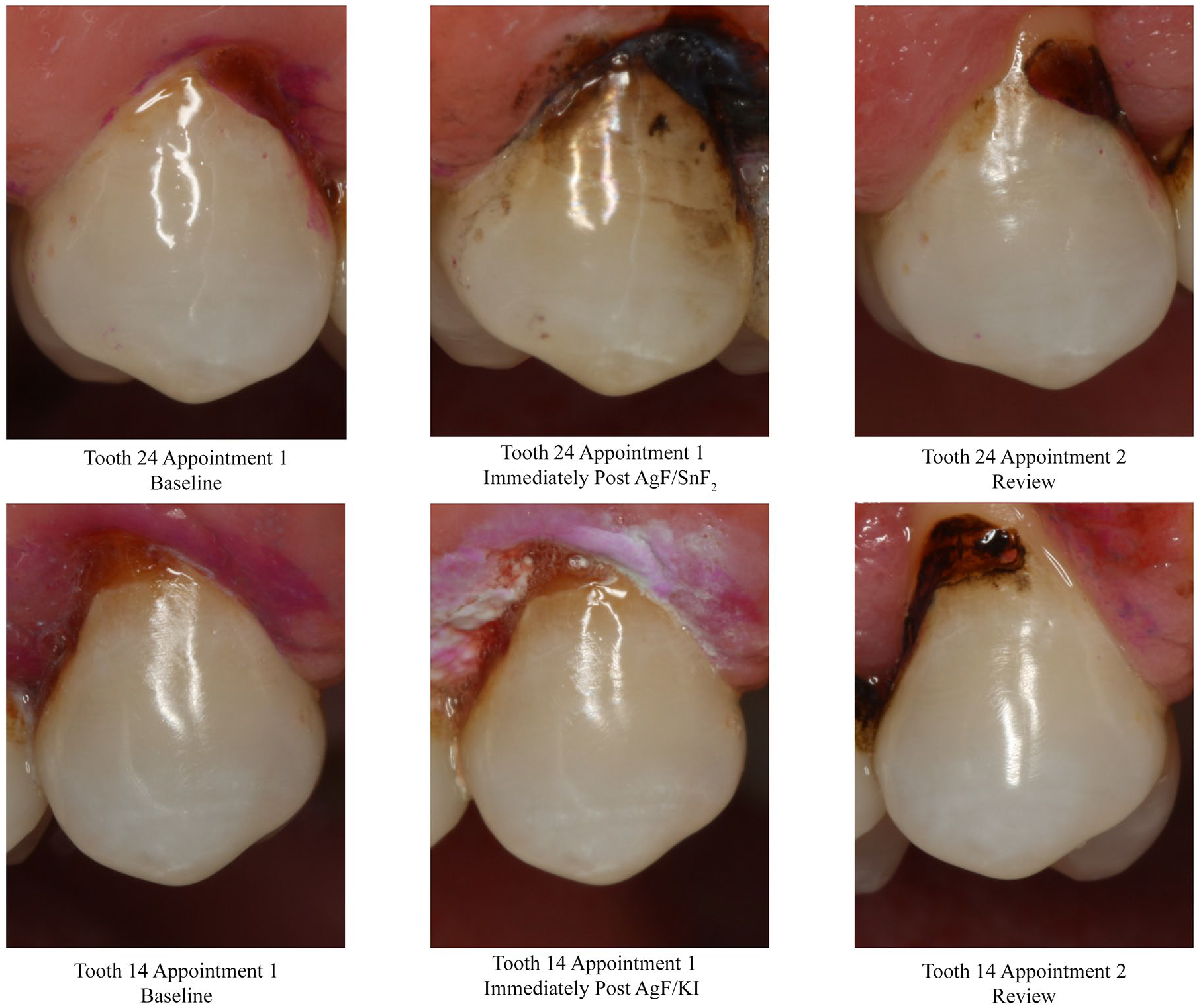
Example of serial images from the 1 patient showing contralateral maxillary first premolar teeth with cavitated carious lesions, at baseline, immediately postoperatively, and then at 3-mo review, for silver fluoride (AgF)/stannous fluoride (SnF2) (tooth 24, upper panel) and for AgF/potassium iodide (KI) (tooth 14, lower panel). Note how immediately after treatment, the lesion is darker for AgF/SnF2 and lighter for AgF/KI, but at 3 mo, both treated lesions appear similar in color.
