
Abstract
Objective
To investigate the potential factors affecting methicillin-resistant Staphylococcus aureus (MRSA) colonization and infection in patients with human immunodeficiency virus (HIV) infection.
Methods
A systematic search of publications listed in electronic from inception up to August 2020 was conducted. A random-effects model was used to calculate odds ratio (OR) with 95% confidence interval (CI).
Results
A total of 31 studies reporting 1410 MRSA events in 17 427 patients with HIV infection were included. Previous hospitalization (OR 1.80; 95% CI 1.37, 2.36), previous antibiotic therapy (OR 2.69; 95% CI 2.09, 3.45), CD4+ count (OR 1.79; 95% CI 1.41, 2.28), Centers for Disease Control and Prevention classification of stage C (OR 2.66; 95% CI 1.80, 3.93), skin lesions (OR 2.02; 95% CI 1.15, 3.55), intravenous device use (OR 2.61; 95% CI 1.59, 4.29) and an MRSA colonization history (OR 6.30; 95% CI 2.50, 15.90) were significantly associated with an increased risk of MRSA colonization and infection. Antiretroviral therapy (OR 0.71; 95% CI 0.50, 0.99) and current antibiotic use (OR 0.13; 95% CI 0.05, 0.32) were significantly associated with a reduced risk of MRSA colonization and infection.
Conclusion
MRSA colonization and infection in HIV-infected patients is associated with a number of risk factors.
Keywords
Introduction
The prevalence of methicillin-resistant Staphylococcus aureus (MRSA) infection has been increasing globally. The infection-causing staphylococci could be a harmless commensal or a potentially life-threatening pathogen.1,2 MRSA infections range from localized skin and soft-tissue infections to disseminated blood stream infections, which result in substantial healthcare costs, morbidity and mortality.3–5 At present, the association of MRSA colonization with human immunodeficiency virus (HIV) infection is of particular interest because of the association of morbidity and mortality with MRSA in patients with HIV infection. 6 The potential reasons for this are that bacterial infections have been considered the most prevalent events affecting patients with HIV infection and that MRSA possesses important virulence factors and frequently acquires resistance to various antibiotics. 7 Although several studies have illustrated MRSA prevalence and severity in patients with HIV infection, the factors predisposing such patients to MRSA colonization and infection have not been illustrated well.7–13
A previous systematic review explored the potential factors associated with MRSA at the time of admission to hospital or an intensive care unit. 14 It included 29 studies and identified that the potential risk factors included previous hospitalization, nursing home exposure, the history of exposure to healthcare-associated pathogens, congestive heart failure, diabetes mellitus, pulmonary disease, immunosuppression and renal failure. 14 A previous systematic review of nine studies with high methodological quality (level A) indicated that antimicrobial use and previous hospitalization were independent risk factors for MRSA colonization in patients with HIV infection. 15 However, these systematic reviews were not restricted to patients with HIV infection and did not perform quantitative analysis.14,15 Identifying the potential risk factors for MRSA colonization and infection is particularly important in patients with HIV infection; however, these risk factors remain to be definitively determined. Therefore, a systematic review and meta-analysis was performed to explore the potential risk factors for MRSA colonization and infection in patients with HIV infection.
Materials and methods
Data sources and search strategy
A systematic search of publications listed in electronic databases (PubMed®, EMBASE and the Cochrane Library) from inception up to August 2020 was conducted using the following key words or Medical Subject Heading terms: (“human immunodeficiency virus” OR “immunodeficiency” OR “immunocompromised” OR “HIV” OR “AIDS”) AND (“Staphylococcus” OR “Staphylococcus aureus” OR “methicillin-resistant Staphylococcus aureus” OR “MRSA” OR “resistant bacterial infection”) AND “human”. Studies reporting the risk factors for MRSA colonization and infection in patients with HIV infection were included in this analysis. There were no restrictions based on language or status. Corresponding authors were contacted to obtain additional data if the reported data were insufficient. A manual review of references from the selected articles was undertaken to identify any other eligible studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis Statement (PRISMA; 2009) guidelines were followed to perform and report this systematic review and meta-analysis. 16
Selection criteria
A study was included if it met all of the following inclusion criteria: (i) Patients: patients with HIV infection; (ii) Exposure: the identified factors were reported in ≥3 studies; (iii) Outcome: MRSA colonization and infection, reported effect estimates, or the reported data could be translated into odds ratio (OR) and 95% confidence interval (CI); and (iv) Study design: cross-sectional, case–control and cohort studies. Studies designed as case reports, case series or reviews, and those involving animal models, were excluded. Two reviewers (X.H. & W.Z.) independently screened the eligible studies based on the title, abstract and full text of each study. Any inconsistency in the data obtained by the two reviewers was settled by a third reviewer (K.H.) by reading the full text of the article.
