
Abstract
Uncomplicated urinary tract infections (uUTIs/acute cystitis) carry a substantial physical and psychological burden that negatively impacts patient quality-of-life, particularly for those who experience recurrent infection. A disconnect can exist between patients and healthcare professionals (HCPs), leading to poor patient-HCP communication, suboptimal treatment, and feelings of frustration and anxiety for many patients. The views of four patient authors with recurrent UTI or chronic uUTI and two HCP authors managing patients with this disease are presented in this Patient Perspectives article. While HCPs recognize both the physical and mental impacts of recurrent uUTIs, most HCPs focus on relieving a patient’s physical symptoms, often resulting in the psychological impact being overlooked. Inadequate testing, lengthy diagnostic procedures, and treatment failure caused by antimicrobial resistance (AMR) further exacerbate the problems associated with uUTIs, limiting the effectiveness of treatment options for patients. Enhancing education for patients and HCPs on AMR and the reasons why treatment failure might occur could improve the discourse between HCPs and patients, leading to improvements in the overall patient experience.
Plain language summary
Urinary tract infections (UTIs or bladder infections) can cause feelings of physical pain, discomfort, frustration and anxiety. Recurrent UTIs are those infections that keep returning after treatment (⩾3 or more infections every year or two infections within 6 months) while in chronic UTI, infection is continuous, and symptoms persist despite treatment. This article explores the perspectives of four patients and two healthcare providers on the care of people who experience UTIs.
Methods used to diagnose UTIs can lead to delays in receiving appropriate medication. Another issue faced is that the bacteria that cause infections can become resistant to medicine, making the medicines less effective. People with recurrent UTIs often feel their healthcare providers overlook the impact of UTIs on their mental health. Poor communication between patients and healthcare providers can lead to misunderstandings as to why treatments do not always work, and infections keep returning.
There is a need for improved care for people with recurrent UTIs and better communication between patients and healthcare providers.
Keywords
Introduction
Uncomplicated urinary tract infections (uUTIs; also known as acute cystitis or bladder infections) occur in 50%–60% of adult women during their lifetime. 1 Of these, 30%–44% will experience a second infection within 6 months of the first infection. 2 uUTIs are defined as short-term, irregular, or recurrent (meaning they keep coming back) infections that occur in non-pregnant women who have no known functional problems within the urinary tract or other pre-existing diseases. 3 uUTIs impact patient quality-of-life (QoL), triggering negative emotions such as frustration, helplessness, and anxiety. 4 This emotional impact may be particularly strong in patients whose treatment fails due to antimicrobial resistance (AMR). 4 Patient views on their experiences of uUTI are reported in the literature; however, the patient-reported experience of recurrent uUTI has received comparatively little focus, 5 with even fewer studies exploring patient views alongside healthcare professionals (HCPs) involved in uUTI care. Qualitative studies to date featuring the views of both patients with uUTI and HCPs have often explored shared decision-making, but not complementing and contrasting perspectives of both groups.6–8
In this Patient Perspectives article, patient and HCP co-authors discuss the similarities and differences in the patient/HCP perspective of the impact and management of recurrent uUTI. Key topics for discussion in this article were identified as of interest to the field following four GSK-led, non-promotional patient council meetings and were further discussed by the authors. This article presents the perspectives of patients and HCPs separately under identified themes, providing a set of complementary narratives discussing issues that are important to patients with uUTI and the HCPs delivering care to these patients.
The author group for this article includes: three female patients with recurrent UTI and one female patient with chronic uUTI (symptoms persist despite treatment 9 ) (aged 40–46 years), and two HCPs (one urologist and one pharmacist). Summaries of these perspectives are presented in Figure 1, alongside selected quotes from the patient and HCP authors of this article. Table 1 provides a summary of patient- and HCP-reported barriers to effective uUTI diagnosis and management. See Supplemental Table 1 for a glossary of terms.

Patient and HCP perspectives with select patient quotes, organized by theme.
Patient- and HCP-reported barriers to effective uUTI diagnosis and management.