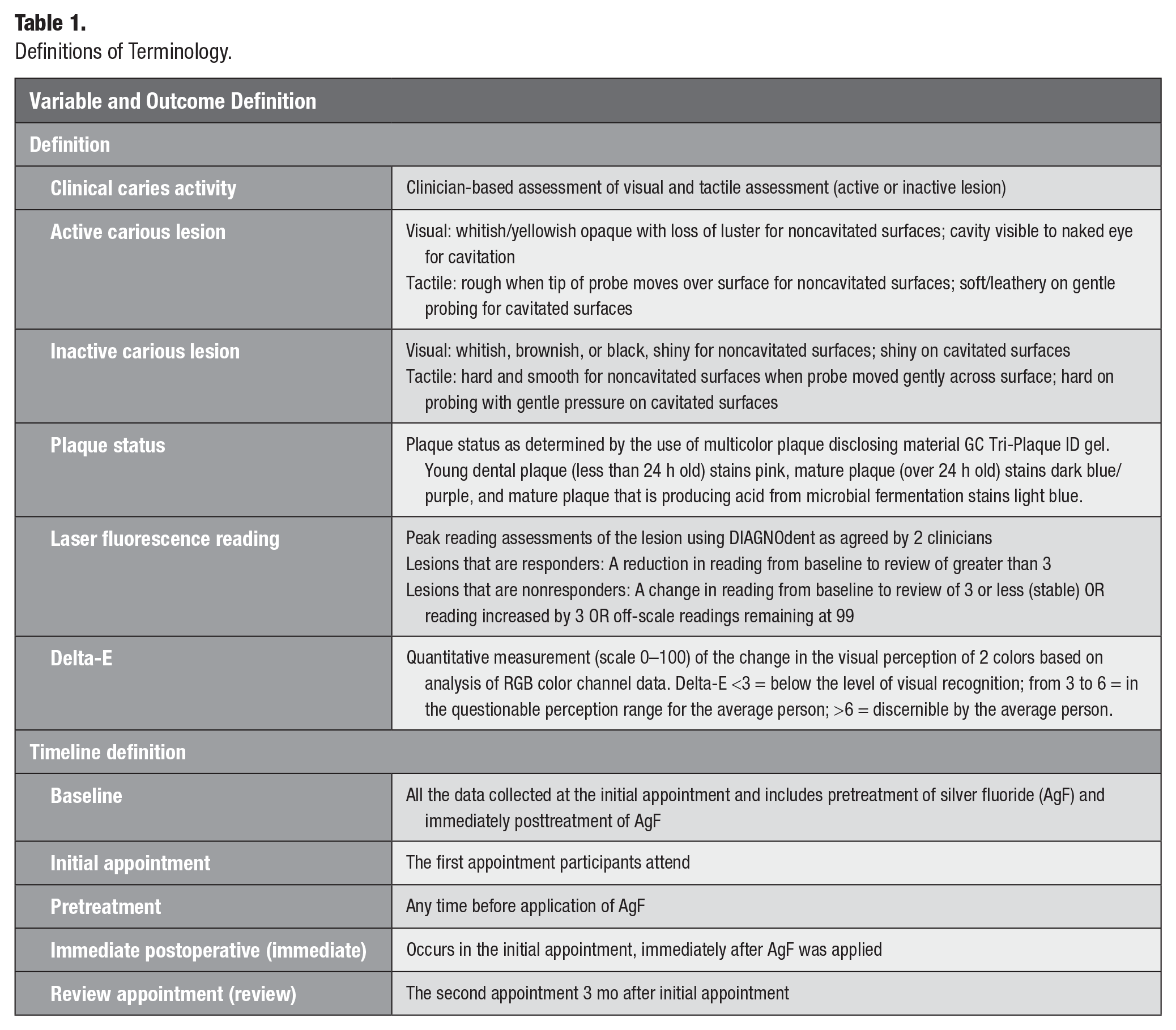
After plaque removal, the carious lesions were assessed using clinical caries activity via clinical visual-tactile (cVT) scoring and measurements of bacterial load on the carious lesion surface via laser fluorescence (LF) using the DIAGNOdent (DIAGNOdent Classic model 2095; KaVo) (Table 1). LF readings were taken with DIAGNOdent wide-area scanning tip (“B tip”) following daily device calibration and the peak value of duplicate readings used.
Definitions of Terminology.
Selected lesions were treated for 60 seach with either AgF followed by KI or by SnF2. The treated sites were photographed to assess immediate color changes and the adjacent gingiva and oral soft tissues inspected for any inflammation or irritation.
The participants were reviewed at their 3-mo review appointment, where dental plaque was assessed and removed by dental prophylaxis, and the same clinical protocol for photographing and assessing the lesions was followed.
At the end of the initial appointment, tailored oral hygiene and lifestyle/diet instructions were given to each participant.
Outcomes
The first outcome examined was discoloration of the treated carious lesion as compared to the adjacent noncarious natural tooth structure and at time intervals (baseline, immediate postoperative, and 3-mo review; Table 1). The second outcome was caries activity as measured using cVT and bacterial load via LF reading.
Additionally, the participant response to color changes in their teeth caused by the treatments were assessed. A short pretreatment questionnaire was administered at the initial appointment to gauge their expectations, with a posttreatment questionnaire at the review appointment. Questions explored attitudes toward AgF staining, the severity of staining, willingness to have AgF applied again, and overall experience of the application process.
Sample Size
The sample size was determined with a power analysis (Statmate 2 for Windows version 2.0; GraphPad Software), using the sample size for a paired t test. The estimated sample size was based on a previous study by the same clinical team that looked at quantitative assessment of lesion response patterns using LF. This study tracked multiple smooth surface lesions in a patient with SN with salivary hypofunction and high caries risk at baseline, over 12 mo (Vlacic et al. 2007). For LF readings, the expected standard deviation (SD) of each group was 15 and the expected correlation (r) among pairs was 0.95. The significance level (α) was set at 0.05 (2-tailed). A sample size of 12 pairs of teeth (1 tooth pair per patient) has a 95% power to detect a difference between LF means of 5 with an α of 0.05 (2-tailed).
