
Abstract
Background:
South Africa has the third-highest adult prevalence rate globally, with women comprising 64% of cases. Despite the accessibility of pre-exposure prophylaxis (PrEP), its adoption among women, particularly young women, remains alarmingly low.
Objectives:
The objective of this initial investigation is to explore factors influencing the intentions of South African women to use PrEP, focusing on sociodemographic factors, HIV sexual risk behaviours and involvement in transactional sex.
Design:
The research utilised an exploratory design employing surveys.
Methods:
Surveys were conducted in 2015 with 64 women aged 19–49 residing in the Eastern Cape Province of South Africa. The data were analysed using descriptive statistics and multiple logistic regression. Data analysis was performed using SPSS 28.0 and R.
Results:
Younger women, compared to older women, were more inclined to intend to use PrEP (p = 0.056, χ2 = 3.655, df = 1, OR 0.92, CI (0.89, 0.99)). Women who used a condom were less likely to intend to use PrEP (p = 0.082, χ2 = 3.025, df = 1, OR 0.29, CI (0.09, 1.14)). Respondents who engaged in transactional sex were more inclined to intend to use PrEP (p = 0.007, χ2 = 7.330, df = 1, OR 6.86, CI (1.82, 31.0)).
Conclusion:
Addressing factors that impact South African women’s intentions to use PrEP is crucial for enhancing the adoption of PrEP among this population.
Plain language summary
South Africa has one of the highest rates of HIV in the world, especially among women, who make up 64% of adults living with HIV in the country. Even though there is a medicine called PrEP that can prevent HIV, not many South African women, especially young women, use it. This study looks at what influences South African women’s decisions to use PrEP, focusing on things like age, sexual behaviour, and involvement in transactional sex. A survey was conducted with 64 women in the Eastern Cape province. The results showed that younger women are more likely to intend to use PrEP than older women. Women who use condoms are less likely to intend to use PrEP. Those involved in transactional sex are more likely to intend to use PrEP. Understanding and addressing factors that affect South African women’s intentions to use PrEP is essential to increase its use among them.
Introduction
South Africa has one of the highest numbers of people living with HIV globally and the third-highest adult HIV prevalence worldwide. 1 Women in South Africa, constituting 64% of the adults living with HIV, are disproportionately affected. 2 Despite the availability of pre-exposure prophylaxis (PrEP) with a daily oral pill of emtricitabine (FTC)/tenofovir (TDF), its uptake among South African women, particularly adolescent girls and young women, remains unacceptably low.3,4 For instance, Donnell et al. 5 conducted a study in 2018 across four countries—Eswatini, Kenya, South Africa and Zambia—and found that out of 3756 women still being followed up after on-site PrEP access began, only 27 (<1%) had initiated PrEP. Similarly, in 2021, Beesham et al. 6 interviewed 13 women from Durban, South Africa, who started oral PrEP during the ECHO trial. Of these, 46% (six women) accessed PrEP after the trial, but 38% (five women) later discontinued it, whilst 54% (seven women) did not access PrEP at all.