Data collection and quality assessment
The data from the retrieved studies were independently extracted by two reviewers (Y.L. & L.Z.) in a standard data abstraction form. Any disagreement was resolved by discussion until a consensus was reached. Data on the selected variables collected from each study included the following: the first author’s surname, publication year, country, study design, sample size, MRSA colonization and infection events, mean age, male proportion, sample type, dominant strain, adjusted factors and reported outcomes.
The methodological quality of each individual study was assessed by using the Newcastle–Ottawa Scale (NOS), which is a comprehensive and partially validated scale for assessing the quality of observational studies. 17 The starring system of NOS is based on selection (4 items), comparability (1 item) and outcome (3 items); and ‘star system’ ranges from 0 to 9 stars. 17 The quality assessment was independently performed by two reviewers (X.H. & W.Z.) and any conflicts between the reviewers were settled by an additional reviewer (N.H.) by reading the full text of the retrieved articles.
Statistical analyses
All analyses were performed using Stata® software (version 10.0; Stata Corporation, College Station, TX, USA). The effect estimates regarding the risk factors for MRSA colonization and infection were assigned as OR and 95% CI for each study and the pooled analyses were performed using a random-effects model.18,19 The heterogeneity across the included studies was assessed using the I2 and Q statistic; and significant heterogeneity was defined as I2 > 50% or PQ statistic < 0.10.20,21 The stability of pooled conclusions for factors reported in ≥10 studies was assessed using sensitivity analysis through the sequential exclusion of individual studies. 22 Subgroup analyses for these factors were evaluated based on country, study design and reported outcomes, and the differences among the subgroups were assessed using the interaction P-test, which assumes that the data distribution met the t-test criteria. 23 Publication bias for the factors reported in ≥10 studies were assessed using the funnel plot, Egger's test 24 and Begg's test. 25 The P-value for pooled results was two-sided and the inspection level was 0.05.
Results
In total, 5743 articles were identified from the initial electronic database searches and 3143 were retained after the removal of duplicate articles. A further 2971 articles were excluded because of irrelevant titles or abstracts and the remaining 172 were used for further full-text evaluations. Of these articles, 141 were further excluded because of unreported risk factors (n = 63), factors in <3 studies (n = 52), unreported MRSA events (n = 17) or review or meta-analysis (n = 9). Reviewing the reference lists of the remaining studies did not yield any new eligible studies as all relevant studies had already been included during the database searches. A total of 31 studies, representing a total of 17 427 patients with HIV infection, were selected for the final meta-analysis.26–56 The details of the literature search and study selection are summarized in a PRISMA flow diagram (Figure 1).

Flow diagram of eligible studies showing the number of citations identified, retrieved and included in the final meta-analysis to identify potential risk factors for methicillin-resistant Staphylococcus aureus (MRSA) colonization and infection in patients with human immunodeficiency virus infection.
The baseline characteristics of the included studies and recruited patients are presented in Table 1.26–56 Of the 31 included studies, eight had a cohort design, 17 had a cross-sectional design and the remaining six studies had a case–control design. These studies reported a total of 1410 MRSA colonization events and the events of MRSA colonization and infection that occurred in each study ranged from 6 to 252. Of the studies, five were conducted in Europe, 15 in North or South America, five in Africa and the remaining six in Asia. In total, 20 studies reported the crude data and the remaining 11 reported adjusted effect estimates. The quality of the included studies was assessed using the NOS, which rated 5 stars to 17 studies and 4 stars to the remaining 14 studies (Table 2).

NA, not available; SCC, staphylococcal chromosome cassette; MSM, men having sex with men; SSTI, skin and soft-tissue infection; HCV, hepatitis C virus.

