
Abstract
Background:
Infectious and parasitic diseases (IPDs) encompass a broad range of illnesses predominantly associated with poverty. They are more prevalent in low- and middle-income countries, including Brazil, where they continue to be among the leading causes of mortality.
Objective:
This study aims to analyze the spatiotemporal dynamics of mortality due to IPDs in Brazil from 2000 to 2019.
Methods:
We conducted an ecological study using data on mortality by IPDs from the Brazilian Mortality Information System. We applied the segmented log-linear regression model to assess temporal trends. For spatial analysis, we used the local empirical Bayesian estimator and Moran indices. Retrospective spatiotemporal scan statistics were performed using the Poisson Probability Distribution Model.
Results:
Between 2000 and 2019, there were 2,155,513 deaths related to IPDs in Brazil. The leading causes of death included acute respiratory infections (n = 1,130,069; 52.49%), septicemia (n = 289,817; 13.46%), human immunodeficiency virus/acquired immunodeficiency syndrome (n = 232,892; 10.82%), tuberculosis (n = 104,121; 4.84%), and neglected tropical diseases such as Chagas disease (n = 94,788; 4.40%) and schistosomiasis (n = 10,272; 0.48%). An increasing temporal trend in the mortality rate from IPDs was observed in Brazil and across all its regions. Additionally, our spatiotemporal scan identified high-risk clusters of death in the Southeast and Northeast regions.
Conclusion:
Mortality from IPDs remains a significant public health concern in Brazil, with an increasing trend observed in all regions. Our findings underscore the urgent need for comprehensive intersectoral public policies. These policies should focus on a greater allocation of resources and investments in the most critical areas, aiming to significantly reduce the number of deaths, particularly in the most vulnerable regions.
Plain language summary
This study focuses on deaths caused by infectious and parasitic diseases (IPDs) in Brazil from 2000 to 2019. These diseases include conditions like acute respiratory infections, septicemia (a severe blood infection), HIV/AIDS, tuberculosis, and neglected tropical diseases such as Chagas disease and schistosomiasis. Our research aimed to understand the patterns and trends in deaths due to these diseases across different regions in Brazil. We found that between 2000 and 2019, there were over 2.1 million deaths due to IPDs in Brazil. The most common causes of death were respiratory infections, septicemia, and HIV/AIDS. The study showed that deaths from these diseases are increasing across the country, with significant high-risk areas identified in the Southeast and Northeast regions. We used various methods to analyze the data, including spatial analysis to identify regions with high death rates. This helped us to see where the most significant problems are and where resources are most needed. The study highlights the urgent need for targeted public health policies and resource allocation to reduce the number of deaths from these diseases, particularly in the most affected areas. It also underscores the importance of ongoing monitoring and intervention to address this critical public health issue. By understanding these patterns, health officials and policymakers can better plan and implement strategies to prevent and control infectious diseases, ultimately saving lives and improving public health across Brazil.
Introduction
Infectious and parasitic diseases (IPDs) represent a broad spectrum of illnesses caused by pathogenic agents, such as viruses, bacteria, fungi, protozoa, helminths, and other parasites. Over many centuries, these diseases have been among the leading causes of death worldwide, significantly shaping the global epidemiological landscape.1,2 Despite a notable decline in morbidity and mortality from these diseases in many countries, thanks to advancements in prevention and control measures, such as improved sanitation and the development of vaccines and antibiotics, IPDs remain a serious global public health concern, particularly in developing countries.1,2
IPDs are closely linked to poverty and higher socio-economic vulnerability.3,4 The World Health Organization (WHO) reports that in 2019, IPDs were responsible for over five million deaths worldwide, primarily in low- and middle-income countries in Latin America, Africa, and Asia. 4 Moreover, six of the top 10 causes of death in low-income countries are attributable to these diseases, including malaria, tuberculosis (TB), and human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS). 4
In South America, Brazil is significantly impacted by IPDs. These diseases continue to be prevalent across much of the country, 5 especially in areas with high social vulnerability, such as the North and Northeast regions, 6 and the peripheral areas of major metropolises in the Southeast. 7 Infectious diseases like TB 8 and neglected tropical diseases (NTDs) such as schistosomiasis and Chagas disease 9 contribute to high morbidity and mortality, posing substantial challenges to the national health system.
