
Abstract
Background:
Uganda is among the 30 high tuberculosis (TB) burden countries, and still grapples with a suboptimal treatment success rate (the sum of cured and treatment completion), which stands at 89.1% for people living with HIV and 91.2% for those without HIV. The Teso region, one of the high TB burden regions in the country, has consistently had a lower treatment success rate (TSR).
Objectives:
To determine the treatment success and associated factors among drug-susceptible TB individuals in the Teso region, Uganda.
Design:
This retrospective study was conducted in the five (5) largest TB diagnostic units in the Teso region of Northeastern Uganda from 1st March 2025 to 28th March 2025.
Methods:
Data were collected from the health facility’s TB treatment register. The primary outcome was treatment success. Data were analyzed using Stata statistical software, version 15.0, and summarized into proportions and frequencies. Modified Poisson regression analysis was conducted to determine factors associated with treatment success and reported as adjusted prevalence ratios (aPR). A p < 0.05 was considered statistically significant.
Results:
Data from 1009 individuals were included in the analysis; the median age was 45 years, with an interquartile range of (28–60). The majority of the individuals, 48.1% (n = 485), were aged 15–49 years. Just over half, 52.9% (n = 534), were male, and 54.5% (n = 550) had bacteriologically confirmed TB. The overall TSR was 91.9%. Factors associated with a higher treatment success were being female (aPR = 1.04; 95% CI: 1.002–1.07, p = 0.041). In contrast, being aged > 49 (Elderly) (aPR = 0.95; 95% CI: 0.89–0.99, p = 0.042) and living with HIV (aPR = 0.93; 95% CI: 0.88–0.98, p = 0.008) were associated with a lower likelihood of treatment success.
Conclusion:
In this study, being female was associated with higher treatment success, while being older than 49 years and having HIV were associated with lower treatment success. This calls for early screening and strengthening TB preventive therapy among the people living with HIV, peer-to-peer support among the elderly for treatment adherence to improve TSR, and to achieve the goal of eradicating TB by 2030.
Plain language summary
This study determines the treatment success and associated factors among drug-susceptible TB individuals in the Teso region, Uganda. Of 1009 people treated for drug-susceptible tuberculosis (TB) in the Teso region of Uganda, the overall treatment success rate was 91.9%. We found that a person’s likelihood of successful treatment was linked to their sex, age, and HIV status. Being female was associated with a higher chance of treatment success. In contrast, being over 49 years of age or living with HIV was associated with a lower chance of successful treatment. To improve TB treatment outcomes and work towards eradicating TB by 2030, we recommend early TB screening, strengthening TB preventive therapy for people living with HIV, and providing peer support to help with treatment adherence, especially for older adults and those with HIV
Introduction
Tuberculosis (TB) remains the leading cause of death from a single infectious disease, with over 10 million new cases annually. In 2023, there were 10.8 million cases reported, an increase from 10.7 million in 2022.1,2 The global TB treatment success rate (TSR) remains suboptimal at 88%, below the expected End TB 90% target, with a total of 1.25 million people dying from TB, including 1.09 million among HIV-negative people and 161,000 people with HIV. 1 In the World Health Organization (WHO) African Region, despite the TB incidence rate declining every year since 2010, 3 the region still accounts for 25% of the global TB burden,4–6 and the treatment success rate remains low at 79%. 7
Uganda is among the 30 high TB/HIV burden countries that collectively accounted for 86% of the global TB burden in 2022 and 2023. 8 The national TB case detection rate decreased from 102% in October–December 2022 to 87% in October–December 2023, with the TSR improving from 90% in 2019 to 91% in the same period.9–11 However, regional disparities in treatment outcomes persist, with some regions falling below the national strategic plan target of greater than 90%. 11 Several patient and systemic level factors have been associated with suboptimal TSR, including being male, older age, prior TB treatment,12,13 HIV coinfection, 5 and drug stock-outs. 14
The Teso region in Uganda has a high TB burden, but TSR has consistently been lower than the national averages, estimated at 80.7%–87% compared to the 2023 national average of 91%.10,11 Understanding the factors contributing to the suboptimal TSR in such rural settings is critical to designing targeted interventions to improve the outcomes to achieve the end TB strategy by 2030.7,9 This study aimed to determine the treatment success and associated factors among drug-susceptible TB individuals in the Teso region.