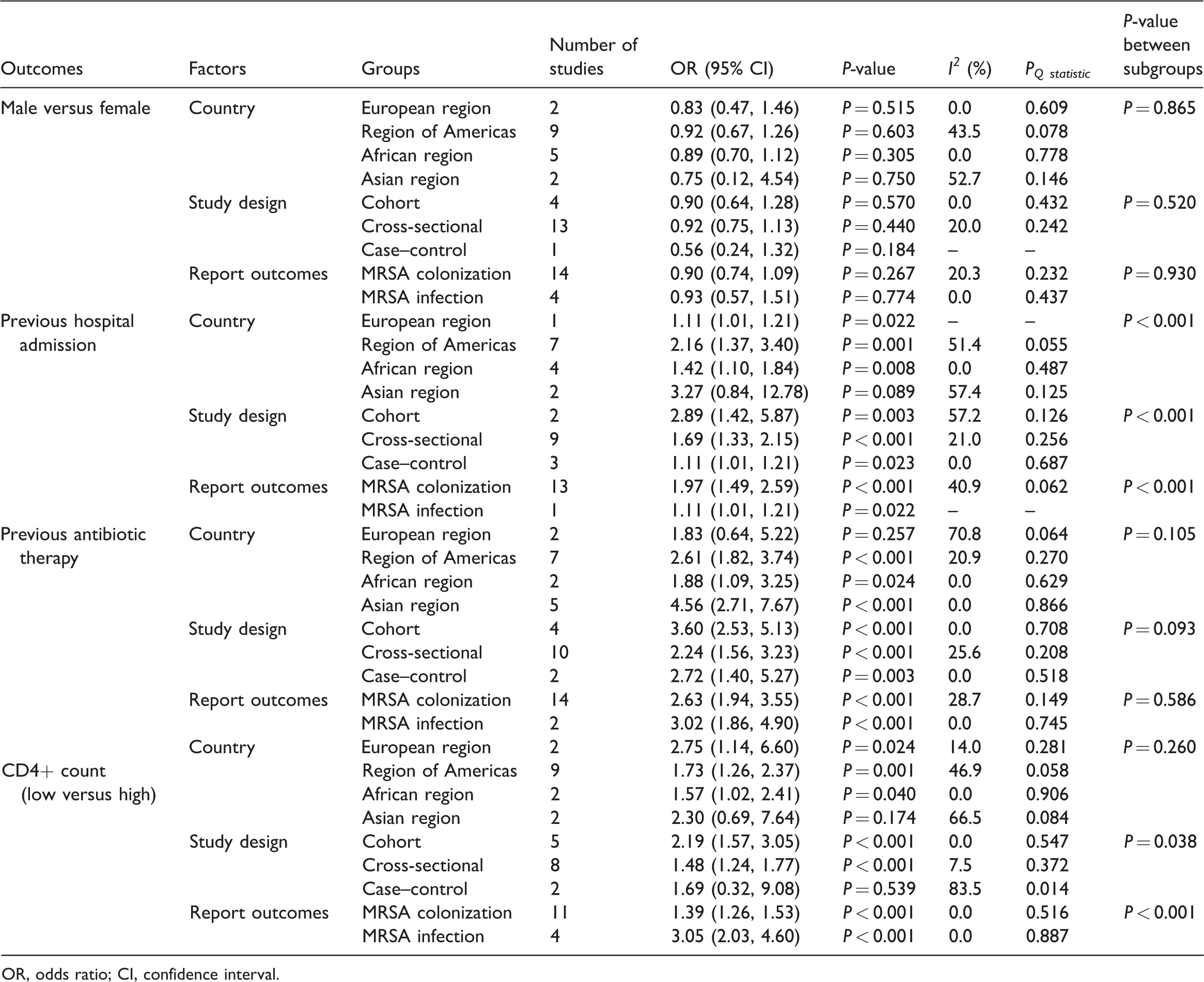
A total of 18 studies reported sex difference as a risk factor for MRSA colonization and infection in patients with HIV infection.27,32,34,36,38–42,44–49,52,53,56 No significant difference was noted between males and females regarding the risk of MRSA colonization and infection in patients with HIV infection (OR 0.91; 95% CI 0.77, 1.07; P = 0.247; Figure 2) and nonsignificant heterogeneity across the included studies was detected (I2 = 10.8%; P = 0.326). When the study conducted by Popovich 2013 was excluded, 41 sensitivity analysis suggested men with HIV infection had a lower risk of MRSA colonization and infection than females with HIV infection (Figure 3A). The results of pooled analyses in all subgroups were consistent with those of the overall analysis and only nonsignificant differences between males and females remained (Table 3). No significant publication bias for sex difference as a risk factor for MRSA colonization and infection was detected (P-value for Egger's test, 0.665; P-value for Begg's test, 0.880; Figure 4A).


Sensitivity analyses: (a) sensitivity analysis for the role of sex difference on the risk of methicillin-resistant Staphylococcus aureus (MRSA) colonization inhuman immunodeficiency virus infection (HIV)-infected patients; (b) sensitivity analysis for the role of previous hospital admission on the risk of MRSA colonization in HIV-infected patients; (c) sensitivity analysis for the role of previous antibiotic therapy on the risk of MRSA colonization in HIV-infected patients; (d) sensitivity analysis for the role of CD4+ count on the risk of MRSA colonization in HIV-infected patients.
OR, odds ratio; CI, confidence interval.

Funnel plots: (a) funnel plot for the role of sex difference on the risk of methicillin-resistant Staphylococcus aureus (MRSA) colonization inhuman immunodeficiency virus infection (HIV)-infected patients; (b) funnel plot for the role of previous hospital admission on the risk of MRSA colonization in HIV-infected patients; (c) funnel plot for the role of previous antibiotic therapy on the risk of MRSA colonization in HIV-infected patients; (d) funnel plot for the role of CD4+ count on the risk of MRSA colonization in HIV-infected patients.