In 2016, the country initiated nationwide support for PrEP scale-up, with guidelines updated in 2020, identifying adolescent and young women as a high-risk population.7,8 Numerous studies have explored factors having a positive influence on PrEP uptake among women in Southern Africa, revealing issues such as multiple partners, perceived HIV risk, being in serodiscordant relationships and the sexual partner’s infidelity.9–12 For example, a qualitative study conducted between 2016 and 2018 by Scorgie and associates of South African and Zimbabwe women found their perceptions of HIV risk and their partner’s personal qualities and behaviour (especially relating to infidelity) were associated with their PrEP uptake. 12 A study published in 2023 exploring motivators for oral PrEP among a sample comprised largely of Black African women (76%) residing in the eThekwini municipality of KwaZulu-Natal, South Africa, conducted by Basda, Reddy and Haffejee found that sexual partner’s infidelity was among the reasons for women to use PrEP. 11
Despite PrEP’s potential as an effective HIV prevention tool, significant gaps remain in understanding the factors that drive uptake among South African women. A key area that needs further exploration is the determinants influencing women’s intentions to use PrEP. According to theories like the theory of planned behaviour, intention is considered a significant predictor of behaviour, reflecting motivation, attitude and perceived control.13,14 One of the few studies on intentions and PrEP uptake among women was conducted by Chittamuru et al. as part of the Just4Us Study (2019–2020) in the USA. Chittamuru et al.’s study explored the relationship between HIV stigma, PrEP stigma and women’s intentions to use PrEP, finding that higher PrEP stigma correlated with lower intentions. 15 However, this study did not examine the influence of sociodemographic variables on intentions to use PrEP. In a related study, Teitelman and colleagues, as part of the Just4Us Study (2017–2018), investigated sociodemographic variables in relation to PrEP intention. They discovered that only Hispanic ethnicity exhibited a significant association in this context. 16 In addition, they observed that positive attitudes towards the benefits of PrEP and perceptions and the belief that others would support their PrEP use were significantly linked to their intentions to use PrEP.
An investigation by Scott and associates conducted from 2017 to 2020 explored multilevel factors that impact the intentions to initiate PrEP among women. 17 The results of this study indicated that favourable attitudes towards PrEP and increased self-efficacy at the individual level, along with the perception of future utilisation of PrEP among peers, perceived low fear or stigma at the community level, and discussing PrEP with a healthcare provider, were all positively associated with women’s intentions to initiate PrEP. Whilst these studies conducted in the USA provide valuable insights, it remains uncertain whether these findings align with the experiences of women in South Africa. The gaps in understanding the determinants of PrEP uptake among South African women arise from the intricate interplay of sociodemographic factors, HIV sexual risk behaviours as well as lifestyle behaviours such as transactional sex.
Sociodemographic factors, such as age, economic status and education, significantly influence individual and population health behaviours. In particular, age is a crucial determinant in shaping health intentions and behaviours.18,19 Understanding the nuanced relationship between age and intentions to use PrEP is essential for tailoring effective interventions that resonate with diverse age groups. For instance, a study by Drallmeier et al., drawing from the Optum de-identified electronic health record data set (2010–2018) in the USA, found that patients who were aged 60 years had significantly lower rates of PrEP initiation compared to those aged 18–29. 20 Likewise, a study by Ohiomoba et al., 21 drawing from data collected by the Kenyan Pamoja Community Based Organization’s DREAMS Initiative, indicated that young Kenyan women who initiated PrEP from 2017 to 2019 discontinued PrEP use earlier than their older counterparts.
Studies have evidenced that deprivation significantly influences health behaviour.22,23 Whilst poverty refers to insufficient resources to fulfil basic needs, deprivation measures quantify the extent of those unmet needs. 24 Utilising data from the 2011 LoveLife survey conducted in four South African provinces, KwaZulu-Natal, Mpumalanga, Eastern Cape and Gauteng—Kamndaya and collaborators examined the impact of material deprivation on HIV sexual risk behaviour among youth. 25 The results indicated a significant association between material deprivation and elevated odds of engaging in high sexual risk-taking among both young women and men. Additionally, the study identified financial difficulty, serving as a proxy for deprivation, as the most prominent factor influencing high sexual risk-taking behaviour in young women. Furthermore, Greif’s study, based on the 2000 Nairobi Cross-Sectional Slum Survey (NCSS), highlighted that housing and food deprivation strongly influenced sexual risk behaviours, such as multiple sexual partnerships and transactional sex, in an impoverished area in Nairobi. 26 To the best of our knowledge, no existing studies are exploring the relationship between deprivation and the acceptance of PrEP in the context of HIV sexual risk behaviours.