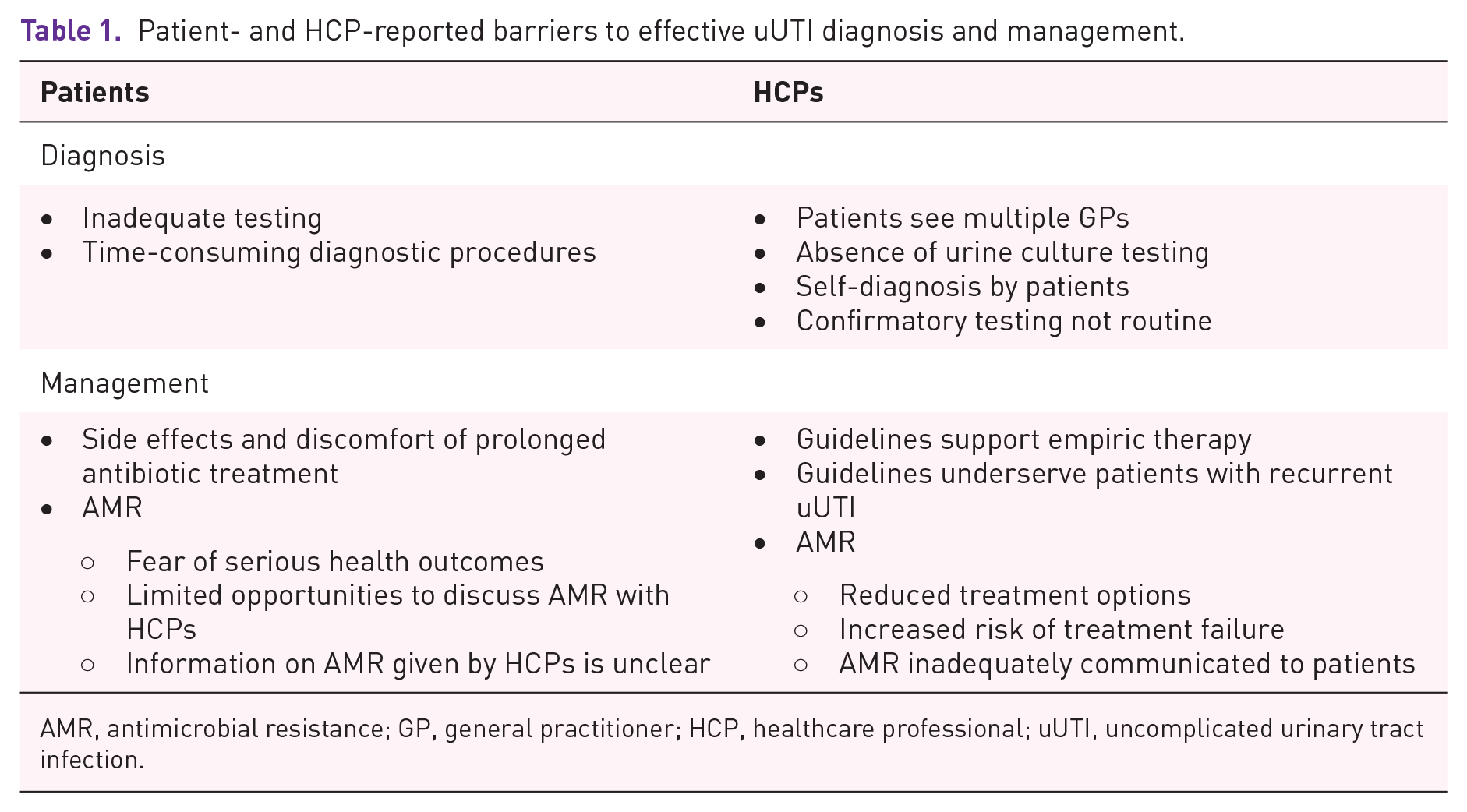
AMR, antimicrobial resistance; GP, general practitioner; HCP, healthcare professional; uUTI, uncomplicated urinary tract infection.