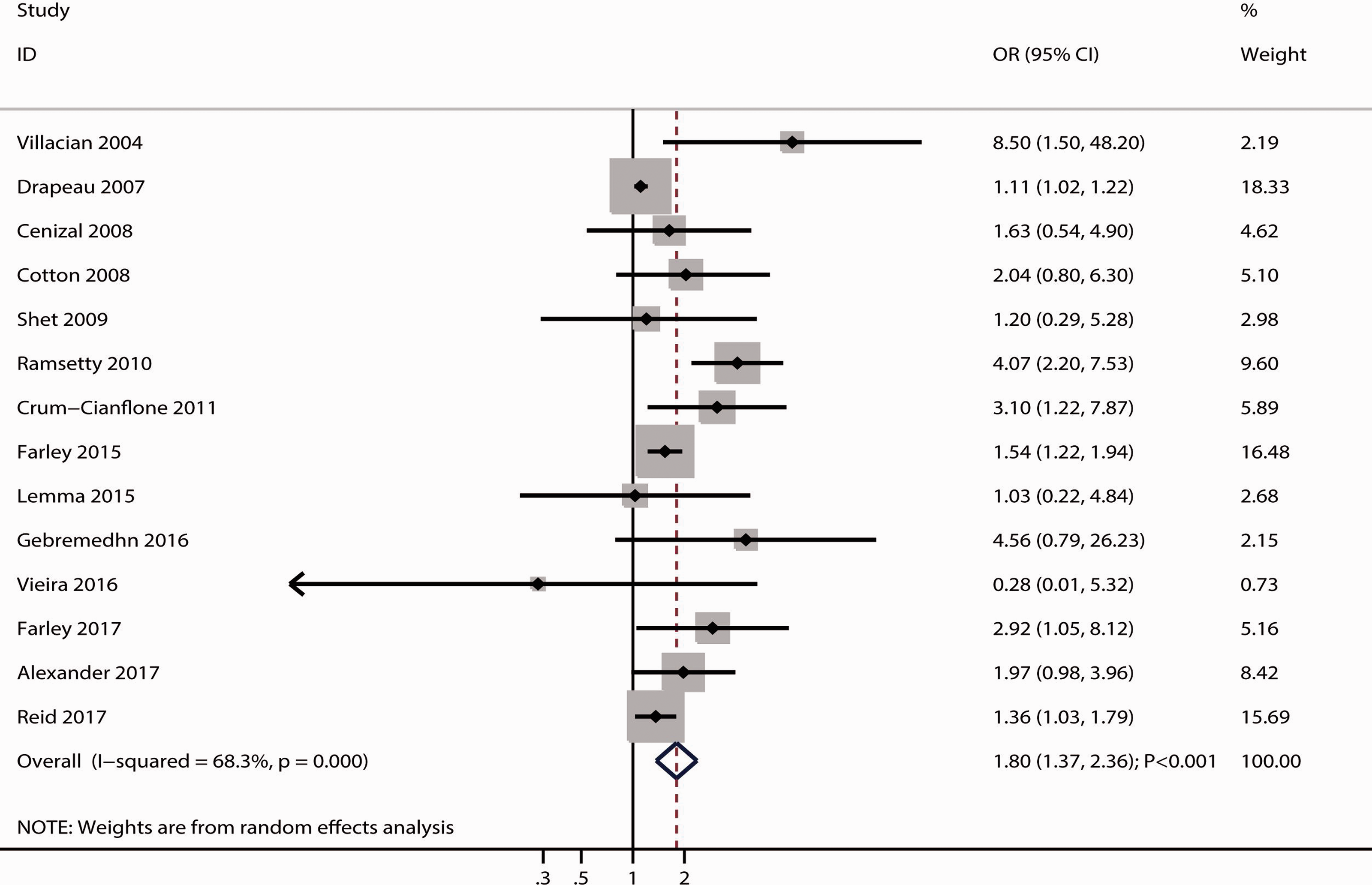
In total, 14 studies reported previous hospitalization as a risk factor for MRSA colonization and infection in patients with HIV infection.29,31,32,34–36,38,45–48,50–52 Previous hospitalization was associated with an increased risk of MRSA colonization and infection (OR 1.80; 95% CI 1.37, 2.36; P < 0.001; Figure 5) and significant heterogeneity was found across the included studies (I2 = 68.3%; P < 0.001). This conclusion was robust and not altered by the sequential exclusion of individual studies (Figure 3B). Although the results of subgroup analyses were consistent with those of the overall analysis in most subgroups, previous hospitalization was not associated with the risk of MRSA colonization and infection for pooled studies conducted in Asia (Table 3). Although Begg's test results revealed no significant publication bias for previous hospitalization (P = 0.324), Egger's test results showed potential significant publication bias for previous hospitalization as a risk factor for MRSA colonization and infection (P = 0.008; Figure 4B). This conclusion was not altered after adjusting for the potential publication bias using the trim-and-fill method. 57
A total of 16 studies reported previous antibiotic therapy as a risk factor for MRSA colonization and infection in patients with HIV infection.27–29,32,35–38,40,43,47,50–53,56 The pooled result indicated that previous antibiotic therapy was associated with an increased risk of MRSA colonization and infection (OR 2.69; 95% CI 2.09, 3.45; P < 0.001; Figure 6) and nonsignificant heterogeneity was detected among included studies (I2 = 19.5%; P = 0.231). Sensitivity analysis indicated the pooled conclusion was stable after excluding any particular study (Figure 3C). Subgroup analyses revealed the negative effect of previous antibiotic therapy on the risk of MRSA colonization and infection in most subgroups; however, previous antibiotic therapy was not associated with this risk when pooled with the results obtained from a study conducted in Europe (Table 3). No significant publication bias for previous antibiotic therapy as a risk factor for MRSA colonization and infection was detected (P-value for Egger's test, 0.417; P-value for Begg's test, 0.192; Figure 4C).