The global health threat of IPDs is exacerbated by human, political, and socio-environmental factors, which have intensified over the last few decades. The occurrence and spread of these diseases are influenced by rapid global interconnection, significant demographic, climatic, and socio-environmental changes, and disparities in access to health, education, and sanitation commonly found in vulnerable populations.1,10,11 Consequently, conditions conducive to the spread of infectious and parasitic agents and failures in prevention and control measures have emerged, leading to new diseases like COVID-19 and the resurgence of previously controlled diseases like measles.1,10,11
Interestingly, many IPDs in Brazil exhibit significant spatial heterogeneity. In this context, geographic information systems can support health services by identifying spatial dynamics and mortality rates associated with these diseases.12,13 Understanding these geographic dynamics aids in planning more effective, region-specific prevention and control strategies. Additionally, monitoring the spatiotemporal evolution and impacts of these diseases can assist in identifying high-risk mortality clusters and formulating targeted public health policies. 13
Moreover, the attention to several IPDs in the country has been minimized due to the COVID-19 pandemic, which has severely impacted the indicators of various diseases nationwide.14–16 Consequently, a comprehensive analysis of the epidemiological landscape of IPDs in Brazil, prior to the pandemic, is crucial for accurately interpreting the spacetime patterns and impacts of these diseases. Therefore, this study aims to assess the spatiotemporal dynamics of mortality due to IPDs in Brazil, covering the two decades before the emergence of the COVID-19 pandemic.
Methods
Type and study design
A population-based ecological study utilizing spatiotemporal analysis techniques was conducted. The study encompassed all deaths related to IPDs in Brazil from 2000 to 2019. This timeframe was chosen based on the implementation of a new version of the Mortality Information System (SIM) in Brazil from 1999 onward. The updated system introduced a revised death declaration (DD), leading to enhanced data recording accuracy, particularly in the detailed completion of the DD. 17 Furthermore, the study period concluded in 2019 to preclude potential distortions in the interpretation of the results due to the COVID-19 pandemic, which began in 2020. This approach allows for a focused analysis of pre-pandemic data, ensuring more consistent and comparable results across the investigated period.
Study area
Brazil, the largest country in South America, covers an area of 8,515,767.049 km2 and has a population of approximately 203 million, ranking it as the fifth most populous nation globally. Politically and administratively, Brazil is divided into 27 federative units (26 states and 1 Federal District), with Brasilia as the capital. For political and operational purposes, these units are grouped into five regions (North, Northeast, Southeast, South, and Central-West), each exhibiting distinct geographic and cultural characteristics 18 (Figure 1). The analysis considered all five regions and the country’s 5570 municipalities. Brazil is marked by significant social inequalities and is endemic for several IPDs, including leprosy, Chagas disease, and schistosomiasis.9,12

Study area: map of Brazil divided into its five regions and into 26 states and one Federal District.
Data source
Data on deaths from IPDs were sourced from the SIM of the Brazilian Ministry of Health. The SIM is integral to the collection, storage, and management of death records in Brazil, using the DD as a standard document completed by medical professionals for all deaths in the country. It’s important to note that SIM data is publicly available on the website of the Department of Informatics of the Unified Health System (DATASUS). The data was obtained using codes from the International Classification of Diseases, 10th Revision (ICD-10): A00-B99, G00-G04, H65-H66, J00-J06, J09-J18, J20-J22, and N70-N73.4,19
Population data were acquired from the Brazilian Institute of Geography and Statistics (IBGE), based on the 2000 and 2010 population censuses and estimates for the intercensal years (2001–2009 and 2011–2019). 20 The digital cartographic mesh of Brazil (divided by states and regions) was extracted in shapefile format from the IBGE website.
Variables and measures
The variables analyzed in this study included:
(a) The number of deaths from IPDs in the 5570 municipalities of Brazil;
(b) Crude mortality rates from IPDs, calculated by dividing the number of deaths by the exposed population and multiplying the result by 100,000 inhabitants for each municipality, state, and region. These rates were also computed according to sex and age group.
Exploratory data analysis
The epidemiological variables used in the descriptive analysis were sex (male and female), ethnicity/color (white and non-white), age group (0–9 years, 10–19 years, 20–39 years, 40–59 years, and 60 years or older), years of education (less than 8 years and 8 years or more), and cause of death (according to the ICD-10 code). These categorized variables were described for Brazil and its regions using absolute and relative frequencies.