Author discussion: Question development and response collection
Questions for patient/HCP author consideration, used to guide this Patient Perspectives article, were developed using patient insights gained from four GSK-led, non-promotional patient council meetings. Patients were recruited via existing patient advocacy networks and support groups, with the aim of including individuals with lived experience of recurrent or chronic UTIs who were willing to contribute to structured discussion forums. Inclusion criteria included: age ⩾18 years, a self-reported history of ⩾2 uUTIs in the past 6 months or ⩾3 in the past year (or continuous symptoms for chronic UTI), and a willingness to participate in non-promotional insight-gathering sessions. Exclusion criteria included current involvement in interventional clinical studies or employment in the pharmaceutical industry. Patients were not remunerated for publication contributions but were reimbursed for time during the initial council meetings in accordance with industry-standard fair market value principles. Insights were gathered during four 2-h virtual patient council meetings conducted between 2022 and 2023. Meetings were facilitated by independent qualitative researchers using semi-structured guides. Notes and verbatim excerpts were collected and synthesized thematically by GSK medical staff and shared with patient and HCP authors for review and validation. Themes emerging from these discussions were used to guide the structure of this manuscript and to formulate the reflective responses from both patient and HCP authors.
Key factors for consideration
Living with uUTI
Patient perspective
Women with uUTI experience a range of challenging physical symptoms including pain, urgent and frequent urination, and bladder/abdominal/vaginal discomfort or pressure. Physical symptoms vary between individuals and can have a negative impact on mental health. 4
The physical and emotional impact of uUTI can reduce the ability of patients to work and partake in social or family life, leading to social isolation. Sexual activities and intimacy can also be affected, with abstinence due to uUTI leading to feelings of frustration and anxiety. 4 Moreover, evidence indicates that recurrent uUTI impairs sexual function and causes sexual distress in approximately 80% of patients.10,11 Unsurprisingly, this leads to significantly lower levels of sexual satisfaction among patients and has substantial negative effects on intimate relationships.12,13 People who have not experienced a uUTI often do not understand its impact, and many patients find it difficult to discuss with others due to its personal nature. However, family members and friends are generally supportive.
Recurrence is a common feature of uUTIs, demonstrating that some patients experience ⩾3 infections every year or two infections within 6 months. 3 Patients often feel anxiety, fear, and dread of future episodes, which worsens the impact on QoL. Frequent episodes can affect family, social, and professional relationships as well as travel, with many choosing not to travel altogether. Many patients blame themselves and worry that they have done something wrong to cause another infection. 4 Some patients proactively look to protect themselves from future infections.
HCP perspective
HCPs note that many patients with uUTI experience lethargy, fatigue, and general unwellness, with elderly patients often presenting with confusion and delirium. Due to time constraints and the need to see many patients, during consultations, HCPs usually focus on treating uUTIs without exploring the emotional, social, or sexual impact experienced by patients. Recent evidence supports the importance of assessing sexual health and function in patients with recurrent uUTI and integrating this into the overall management strategy. 12 This is crucial given the association between recurrent uUTI and sexual dysfunction,10–13 in addition to some patients reporting feeling as though they are being ignored, or that the detrimental impact of uUTI on their relationships is underestimated by their HCP. 14 Similarly, HCPs often do not explore the impact of uUTI on family and social relationships, despite recognizing the importance of support from family and friends. As noted by patients, the frequency of uUTIs varies between individuals. Therefore, HCPs should consider whether new episodes are a continuation of a previous infection or a new infection altogether.
Diagnosis and management
Patient perspective
uUTI treatment may not always be effective due to inadequate testing and time-consuming diagnostic processes.15–17 When prescribed, urine culture tests can guide antibiotic decisions and reassure patients that an appropriate treatment will be provided. However, as it can take up to 3 days to obtain the results, symptoms may worsen between the initial test and the start of treatment.
Prolonged antibiotic use can lead to side effects and discomfort. Treatment failure due to AMR can also occur, causing infections to persist and an increased risk of complications. This can be frustrating for patients, especially if they have previously had successful antibiotic treatment. Patients may seek further medical advice or guidance on uUTI prevention (e.g., from specialist websites). Some patients look for supplementary treatments (including cranberry products, D-mannose, and herbal medicines) to take alongside their antibiotic prescription or at the start of an infection.
The possibility of AMR can lead to fear of serious health outcomes, such as sepsis or even death. Opportunities for patients to discuss their fears of AMR can be limited, and HCPs may not provide clear information.