Methods
Study design
We conducted a retrospective study involving quantitative data collection from five health facilities’ TB treatment registers using a data abstraction tool adopted from the literature on factors affecting TSR and piloted at TASO Soroti Centre of Excellence for validity.13,15 Data collection was conducted from 1st March 2025 to 28th March 2025, and findings were reported in accordance with Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines (Supplemental material). 16
Study setting
The study was conducted in the five (5) largest public health facilities across the districts of Kumi, Serere, Bukedea, and Ngora in the Teso region of Northeastern Uganda. The selected facilities included Atutur Hospital and Kumi HC IV in Kumi district, Serere Health Center IV in Serere district, Bukedea Health Center IV in Bukedea district, and Ngora HC IV in Ngora district. 17 These health facilities were purposively selected due to their high number of clients treated for TB. Each health facility serves as a TB diagnostic and treatment unit, with a designated TB focal person (who is either a nurse or a clinical officer) supervised by the District TB and Leprosy Supervisor, who oversees TB treatment and management at the district level.
The combined population of these districts was estimated at 1,141,833 in 2024, 18 with a low HIV/AIDS prevalence rate of 4.2% compared to the national average, 19 a high poverty rate of 3.6%, with 10.7% of the population having an acute respiratory infection, and 5.2% having smoking behavior. 20 The districts are rural, and most residents are subsistence mixed farmers, keeping goats, cattle and tending crops for a livelihood.
Study population
We included all individuals diagnosed with drug-susceptible TB and started on TB treatment between 1st October 2021 and 30th December 2023, as recorded in the health facility registers at the study sites. We excluded individuals with incomplete data on key variables such as HIV status (this is a major predictor of treatment outcome, and its absence is critical in analysis), age, gender, and disease type. Individuals with multidrug-resistant TB were also excluded from the study due to a different treatment protocol.
Minimum sample size estimation
We determined a minimum sample size of 987 using Kish Leslie’s formula (1965) for single populations, considering a 95% confidence, a 5% margin of error, a design effect of 2.5, a nonresponse rate of 10%, and a TSR of 63.9% from a previous study conducted in rural settings of Uganda. 21 To improve the precision of our estimate, we reviewed 1062 records. After excluding 53 records, a final sample of 1009 was included in the analysis.
Sampling procedure
We conducted a census of all eligible TB patients within the selected health facilities during the study period.
Data collection and instruments
Using a designed data abstraction tool focusing on key routinely collected data, which was pretested at the TASO Soroti center of excellence, data were extracted on both the exposure and outcome variables from the health unit TB registers from the time treatment started until the end of treatment. Those with missing data were cross-checked with electronic medical records to ensure accuracy and completeness.
Study variables
The independent variables included demographic characteristics (age, gender), disease classification categorized as bacteriologically confirmed TB patients (BC) (where a biological specimen is positive for TB by urine lipoarabinomannan, GeneXpert, culture, Truenat or Microscopy), clinically diagnosed TB patient (CD) (diagnosed with active TB based on clinical assessment, suggestive histology and chest X-ray diagnosis), and extrapulmonary TB (a diagnosis of TB outside the lungs), 22 TB treatment type categorized as new or retreatment; referral source (Facility or community), GeneXpert access, Nutritional assessment conducted using mid-upper arm circumference (MUAC) and documented in the Health Unit TB register as red (<11.5 cm), indicating severe acute malnutrition, yellow (11.5–12.5 cm), indicating moderate acute malnutrition, and green (>12.5 cm), meaning well nourished. The individuals whose MUAC was not taken or not registered were categorized as having no nutritional assessment done.
The primary outcome
The primary outcome was TB treatment Success, computed as the sum of treatment completion and cure. “No” Treatment Success Computed as Death, lost to follow up, and non-evaluation according to the WHO criteria. 23
Operation definitions
Operation definitions as per the WHO guidelines 2013 and the national TB leprosy program.23,24
Drug-susceptible TB
A BC or CD case of TB without evidence of infection with strains resistant to rifampicin and isoniazid, as determined by WHO rapid molecular tests (such as GeneXpert MTB/RIF) or phenotypic drug susceptibility testing.
Treatment completion
A TB patient who completed treatment without evidence of failure, but with no record to show that sputum smear or culture results in the last month of treatment and on at least one previous occasion were negative, either because tests were not done or because results are unavailable.
