
Abstract
Introduction:
Skin abscesses are one of the most common infections among people who inject drugs (PWID).
Objective:
To examine factors associated with the frequency of abscesses in the previous 3 months among PWID.
Design:
We conducted a cross-sectional analysis of baseline data from a prospective longitudinal cohort of PWID.
Methods:
Between April 2021 and November 2022, PWID were recruited from community settings in Los Angeles, CA, and Denver, CO. Participants completed an interview covering sociodemographic, drug use, and related risk behaviors. Participants were asked if they had abscesses in the last 3 months. Those reporting “yes” quantified the number of abscesses. Responses were classified as None, 1, or 2 or more. We used bivariate analysis and multi-nominal regression to examine factors associated with the frequency of abscesses.
Results:
Among participants (n = 472), 62% reported no abscesses, 16% reported 1 abscess, and 22% reported 2+ abscesses in the last 3 months. Compared to participants with no abscess, 1 abscess was associated with receiving buprenorphine treatment (adjusted odds ratio (AOR) = 3.27; 95% CI = 1.58, 6.78), being injected by another person (AOR = 3.06; 95% CI = 1.72, 5.45), injecting 3+ times a day (as compared to less than daily, AOR = 2.92; 95% CI = 1.28, 6.65), licking syringe prior to injection (AOR = 1.96; 95% CI = 1.03, 3.74), and being Latino (AOR = 0.25; 95% CI = 0.12, 0.54). Having 2+ abscess was associated with daily heroin use (AOR = 2.35; 95% CI = 1.26, 4.39), being injected by another person (AOR = 1.92; 95% CI = 1.16, 3.18), daily methamphetamines use (0.50; 95% CI = 0.30, 0.83) and those reporting 10+ rushed injection (as compared to none, AOR = 1.85, 95% CI = 1.04, 3.29) in the last 3 months.
Conclusion:
Our findings underscore a multi-level approach to reducing abscesses in this population. Increased education around safe injection practices, institutional interventions—that is, addressing healthcare stigmatization and expanding clinical harm reduction—as well as structural interventions (safe supply, overdose prevention programs, housing) should be considered.
Keywords
Introduction
Skin and soft tissue infections (SSTIs) include abscess and cellulitis, and hospitalizations for the same are increasing rapidly across the United States among people with substance use disorders.1–3 Abscesses are a localized infection containing pus or infected fluid. They can occur nearly anywhere in the body, but among people who inject drugs (PWID) are most commonly found in the skin and soft tissues. While injecting, bacteria and other pathogens that may be on contaminated injection equipment or commensal on the skin enter the body when the skin barrier is broken. 4 Potential contributors to the development of acute infections such as abscess among PWID are tissue damage, chronic inflammation, and impaired circulation that may lead to increased bacterial growth and have been tied to repeat injections via nonsterile equipment.5,6 Given the increases in injection drug use in the US and the inadequate availability of harm reduction services, skin abscesses have become one of the most common acute infectious complications among PWID, with a reported lifetime incidence upward of 60%.5,7–11 A recent study among a national sample of PWID showed that 42.9% had a history of abscesses. 7 Data show that PWID often delay seeking clinical treatment anywhere between 2 days and 2 weeks for abscesses. 12 Additionally, PWID often attempt to self-treat due to societal stigma, limited access to treatment, and high costs associated with treatment.4,10,13–15 In San Francisco, a study found that 48% of PWID with abscesses had not sought treatment for at least one abscess, 27% had self-treated through incision and drainage, and 16% had resorted to antibiotics that were prescribed to another individual. 16 PWID self-treat at high rates, through lancing and sometimes by shared antibiotics.4,12 These factors, including delays in seeking medical care, self-treatment, and associated complications, contribute to longer hospital stays and more invasive procedures, ultimately leading to higher healthcare costs associated with treating.4,12
In 2001, 37.5%–58% of PWID were hospitalized due to SSTIs, amounting to a financial cost exceeding $190 million.17,18 According to data from the Centers for Disease Control and Prevention in 2013, cutaneous (skin-related) abscesses led to approximately 2% of visits to the emergency department. Moreover, 0.9% of all emergency department patients required incision and drainage procedures. 19 Between 1993 and 2010, hospitalization rates for community-onset SSTI doubled from 4 to 9 per 100,000 individuals nationwide, pertinently in the 20–40 age range. 20