Various sexual risk behaviours are key predictors of HIV exposure. Engaging in condomless sex greatly increases the risk, emphasising the critical role of consistent and correct condom use as a crucial preventive measure. Moreover, consuming alcohol before sexual activity can impair judgement and decision-making, increasing the chances of contracting HIV and other sexually transmitted infections.27–29 Likewise, substance use before sex also diminishes judgement, further raising the likelihood of risky behaviour.30–32 A new assessment of the Just4Us Study, investigating different types of substance use in the preceding 3 months with PrEP intention, discovered that women who used hallucinogens, prescription opioids or engaged in polydrug use demonstrated significantly higher intentions to use PrEP compared to their counterparts. 33
In low- and middle-income countries such as South Africa, women often face systemic challenges such as poverty, lack of job opportunities and limited access to education. These factors can contribute to some women feeling compelled to engage in transactional sex as a means of economic survival. Transactional sex and sex work are related concepts but have distinct characteristics. Engaging in sex work typically involves a more structured trade of sexual services for money or goods and may be a deliberate profession for certain individuals. On the other hand, transactional sex often underscores a less formal and occasionally coercive nature of the exchange, frequently prompted by urgent economic or survival requirements for necessities like food and shelter. Numerous studies examine factors influencing PrEP uptake among women who are sex workers.34,35 However, studies of factors influencing PrEP uptake among women who engage in transactional sex are sparse. Chimbindi et al. conducted a study between 2017 and 2018 among young women who sell sex in a rural area of KwaZulu-Natal, South Africa, to examine their awareness of PrEP. 36 The results indicated that most women lacked awareness of PrEP, though there was no effort made to explore the factors associated with their awareness or their intentions to use PrEP. However, a study conducted by Bien-Gund et al. (2017–2018) among women at high risk of HIV infection in Kenya revealed that engaging in transactional sex within the past 12 months was positively correlated with PrEP utilisation. 37 Furthermore, a qualitative investigation conducted between 2016 and 2017 led by Camlin et al. 38 aimed at comprehending the demand for PrEP among young adults in rural Kenya and Uganda found that women perceived PrEP as a tool to manage their risk in the context of transactional sex.
The motivation for this study stems from the existing gaps in understanding the determinants of PrEP uptake among South African women, particularly in relation to the complex interplay of sociodemographic factors, HIV sexual risk behaviours and lifestyle behaviours such as transactional sex. Whilst sociodemographic factors such as age, economic status and education significantly influence health behaviours, the specific relationship between these factors and the intentions to use PrEP remains underexplored. Age, for instance, has been shown to shape health-related intentions, yet its impact on PrEP uptake across different age groups in South Africa is poorly understood. Additionally, while deprivation is known to affect health behaviours, no studies to date have examined how it influences the acceptance of PrEP in the context of HIV sexual risk. In South Africa, where women often face systematic challenges such as poverty and limited job opportunities, some are compelled to engage in transactional sex, yet research on how these circumstances affect PrEP uptake is sparse. This study aims to address these knowledge gaps by exploring the connections between sociodemographic factors, HIV sexual risk behaviours, transactional sex and women’s intentions to utilise PrEP, ultimately contributing to more effective HIV prevention strategies for South African women.
Methods
This (H13-RTI-HIV-002) study received review and approval from the Institutional Review Board of Nelson Mandela University. These exploratory data were collected through surveys conducted in 2015. The participants were women from New Brighton and Kwazakhele townships, located approximately 8 km north of Gqeberha/Port Elizabeth in the Eastern Cape Province of South Africa. Potential participants were recruited from health clinics and through word-of-mouth. They were invited to participate in a survey aimed at understanding their feelings, beliefs and behaviours concerning their health, as well as a new medication that could help prevent HIV infection.
Setting
The Eastern Cape is the poorest province in terms of average monthly household expenditure among the nine provinces in the country. 39 About 96% of the population is ethnic African or Black, with the majority living at or below the poverty level (64%). 40 New Brighton and Kwazakhele townships are characterised by informal development, with underdeveloped road structures, limited public and recreational spaces and a lack of social services. 41
Recruitment
Research assistants – Black South African women fluent in isiXhosa and English – recruited potential participants from community health clinics and through word of mouth. They obtained informed consent from volunteer participants and administered the survey. Eligible women were aged 18–55 and self-reported as HIV-negative. Potential participants were invited to complete a survey aimed at understanding women’s feelings, beliefs and behaviours regarding their health and a new medication that could help prevent people from becoming infected with HIV.