HCP perspective
Conversations between patients with recurrent uUTI and HCPs typically occur within primary care (e.g., general practitioners). In this setting, patients often see multiple general practitioners and may not have the opportunity to discuss concerns. They are also often treated without urine culture testing. Self-diagnosis is common, and resources may not allow for further investigations. Confirmatory diagnostic testing (such as microscopy, culture, and susceptibility) supports targeted treatment of infection but is not routinely used and is often saved for patients with complex needs. Treatment guidelines, used to inform antibacterial treatment in primary and secondary care, are designed for empirical therapy. This means patients are typically not tested, and their treatment is decided based on their previous experience with a suspected illness and its associated treatment. 18 Guidelines may therefore underserve patients with recurrent uUTI and could be improved.
The increasing burden of AMR 19 presents a significant challenge for HCPs. The problem is twofold: the rise in patients with AMR-related uUTIs and a dwindling number of effective treatment options. As the number of patients with AMR-related uUTI increases, the therapeutic options available to treat these infections caused by AMR bacteria decrease, increasing the likelihood of treatment failure. 20 From a public health perspective, uUTI treatment failure can result in morbidity and mortality, with a high financial impact. 20 Antimicrobial stewardship programs are essential in the fight against AMR. These programs promote the optimal use (antibiotic selection, dose, and duration) and prevention of misuse of antibiotics.20,21 As a result, stewardship programs can improve patient outcomes, control AMR and its spread, and safeguard public health.20,21 Antimicrobial stewardship is especially crucial in urology and the treatment of UTI, 21 for which three-quarters of patients report receiving an antibiotic prescription. 22
The increased risk of treatment failure associated with AMR is often not adequately explained to patients. This lack of understanding can leave them feeling powerless and unprepared if their treatment fails. Improving communication between patients and HCPs is crucial. By educating both groups on the risks and consequences of AMR, patients can be empowered to take an active role in their care. This education should include clear guidance on what to do if symptoms persist despite completing antibiotic treatment. Effective communication and patient education are key components of better managing AMR and fostering patient empowerment.
HCP factors
Patient perspective
Many HCPs lack an adequate understanding of the physical, mental, and emotional impact of recurrent and chronic uUTIs. 4 Advice from HCPs can also be outdated, pushing patients to look for information from other sources (such as specialist websites). Furthermore, information on holistic approaches to care is lacking. To improve the quality of care and treatment received, it can be helpful to see an HCP who has substantial knowledge and experience with treating recurrent uUTI.
HCP perspective
To improve the care provided by HCPs, specialist UTI clinics should be more widely established that allow longer consultation time for targeted management of patients with uUTIs. Existing specialist UTI clinics at centers in the UK and other European countries, for example, centralize care under one roof to help resolve the often fragmented care that some patients experience. 23 These clinics typically adopt multidisciplinary and patient-centered approaches and aim to improve patient outcomes and reduce the burden of UTI care on healthcare systems; in doing so, such clinics offer real-world guidance for how specialist UTI clinics can be successfully established. 23
In everyday practice, HCPs should aim to supply patients with all the resources they need to manage their symptoms and prevent future episodes. HCPs may not fully appreciate the physical, mental, and emotional impact of recurrent uUTIs. Continuing medical education programs are therefore important to improve HCP awareness and understanding of the broader impact of uUTIs for patients. Existing programs commonly focus on the diagnosis and treatment of uUTIs, while education on the substantial mental and emotional impacts of uUTI is comparatively overlooked and is an important unmet need. Furthermore, there is a need to better educate HCPs about evidence-based holistic and non-antibiotic approaches to treatment.
Tools designed to measure QoL could be used during consultations to support meaningful discussions about the full impact of uUTI and could provide further insights into the overall effectiveness of treatment for patients.
Recommendations
Patient recommendations
There is a need for better treatments that are more tolerable in patients with uUTI, as side effects are frustrating and potentially serious for patients. Treatment failure is equally as frustrating for patients, and diagnostic testing is often time-consuming and inadequate. Patients want the antibiotics they are prescribed to resolve their symptoms of uUTI first time and as quickly as possible. Updated testing and diagnostic processes could improve diagnostic accuracy and ensure that effective treatment is prescribed in a timely manner. Such advances are on the horizon with the ongoing development of accessible, rapid, and accurate diagnostic tests. 24
It is this article’s patient author view that information from HCPs on holistic treatments is lacking, leading to patients searching for alternate remedies/preventative measures on online websites. HCPs should consider providing advice on holistic approaches to care that improve the gut microbiome and strengthen the immune system. Patients should also be guided on how to lessen the risk of future uUTI episodes (e.g., by practicing self-care after sex). Altogether, this could enable patients to achieve a sense of bodily control, helping to improve their confidence in managing their uUTI.