Much of the data in this area is examined and interpreted on an individual level as injection behaviors associated with SSTIs, which include reusing syringes, sharing non-sterile injection equipment, injection by someone else, environmental contamination of injection equipment, and water sources for drug preparation.21–26 Practices such as high frequency injecting, groin injecting, skin popping and muscling, and repeated injections into the same area can lead to local bacterial infections and even chronic wounds among PWID.16,21,26–31 Murphy and colleagues reported that injecting a combination of cocaine and heroin, also known as “speedball,” may increase the risk of abscess due to soft-tissue ischemia. 28 Additionally, PWID experiencing opioid withdrawal symptoms often inject more frequently to manage withdrawal symptoms, leading to an increased risk of abscesses. 30
The vast majority of extant literature in this area measures abscess occurrence using binary measures, that is, lifetime prevalence or current infection.8,10,16,32 To address this gap, in this analysis, we examined factors associated with the frequency of abscesses (self-reported number of abscesses) in the previous 3 months among PWID experiencing major structural vulnerabilities in a community recruited sample from Los Angeles, CA, and Denver, CO. In addition to examining individual-level factors, we sought to illuminate structural drivers by contextualizing our findings, wherever possible, within the built environment and broader socio-structural and political configurations that exacerbate what is seen as “risk behavior.”33–36 Accordingly, we discuss structural and institutional pathways for intervention. 37
Methods
Sampling and recruitment
To examine the potential impact of cannabis legalization of cannabis and opioid use among PWID, we recruited PWID from community settings and service organizations (i.e., syringe service sites, shower, bathroom, and laundry facilities for unhoused people, and other community locations) in Denver, Colorado, and Los Angeles, California between April 2021 and November 2022. These sites were selected for convenience and to permit data collection in outdoor settings to minimize COVID-19 transmission risk. To be eligible for the study, participants had to report being 18 years of age or older, any opioid use, and self-reported drug injection within the past 30 days, which was confirmed by visual inspection of injection sites. 38 After providing informed consent, participants answered questions on demographic and socioeconomic characteristics, drug use patterns, injection-related risk behaviors, drug treatment involvement, health items, among other items in a one-on-one computer-assisted personal interview using the Questionnaire Development System (Nova Research, Bethesda, MD). Participants received $20 for completing this interview. This cross-sectional analysis included data from 472 PWID, representing 223 from Los Angeles and 249 from Denver. All study procedures were reviewed and approved by the Institutional Review Board at the University of Southern California. 39 Authors referenced the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines to generate this manuscript (Supplemental Material 1). 40
Study measures
In this study, we examined risk factors for skin abscesses. Participants who responded, “yes” to the “In the last 3 months, have you had an abscess related to injection drug use, even if it did not “come to a head,” drain, or require treatment of any kind?” were next asked how many abscesses they have had in the last 3 months, that is, frequency of abscesses. We used these questions to construct three groups for our outcome variable, namely: no abscesses, 1 abscess, and 2 or more.
Our questionnaire was informed by previous research (Supplemental Material 2: Questionnaire).29,30,41 These items included sharing of syringes and other drug paraphernalia (cookers, cotton, and rinse/mix water) as well as new items such as licking syringes or needles prior to injection, wiping the injection site with salvia, and re-using cotton. We used the following items to collect information for these new behaviors. For needle licking prior to injection, we asked, “In the last 3 months, have you licked the needle or wetted or moisten a needle with saliva/spit prior to injecting with a needle?” And if they responded “yes,” participants were asked “how often did you wet or moisten a needle with saliva/spit before injecting yourself?” Response options were on a five-point scale anchored by “None” and “All.” We used this latter item to construct a bivariate classification where none and those participants who report no needle licking to the prior item as “No” and those reporting some to all as “Yes.” We also asked, “In the last 3 months, have you used saliva/spit to wipe or “clean” a spot on your body that you then injected into?” Response options were “Yes” or “No.” Lastly, we asked, “In the last 3 months, have you re-used your own cotton or filter? That is, saved it and then re-wetted it to get residual drug from it or used it again because an unused cotton or filter was not available.” Response options were “Yes” or “No.” in the last 3 months, and other behaviors previously associated with bacterial infections among PWID. We asked, “In the last 3 months, how many times have you rushed your injection because you were concerned someone would see or interrupt you?” We categorized responses as “None,” “1 to 9 times,” and “10 to more times.”