Time trend analysis
Temporal trends were analyzed using crude mortality rates from IPDs according to the regions of Brazil, sex, and age group. The Joinpoint linear regression model (segmented linear regression) was employed. 21 This method identified changes in trend data over time, adjusting the data to a time series with the minimum number of joinpoints (zero indicates a line without inflection points), and tested the statistical significance of including additional joinpoints.21,22
The best model was selected using the Monte Carlo permutation method, considering p-value < 0.05 and 95% confidence intervals (95% CI). Annual percentage changes (APCs) and their respective 95% CI were calculated to describe and quantify the trends. When more than one significant inflection point was detected, the average annual percentage change (AAPC) was calculated. Trends were deemed significant if APCs had a p-value of <0.05 and their 95% CI did not include zero. Positive, significant APCs indicated an increasing trend; negative, significant APCs indicated a decreasing trend; and non-significant trends were described as stable, irrespective of APC values.21,22
Spatial and spatiotemporal analysis
Choropleth maps of Brazil were generated for spatial and spatiotemporal analyses, illustrating mortality from IPDs across two distinct periods: Period 1 (2000–2009) and Period 2 (2010–2019). This division into temporal intervals enables a clearer visualization and understanding of the mortality landscape from these diseases over the past two decades in Brazil.
Initially, crude mortality rates were utilized in the analysis. However, to reduce instability caused by random case fluctuations, the local empirical Bayesian estimator was employed. This model smoothed the crude rates using weighted averages, resulting in a new corrected coefficient that more accurately reflects the epidemiological scenario. This method helps reduce data fluctuations in smaller areas. A key advantage of Bayesian rates is the increased influence of neighboring municipalities, enhancing regional coherence in the results. 23 For ease of visualization, both raw and smoothed rates were displayed on thematic maps stratified into five equal interval categories: (a) <1, (b) 1–20, (c) 21–40, (d) 41–60, (e) >60 deaths per 100,000 inhabitants.
Subsequently, crude mortality rates were used to calculate the Global Moran Index to investigate the presence of spatial autocorrelation in mortality from IDPs. This index assesses the presence of spatial patterns in data distribution. Moran’s Global Index, ranging from −1 to +1, estimates the correlation of a variable’s values at different locations. Values near 0 suggest no spatial autocorrelation; positive values (0 to +1) indicate positive spatial autocorrelation, where high-value areas are near other high-value areas and vice versa; negative values (−1 to 0) suggest negative spatial autocorrelation, where high-value areas are near low-value areas. 23
Upon detecting autocorrelation, local autocorrelation was examined using the Local Moran Index (Local Spatial Association Index – LISA), identifying spatial dependence patterns. A dispersion diagram was then created with the following spatial quadrants: Q1 (high/high) and Q2 (low/low), indicating municipalities with values similar to their neighbors and positive spatial association; Q3 (high/low) and Q4 (low/high), indicating municipalities with different values from their neighbors and no spatial association. Results were deemed significant at p-value < 0.05 and were depicted in Moran maps.23,24
Finally, spatiotemporal analysis was conducted to identify and evaluate high-risk spatiotemporal clusters of deaths from IPDs. We used the number of deaths from IPDs in the 5570 municipalities of Brazil, along with the population data of these municipalities for the years under study. Clusters were identified using scanning statistics (SaTScan) with a retrospective space-time analysis type, employing the Poisson probability distribution model. The parameters included a one-year aggregation time; no geographic or temporal overlap of clusters; circular clusters; a maximum spatial cluster size of 50% of the population at risk; and a maximum temporal cluster size of 50% of the study. 25
Clusters were detected using the log-likelihood ratio (LLR) test, and relative risks (RR) of mortality for each cluster compared to its neighbors were calculated. Results with a p-value of<0.05 were considered significant, based on 999 Monte Carlo simulations, and represented in maps and tables. 25
Software used
Microsoft Office Excel 2017 was used for data tabulation and descriptive analysis. Joinpoint Regression Program 5.0.2 was used to analyze the time trend. TerraView 4.2.2 was used to perform spatial analysis and QGis 3.28.7 assisted in creating choropleth maps. SaTScan™ 9.6 (Martin Kulldorff, Boston, MA, USA) was used to perform the spatiotemporal scan.