Randomization and Blinding
Participants were blinded to the material used. A random number generator was used to allocate treatments within lesion pairs. Assessments of treated lesions at 3 mo were made without reference to previous records regarding the treatment used. Clinical data were deidentified prior to data entry and analysis.
Data Analysis
Statistical analysis was undertaken using Jamovi software version 2.2.5 (The Jamovi Project). Graphs were created using Microsoft 365 Excel Version 2304 (Microsoft Corporation). A P value of <0.05 was used as the threshold for statistical significance. Prior to analysis, data sets were assessed using the Shapiro–Wilk normality test. Based on Levene’s homogeneity of variance test, all data sets had comparable variance. Where data sets had normal distributions, the independent and paired-sample Student’s t tests were used to compare the means of continuous data. Any situations where data sets did not follow a normal distribution were dealt with by using the Wilcoxon rank or Mann–Whitney U tests. For categorical data, the χ2 test of independent association and the McNemar test were used.
To determine lesion response patterns, LF reading and cVT scoring were used. A change in the LF reading of more than 3 was considered important, based on the manufacturer’s instructions. The treated lesions were categorized as responders (LF readings reduced by 3 or more) or nonresponders (stable or increasing readings) (Table 1). In addition, lesions were classified at both visits based on their clinical characteristics (Nyvad et al. 1999) as either active or inactive (Table 1).
The outcome of color change was analyzed based on image analysis of sequential digital photographs of the treated areas using Adobe Photoshop CC 2019 software (ver. 22.4.3; Adobe) to determine changes in luminosity and delta-E values for the 2 regions of interest (carious region and the adjacent region of noncarious natural tooth structure). Delta-E was used as this is a standard method for comparing color changes and provides insight into whether such changes are meaningful (Athanassiadis et al. 2022). An average person will detect a color change for delta-E values of greater than 6, while a trained person can detect changes at a delta-E value of 3 (Athanassiadis et al. 2022) (Table 1).
The 2 regions of interest were selected for separate analysis following methods described previously (Athanassiadis et al. 2022) (Appendix Fig. 1), with areas of flash reflections excluded. Delta-E values were calculated from red, green, and blue (RGB) color channel data using an online calculator (http://www.colormine.org/delta-e-calculator/cie2000), for baseline to immediate postoperative, for immediate postoperative to 3-mo review, and for baseline to the 3-mo review. Luminosity values were calculated from RGB data using the following formula:
Luminosity = (0.2126 × Red) + (0.7152 × Green) + (0.0722 × Blue).
Relationships between luminosity, delta-E, and AgF product type were explored through statistical analysis, with additional analyses for potential effect modifiers (tooth type, carious lesion type, arch type, plaque status). The extent of plaque over the lesion and its status (Table 1) was calculated based on the pixel count (Walsh and Healey 2019; Tabatabataee et al. 2021). Changes in LF reading and luminosity values were assessed using bivariate data analysis.
To assess the reproducibility of the image analysis approach, a repeat assessment of 44 images for RGB channel data (including at least 1 tooth series from each participant) was undertaken 4 mo later. Linear regression analysis of the initial and repeat data for baseline, immediate, and review showed high reproducibility (Appendix Table 1).
The assessment of the 2 questionnaires explored how participants viewed the AgF staining, whether they would be willing to have AgF applied again, and their experience of the application process.
Results
Participants
During recruitment, 22 individuals with SN met the inclusion criteria with suitable paired lesions, and of these, 12 agreed to participate in the study (Appendix Fig. 2). The mean age was 50.4 y (range, 34–73 y). The mean interval between the baseline and the 3-mo review visit was 94.2 d (median, 91.0 d; range, 70–140 d). All participants completed the study.
Across the 12 participants, there were 28 pairs (56 teeth, 12 maxillary and 44 mandibular arch; 48 with cavitated lesions extending into dentine and 8 with incipient smooth surface caries) (Table 2). The 8 noncavitated lesions were a mixture of root caries and cervical third caries. All lesion pairs had lesions of the same type, and all included lesions were readily accessible.
Participants and Sites.