Potential characteristics were selected based on biological plausibility (i.e., licking a needle prior to injection could introduce bacteria from a person’s mouth into their bloodstream), and prior empirical findings.8,16,28,31 We considered the following variables as potential covariates: gender (male or not male), race/ethnicity (white, Black, Latinx, Native American, Asian or Pacific Islander, mixed), age (<30, 30–39, 40–49, or 50 or older), relationship status (single, married, living as married), sexual partners (types—steady, casual, paid), and sexual orientation (heterosexual, bisexual, gay, or lesbian). Socioeconomic characteristics examined included monthly income (<$1000, $1001 to $1400, or 1401 to $2100, or $2101 or more), unstably housed (yes or no), income sources (job, unemployment, veteran’s benefits, welfare, disability, social security, spouse, family, friends, recycling, panhandling, and illegal or possibly illegal sources), and education (high school graduate or equivalent).
Drug use measures included injection frequency, drugs by type and frequency of use (daily or not), and years of injection. Injection frequency was the sum of self-reported injection times with the following drugs: cocaine, crack cocaine, methamphetamine, heroin, speedball (admixture of cocaine and heroin), goofball (admixture of heroin and methamphetamine), and non-medical use of prescription opiates, stimulants, sedatives, tranquilizers, methadone, and buprenorphine in the last 3 months. We converted the injection frequency in the last 3 months into a categorical variable with the following classifications: less than daily use (<89 injections), once or twice a day (90–269 injections), and three or more times a day (≥270). Years of injection were calculated by subtracting current age from age at first injection and categorized as <10 years, 10–19 years, and 20 or more years.
We also considered factors that have been associated with health outcomes among PWID including contact with security guards, police and other criminal justice involvement (e.g., parole and probation),42,43 receiving and giving assistance with injection, 44 syringe coverage and syringe reuse,45,46 withdrawal symptoms from opioids, methamphetamines and cocaine,47,48 rushed injection,49,50 involvement in substance use treatment (e.g., current enrollment and enrollment in the last 3 months in methadone, buprenorphine, residential, and outpatient treatment), and any mental health disorder diagnosis.
Statistical analysis
We conducted a primary analysis of data collected from the baseline survey of the larger longitudinal cohort. After descriptive analysis, we conducted bivariate analyses to determine factors associated at the p < 0.05 level with no abscesses, 1 abscess, and 2 or more abscesses (Table 1) using chi-square tests for categorical variables, and t-tests and Spearman’s Rho for continuous variables. We considered the variables listed above in the domains of demographics, socioeconomic characteristics, displacement, and substance use behaviors as potential correlates and confounders. Variables significant in bivariate analyses were then assessed for collinearity within domains using Pearson correlation coefficients. Collinear variables (Pearson correlation coefficient > 0.30) were included in the final analyses based on the strength of association with the dependent variable, whereby variables with weaker associations were dropped from multivariate analyses.
Selected sample characteristics by self-reported abscess frequency among PWID in Los Angeles, CA, and Denver, CO in the last 3 months (n = 472).