Ethical considerations
This study used public domain secondary data that did not contain any personal identification and followed national and international ethical recommendations, such as the rules of the Helsinki Convention and Resolution 466/2012 of the National Health Council (CNS).
Results
A total of 2,155,513 deaths related to IPDs were registered in Brazil between 2000 and 2019. A total of 2716 cases (0.13% of records) were excluded as they did not have a municipal allocation. The regions that presented the highest percentages of deaths were the Southeast (n = 1,113,008; 51.70%) and the Northeast (n = 487,520; 22.65%), together representing 84.35% of the total deaths from IPDs in the country. When analyzing sociodemographic characteristics in Brazil, we found higher mortality among men (n = 1,157,992; 53.79%), white people (n = 1,155,777; 53.69%), individuals aged 60 years or older (n = 1,332,190; 61.88%) and those with less than 8 years of schooling (n = 1,197,355; 55.62%). Interestingly, in the North, Northeast, and Central-West regions there was a predominance of deaths among non-white people (73.57%, 61.15%, and 51.92%, respectively) (Table 1).
Sociodemographic characteristics of infectious and parasitic diseases deaths in Brazil, 2000–2019.
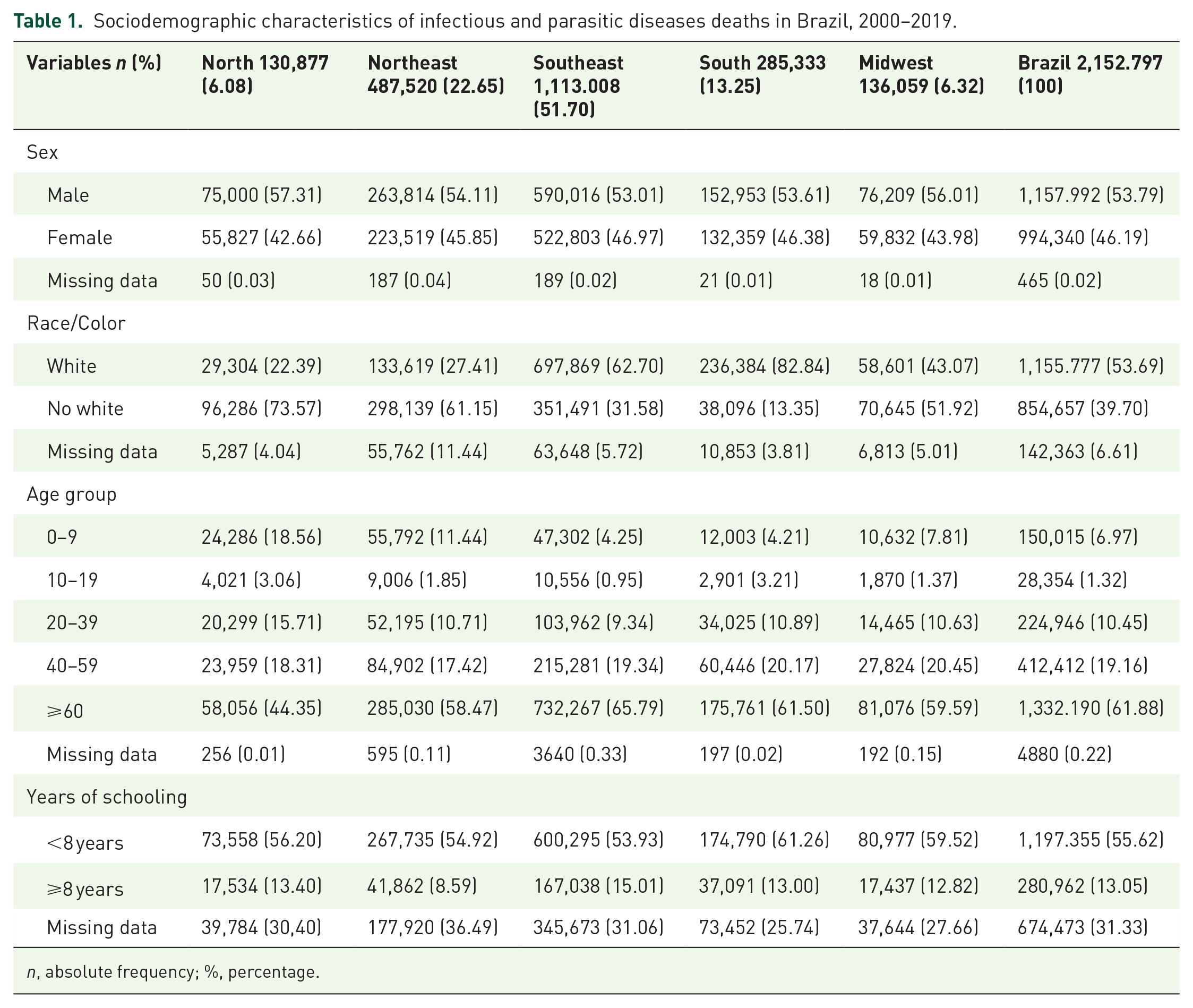
n, absolute frequency; %, percentage.