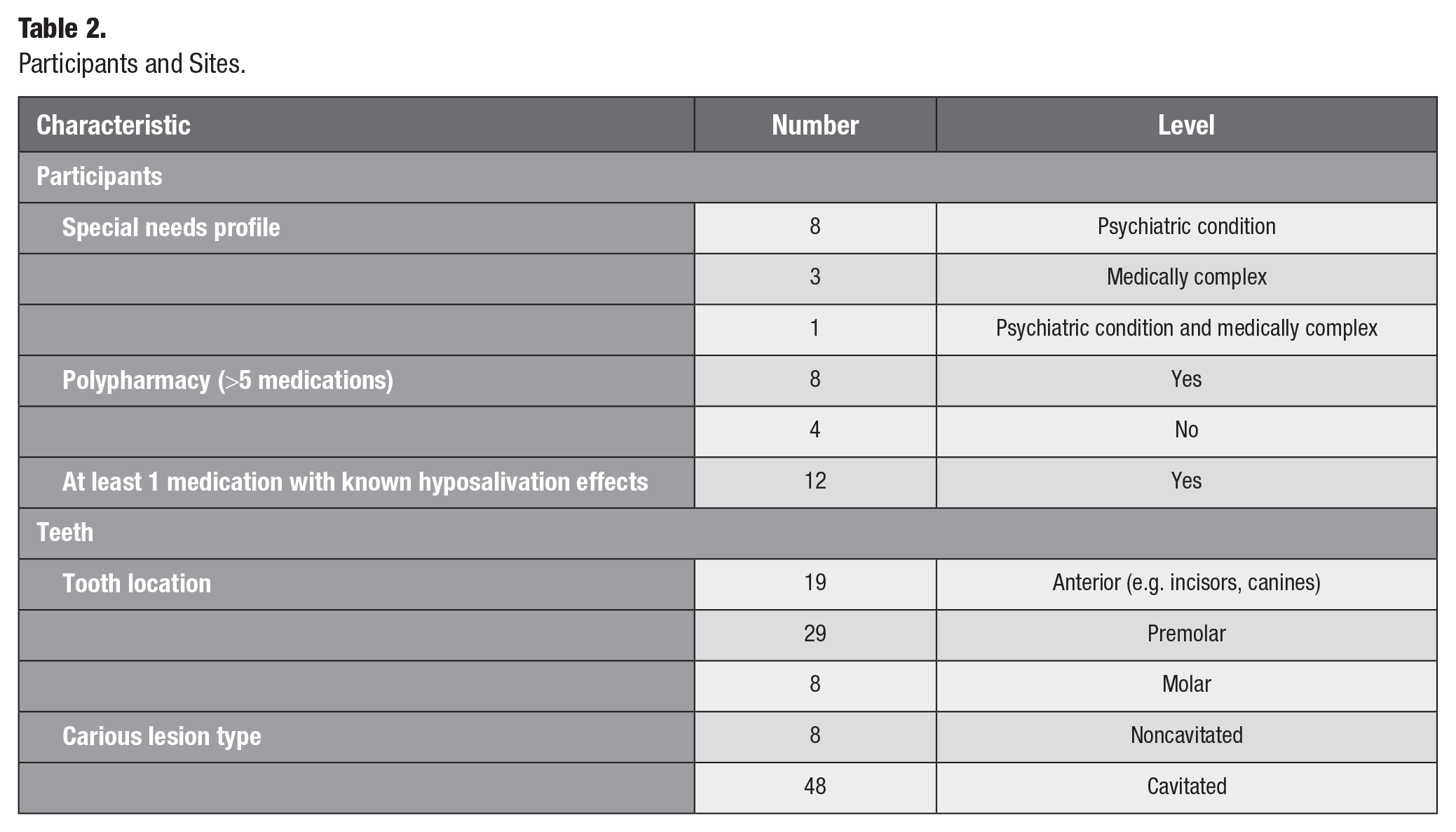
With 28 pairs of teeth, a post hoc power analysis based on the standard deviation of the differences across both AgF products showed that the study had an 80% power to detect a delta-E difference of 7.94, a luminosity difference of 18.53, and a fluorescence difference of 11.63, with a significance level (α) of 0.05 (2-tailed).
Caries Activity
The cVT assessment response patterns were as follows: nonresponders (active lesions staying active or inactive lesions becoming active; AgF/SnF2 n = 1, AgF/KI n = 2), responders (active lesions becoming inactive; AgF/SnF2 n = 23, AgF/KI n = 23), and stable (inactive lesions staying inactive; AgF/SnF2 n = 4, AgF/KI n = 3). Since the LF reading had an upper limit of 99, any readings of 99 at review would not reflect numerically the caries activity of the lesion. Thus, for LF readings, samples where the baseline and the review score were both 99 were not included in this analysis (n = 6). The LF reading response patterns were as follows: nonresponders (increased reading by >3; AgF/SnF2 n = 5, AgF/KI n = 5), responders (lowered reading by >3; AgF/SnF2 n = 16, AgF/KI n = 20), and stable (change of 3 or less; AgF/SnF2 n = 3, AgF/KI n = 1).
Delta-E and Luminosity
Both treatments caused darkening of the lesion from baseline to 3 mo, with reduced luminosity (Fig. 2; repeated-measures nonparametric analysis of variance AgF/SnF2 P = 0.0009; AgF/KI P = 0.0361). AgF/SnF2 caused significantly more darkening immediately after application at the initial appointment than AgF/KI (mean delta-E values 16.34 ± 8.1, 95% CI = 13.2–19.5 vs. 10.00 ± 5.6, 95% CI = 7.9–12.2; P = 0.001). Delta-E values from the immediate postoperative situation to the 3-mo review were not significantly different for AgF/SnF2 (mean 13.03 ± 9.6, 95% CI = 9.3–16.8) and AgF/KI (mean 14.35 ± 8.9, 95% CI = 10.9–17.8; P = 0.402). In terms of the overall effect of treatment from baseline to 3 mo, once again the delta-E values were not statistically significant (AgF/SnF2 mean 8.65 ± 6.2, 95% CI = 6.2–11.1; AgF/KI mean 11.33 ± 8.3, 95% CI = 8.1–14.5; P = 0.286). Thus, the null hypothesis that there was no difference in darkening at 3 mo between the 2 products was not rejected. Significantly greater changes were seen in treated lesions than in the adjacent noncarious natural tooth structure, both immediately after treatment and at the 3-mo review (P < 0.0001).