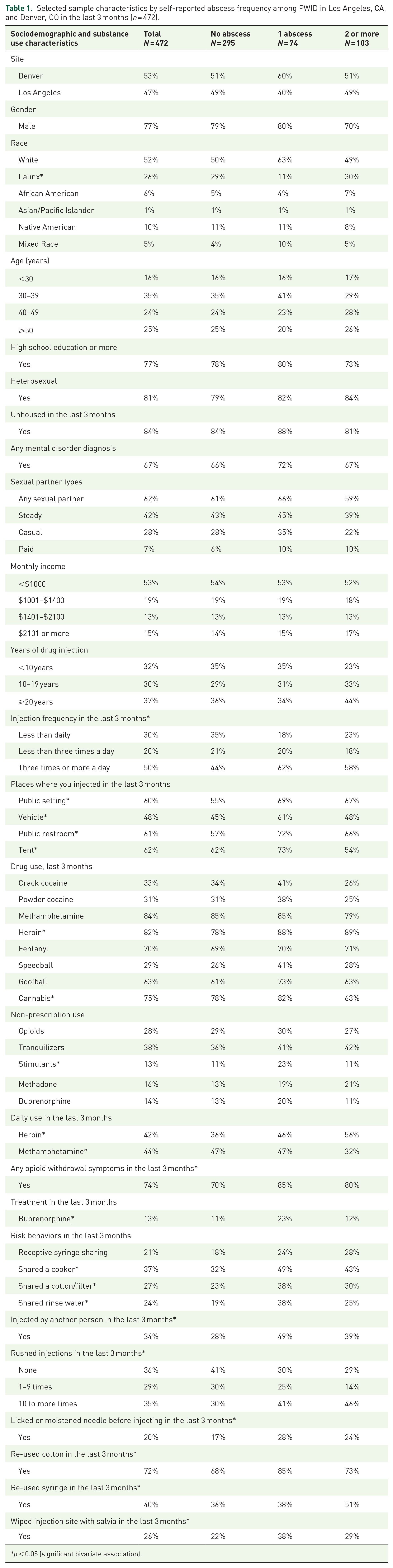
p < 0.05 (significant bivariate association).
We used multinomial logistic regression to calculate odds ratios for 1 abscess or 2 or more abscesses (with no abscess as the referent) while controlling for confounding. Variables not significant in multivariate analyses (p < 0.05) at each step were removed from models with the exception of recruitment city. For models, adjusted odds ratio (AOR) and 95% confidence intervals (CIs) were estimated. All analyses were performed using SPSS, Version 25 (IBM Corp., Armonk, N.Y., USA).
Results
Sample characteristics consisted of 472 participants (249 from Denver and 223 from Los Angeles) of which 77% were male, 52% were White, 26% were Latinx, 10% were Native American and 6% were Black, a plurality were between the ages of 30 and 39 (35%), followed by 25% of whom were over 50 years old, and 24% who were between 40 and 49 years old (Table 1). The majority were unstably housed (84%), high school educated (77%), and low income (53% had monthly income of less than $1000). In terms of drug use patterns, 70% reported daily injection, 44% reported daily methamphetamine use, and 42% reported daily heroin use.
Among participants (n = 472), 62% reported no abscesses, 16% reported 1 abscess, and 22% reported 2 or more abscesses in the last 3 months. Of the participants who reported at least 1 abscess, mean number of abscesses was 3.94 (standard deviation = 8.35), median = 2 (interquartile range = 1, 4). In bivariate analysis (Table 1), we found significant associations between frequency of abscesses and demographic (Latino ethnicity), drug use practices (past 3 month use of heroin, along with daily use of heroin and methamphetamines), injection frequency, opioid withdrawal symptoms, buprenorphine treatment, public injection, sharing cookers, cotton, and filters, being injected by another person, and rushed injection frequency. Of note were significant bivariate associations between frequency of abscesses injecting in vehicles and tents, using cannabis and non-prescription stimulants in the last 3 months.