Cured
A pulmonary TB patient with bacteriologically confirmed TB at the beginning of treatment who was smear- or culture-negative in the last month of treatment and on at least one previous occasion. Negative smear microscopy at the end of treatment and on at least one previous follow-up test at 2 or 5 months.
Treatment failure
A TB patient whose sputum smear or culture remained smear-positive after 5 months of treatment.
Defaulted
A patient who interrupted their treatment for two consecutive months or more.
Died
A TB patient who dies for any reason before starting or during treatment.
Lost to follow-up
A TB patient who did not start treatment or who completed more than 1 month of treatment and was interrupted for two consecutive months or more. 24
Not evaluated
TB patient for whom no treatment outcome is assigned.
Data analysis
The collected data were then entered into a Microsoft Excel sheet and exported to Stata Statistical Software: Release 15 (StataCorp LLC, College Station, TX, USA), where it was cleaned, validated, and analyzed. 25
Descriptive statistics for the study participants were summarized as proportions for categorical variables, means and standard deviations for continuous variables with a normal distribution, and medians with interquartile ranges (IQRs) for continuous variables with skewed distributions. The association between treatment success and categorical variables was determined using the Chi-square test, and Student’s t-test was used for numerical variables. Significant overall findings from the Chi-square were further explored with post-hoc pairwise tests using a Bonferroni-adjusted correction to control the family-wise error rate. To determine factors associated with treatment success, we performed a modified Poisson regression analysis, estimating adjusted prevalence ratios (aPR) with robust standard errors using the variance-covariance matrix of the estimators method. Modified Poisson regression was chosen over logistic regression because our outcome had a prevalence greater than 10%, where the odds ratio from logistic regression can overestimate the degree of association compared to relative risks. 26 All variables with a p < 0.2 at bivariate analysis were included in the multivariable model. A p < 0.05 was considered statistically significant.
Results
Recruitment of individuals in the study
Of 1062 records of individuals with TB assessed, 53 were excluded, including 12 who had no TB treatment categories, 4 had no treatment outcomes, 4 had incomplete age and gender, 15 had unknown HIV status, and 18 had rifampicin resistance. A total of 1009 individuals with TB were included in the final analysis (Figure 1).

Study profile for treatment outcome analysis for patients with drug-susceptible tuberculosis in the Teso region, Uganda.
Social demographic characteristics of study participants
The median age of all the study individuals was 45 years (IQR 28–60). Of the participants, 9.5% (n = 96) were aged less than 15, while 48.1% (n = 485) were aged 15–49 years. Most of the individuals, 52.9% (n = 534), were male, and 54.5% (n = 550) were BC TB. The majority, 90.4% (n = 912), were newly diagnosed with TB, and 82.2% (n = 829) had been assessed for nutrition status using age-specific MUAC tapes. A total of 68.0% (n = 686) had accessed GeneXpert, while 69.9% (n = 705) were diagnosed with TB at the facility. Overall, 30.9% (n = 312) were HIV positive, and 69.1% (n = 697) were HIV negative, as shown in Table 1.
Sociodemographic characteristics of individuals with susceptible TB in the Teso region, Uganda, between October 2021 and December 2023.
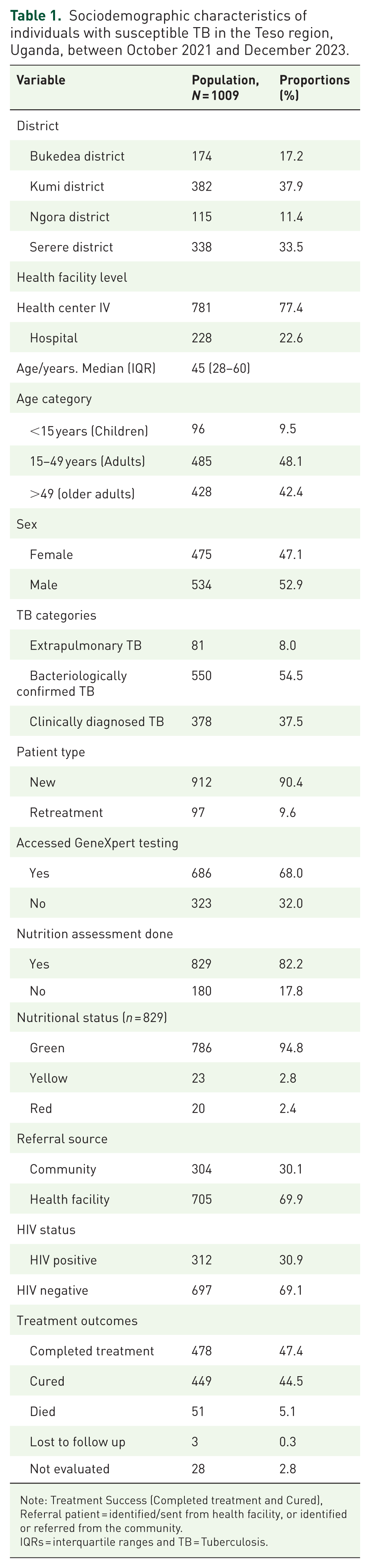
Note: Treatment Success (Completed treatment and Cured), Referral patient = identified/sent from health facility, or identified or referred from the community.
