
Abstract
Background:
In many low- and middle-income countries, including Ethiopia, dolutegravir (DTG)-based regimens are the preferred first-line regimens for people living with HIV (PLWH). However, there are concerns about hyperglycemia and, in certain circumstances, diabetes mellitus in individuals who have switched to DTG.
Objective:
To assess the prevalence and factors associated with hyperglycemia among PLWH on DTG-based antiretroviral therapy (ART).
Design:
An institutional-based cross-sectional study.
Methods:
The study was carried out from December 1, 2021 to February 30, 2022, and included 423 participants who were recruited via a simple random sampling technique. We enrolled PLWH aged 18 years or older who had been on DTG-based ART for more than 6 months. Data were collected by using an interviewer-administered structured questionnaire, medical card review, physical measurement, and biochemical measurements. Hyperglycemia was defined as a fasting blood glucose level ⩾110 mg/dl. Multivariable logistic regression was used to identify factors associated with hyperglycemia, using SPSS version 26.0 software. Variables with a p-value of <0.05 were considered statistically significant.
Results:
The prevalence of hyperglycemia among PLWH receiving DTG-based ART was 12.1% (95% CI: 9.2–15.1). Age (AOR = 1.04, 95% confidence interval (CI): 1–1.08, p = 0.036), BMI (AOR = 1.09, 95% CI: 1.01–1.17, p = 0.022), and triglyceride level (AOR = 2.44, 95% CI: 1.28–4.64, p = 0.006) were significant predictors of hyperglycemia among PLWH on DTG-based ART.
Conclusion:
Overall, our study revealed a high prevalence of hyperglycemia (12.1%) among PLWH receiving DTG-based ART. Age, BMI, and triglyceride levels were significant predictors of hyperglycemia. These findings underscore the importance of monitoring blood glucose levels in PLWH receiving DTG-based ART, with a special emphasis on patients with advanced age, increased BMI, and increased triglyceride levels.
Background
The increased availability of antiretroviral therapy (ART) has resulted in decreased deaths related to acquired immunodeficiency syndrome (AIDS) and a longer life expectancy for people living with HIV (PLWH) worldwide.1,2 Despite the recognized advantages of ART, its use is not without adverse effects. PLWH are at a greater risk of developing long-term noncommunicable diseases such as diabetes mellitus (DM) and cardiovascular disease (CVD).3,4 A study has shown that men living with HIV on ART are four times more likely to develop DM than those without HIV. 5 Protease inhibitors, and to a lesser degree, nucleoside/nucleotide reverse transcriptase inhibitors and nonnucleoside reverse transcriptase inhibitors (NNRTIs), disrupt the metabolism of glucose and lipids, resulting in hyperglycemia, dyslipidemia, and insulin resistance.6,7 Integrase strand transfer inhibitor (INSTI)-based regimens are advised as the first-line ARTs for the majority of PLWH, according to several recent clinical guidelines. 8
Dolutegravir (DTG), a more recent and prominent second-generation INSTI, works by blocking the HIV integrase enzyme, which stops the virus from integrating its genetic material into host DNA and ultimately prevents viral replication. 9 The World Health Organization (WHO) has endorsed DTG as the primary drug of choice for both first- and second-line ART for all PLWH because of its effectiveness, strong resistance barriers, positive safety and tolerance attributes, and affordability. 10 As a result of the WHO’s endorsement, the 2018 HIV treatment guidelines issued by the Ethiopian Ministry of Health also advocated for the implementation of DTG-based ART as the preferred first- and second-line treatment in the country. 11
Despite its advantages, recent findings from clinical studies, case reports, and case series have indicated a link between DTG and glucose metabolism disorders, such as hyperglycemia.12 –15 Although the evidence is equivocal, the potential cause of DTG-associated hyperglycemia is that DTG suppresses insulin secretion and signaling, possibly via magnesium chelation.16,17 According to research carried out in the USA among PLWH on a DTG-based regimen, 1.4% of patients developed DM, and 13% of patients had prediabetes. 16 Studies in Uganda indicate varying prevalence rates of hyperglycemia among DTG-treated patients, with rates of 19.8%, 18 12.8%, 19 and 7.3% 20 at different hospitals and a case-control study finding that DTG use increases the risk of hyperglycemia sevenfold. 21 Two comparative cross-sectional studies in Ethiopia reported varying prevalence rates of hyperglycemia among PLWH on DTG-based ART, with rates of 17.2% in Northeast Ethiopia 22 and 35.9% in Southwest Ethiopia. 23 The exact rate of hyperglycemia among PLWH receiving DTG-based ART in Ethiopia is currently unknown. Therefore, there is a significant need to research this gap, especially as the majority of PLWH in Ethiopia are receiving DTG-based ART. Thus, this study aimed to determine the prevalence and factors associated with hyperglycemia among PLWH on DTG-based ART at the ART clinic of Debre Markos Comprehensive Specialized Hospital (DMCSH), Northwest Ethiopia.