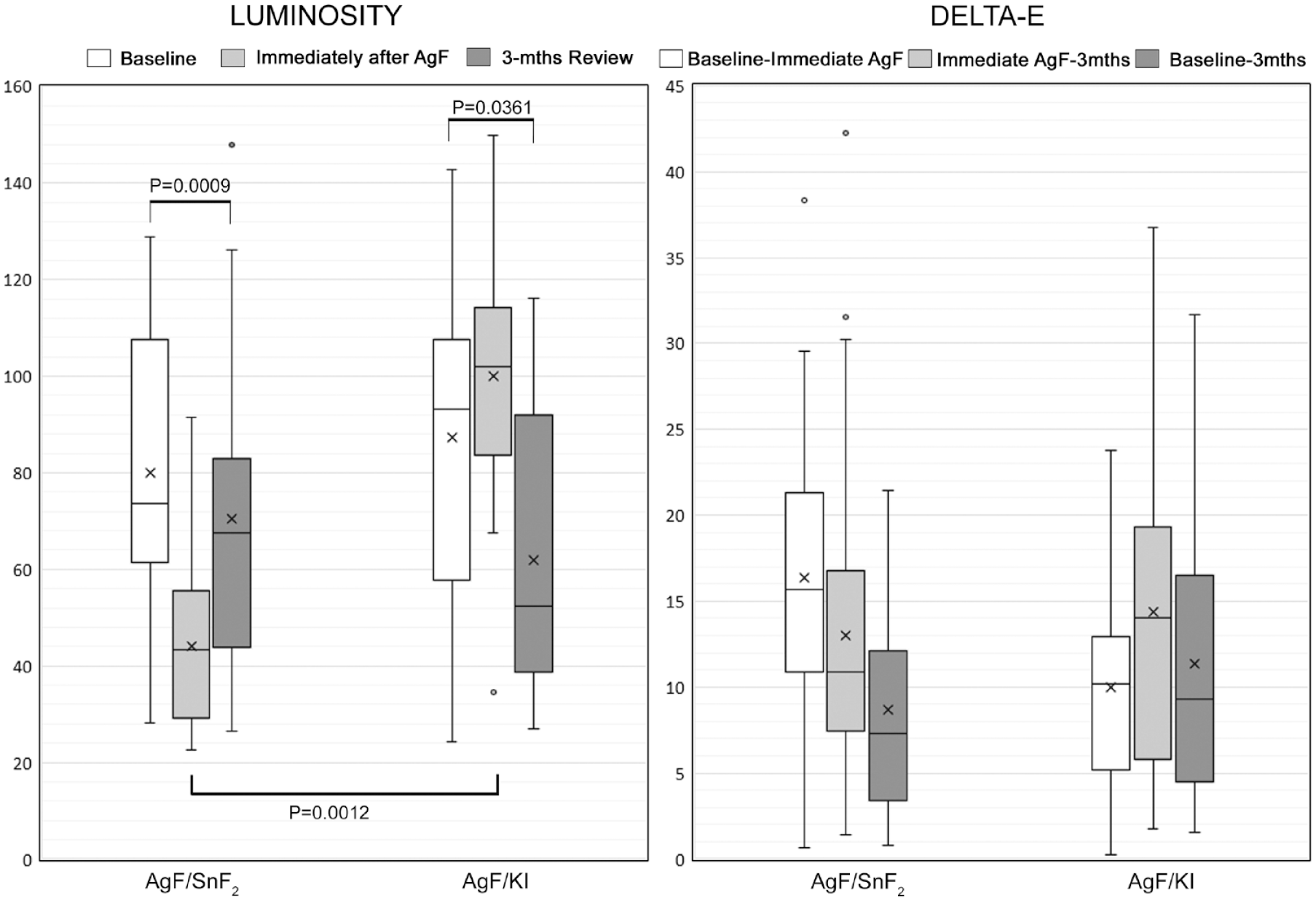
Luminosity and delta-E data. The left panel shows box-and-whisker plots for luminosity at baseline, immediately after silver fluoride (AgF) application, and at 3-mo review for AgF/stannous fluoride (SnF2) and AgF/potassium iodide (KI). The right panel shows the corresponding delta-E data for the same lesions. In these box-and-whisker plots, the box is the interquartile range, the median is shown as a horizontal line, whiskers show the maximum and minimum values, and the dots indicate outliers. The arithmetic means are shown as “x.” Luminosity changes for both AgF/SnF2 and AgF/KI from baseline to 3 mo were significant (P = 0.0009 and P = 0.0361, respectively). AgF/SnF2 caused significantly more darkening immediately after application at the initial appointment than AgF/KI (P = 0.0012).