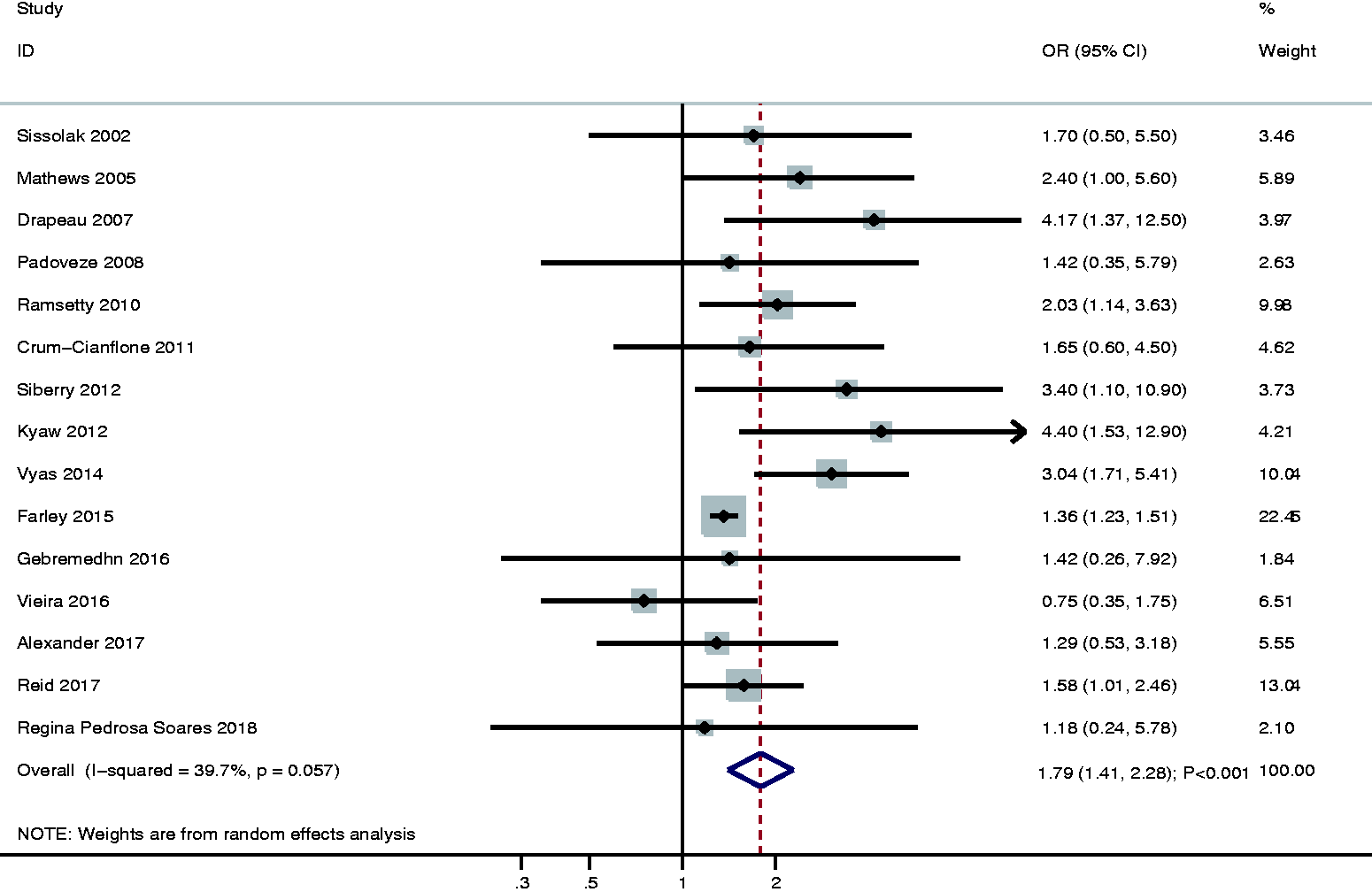
In total, 15 studies reported the CD4+ count for the risk of MRSA colonization and infection in patients with HIV infection.26,30,31,33,36,38–40,44,45,47,48,51–53 A low CD4+ count was associated with an increased risk of MRSA colonization and infection (OR 1.79; 95% CI 1.41, 2.28; P < 0.001; Figure 7) and a potential significant heterogeneity was detected across the included studies (I2 = 39.7%; P = 0.057). The results of sensitivity analysis showed that the pooled conclusion did not change after the sequential exclusion of any individual study (Figure 3D). Subgroup analyses showed that low CD4+ count was not associated with an MRSA colonization and infection risk when pooled with studies conducted in Asia or studies with a case–control design (Table 3). Although Begg's test results indicated no significant publication bias (P = 0.843), Egger's test results revealed a potential publication bias for CD4+ count as a risk factor for MRSA colonization and infection (P = 0.043) (Figure 4D). The pooled conclusion remained unaltered after adjusting for publication bias using the trim-and-fill method. 57
Eight and seven studies reported that highly active antiretroviral therapy (HAART) and antiretroviral therapy (ART), respectively, were associated with an MRSA colonization and infection risk (Figure 8).26,28–33,35,37–39,44,45,53 ART was associated with a reduced risk of MRSA colonization and infection (OR 0.71; 95% CI 0.50, 0.99; P = 0.041), whereas HAART was not associated with this risk (OR 0.86; 95% CI 0.57, 1.32; P = 0.495). A significant heterogeneity was detected for ART (I2 = 49.6%; P = 0.064), but nonsignificant heterogeneity was detected for HAART (I2 = 20.1%; P = 0.270).