Methods and materials
Study design, settings, and period
An institutional-based cross-sectional study was conducted at DMCSH from December 1, 2021 to February 30, 2022. DMCSH is located in the Debre Markos City Administration, approximately 299 km from Addis Ababa, the capital of Ethiopia, and 264 km from Bahir Dar, the capital of the Amhara Regional State. The hospital serves over 3.5 million individuals in the town and surrounding districts. Besides offering general services, it has been providing HIV/AIDS interventions, including diagnosis, treatment, and monitoring, since 2005. The hospital has been serving more than 3574 PLWH. DTG-based ART was initially introduced at the DMCSH in April 2019.
Population and eligibility criteria
We enrolled all PLWH aged 18 years or older who had been on DTG-based ART for more than 6 months. Patients with known DM, renal problems, thyroid problems, chronic liver disease, mental health problems, or any other serious health problems (e.g., those with active cancer, heart failure, or who require immediate intensive care), and patients who were not able to provide appropriate information were excluded.
Sample size and sampling technique
In this study, the sample size was calculated via a single population proportion formula with the following assumptions: 50% prevalence of hyperglycemia because of no previous study in the area, 5% margin of error, 95% confidence interval (CI), 10% nonresponse rate, and the total sample became 423. The study subjects were recruited via a simple random sampling technique.
Data collection procedure
Both the data collectors and supervisors were trained for 1 day on the research’s objective and methodology, as well as the data collection approach. The principal investigator oversaw the data collection, and the collected information was reviewed for thoroughness, accuracy, and comprehensibility. Nurse professionals used a structured questionnaire to gather sociodemographic and relevant clinical information. Data on demographic, behavioral, and clinical characteristics were collected directly from participants and from medical records by nurse professionals using a structured questionnaire modified from the WHO stepwise approach to chronic disease risk factor surveillance questions. 24 Nurse professionals gathered anthropometric measurements such as height, weight, waist circumference (WC), and hip circumference with a standard balance and a SECA meter. Body mass index (BMI) was calculated by dividing weight in kilograms (kg) by height in meters squared (m2). Nurse professionals in ART services determine blood pressure (BP) with an automated sphygmomanometer. The participant’s final BP was calculated by averaging three measurements that were taken at 5-min intervals.
Laboratory tests
A laboratory technologist collected approximately 9 ml of fasting venous blood from each participant. Blood samples in vacutainer tubes were clearly labeled and transported immediately to the laboratory for analysis in a cooler box. Sample for fasting blood glucose (mmol/l) was collected by finger pricking and analyzed using an Accu-Chek glucometer manufacturer’s specifications care machine. In this study, we used a single fasting blood glucose measurement to diagnose hyperglycemia.22,25 The lipid profile was analyzed using a Cobas C111 analyzer after centrifugation for 10 min at 10,000 relative centrifugal force. CD4 count (cells/μl) samples were collected in ethylenediaminetetraacetic acid (EDTA) containers and assayed via a Becton Dickinson flow cytometer. Viral load (VL) (copies/ml) samples were collected in EDTA containers and analyzed via a COBAS® Ampliprep/COBAS® (Roche Diagnostics, Ltd., Rotkruez, Switzerland) TaqMan PCR analyzer. Blood collection, serum separation, and laboratory analysis were performed by experienced medical laboratory technologists.