In multinomial logistic regression (Table 2), we found that as compared to participants with no recent abscesses (62%), having 1 abscess was associated with receiving buprenorphine treatment (AOR = 3.27; 95% CI = 1.58, 6.78), being injected by another person (AOR = 3.06; 95% CI = 1.72, 5.45), injecting 3 or more times a day (as compared to less than daily, AOR = 2.92; 95% CI = 1.28, 6.65), licking needle prior to injection (AOR = 1.96; 95% CI = 1.03, 3.74), and being Latino (AOR = 0.25; 95% CI = 0.12, 0.54). Compared to individuals with no recent abscesses, reporting 2 or more abscess was associated with daily heroin use (AOR = 2.35; 95% CI = 1.26, 4.39), being injected by another person (AOR = 1.92; 95% CI = 1.16, 3.18), daily methamphetamine use (0.50; 95% CI = 0.30, 0.83) and those reporting 10 or more rushed injections (as compared to none, AOR = 1.85, 95% CI = 1.04, 3.29) in the last 3 months.
Multinomial regression analysis of frequency of abscesses among people who inject drugs, Los Angeles, CA and Denver, CO, 2021–22, (n = 472).

Discussion
In this study, we found several individual and behavioral factors that were associated with skin abscesses. That said, “risk behaviors” are often used to perpetuate blame, institutionalize stigma, and attempt to discipline people who use drugs via biomedical techniques. 36 In this article, we aimed to contextualize our findings, where possible, within the built environment in an effort to shift the unit of examination away from individuals and onto sociopolitical arrangements that exacerbate risks and vulnerabilities. As such, we emphasize the role of structural interventions that alter these arrangements to reduce health risks associated with abscess among PWID.34,37,42
A total of 38% of this community recruited sample of PWID in Los Angeles, CA, reported at least one abscess in the last 3 months. We found that compared to people who reported no rushed injections, people who reported 10 or more rushed injections in the past 3 months had significantly higher odds of having 2 or more abscesses. Ethnographic data show that the risk of injecting in public settings leads to a shift in attention toward environmental threats rather than the injection practice itself.37,51 For instance, in one study, PWID described adequate knowledge about SSTI but emphasize socio-structural contexts that restrict their ability to enact known mitigation steps. 13 In that study, PWID emphasized how housing instability, fear of violent victimization such as being assaulted in an abandoned building led to public injection as well as other concerns like rapid onset of withdrawal and police. 13
In our data, rushed injections were associated with more abscesses. Similarly, other health outcomes associated with rushed injections have public health implications. Further, the existing literature establishes a relationship between rushed injections and fear of law enforcement. One study showed that human immunodeficiency virus (HIV) infection was associated with rushed injections due to police presence, fear of being arrested, fear of being arrested for planted drugs, and physical violence. 52 In another study, using pre-filled syringes (where syringes are purchased pre-filled with the injection substance) was independently associated with ever having a rushed injection due to police presence as well as injecting most often in public. 53 While our study did not specifically ask about the reason for rushed injection the following underscore pervasive structural vulnerabilities in our population: (1) 84% were unhoused/unstably housed and 60% reported injecting in a public setting, (2) 53% had a monthly income less than $1000, and (3) 67% had a mental health diagnosis. Importantly, among people with a higher frequency of abscess, almost three-quarters were injected in public settings (71%) and public restrooms 70%. Given the independent health risks associated with unsheltered houselessness, 54 immiseration (i.e., structurally enforced material deprivation), 55 and mental health,56,57 our findings underscore the need for policy-level and institutional interventions. Ethnographic findings, in addition to the data from our study, emphasize the need for interventions that alleviate these risks, starting with increasing access to public restrooms and Water, Sanitation, and Hygiene (WaSH) services to have access to potable water and soap.51,58–61
A higher frequency of abscesses was also associated with being injected by another person. While this is consistent with existing reports,29,62 potential drivers are largely unknown. Almost 40% of PWID in a community-based sample from Vancouver needed help with injecting. 63 Existing data shows that people who need help injecting are younger, have less experience, are female identifying, and are at higher risk for HIV and Hepatitis C (HCV) infections.63–65 Qualitative studies interviewing people who have been injected by someone else have predominantly examined gender dynamics since rates of receiving injections are higher among women.62,64,66,67 These studies showed various associated physical harms among women who are injected by someone else—such as “misses” (missed veins), “blown” veins, that is, overloading of a vein—which resulted in bruises, extreme pain, swelling, citric burns and less often, blood clots, and HCV.68,69 PWID attribute these outcomes to the injecting person’s impatience and/lack of attention due to withdrawal or substance intoxication. 