Six and seven studies reported the association of Centers for Disease Control and Prevention (CDC) classification and viral load, respectively, with the risk of MRSA colonization and infection (Figure 9).26,27,30–32,34,37,44,48,49,53,54 The CDC classification of stage C was associated with an increased risk of MRSA colonization and infection (OR 2.66; 95% CI 1.80, 3.93; P < 0.001), whereas the viral load was not associated with this risk (OR 1.64; 95% CI 0.95, 2.83; P = 0.075). No heterogeneity was detected for CDC classification of stage C (I2 = 0.0%; P = 0.516), whereas significant heterogeneity was detected for viral load (I2 = 61.1%; P = 0.017).

The number of studies that reported the association of current antibiotic use, skin lesions, intravenous device use, current trimethoprim–sulfamethoxazole (TMP–SMX) use, and an MRSA colonization history with the risk of MRSA colonization and infection was three, four, four, eight, and six, respectively (Figure 10).26–29,32–35,37,38,40,47,48,51,55 Skin lesions (OR 2.02; 95% CI 1.15, 3.55; P = 0.015), intravenous device use (OR 2.61; 95% CI 1.59, 4.29; P < 0.001) and an MRSA colonization history (OR 6.30; 95% CI 2.50, 15.90; P < 0.001) were associated with an increased risk of MRSA colonization and infection, whereas the current use of antibiotics was associated with a reduced risk of MRSA colonization and infection (OR 0.13; 95% CI 0.05, 0.32; P < 0.001). The current use of TMP–SMX was not associated with an MRSA colonization and infection risk (OR 1.48; 95% CI 0.81, 2.69; P = 0.203). Significant heterogeneity was detected for an MRSA colonization history (I2 = 72.9%; P = 0.002), but not for current antibiotic use (I2 = 0.0%; P = 0.399), skin lesions (I2 = 0.0%; P = 0.706), intravenous device use (I2 = 0.0%; P = 0.553) and current TMP–SMX use (I2 = 39.7%; P = 0.114), across the included studies.