Visual Perception of Lesion Color Changes Based on Delta-E
Of the 56 teeth that were treated, darkening of the dentine that would be readily discernible by the average human eye (delta-E above 6) occurred in 46 teeth (82.1%) immediately and in 35 teeth (62.5%) from baseline to 3 mo. There were no significant differences between the 2 treatment groups for either time period (P = 0.108 and P = 0.506). Responding lesions showed larger and more perceptible color changes immediately after either AgF application (AgF/KI P = 0.002; AgF/SnF2 P = 0.024). Changes in noncarious adjacent natural tooth structure were not significant. Delta-E scores were not significantly affected by tooth type (P = 0.096), arch type (P = 0.448), or lesion type (cavitated vs. noncavitated, P = 0.284) (Appendix Tables 2 and 3).
Association between Luminosity and Response Patterns Based on Fluorescence Readings
When lesions were categorized by their fluorescence changes into responders (reduced fluorescence) and nonresponders (no change or increased fluorescence), when taken across both groups, the responding lesions were darker at baseline, with lower luminosity values (mean 78.5 ± 29.9, 95% CI = 68.3–88.6 vs. 105.3 ± 8.2, 95% CI = 86.8–123.7; P = 0.031), and also darker at review (60.2 ± 27.6, 95% CI = 50.8–69.5 vs. 91.0 ± 21.5, 95% CI = 75.6–106.4; P = 0.008, respectively). When considering the 2 products separately, nonresponding lesions for AgF/KI were lighter than responding lesions at baseline (113.8 ± 20.8, 95% CI = 87.9–139.7 vs. 83.5 ± 32.2, 95% CI = 68.5–98.6; P = 0.050) and also at review (91.8 ± 11.6, 95% CI = 77.4–106.2 vs. 57.2 ± 27.1, 95% CI = 44.5–69.8; P = 0.035) (Fig. 3). The same trend was seen for AgF/SnF2, even though differences did not reach the threshold for statistical significance for lesions at baseline (96.8 ± 29.7, 95% CI = 59.8–133.7 vs. 72.1 ± 26.4, 95% CI = 58.0–86.2; P = 0.210) or at review (90.1 ± 30.1, 95% CI = 52.8–127.5 vs. 63.9 ± 28.8, 95% CI = 48.5–79.2; P = 0.143) (Fig. 3). Tooth type, carious lesion type, arch type, and plaque status did not influence the laser fluorescence readings (See et al. 2024).
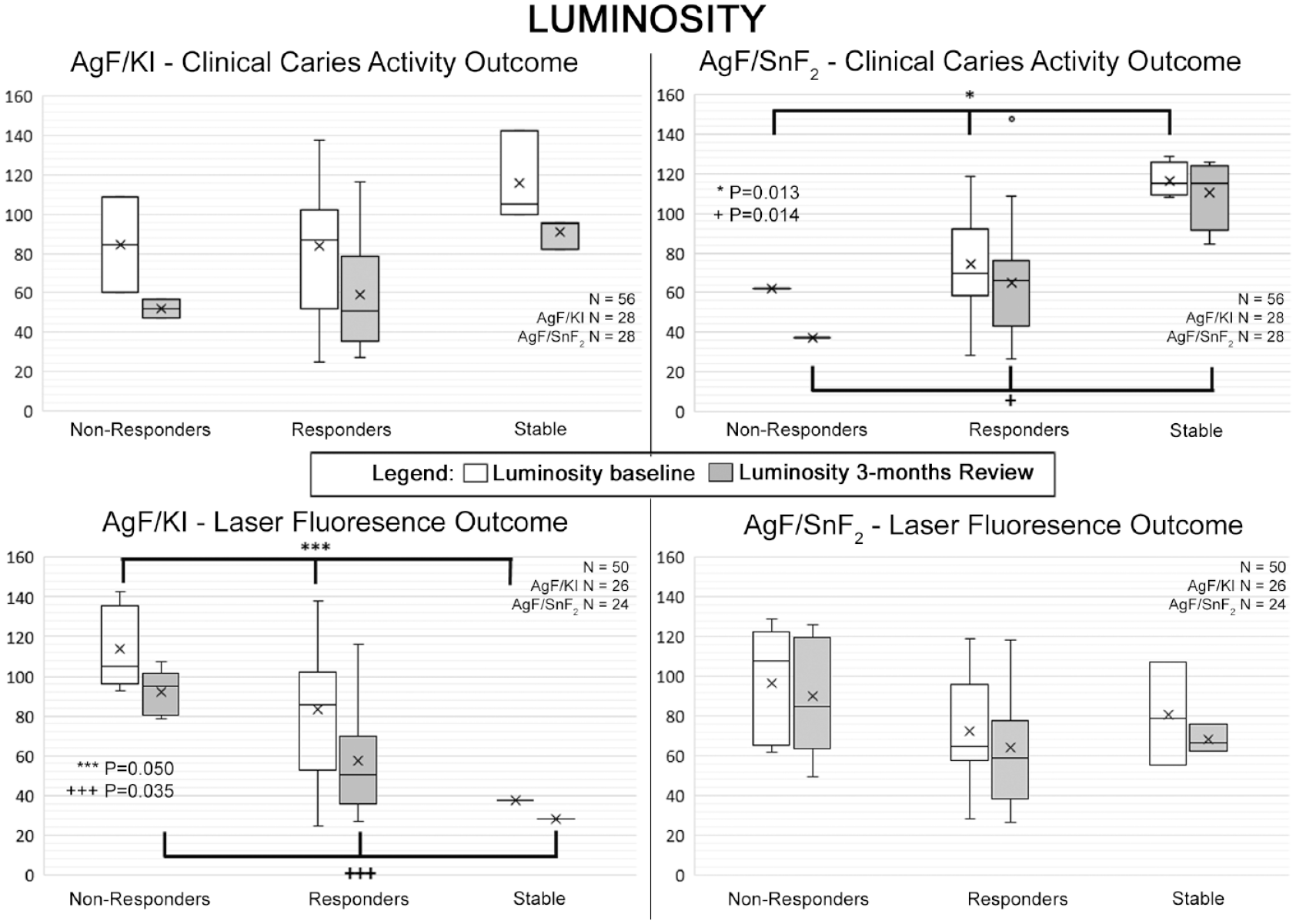
Data analyses by response pattern for each product according to clinical caries activity based on clinical visual-tactile (cVT) (upper series) and laser fluorescence (LF) readings for bacterial load (lower panel) for the baseline before treatment and the 3-mo review. For LF readings, samples where the baseline and the review score were both 99 were not included in this analysis (n = 6). LF reading response patterns were as follows: nonresponders (increasing reading by >3), responders (lowered reading by >3), and stable (change of 3 or less). In the box-and-whisker plots, the box is the interquartile range, the median is shown as a horizontal line, and whiskers show the maximum and minimum. The arithmetic means are shown as “x.” For sites classed as responders based on clinical caries activity, luminosity was less for silver fluoride (AgF)/stannous fluoride (SnF2) at baseline (P = 0.013) and at review (P = 0.014). Based on LF outcomes, luminosity was less for AgF/potassium iodide (KI) responders at baseline (P = 0.050) and at review (P = 0.035).