IQRs = interquartile ranges and TB = Tuberculosis.
TB treatment outcomes
The overall TSR was 91.9% (n = 927) (95% CI: 90.0%–93.4%), including a treatment completion of 47.4% (n = 478), and a cure rate of 44.5% (n = 449). Unsuccessful outcomes included death at (5.1%, n = 51), lost to follow-up (0.3%, n = 3), and not evaluated at (2.8%, n = 28).
In bivariate analyses, the TB categories (Bacteriologically Confirmed TB, Extrapulmonary TB, and Clinically Diagnosed TB) and HIV status were statistically significantly associated with treatment success, as shown in Table 2.
Bivariate analysis of treatment success and associated factors among individuals with susceptible TB in the Teso region, Uganda, 2021–2023.

Note: ** = Statistically significant p-values, HIV = human immune deficiency virus; TB = tuberculosis.
In this study, the treat TSR was higher among individuals who were HIV negative as compared to those living with HIV (93.8% vs 87.5%).
The treatment success was highest among individuals with clinically diagnosed TB (93.9%), followed by those with bacteriologically confirmed TB (91.5%), and lowest in those with extrapulmonary TB (85.2%). This variation was statistically significant, and post-hoc pairwise comparisons with Bonferroni correction showed that Extrapulmonary TB had a significantly lower TSR than the Clinically Diagnosed TB (Table 3).
Post hoc pairwise comparisons of treatment success with Bonferroni correction.

Bonferroni-adjusted significance level = 0.05/3 = 0.0167.
Note: BC = Bacteriologically confirmed TB, CD = clinically diagnosed TB, EPTB = Extrapulmonary TB and TB = tuberculosis.
Although not significant, the treatment success was higher among individuals who had accessed Gene Xpert testing for timely diagnosis as compared to those who had not (93% vs 89.5%)
In multivariable analyses, as shown in Table 4, the factors associated with treatment success were age >49, being female, and living with HIV. The prevalence of treatment success among those aged >49 years was 0.95-fold lower compared to the children aged <15 years (aPR = 0.95, 95% CI: 0.89–0.99, p = 0.042). The prevalence of treatment success was 1.04-fold higher among females as compared to males (aPR = 1.04, 95% CI: 1.002–1.07, p = 0.041). The prevalence of treatment success was significantly lower among the HIV positive individuals as compared to the HIV negative (aPR = 0.93, 95% CI: 0.88–0.98, p = 0.008).
Factors associated with treatment success rate among drug-susceptible TB in the Teso region, Uganda, 2021–2023.

Note: **indicates statistically significant p values (p < 0.05).
Discussion
This study assessed treatment success and associated factors among drug-susceptible TB individuals in the Teso region. We found that older age ( greater than 49) and HIV coinfection were associated with lower treatment success, while being female was associated with a higher treatment success. These findings highlight the need for targeted interventions to improve treatment outcomes, such as intensified adherence counseling among people living with HIV and other age and gender specific treatment outcome improvement packages.
The treatment success rate in this study was 91.9%, meeting the WHO target of 90% set by the World Health Organization and adopted by the Ministry of Health, Uganda.1,2 This aligns with studies from Ethiopia, where the TSR ranged from 89% to 92%,27–29 but is higher than the rates reported in other studies done in Uganda (80.1%–82.9%),13,21,30 South Africa, Mozambique, and Nigeria (53%–89.8%).31–33 These disparities may stem from differences in sample size and the sociodemographic characteristics of these studies. This high TSR observed in our study may reflect the intensified use of quality improvement approaches, community follow-up activities by cough monitors and health workers, and the use of line lists for monitoring treatment retention to ensure that clients are followed up in a timely manner to complete TB treatment.