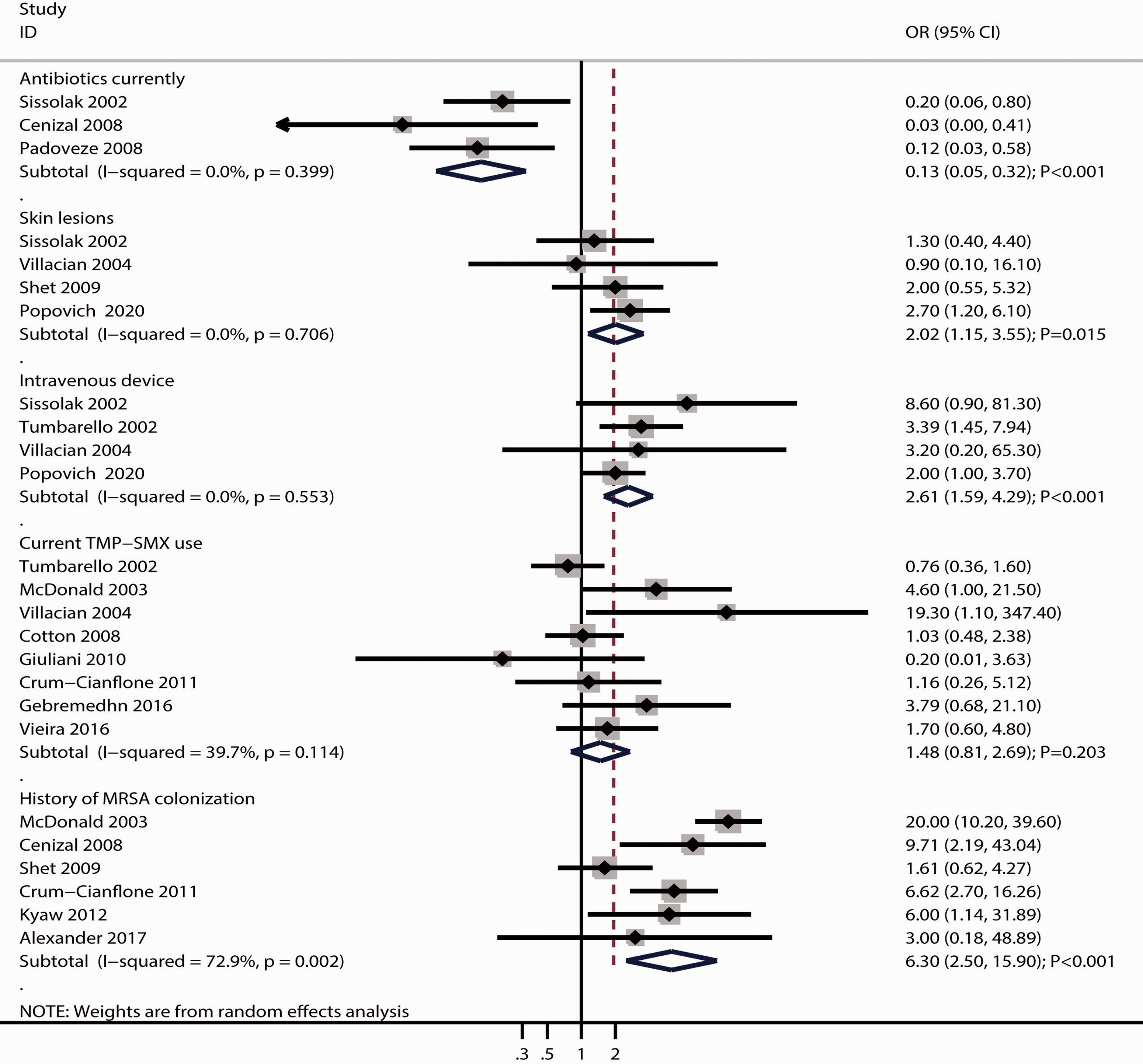
Association of current antibiotic use, skin lesions, intravenous device use, current trimethoprim–sulfamethoxazole (TMP–SMX) use and a history of methicillin-resistant Staphylococcus aureus (MRSA) colonization with the risk of MRSA colonization in patients with human immunodeficiency virus infection. OR, odds ratio; CI, confidence interval.26–29,32–35,37,38,40,47,48,51,55
Discussion
From 31 studies, the present meta-analysis analysed data from a total of 1410 MRSA events in 17 427 patients with HIV infection. The current findings suggest that previous hospitalization, previous antibiotic therapy, CD4+ count, CDC classification stage C of HIV, skin lesions, intravenous device use and an MRSA colonization history increase the risk of MRSA colonization and infection, whereas ART and the current use of antibiotics reduce the risk of MRSA colonization and infection. The association between previous hospitalization and MRSA colonization and infection risk varied when stratified by country, study design, and reported outcomes, whereas that between CD4+ count and MRSA colonization and infection risk varied when stratified by study design and reported outcomes.
A previous systematic review performed reported that the overall prevalence of MRSA colonization was 6.9% in patients with HIV infection. 58 Previous hospitalization within 12 months and previous or current incarceration were associated with an increased risk of MRSA colonization, whereas current ART and TMP–SMX use were not associated with this risk. 58 A previous study reported that the prevalence of MRSA in patients with HIV infection was 7%, with the highest prevalence observed in Southeast Asia (16%), second highest in the Americas (10%) and the lowest in Europe (1%). 59 Moreover, they reported that previous MRSA infection, hospitalization in the previous year and antibiotic use increased the risk of MRSA colonization in these patients. 59 However, these two previous studies did not address whether the pooled results vary based on country, study design and reported outcomes.58,59 Therefore, the present study aimed to identify the comprehensive risk factors for MRSA colonization and infection in patients with HIV infection.