Assessment of Participant Attitude toward AgF Application and Discoloration
Prior to the use of AgF, most participants were willing to have an AgF material applied so that the caries process could be stopped, and the teeth did not require restoration (8 of 12 for anterior teeth and 9 of 12 for posterior teeth). Staining was seen as preferable to tooth loss (Appendix Table 4).
At the review appointment, all 12 participants were willing to have AgF used again. One participant was “not satisfied” but commented that “I’m socially isolated enough that the coloring is mortifying but rarely affects my life.” All others were satisfied despite the staining and commented that it was less obvious than first imagined and was not a concern, especially for posterior teeth. Additionally, all participants believed that the process of AgF application was simple, fast, and pain free (Appendix Table 5).
No adverse or unintended soft tissue effects were seen immediately after application for either product or at review, and none were reported in the questionnaire.
Discussion
The strengths of this study are its split-mouth design, the reproducibility of the photographic analysis of changes in lesion color, and the standardized lesion assessments using laser-induced fluorescence. Both these methodologies are readily available on the market, and this facilitates further studies on AgF in everyday clinical practice using these same methods.
A limitation of the study is that the overall number of participants was small, and numbers within each domain of SN were low, and those with limited cooperation were not included. Another limitation was that the quality of home oral care practice that could affect caries risk was not tracked over time during the 3-mo period between visits, even though dental plaque was assessed at the beginning and end of the study. A further limitation was that for the study population, the timing of attendance for review visits was complicated by COVID-19 pandemic-related restrictions to the operation of the clinical service, as well as by periods of hospitalization for some participants.
Overall, the present results are promising for the use of the AgF/KI and AgF/SnF2 approaches. Of the 2 products, color changes at the time of placement were greater with AgF/SnF2 than for AgF/KI, which reflects the different agents used. Immediate visual effects were more apparent with the SnF2 combination with AgF than when KI was used immediately after AgF. The explanation for this is that SnF2 can cause staining by reacting with denatured proteins and forming darker stannic sulfide (Ellingsen et al. 1982). The formation of dark products reflects the original design intent, since areas that do not stain were found to be 4.6 times more likely to show caries progression (Craig et al. 2013).
When KI is applied after AgF, some excess silver ions will react to form silver iodide. This light yellow compound will cover the site and obscure the appearance of dark tooth structure, at least for a short period of time, until the silver iodide decomposes, especially as it reacts to ambient light (Almuqrin et al. 2023). As well, by consuming excess silver ions on the tooth surface, less formation of silver phosphate will occur when KI is used (Haiat et al. 2021).