69 Other findings show that among subpopulations of PWID, particularly women and people with disabilities, risks associated with being injected are amplified by existing vulnerabilities. 68 Given the complex dynamics between vulnerabilities such as age, experience, gender, and disability associated with being injected by other people, we would be remiss if we did not draw attention to interventions addressing material and subsistence insufficiencies that can exacerbate these vulnerabilities. People who use drugs led interventions, such as teaching individuals how to self-inject, is one way to reduce harm associated with these practices, however, they are focused on individual behavior change.68,70 Data from Vancouver Area Network of Drug Users, show that supervised consumption sites (SCS) reduce health risks associated with being injected by another person. 68 While our findings do not present gender differences in abscesses, there is a female-specific association between sex work, abscess, and injection drug use among PWID. These intersectional risks should be considered via PWID-led programmatic development and clinical care.32,33
Concurrent with existing reports, needle licking was associated with a higher risk of abscess.16,29,71 Needle licking can contaminate syringes and other injection equipment, oral bacteria, and infections arising from oropharyngeal flora pose serious health risks such as abscess, cellulitis, and even endocarditis.29,72–77 Behavioral and structural factors are associated with needle licking, necessitating a multilevel approach to interventions. In qualitative studies, participants report licking needles to test for quality assurance of substance, to reduce dose wastage during preparation, as a part of their preparation ritual, and to clean the needle. 71 Importantly, fentanyl was flooding the illicit drug market during our data collection period. Multiple reports from the fentanyl transition showed that participants’ taste supply to check for contamination.78–80 Data also indicates that PWID engage in needle licking when potable water is unavailable. 72 WaSH insecurity among unhoused communities in Los Angeles is a barrier to accessing water, accentuated by extant reports of unhoused people accessing water from fire hydrants and storing water for nighttime use. 58 While needle licking can be addressed behaviorally, factors in the built environment, such as lack of potable water, the systemic and structural violence of the illicit drug market,81–83 and limited access to drug checking may also drive these perceived “risk” behaviors. 84 Behavioral and educational programmatic interventions have been effective in reducing needle licking.85–92 Additionally, expanding sterile syringe coverage, 21 access to alcohol wipes and other supplies,9,28 and policy level interventions to address water equity and security for unhoused people are necessary measures to reduce infection risk.58,61,85
In contrast to existing data, which shows that buprenorphine treatment is largely protective against injection-related infections, 86 our study found that reporting 1 abscess in the last 3 months was associated with current enrollment in buprenorphine treatment. This contrasts with existing data, which shows that buprenorphine treatment is largely protective against injection-related infections. 86 We believe this is influenced by multiple events that occurred during the study period: (1) the illicit opioid market transitioned from heroin to fentanyl and (2) there was a shift from injecting heroin to smoking fentanyl. The illicit opioid market transition was marked by heroin scarcity and increased fear of withdrawal episodes among PWID. 93 Extant data show that withdrawal is a driver of treatment initiation, and data show that PWID rely on MOUD to mitigate fluctuations in the illicit opioid supply.94,95 Given these factors, it is possible that PWID who were injecting heroin and were unable to find it due to the market shift sought buprenorphine treatment and reported abscesses that occurred from injection drug use in the previous 3 months. That said, there are several possible explanations for this finding that are beyond the scope of our data and should be considered with some important limitations in mind. In this study we asked participants who reported that they had participated in substance use treatment in the last 3 months, “Are you currently enrolled in any kind of substance use treatment?” and if they said “yes,” we asked, “Which treatments are you currently receiving?” of which buprenorphine was one of the options. Due to this, we are only able to conclude that participants were receiving buprenorphine treatment at the time of the survey and that it was a prescribed buprenorphine (given that we had a separate survey item for non-prescribed buprenorphine). However, we would place limited emphasis on this finding as we are unable to provide several important details pertaining to dosage and time under treatment. Future longitudinal studies should explore this further.