This current meta-analysis identified several risk factors for MRSA colonization and infection in HIV-infected patients, including previous hospitalization, previous antibiotic therapy, CD4+ count, CDC classification of stage C, skin lesions, intravenous device use and an MRSA colonization history. Several reasons could explain these results. First, previous hospitalization could increase interactions with other potentially infected patients as well as healthcare staff and contact with materials contaminated with MRSA. Secondly, a higher frequency of antibiotic exposure could accelerate the progression of antimicrobial resistance.60,61 Thirdly, CD4+ count reflects the severity of immunodeficiency, which could increase the susceptibility to MRSA colonization and infection. Fourthly, CDC classification of stage C was significantly associated with the severity of infection in these patients; the susceptibility to MRSA colonization and infection was stronger in patients with a CDC classification of stage C than those with a CDC classification of stage A or B. Fifthly, skin lesions are significantly associated with infection and antibiotic exposure. Sixthly, the use of intravenous devices could increase the risk of MRSA colonization. 62 Finally, a previous MRSA colonization history was associated with persistent colonization in nares or other body sites.63,64
This current meta-analysis found that ART and current antibiotic use were associated with a reduced risk of MRSA colonization and infection. The potential reason for this is likely associated with the reduced infection severity in these patients, which could be attributed to ART and the current use of antibiotics. However, sex difference, HAART use, viral load and current TMP–SMX use did not affect the risk of MRSA colonization and infection in patients with HIV infection. These results could be explained by the number of included studies, adjusted factors, statistical power and the reliability of results reported by each study. Although most of the pooled conclusions were stable, male patients with HIV infection potentially had a lower prevalence of MRSA colonization and infection than female patients. This could be explained by the sex difference in the prevalence of MRSA colonization and infection among patients with HIV infection.
This current meta-analysis observed that the country affected the association of previous hospitalization and study design or reported outcomes affected that of previous hospitalization and CD4+ count with the risk of MRSA colonization and infection. In addition, previous hospitalization and CD4+ count did not affect the risk of MRSA colonization and infection for pooled studies conducted in Asia. Moreover, CD4+ count was not associated with the risk of MRSA colonization and infection in pooled case–control studies. This could be because the number of studies in these subgroups was smaller than expected, whereas the pooled 95% CI was broad and nonsignificant associations were observed. Finally, the definition of MRSA colonization and infection varies, which could affect the potential risk factors (Table 2).
This current meta-analysis had the following limitations: (i) the included studies had cohort, case–control and cross-sectional designs; causality could not constructed, and uncontrolled selection, recall or other biases were not assessed; (ii) most studies reported the results of crude data and these results were not adjusted with potential covariates, which could affect the risk of MRSA colonization and infection; (iii) the heterogeneity for several factors were not fully explained by sensitivity and subgroup analyses; (iv) the study was not registered in PROSPERO and the transparency of the current study was restricted; and (v) the inherent limitations of traditional meta-analysis based on published articles, including publication bias, and the analysis based on pooled data prevented the performance of more detailed stratified analyses.
In conclusion, the findings of this current meta-analysis provide a comprehensive list of risk factors for MRSA colonization and infection in patients with HIV infection. These risk factors include previous hospitalization, previous antibiotic therapy, CD4+ count, CDC classification of stage C, skin lesions, intravenous device use and an MRSA colonization history. The potential protective factors were ART and the current use of antibiotics. The results of this current meta-analysis should be verified by further large-scale prospective studies.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211063019 - Supplemental material for Risk factors for methicillin-resistant Staphylococcus aureus colonization and infection in patients with human immunodeficiency virus infection: A systematic review and meta-analysis
Supplemental material, sj-pdf-1-imr-10.1177_03000605211063019 for Risk factors for methicillin-resistant Staphylococcus aureus colonization and infection in patients with human immunodeficiency virus infection: A systematic review and meta-analysis by Xuefei Hu, Keao Hu, Yanling Liu, Lingbing Zeng, Niya Hu, Xiaowen Chen and Wei Zhang in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605211063019 - Supplemental material for Risk factors for methicillin-resistant Staphylococcus aureus colonization and infection in patients with human immunodeficiency virus infection: A systematic review and meta-analysis
Supplemental material, sj-pdf-2-imr-10.1177_03000605211063019 for Risk factors for methicillin-resistant Staphylococcus aureus colonization and infection in patients with human immunodeficiency virus infection: A systematic review and meta-analysis by Xuefei Hu, Keao Hu, Yanling Liu, Lingbing Zeng, Niya Hu, Xiaowen Chen and Wei Zhang in Journal of International Medical Research
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Department of Science and Technology of Jiangxi Province (grant no. 20151BBG70226).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.