Both AgF and SDF cause dentine discoloration in treated lesions due to excess ionic silver, forming various compounds, including silver phosphate, silver oxide, and silver sulfide, through reactions with tooth structure and microorganisms (Almuqrin et al. 2023). Some of these silver compounds will break down to release more silver ions (Hiraishi et al. 2022), while others eventually become reduced to elemental silver (Sayed, Matsui, Hiraishi, et al. 2019). Silver ions exhibit strong antimicrobial actions, damaging microbial cell walls, denaturation of enzymes, and inhibition of DNA replication (Peng et al. 2012). They bind to collagen (Sayed, Matsui, Uo, et al. 2019), which ensures a long-lasting antibacterial action. These points explain why there is a connection between a desirable response occurring in a treated lesion and the presence of greater amounts of silver in its various forms in the dentine and hence darkening. In this study, responding lesions darkened more than nonresponding lesions, suggesting that lesions not darkening over time, when reviewed (e.g., at 3 mo), may require a second treatment to achieve caries arrest. This aspect should be explored in further studies.
The present study used fluorescence readings of the bacterial load within the dentine to categorize lesions into responders and nonresponders. When silver ions are present, they exert strong inhibitory effects on bacteria such as Streptococcus mutans, Actinomyces naeslundii, Streptococcus sobrinus, and Lactobacillus acidophilus (Haiat et al. 2021; Zhang et al. 2021). In line with this, a reduction in fluorescence readings will occur as bacterial growth within the dentine is inhibited.
Changes in lesion color can occur due to changes in bacterial metabolic activity, which alter bacterial synthesis of pigments. Highly active dentine carious lesions may contain more lactobacilli and Actinomycetes (Martin et al. 2002), and the latter can generate dark pigments (Sarkonen et al. 2001), especially Actinomyces odontolyticus, which is found in advanced dentine carious lesions (Batty 1958). There is no clear cause-and-effect connection between the numbers and type of bacteria in carious dentine and the color, and hence color should not be used as a sole indicator of carious lesion status (Lynch and Beighton 2009).
This study indicated that tracking luminosity may show statistically significant changes over time that are not relevant to patients, as they are below their threshold for visual detection. Dentists, on the other hand, are more attuned to color changes because of professional training, particularly in relation to recording shades of teeth. Therefore, detecting visual changes may be more clinically relevant for a dentist to track the response of the carious lesion after AgF application. Previous studies caution against using color as a sole indicator of carious lesion status, due to unclear cause-and-effect connection between the numbers and type of bacteria in carious dentine and the color (Lynch and Beighton 2009). Rather, visual and conventional tactile assessment can be used (Sayed et al. 2021; Hiraishi et al. 2022). From the results of this study, a clinical protocol could be developed where changes in color in combination with cVT and LF assessment are used to indicate the need for reapplication of AgF at the review appointment.
The results from this study show that both AgF/KI and AgF/SnF2 cause similar darkening of treated lesions by 3 mo but not of the adjacent enamel. While this color change is visibly evident to nonexpert observers in almost two-thirds of treated teeth at 3 mo posttreatment, it does not present a major concern to most participants. The participants’ experience was positive in terms of the speed and comfort of the application process. This reflects another study where participants may be more prepared to accept some staining in situations where the management of pain and disease are higher priorities than aesthetics (Magno et al. 2019).
Future research should explore how well AgF and SDF materials work and are accepted by patients in private dental practice, since this may be different to the cohort of patients with SN attending a public-sector SND service for adults. Patients seeking dental care in a private setting may be less willing to have a treatment that could impair the appearance of individual teeth within the aesthetic zone. Previous studies have highlighted parental reluctance to accept treatments causing staining of the treated carious lesions in their children’s teeth (Alshammari et al. 2019). If darkening is a major obstacle to acceptance, more emphasis can be expected on forms of AgF that may be less able to cause staining (Almuqrin et al. 2023) and on techniques where the treated root surface is covered with an opaque restorative material so that staining is no longer visible.
Conclusion
Both AgF products effectively arrested caries in adults with SN, leading to similar darkening of treated sites at 3 mo. AgF treatment provides a practical solution for patients with low tolerance for dental procedures, reducing barriers to timely care. The treatment protocol’s simplicity makes it readily adoptable in everyday practice. Future research should explore responses among subpopulations with SN and assess the effects of multiple AgF applications on lesion progression, bacterial load, and tooth discoloration.
Author Contributions
L. See, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; S. Zafar, C. Lopez Silva, contributed to conception, design, critically revised the manuscript; D. Fu, contributed to data acquisition, critically revised the manuscript; D.H. Ha, contributed to data analysis and interpretation, critically revised the manuscript; L.J. Walsh, contributed to conception, design, data analysis and interpretation, drafted and critically revised the manuscript. All authors have their final approval and agree to be accountable for all aspects of work.
Supplemental Material
sj-pdf-1-jct-10.1177_23800844241246199 – Supplemental material for Tooth Discoloration from 2 Silver Fluorides Used in Adults with Special Needs: A Randomized Trial
Supplemental material, sj-pdf-1-jct-10.1177_23800844241246199 for Tooth Discoloration from 2 Silver Fluorides Used in Adults with Special Needs: A Randomized Trial by L. See, S. Zafar, D. Fu, D.H. Ha, L.J. Walsh and C. Lopez Silva in JDR Clinical & Translational Research
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by research grants from the University of Queensland School of Dentistry and a UQ Colgate-Palmolive student research grant. Riva Star Aqua was provided by SDI, but the study was not sponsored by SDI, and the company had no input into the design and execution of the study.
A supplemental appendix to this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.