HCP recommendations
Expert consensus on patient care in uUTI 18 has emphasized the urgent need for rapid point-of-care diagnostic tests that can identify the causative uropathogen and provide information on antimicrobial susceptibility to predict patient response to treatment. Progress in the development of such tests, which can provide results in minutes to hours, has recently been reviewed 24 ; these include portable, particle counter instruments, 25 PCR-based methods,26,27 and enhanced disk diffusion methods. 28 Rapid Diagnostic tests could enable HCPs to identify the correct antibiotic treatment at initial patient contact, thereby reducing overprescription and inappropriate use of antibiotics and improving patient care.
The increased risk of treatment failure associated with AMR is often inadequately explained to patients, leading to a lack of understanding that can leave them feeling powerless and unprepared if their treatment fails. HCPs should thoroughly describe the actions for patients to take if symptoms persist or worsen, which will improve patient empowerment and confidence.
The emotional impact that uUTIs have on patients can be equally as significant as the physical symptoms 4 ; however, these are rarely discussed between patients and HCPs. Education on the emotional symptoms of uUTIs and the development of new uUTI-specific QoL assessment tools could help HCPs to understand the true impact of uUTIs on patients.
Study strengths, limitations, and future research
In this Patient Perspectives article, with patient and HCP authors represented in the author byline, we report the views of patients with both recurrent and chronic uUTIs, which is important for understanding the holistic impact of the condition. In addition, the perspectives reported here include themes and challenges that both patients and HCPs in the UK face, helping to form a well-rounded view of the condition. Lastly, this article promotes greater awareness of uUTIs and contributes to the available literature. Our work has some limitations, such as the inclusion of only four patients and two HCPs coming from the UK (with one exception in the patient group). Indeed, as three of the patients and both HCPs were from the UK, our work inevitably reflects mostly UK-based perspectives. As such, we acknowledge that the small sample size and focus on one country may limit the generalizability of the perspectives to patients and clinical practice in other countries. Even so, many of the perspectives raised by the patients centered on key issues of living with uUTI: symptom burden, emotional impacts, treatment side effects, and AMR. These issues are likely to be of concern for most patients, irrespective of country of residence. We also acknowledge and recognize as a potential limitation the involvement of industry in this work, most notably the patient council meetings upon which the current article is based. The perspectives and recommendations presented herein, however, are those of the six non-industry-affiliated authors. Our discussion should be interpreted considering the inherent limitations of a small, UK-based sample.
Future work in this vein should consider consulting more patients for their views, to strengthen any viewpoint highlighted. In addition, including HCPs from different geographical locations and specialities would improve the diversity and robustness of the HCP perspectives.
Conclusion
Patient empowerment and personalized care could be facilitated by improved HCP knowledge of the physical and emotional impact of uUTIs. A better understanding of the full patient experience and an increased focus on the impact of AMR could enable improved discussions and shared decision-making between patients and HCPs.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251355384 – Supplemental material for Understanding patient and healthcare provider perspectives of uncomplicated urinary tract infection: patient journey, disease management, and the impact of antimicrobial resistance
Supplemental material, sj-docx-1-tai-10.1177_20499361251355384 for Understanding patient and healthcare provider perspectives of uncomplicated urinary tract infection: patient journey, disease management, and the impact of antimicrobial resistance by Bhaskar Somani, Maria Sanchez-Grande, Aida Idrissi Kaitouni, Abbe Whittle, Miriam Thun-Winter, Amina Benkiran, Aruni Mulgirigama and Stephen Hughes in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
Medical writing support for the development of this manuscript, under the guidance of the authors, was provided by Rosie Robson, MSc, and Niamh Southern, MPhil, of Ashfield MedComms, an Inizio company, and funded by GSK.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.