Like much of the existing data, both injection frequency and daily heroin use were associated with higher frequency of abscesses in the last 3 months.10,96 These underscore a need for harm reduction interventions that facilitate safer injection and those that move away from injection drug use. Among other factors, abscesses from street-based heroin use occur due to illicit market contaminants leading to an unregulated drug supply. 86 While safe supply is heavily discussed for its impact in overdose prevention due to regulated doses, medical heroin (diacetylmorphine) may also reduce the risk of abscesses. 97 Heroin-assisted treatment (HAT) involves the provision of medical heroin at clinics and is an evidence-based intervention for reducing negative health outcomes associated with opioid use.98–103 For abscesses, providing regulated doses of medical-grade heroin may reduce the risk of abscess that arise from illicit market substances that are often cut with non-sterile and harmful materials. 97 Additionally, syringe services programs, medication for opioid use disorder, behavioral, psychosocial, and educational programmatic interventions have all been effective in reducing receptive syringe sharing and self-treatment practices among PWID.87–92
Structural harm reduction for risks associated with injection drug use and daily heroin starts with accessible, safe, and permanent housing. 104 There is substantial evidence to link the impacts of housing and related violence, such as forced displacement and sweeps on substance use-related health and fatalities.55,105–107 Increased access to housing can prevent negative health outcomes associated with harmful injection practices, such as rushed injection and sharing. Similarly, Overdose Prevention Programs (OPPs) offer individuals a safe, sterile, and protected environment where people can use them safely. OPPs are an evidence-based intervention that reduces the risk of rushed injections among PWID and are evidenced based in reducing the risk of SSTIs. 108 OPPs,109–113 both sanctioned and unsanctioned, are effective at reducing emergency room visits, neighborhood crime, and injection behaviors like injecting alone and receptive syringe sharing, and rushed injections. 112 OPPs co-located within service centers where PWID can access other wrap-around services, such as housing, healthcare, and basic needs, have been shown to promote safety, respite, and are effective community-building initiatives. 114
Having 2 or more abscesses was also associated with daily methamphetamine use. In the existing literature, methamphetamine is associated with Methicillin-resistant Staphylococcus aureus colonization. Methamphetamines promote the formation of biofilm, which can hinder immune responses and wound healing.115,116 This can result in individuals being more prone to infections.115,116 These findings, in addition to the rapid increase in opioid stimulant co-use that characterizes the third and fourth waves of the opioid crisis, present an opportunity to discuss harm reduction interventions for people who use stimulants.117–120 Low threshold interventions to reduce methamphetamine injection, such as the distribution of gelatine capsules and those that reduce pipe sharing among people who are smoking, continue to be important.121,122 However, among other factors, withdrawal remains a barrier to methamphetamine treatment.123–125 There is limited and mixed evidence about the effectiveness of prescribing psychostimulants for treatment of stimulant use disorder;118,126 however, the data are sparse and warrant continued examination. Qualitative data show that people who use stimulants can be supported by increased provider knowledge about stimulant use to reduce occurrences of stigmatizing patient-provider interactions, SCS for people using stimulants, sterile equipment such as pipes and sharps containers, and better withdrawal management for stimulants to reduce the risk of PDDs. 127
Medical settings continue to be a missed opportunity to treat, prevent, and support PWID with abscesses. The high rates of self-treatment and patient direct discharges (PDD) associated with abscess present a much-needed avenue to discuss the importance of integrating harm reduction service delivery into clinical.128–131 While this involves comprehensive withdrawal management within hospital settings, most PWID attempt to self-treat abscess and delay seeking medical treatment via pressing puss out, using a hot/warm compress, and hydrogen peroxide.12,132 Extant findings show that PWID report several barriers to getting care, such as extended wait times, fear of going to hospitals, and concerns about being identified as persons who inject drugs. 132 Collaborative programs, between multiple medical spaces such as emergency rooms and wound care clinics that are developed around the expertise of PWID are more likely to reduce barriers to accessing health services and are also more cost effective.131,133–139 Community-based harm reduction service delivery can provide a bridge to accessing care via clinical locations like emergency departments. Mobile outreach clinics, 133 abscess and wound clinics can provide accessible, low-barrier care to PWID.134,140 Such sites often accept walk-ins, are well integrated with syringe services programs and wrap-around resources, are connected to MOUD, and harm-reduction based, eliminating several barriers to seeking care at hospitals cited by PWID who delay treatment for abscess.12,21,141,142