Data processing and analysis
The collected data were checked and cleaned before being entered and analyzed with SPSS version 26.0 software. Categorical data were summarized using frequencies and proportions. Continuous variables are presented as median and interquartile range (IQR). The chi-square test was used to test for statistically significant associations between two categorical variables. A binary logistic regression model was employed to determine the independent variables associated with hyperglycemia. The variables with p-values < 0.25 in the bivariable logistic regression analysis were incorporated into a multivariable logistic regression model to control for the effect of confounding variables. Crude and adjusted odds ratios with 95% CI are reported, and a p-value < 0.05 was considered statistically significant. Hosmer and Lemeshow tests were used to assess the goodness of fit of the final logistic model.
Definition of terms
Diabetes mellitus was defined as a fasting blood glucose level of ⩾126 mg/dl. 26
Hyperglycemia was defined as a fasting blood glucose level ⩾110 mg/dl.22,26,27
Prediabetes was defined as a fasting glucose level between 110 and 125 mg/dl.26,28
Dyslipidemia was defined according to the National Cholesterol Education Program Adult Treatment Panel III guidelines as having LDL-C levels of ⩾130 mg/dl, total cholesterol (TC) levels of ⩾200 mg/dl, triglycerides (TG) of ⩾150 mg/dl, and high-density lipoprotein cholesterol (HDL-C) levels of < 40 mg/dl for men and < 50 mg/dl for women, either in isolation or in combination. 29
Hypertension was defined as systolic BP ⩾ 140 mmHg and/or diastolic BP ⩾ 90 mmHg. 30
BMI was classified as underweight (<18.5 kg/m2), normal weight (18.5–24.9 kg/m2), overweight (25–29.9 kg/m2), and obese (⩾30 kg/m2). 31
Waist circumference: a normal WC is ⩽80 cm for females and ⩽94 cm for males, according to WHO categorization. Abnormal WC was defined as WC >80 cm for females and >94 cm for males. 32
Waist-to-hip ratio: a normal WHR is <0.90 for males and <0.85 for females, according to WHO categorization. Abnormal WHR was defined as WHR ⩾ 0.9 in males and ⩾0.85 in females. 32
Viral load: VL ⩽ 1000 copies/ml was categorized as suppressed, and VL > 1000 copies/ml was categorized as nonsuppressed. 33
CD4+ T-cell count: a CD4+ T-cell count of ⩾500 cells/mm3 is within the normal range for a competent immune system and a CD4+ T-cell count of <500 cells/mm3 indicates a compromised immune system 34
Adherence to ART: an adult’s recent adherence to ART is considered poor if they take less than 85% of the prescribed dose, fair if they take 85%–94%, and good if they take 95% or more of the dose. 35
Opportunistic infections refer to the list of opportunistic diseases recorded in the national comprehensive HIV prevention, care, and treatment guidelines. 35
Sufficient physical exercise: adults should perform at least 150–300 min of moderate-intensity aerobic physical activity, or at least 75–150 min of vigorous-intensity aerobic physical activity, or an equivalent combination of moderate-intensity and vigorous-intensity activity per week and otherwise insufficient. 36
Smoking status: “smoker” for participants who had smoked at least one cigarette within the last 1 year.37,38
Alcohol drinking status: “alcohol drinker” for participants who consumed any type of alcoholic beverage more than once per week in the past year regardless of the amount.39,40
Results
Sociodemographic characteristics of the participant
Among the 423 participants, 73.3% were female. The median age of the study participants was 41 years (IQR: 37, 49), with 43.5% of the participants aged between 31 and 40 years. Among the participants, 51.8% lived in rural areas, 37.6% could not read and write, and 35.7% were farmers (Table 1).
Sociodemographic characteristics of the study participants.

Students, drivers, and pensioners.
ETB, Ethiopian birr.