Data collection
Women who agreed to participate completed informed consent. After providing written informed consent, participants received a 5-min presentation on women and PrEP, which provided basic information about PrEP (e.g. what PrEP is, why take PrEP, reasons women take PrEP, and the health effects of PrEP). Questions raised by the women were addressed after the presentation. Surveys were administered in a group setting at a local community centre. Surveys were conducted in English. Research staff provided translations in isiXhosa when needed. Data were collected using pencil and paper questionnaires. Surveys lasted approximately 90 min. Participants received 25R (about 2 US$) for completing the survey.
The final questionnaire included the following variables (Table 1): sociodemographic questions, social deprivation, HIV sexual risk behaviours, including drinking and using drugs before sex, transactional sex and intentions to use PrEP. The questionnaire included predefined options for responses.
Variables and questions.

PrEP, pre-exposure prophylaxis.
Data analysis
We calculated descriptive statistics for sociodemographic and HIV sexual risk behaviours. One participant was identified as being 16 years old and was therefore excluded from the data analysis in accordance with ethical guidelines. Exploratory factor analysis was used to examine the underlying relationships among variables assessing deprivation. Nine questions were used to capture various dimensions of deprivation, and the analysis revealed two distinct clusters of variables: household infrastructure and household material deprivation. Table 1 lists the questions for household infrastructure deprivation and household material deprivation. Reliability coefficients for household infrastructure deprivation and household material deprivation are α = 0.82 and 0.75, respectively. Correlations using Spearman’s rho were used to examine the relationships between the independent variables and PrEP intentions (Table 3).
Chi-square statistics and t-tests were used to further understand the relationship between sociodemographics, HIV risk behaviours, transactional sex and intentions to use PrEP. Chi-square statistics were used to assess the bivariate independence of categorical variables, condom usage, and transactional sex choice, whilst a t-test was used to assess the significance of the quantitative variable age as a factor for respondents’ choice to use PrEP. Data analysis to examine the relationship between the predictor and dependent variables included three categorical and one continuous variable. The categorical variables were the respondent’s intention to use PrEP, the dependent variable in the study, the respondent’s use of a condom and their engagement in transactional sex. A binary coding system was used for the categorical variables, whilst the fourth variable, age, was assessed as a continuous variable. A multiple logistical regression model evaluated respondents’ intentions to use PrEP in relation to condom use and transactional sex, which were selected based on the significance levels from the previously mentioned chi-square and t-test inferential results. A binomial link function was employed, and the analysis was conducted using R version 4.2.2 (2022-10-31).
For this analysis, the dataset was reduced to 50 respondents due to 14 cases with missing data. During the initial analysis, we included the variable “alcohol use” as an independent variable in assessing the intention to use PrEP. However, this variable was removed because it was found to be statistically insignificant (p-value = 0.484, OR = 0.28, 7.22) and removed from the final analysis. Based on the initial exploratory analysis, age, condom use and transactional sex choice were included in the model-building process. Given the exploratory design of this study, all statistical tests were evaluated using a significance level of 0.01. The fitted logistic model was:

Variables in the logistic regression model are defined as follows:


Results
As indicated in Table 2, the sample predominantly consisted of young adult women, with the majority (66%) unemployed. Three-fifths of the participants had completed either a high school or post-secondary level of education. Forty per cent of the participants reported an extremely low monthly income. On a scale of 1.00–2.00, the average scores for household infrastructure and household material deprivation were 1.49 and 1.26, respectively. These results indicate that, on average, most respondents experienced relatively lower levels of deprivation. Regarding HIV sexual risk behaviours, 31% of the women reported not using condoms the last time they had sex. Thirty-nine per cent of the women reported sometimes consuming alcohol before having sex. Thirty-four per cent reported engaging in transactional sex. Forty-two per cent of the women reported an intention to use PrEP.