Limitations
Results from this study have several limitations to consider. These analyses use a cross-sectional study design, which means that the direction of associations is unknown. Future studies using longitudinal designs should examine these relationships. While abscesses can occur anywhere in the body, we examined the number and self-reported abscesses, so it is important to note that these are skin abscesses and that they could include other injection-related soft tissue infections, such as cellulitis, since we did not verify this with a clinician’s diagnosis. Regardless, we used the term “abscess” in the manuscript because the survey item specifically asked participants “In the last 3 months, have you had an abscess related to injection drug use, even if it did not “come to a head,” drain, or require treatment of any kind?” Further, there is some data to show that PWID can accurately identify and describe abscesses to self-treat. 141 That said, self-report data are also subject to recall and social desirability bias. However, in reliability and validity studies among similar samples of PWID, reports have been found to have acceptable psychometric properties.143–145 Our sample is not representative of PWID in Los Angeles, CA, and Denver, CO, because we used convenience sampling approaches. This was done because we collected data during the COVID-19 pandemic and typical approaches that rely upon snowball sampling, such as respondent-driven sampling and target sampling,146,147 were not feasible. Lastly, the study was not powered to examine risk factors for abscesses and so may be underpowered to fully examine these associations.
Conclusion
Our findings demonstrate overlapping and intersecting behavioral and structural risk factors for abscess, such as rushed injections, being injected by others, and needle licking. These risk factors may be intensified by existing structural vulnerabilities, housing insecurity and immiseration. Substance use-related factors, such as daily heroin and methamphetamine use, were also associated with increased frequency of abscesses. Our findings point to a multi-level approach to reducing abscess prevalence by increased education around safe injection practices, institutional interventions (e.g., reduced healthcare stigma, clinical harm reduction), and structural interventions such as OPP, safe supply, and housing.
Supplemental Material
sj-docx-1-tai-10.1177_20499361251344765 – Supplemental material for Risk factors for multiple skin abscesses among community-recruited people who inject drugs in Los Angeles, CA, and Denver, CO: a cross-sectional study
Supplemental material, sj-docx-1-tai-10.1177_20499361251344765 for Risk factors for multiple skin abscesses among community-recruited people who inject drugs in Los Angeles, CA, and Denver, CO: a cross-sectional study by Siddhi S. Ganesh, Gilbert A. Orta Portillo, Daniel R. Trigo, Katrina Ninh, Karina Dominguez Gonzalez, Patricia Wilkins, Eric Kovalsky, Karen F. Corsi, Joshua Barocas and Ricky N. Bluthenthal in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-2-tai-10.1177_20499361251344765 – Supplemental material for Risk factors for multiple skin abscesses among community-recruited people who inject drugs in Los Angeles, CA, and Denver, CO: a cross-sectional study
Supplemental material, sj-docx-2-tai-10.1177_20499361251344765 for Risk factors for multiple skin abscesses among community-recruited people who inject drugs in Los Angeles, CA, and Denver, CO: a cross-sectional study by Siddhi S. Ganesh, Gilbert A. Orta Portillo, Daniel R. Trigo, Katrina Ninh, Karina Dominguez Gonzalez, Patricia Wilkins, Eric Kovalsky, Karen F. Corsi, Joshua Barocas and Ricky N. Bluthenthal in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
We would like to thank the study participants for their time and effort in this project. We would also like to thank the following individuals who meaningfully contributed to the study: Cheyenne J. Page for study coordination; Jesse L. Goldshear, Kelsey Anne Simpson, Anthony J. Dimario, Srehith Sannareddy, Pooja Shah, Andrew Bong, and Kelly Park for their support with data collection; Selena Venegas and Rebecca Smeltzer for invaluable administrative support.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.