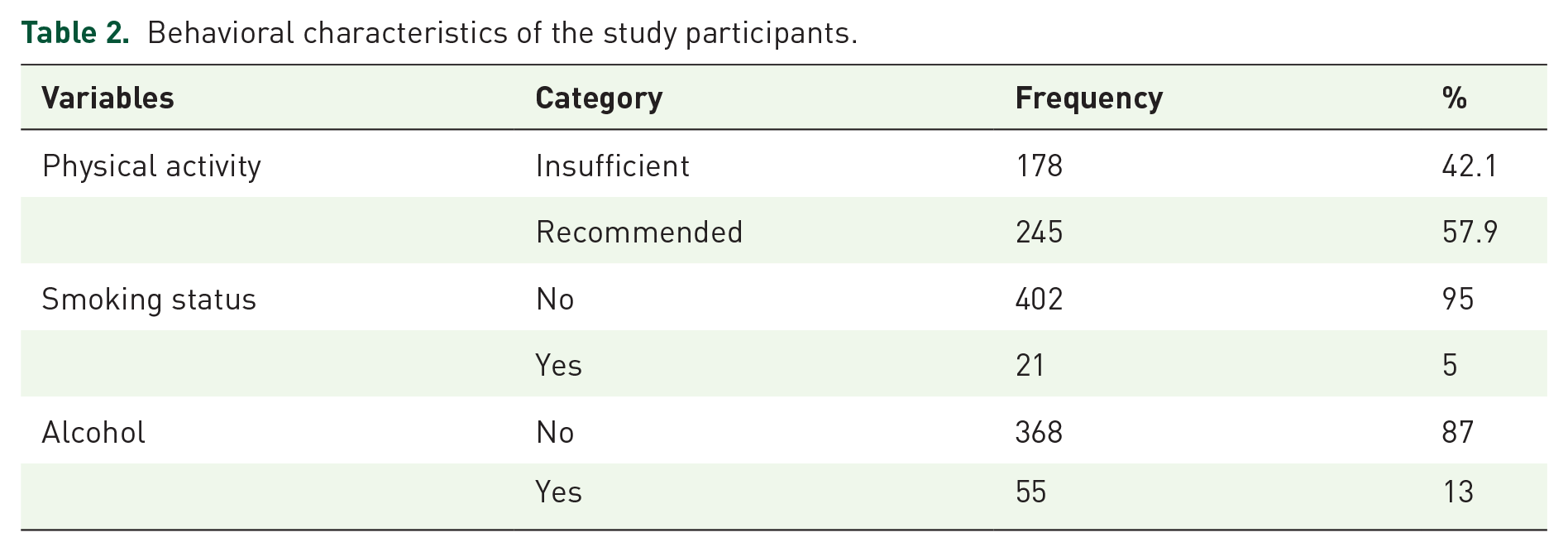
Behavioral characteristics of the participant
About 13% of the participants had a history of alcohol consumption, 5% had a history of smoking cigarettes, and 42.1% had insufficient physical activity (Table 2).
Behavioral characteristics of the study participants.
Clinical characteristics of the participants
Nearly half of the participants (49.6%) had been living with HIV for more than 7 years and 56.5% had been using ART for more than 5 years. A total of 60.3% of the participants had been using DTG-based ART for at least 2 years, 53.9% had CD4+ T-cell counts <500 cells/mm3, 6.6% had a history of opportunistic infections in the last 6 months, and 11.3% had a family history of DM (Table 3).
Clinical characteristics of the study participants.

ART, antiretroviral therapy; CD4, cluster of differentiation 4; CVD, cardiovascular disease; DM, diabetes mellitus; DTG, dolutegravir; HIV, human immunodeficiency virus; OIs, opportunistic infections; WHO, World Health Organization.
Anthropometric and biochemical characteristics
A total of 25.8% and 10.2% of the patients were overweight and obese, respectively. A total of 22.9% had increased WC, 34.75% had increased waist-to-hip ratios, 8.5% had increased BP, and 61.2% had low HDL-C levels (see Table 4).
Anthropometric and biochemical characteristics of the study participants.

<40 mg/dl for men and <50 mg/dl for women.