Characteristics of the total sample (n = 64).
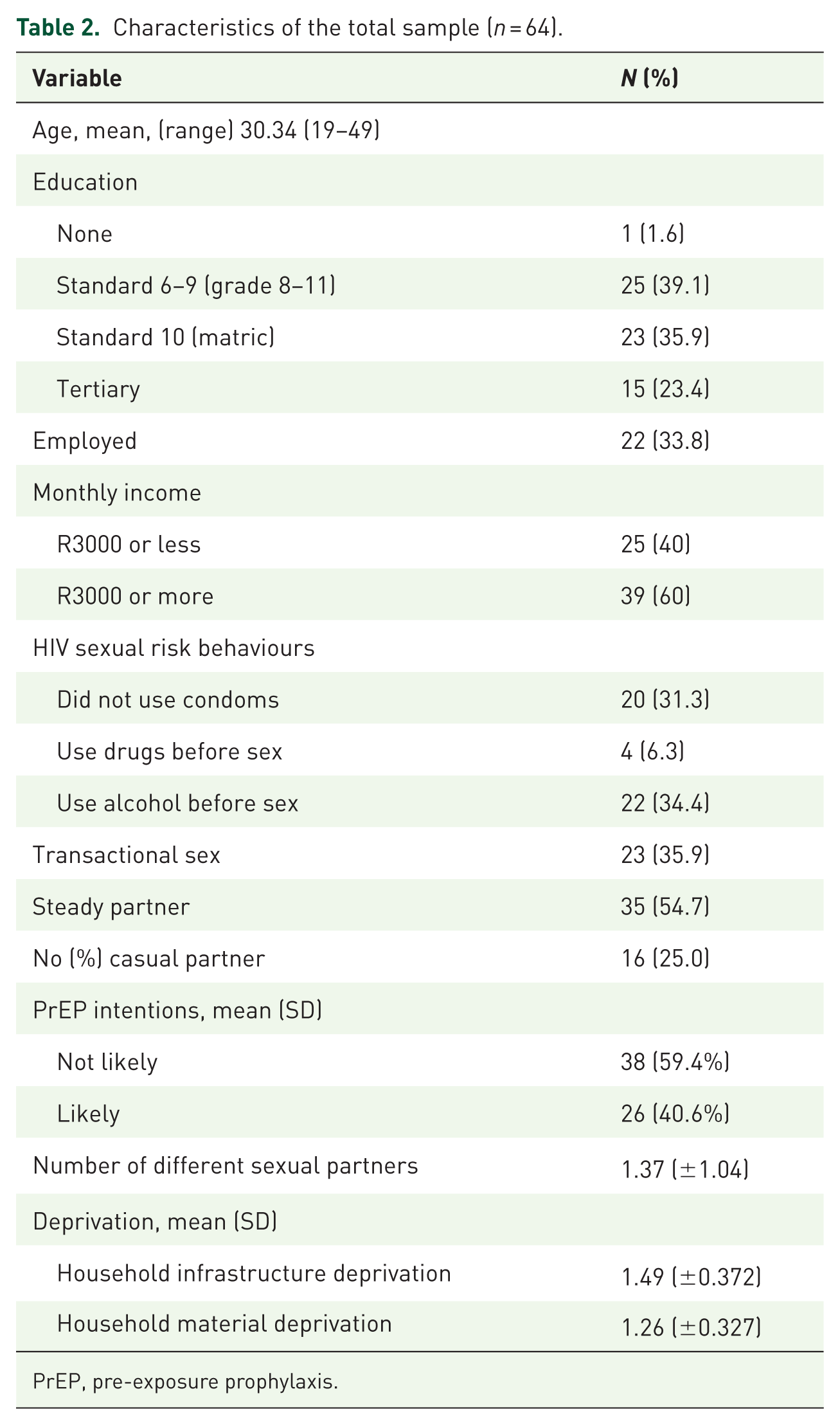
PrEP, pre-exposure prophylaxis.