The treatment success rates among those aged >49 years were lower than those among young individuals aged < 15 years. This finding aligns with similar studies from Uganda, which reported that older individuals had twice the odds of poor TB treatment.13,34 These results are also consistent with findings in Zambia and India.35,36 and other Eastern African countries, including Kenya 37 and Tanzania. 38 The consistency of these findings across low- and middle-income countries highlights several age-related vulnerabilities, including a lack of peer support for treatment adherence, a higher burden of comorbidities such as hypertension, and an increased risk of anti-TB drug-related renal and hepatotoxicity side effects, which can lead to low treatment adherence rates and lower TSR.15,39 These findings underscore the need for national programs to develop geriatric-sensitive TB care models, including community approaches such as assigning community health workers to provide psychosocial support for older TB patients and community directly observed therapy to ensure treatment completion.
In this study, females had higher treatment success than males. This is similar to the results from India, where females had 1.41 times higher likelihood of successful treatment. 40 This may be explained by women’s better health-seeking behavior, such as being more likely to seek health care services, being enrolled under direct observed therapy (DOT), and adhering to treatment. In addition, in vitro studies suggest that the female sex hormone modulates and improves the immune response, leading to better outcomes.41–44 This pattern is not universal, as contrasting findings from Karamoja in Uganda45,46 reported higher treatment success among males. This difference shows that gender is a social determinant of TB outcomes that can be mediated by sociocultural norms, economic opportunities, and accessibility of health services.
In this study, the TB-HIV coinfection was 30.9%, comparable to rates in Brazil and Ghana (30%–44%)47,48 but higher than those in Japan, Ethiopia, and China (3.5% and 6.8%),49–51 likely due to regional variations.
The significantly lower TSR among people living with HIV in our study is a critical challenge across several regions.52,53 This aligns with other African countries such as Ethiopia. 52 and Nigeria 31 Asian Countries like Uzbekistan, 54 India, Malaysia,12,55 and America.56,57 This lower treatment success may be attributed to pill burden, the drug interaction between the anti-TB drugs and the antiretroviral therapy (ART), HIV-related immune suppression, which increases the progression of latent TB, slow response to TB treatment, and consequently, low treatment outcomes.15,58–61 To improve the suboptimal TB outcomes in TB/HIV coinfected individuals, there is a need for health systems to offer services using an integrated, patient-centered care model, including early screening, bidirectional ART, TB preventive therapy, and joint management of side effects or complications.
Limitations and strengths
The study had several limitations, including the use of secondary data, which is often associated with incompleteness and missing variables, including HIV status. Furthermore, the generalizability of our findings may be limited to similar rural settings, as the study was conducted in selected rural facilities. We also did not explore the contribution of socioeconomic factors such as income and education to treatment success. However, the study has notable strengths, including its large sample size and the inclusion of several public health facilities (a hospital and Health Center IVs), which enhanced participant diversity, enhancing the generalizability of the findings.
Conclusion
This study found that being aged >49 years and living with HIV were associated with poor treatment success, while being female was associated with better treatment outcomes. There is a need to strengthen the integration of TB and HIV management in terms of timely TB screening and initiation of eligible patients on available TB preventive therapy to avert incident TB among people living with HIV (PLHIV), and also improve the treatment outcomes. There is a need to innovate and implement both community and facility-based TB differentiated models of care, like DOT targeting people at high risk of poor outcomes, such as males and older adults, to achieve the goal of the End TB strategy. Additional research is needed to understand the interplay of patient-level social and behavioral characteristics and health system determinants on TB treatment success.
Supplemental Material
sj-doc-1-tai-10.1177_20499361251405334 – Supplemental material for Treatment success and associated factors among drug-susceptible tuberculosis patients in Teso region, Uganda: a retrospective study
Supplemental material, sj-doc-1-tai-10.1177_20499361251405334 for Treatment success and associated factors among drug-susceptible tuberculosis patients in Teso region, Uganda: a retrospective study by Saadick Mugerwa Ssentongo, Bonniface Oryokot, Ronald Opito, Gerald Ochieng, Peter Sekiranda, Baker Bakashaba and Kenneth Mugisha in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
The authors would like to acknowledge the support rendered by the facility in charge of Atutur Hospital, Kumi HC IV, Serere Health Center IV, Bukedea Health Center IV, and Ngora HC IV for their support during the data collection process.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.