BMI, body mass index; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglyceride.
Hyperglycemia among PLWH on dolutegravir-based ART
Among the 423 study participants, 51 had fasting blood glucose levels ⩾110 mg/dl, resulting in an overall prevalence of hyperglycemia of 12.1% (95% CI: 9.2–15.1) as indicated in Figure 1.

Prevalence of hyperglycemia among PLWH on DTG-based ART at DMCSH.
Among these individuals, 8.5% (36/423) were identified as prediabetics, while 3.6% (15/423) were identified as diabetics.
Factors associated with hyperglycemia among PLWH on dolutegravir-based ART
Age, gender, residence, physical activity, alcohol consumption, VL, WHO clinical stage, duration of HIV/AIDS diagnosis, duration of DTG-based ART, family history of DM, BMI, waist-to-hip ratio, TC, and TG levels had a p-value ⩽ 0.25. However, in the multivariable logistic regression, age (AOR = 1.04, 95% CI: 1–1.08, p = 0.036), BMI (AOR = 1.09, 95% CI: 1.01–1.17, p = 0.022), and TG level (AOR = 2.44, 95% CI: 1.28–464, p = 0.006) were predictors of hyperglycemia among PLWH on DTG-based ART (Table 5).
Factors associated with hyperglycemia among PLWH on dolutegravir-based ART at DMCSH.

Statistically significant at p < 0.05.
AOR, adjusted odd ratio; ART, antiretroviral therapy; BMI, body mass index; COR, crude odd ratio; DM, diabetes mellitus; DMCSH, Debre Markos Comprehensive Specialized Hospital; DTG, dolutegravir; PLWH, people living with HIV; WHO, World Health Organization.
Discussion
This study was designed to determine the prevalence of hyperglycemia and its associated factors among PLWH on DTG-based ART. The overall prevalence of hyperglycemia among PLWH on DTG-based ART was 12.1% (95% CI: 9.2–15.1). About 8.5% (36/423) had prediabetes, while 3.6% (15/423) had DM. We also found that age, BMI, and TG levels were significant predictors of hyperglycemia among PLWH on DTG-based ART.
The prevalence of DM in our study was comparable to the 2021 International Diabetes Federation (IDF) report, 41 which indicated a national prevalence of 3.3% among the adult population in Ethiopia, as well as to the 2016 WHO report, 42 which noted a national prevalence of 3.8% of DM in the general population of Ethiopia. The prevalence rate of hyperglycemia in this study was consistent with other published data from the USA 16 and Central Uganda, 19 which reported prevalences of 13% and 12.8%, respectively. However, the prevalence of hyperglycemia in this study was higher than that reported in a study conducted at a regional referral hospital in Uganda (7.3%). 20 The observed variation could be due to differences in sociodemographic and lifestyle characteristics, genetic predispositions, study methodologies, and HIV and ART management protocols.19,43 For example, a study conducted at a regional referral hospital in Uganda included those who had been exposed to DTG-based ART for at least 12 weeks; however, our study included those who had been exposed to DTG-based ART for at least 6 months. These factors could explain the discrepancy.
On the other hand, the prevalence of hyperglycemia in this study is lower than the previous findings reported in Eastern Uganda (19.8%), 18 Northeast Ethiopia (17.2%), 22 and Southwest Ethiopia (35.9%). 23 The observed discrepancies may be attributed to several factors. For instance, variations in the ART exposure history among participants could play a role, as our study included individuals with prior ART experience, while the studies conducted in Northeast Ethiopia and Eastern Uganda focused on ART-naïve participants. In addition, there was a difference in sample sizes; studies from Eastern Uganda, Southwest Ethiopia, and Northeast Ethiopia used a smaller sample size, whereas our study used a larger sample size. Furthermore, differences in blood glucose testing methods may have contributed to the discrepancies; we used fasting blood sugar tests, while the study from Southwest Ethiopia used random blood sugar tests.