As shown in Table 3, a perfect negative correlation was observed between drinking before sex and drug use before sex (ρ = –1.000, p < 0.01, n = 60). This result reflects a consistent inverse pattern in a small subset of the sample, where participants who reported one behaviour did not report the other. Given the small sample size and potential for restricted response variability, this finding should be interpreted with caution. Bivariate analysis revealed condom use (χ2 = 6.727, df = 2. p = 0.035), drinking before sex (χ2 = 5.28, df = 1, p = 0.022) and transactional sex (χ2 = 8.21, p = 0.004) were statistically associated with PrEP intentions. Among women who sometimes drink alcohol before a sexual encounter, 60.9% indicated they were likely to use PrEP. In contrast, 30.6% of women who reported never drinking alcohol before a sexual encounter stated that they were likely to use PrEP. Even though there was a significant association between drinking before sex and PrEP Intentions, this variable was excluded from the multiple regression analysis due to missing data. The inclusion of this variable resulted in a reduction of the sample size to 46 observations.
Spearman’s rho correlations matrix between demographic, behavioural and socioeconomic factors and PrEP intentions.

Due to the small sample size (n = 64), analyses employed an exploratory alpha level of p < 0.10 to minimise the risk of Type II error. Values are Spearman’s rho (ρ).
p < 0.10 (two-tailed). **p < 0.05 (two-tailed).
Significant level for PrEP intentions and condom use is shown in Table 3 underline.
PrEP, pre-exposure prophylaxis.
Shown in Table 4 is the distribution of intentions to use PrEP across different HIV sexual risk behaviours. As shown in Table 5, transactional sex was highly significant with a p-value < 0.007, whilst variables age and condom use were significant at the 10% level, with p-values between 5% and 10%. Based on the significance level, all three independent variables were considered important predictors of PrEP intention. Assuming all variables are fixed, the results imply that the intention to use PrEP declines as age increases. Hence, women of younger age were more prone to expressing an intention to use PrEP. Respondents who used condoms were less likely to express an intention to use PrEP, suggesting that those who did not use condoms were more likely to have an intention to use PrEP. Lastly, respondents involved in transactional sex showed a higher inclination to express an intention to use PrEP. In contrast, those not engaging in transactional sex were less likely to have such an intention.
Association between HIV sexual risk behaviours and intentions to use PrEP n = 64.

PrEP, pre-exposure prophylaxis.
Effect of age, condom use and transactional sex on intentions to use PrEP (n = 50).

CI, confidence interval; PrEP, pre-exposure prophylaxis.
Discussion
This exploratory study aimed to examine the determinants of intentions to use PrEP among women in South Africa, focusing on the relationship between sociodemographic factors, sexual risk behaviours, transactional sex, and PrEP intentions. By understanding these factors, the study sought to contribute to more effective HIV prevention strategies tailored to South African women. The findings provide insights into how age, condom use and transactional sex influence women’s intentions to use PrEP. To our knowledge, this is one of the few studies to examine transactional sex among women who were not sex workers.
In 2015, when the data for this study were collected, PrEP was not yet available through public health channels in South Africa. At the time, little was known about how women might perceive or respond to PrEP as a future HIV prevention method. Although our analysis was conducted in a pre-rollout context, the findings remain highly relevant, particularly when considered through the lens of behavioural intention theory, which identifies intention as a significant predictor of future behaviour. Our data, thus, provide a valuable baseline perspective on which populations may have been most receptive to PrEP, even before it became widely accessible.