Our results support earlier evidence from case reports, case series, and randomized controlled trials that indicate a relationship between DTG and disrupted glucose metabolism.13,14,44,45 The exact mechanism through which DTG induces disrupted glucose metabolism is not fully known, but it is speculated that DTG triggers insulin resistance by chelating magnesium ions, which are required as cofactors for insulin to operate effectively.16,17
Age, BMI, and TG levels were found to be significantly associated with hyperglycemia in PLWH receiving DTG-based ART. For every year of age increase, patients were 4% more likely to have hyperglycemia. This finding aligns with previous investigations in Uganda, 19 Iran, 46 and Malawi. 47 The possible reason could be the age-related deterioration of pancreatic islet cell function and increased insulin resistance, which in turn increases the likelihood of developing hyperglycemia. 48 Prior research has also indicated that the risk of insulin resistance increases as PLWH continue to live longer while on ART. 34
BMI was also another predictor of hyperglycemia among PLWH on DTG-based ART. For a kg/m2 increase in BMI, the odds of hyperglycemia among DTG-treated patients increased by 9%. This finding is supported by research from Zimbabwe, 49 Ethiopia, 50 and Senegal 51 and could be attributed to the fact that increased BMI causes insulin resistance in body cells, resulting in hyperglycemia. 49 Weight gain has been shown to have a greater effect on the risk of hyperglycemia in PLWH than in the general population. 52 Moreover, some studies have shown that using DTG leads to increased weight gain, 53 but the potential long-term metabolic implications of this outcome remain incompletely understood. Growing data suggest that DTG-associated weight gain leads to an increased risk of hyperglycemia, hypertension, and metabolic syndrome, along with increased cardiovascular risk. 54
In addition, TG levels were predictors of hyperglycemia among PLWH on DTG-based ART. The odds of having hyperglycemia were 2.44 times more likely among those who had a TG level ⩾150 mg/dl as compared to those who had a TG level < 150 mg/dl. This finding is supported by studies carried out in Malaysia, 55 Ethiopia, 25 and Nigeria. 56 A possible explanation could be that hypertriglyceridemia can increase insulin resistance in peripheral tissues. 57 The metabolites of TGs, such as free fatty acids, diacylglycerol, and others, can regulate insulin signaling pathways through the activation of several serine/threonine kinases, which suppress insulin receptor and tyrosine phosphorylation of insulin receptor substrates, resulting in peripheral insulin resistance.58,59
Strengths and limitations
Regarding strength, this is one of the first studies in Ethiopia that attempted to assess hyperglycemia among PLWH receiving DTG-based ART, hence ultimately adding to the limited data and laying the groundwork for future studies. Despite this strength, this study has several limitations. As a cross-sectional study, we cannot establish causal relationships between hyperglycemia and the factors. In addition, the self-reported responses for certain items may be influenced by recall bias due to their subjective nature. Furthermore, participants’ baseline fasting blood glucose measurements were unavailable because they were not part of routine clinical practice in Ethiopia. The study also lacked data on participants' use of lipid-lowering or BP medications, which could potentially confound the observed prevalence of hyperglycemia. Moreover, because the study population was drawn from a single institution and blood glucose levels were determined using a one-time sampling method, the results should be interpreted with caution.
Conclusion
Overall, our study revealed a high prevalence of hyperglycemia (12.1%) among PLWH receiving DTG-based ART at the ART clinic of a hospital in Northwest Ethiopia. Age, BMI, and TG levels were significant predictors of hyperglycemia among PLWH on DTG-based ART. These findings underscore the importance of monitoring blood glucose levels in PLWH receiving DTG-based ART, with a special emphasis on patients with advanced age, increased BMI, and increased TG levels. In addition, given the widespread utilization of DTG-based ART, health policies should encourage glucose monitoring as a basic aspect of HIV care. Furthermore, we propose that researchers conduct a large-scale prospective cohort study to determine cause–effect relationships.
Footnotes
Acknowledgements
First, we would like to thank the Debre Markos University for giving us the chance to perform this research. We are also grateful to the DMCSH for providing permission for data access authorization to enable us to conduct the study. We would like to express our heartfelt gratitude to our study participants for their voluntary participation in the study and success of the study.