The time lag between data collection and current implementation presents a unique opportunity to reflect on the intention–behaviour gap. While the women in this study—especially younger women and those engaged in transactional sex—expressed high levels of intent to use PrEP, more recent research suggests that actual uptake and sustained adherence remain low, particularly among the same demographic groups. Structural and social barriers such as stigma, lack of partner support, inadequate knowledge and limited health system access have all been identified as key obstacles to translating intention into action.3,42–44
By situating our findings within this broader trajectory, we highlight the importance of not only identifying who is likely to be motivated to use PrEP but also ensuring that interventions are designed to help convert intention into sustained use. This further validates the need for multi-level, contextually appropriate approaches that address both motivational and structural determinants of PrEP uptake.
The results demonstrated that younger women were more likely to express intentions to use PrEP. This is consistent with previous research 20 and may reflect a generational shift in attitudes towards sexual health, with younger women more open to biomedical prevention tools. However, the discrepancy between high intentions and low actual uptake among young women emphasises the need for targeted interventions that address both access and socio-cultural challenges. Stigma, healthcare navigation barriers, and relationship power dynamics may all inhibit young women from acting on their intentions to use PrEP. This highlights the need for age-tailored programming that improves access, builds trust in health services, and supports PrEP use within relational contexts.
While no direct relationship between deprivation and PrEP intentions was found in this study, the exploration of deprivation and its impact on sexual risk behaviours adds a valuable dimension to our understanding of HIV prevention in low-resource settings. Since 2015, economic vulnerability has remained a key driver of risk behaviour in South Africa.24,45,46 Previous studies, such as Kamndaya et al., 25 have demonstrated links between material deprivation and sexual risk-taking. Although our analysis did not detect a direct association between deprivation (as measured through household infrastructure and material deprivation) and PrEP intentions, this may be due to limitations in sample size and the localised context. The findings also suggest that deprivation does not operate uniformly as a risk factor for all individuals; some demonstrate resilience and engage in health-seeking behaviours even in resource-constrained settings. These nuances underline the importance of future research to better understand how deprivation intersects with HIV prevention choices and the necessity of addressing underlying economic vulnerabilities to support long-term public health strategies.
Another key objective of this study was to assess how sexual risk behaviours, such as condom use, relate to intentions to use PrEP. The results showed that women who reported not using condoms during their last sexual encounter were more likely to report intentions to use PrEP. This aligns with previous research showing that inconsistent condom use is associated with increased interest in biomedical prevention tools.47,48 For many women, PrEP represents a practical, autonomous alternative to partner-dependent protection methods, particularly in situations where negotiating condom use is difficult or unsafe. PrEP’s discreet and self-managed nature may make it more acceptable and feasible for women seeking control over their HIV prevention without needing partner cooperation.
Participants were recruited from public health clinics where they were seeking routine care. The demographic and behavioural profiles of the women (e.g. employment status, relationship patterns) were consistent with a general clinic-attending population rather than individuals engaged in informal sex work. While some overlap may exist between transactional sex and sex work in other contexts, in this study, we intentionally used a broader behavioural measure without applying identity-based labels.
In exploring the relationship between transactional sex and PrEP, this study makes a novel contribution by focusing on women who engage in transactional sex but do not identify as sex workers. Consistent with previous findings, 37 the study found that these women were more likely to express intentions to use PrEP. This is particularly noteworthy given that prior research has often focused on formal sex workers, whereas this study addresses a population often overlooked in PrEP research. Women involved in transactional sex—often for economic survival but not within the formal sex work sector—may recognise their heightened vulnerability to HIV and be more motivated to adopt self-protective behaviours like PrEP.
To effectively intervene in this population, it is essential to implement non-stigmatising, community-based delivery models that allow women to access PrEP without needing to disclose involvement in transactional relationships. Furthermore, PrEP interventions should be integrated with broader empowerment and livelihood programs, including job training, financial literacy training, and youth mentorship programs. This approach can reduce economic reliance on transactional partnerships over time while simultaneously affirming women’s agency and autonomy in choosing to protect their health. Programs like DREAM 21 or “Sisters with a Voice” 49 have demonstrated the benefits of bundling PrEP with social and economic supports. Additionally, relationship-focused risk navigation tools and digital self-assessment aids may help women in transactional partnerships make informed decisions without increasing their interpersonal risk. While upstream strategies addressing poverty and gender inequality are critical in the long term, intermediate supports like conditional cash transfers or housing assistance can offer immediate buffers against economic precarity while increasing the feasibility of consistent PrEP use.
In summary, this study’s findings highlight important pre-rollout predictors of PrEP interest and shed light on the complexity of translating intention into behaviour in real-world settings. Revisiting these findings in light of the current PrEP landscape in South Africa underscores the continued need for context-sensitive, multi-level interventions that centre women’s lived realities and equip them with the tools to make and sustain health-promoting choices.
Limitations
This study had several limitations. Although data from 2015 may raise questions about its applicability to current contexts, the study’s findings offer lasting value due to the persistence of many of the socioeconomic and behavioural challenges South African women face today. One limitation is that certain aspects of the HIV prevention landscape, such as the availability and awareness of PrEP, have evolved since the time of data collection. However, the core determinants of health behaviours—such as age, condom use and engagement in transactional sex—remain critical factors that influence PrEP intentions, making these findings still relevant. The small sample size limited the statistical power of the analysis, particularly in detecting associations between some variables. The perfect negative correlation between drinking before sex and drug use before sex may be attributable to the small sample size and restricted response patterns. Such extreme values should be interpreted cautiously and warrant further examination in larger, more diverse samples. The cross-sectional design also prevents making causal inferences. Generalisability should not be assumed to extend to women residing in other parts of South Africa.
Additionally, the use of self-reported data may have introduced bias, particularly with respect to sensitive behaviours like condom use, alcohol consumption and transactional sex. The exclusion of alcohol consumption before sex from the regression model due to missing data is another limitation, as it was found to be associated with PrEP intentions in the bivariate analysis. Including this variable could have provided further insights into the factors influencing PrEP intentions. Given the self-selected nature of the participants in this study, namely those able to attend a clinic, there is reason for caution in interpreting these findings. The data were collected using pencil and paper questionnaires, which can potentially introduce bias. Yet, the benefits of paper surveys stem from their independence from tablets or mobile devices, addressing a prevalent technological resource limitation in low- and middle-income countries such as South Africa.
Despite its limitations, this study has several implications for HIV prevention efforts in South Africa. This study is notable for being one of the few that investigate the relationship between sociodemographic factors, HIV risk behaviours, transactional sex and intentions to use PrEP among women in a South African context. It provides a unique and relevant understanding of the dynamics of PrEP intentions within this vulnerable population. Age-specific interventions that focus on promoting PrEP among younger women could be highly effective, as younger women were more likely to express an intention to use PrEP. Addressing the socioeconomic challenges that drive transactional sex is critical for enhancing PrEP uptake among this vulnerable population. The preliminary nature of the findings underscores the need for more extensive research with larger samples to either confirm or extend the results.
Conclusion
This study provides key insights into the sociodemographic and behavioural factors influencing PrEP intentions among South African women. Age, condom use and transactional sex were identified as significant predictors of PrEP intentions, suggesting that younger women and those engaged in higher-risk sexual behaviours are more likely to consider PrEP as an HIV prevention tool. The results highlight the significance of the impact of transactional sex on the intentions of South African women to adopt PrEP. It is recommended to expand the focus on transactional sex beyond sex workers to encompass a wider demographic of women. Specifically, it is crucial to give increased attention to addressing the vulnerabilities of young women, a population disproportionately susceptible to HIV. Factors such as alcohol consumption before sex and the absence of condom use should be considered for the development and implementation of effective HIV prevention interventions. Further research is needed to explore the role of deprivation in shaping PrEP intentions and to develop comprehensive interventions that address the economic vulnerability contributing to HIV risk among South African women.
Footnotes
Acknowledgements
The authors extend their gratitude to Dr Nceba Nyembezi for his invaluable contributions to cleaning and coding, Ms Anri Van der Merwe for her assistance with data storage, the nurses at the recruitment clinics and the women who participated in this study.