Notably, acute respiratory infections were the main cause of death related to IPDs in Brazil (n = 1,130,069; 52.49%). Furthermore, other important causes of death were septicemia (n = 289,817; 13.46%), HIV/AIDS (n = 232,892; 10.82%), TB (n = 104,121; 4.84%), and intestinal infections and parasites (n = 104,060; 4.83%). NTDs, such as Chagas disease (n = 94,788; 4.40%) and schistosomiasis (n = 10,272; 0.48%), have assumed a prominent position as significant causes of mortality in Brazil and its regions (Table 2).
Main causes of death from infectious and parasitic diseases in Brazil and regions, 2000–2019.

n, absolute value; %, percentage.
Table 3 illustrates the temporal trends in mortality rates from IPDs across Brazilian regions, genders, and age groups. An increasing trend was observed nationally, with an AAPC of 2.1 (95% CI = 1.8 to 2.4; p-value < 0.05). This upward trend was also seen in all regions, most notably in the Northeast (AAPC = 3.2; 95% CI = 2.8 to 3.6; p-value < 0.05) and the South (AAPC = 2.1; 95% CI = 1.6 to 2.6; p-value < 0.05), surpassing the national increase. Furthermore, an increase in mortality rates was found in both genders, with females experiencing the highest growth (AAPC = 2.8; 95% CI = 2.5 to 3.1; p-value < 0.05). A decreasing trend in mortality rates was noted across all age groups except for the elderly (>60 years), who saw a significant rise (AAPC = 2.3; 95% CI = 1.9 to 2.7; p-value < 0.05).
Temporal trends in infectious and parasitic diseases mortality rates by region, sex, and age group in Brazil, 2000–2019.

p-Value < 0.05.
APC, annual percentage changes; AAPC, average annual percentage changes.
Regarding the spatial distribution of crude mortality rates from IPDs, the first period (2000–2009) revealed high mortality areas dispersed throughout all regions. However, smoothed rates indicated that high mortality rates were primarily concentrated in Southeastern municipalities. In the second period (2010–2019), there was a marked increase in high mortality areas for both crude and smoothed rates, predominantly in the Southeast, Central-West, Northeast regions, and a substantial portion of Rio Grande do Sul (South region). Notably, there was an increase in municipalities with high mortality rates (>60/100,000 inhabitants), from 551 in the first period to 2290 in the second period (Figure 2(a) and (b)).

Spatial analysis of mortality from infectious and parasitic diseases in Brazil, in two time periods. (a) Crude mortality rate and (b) smoothed mortality rate.
Positive and significant spatial autocorrelation was identified in both periods analyzed (Period 1: I = 0.4495, p-value = 0.001; Period 2: I = 0.5651, p-value = 0.001), underscoring spatial dependence in mortality from IPDs among Brazilian municipalities. Clusters of high-risk municipalities, especially in the Southeast region, were observed (high/high—in red) (Figure 3(a)), along with an increase in the number of affected locations (Period 1 = 836; Period 2 = 920).

Spatial analysis of mortality from infectious and parasitic diseases in Brazil, in two time periods. (a) Moran Map (LISA cluster) and (b) spatiotemporal scanning analysis.
The spatiotemporal analysis detected 13 statistically significant high-risk mortality clusters in the first period and 11 in the second (Figure 3(b) and Table 4). The primary clusters for periods 1 (2005–2009) and 2 (2015–2019) both had a relative risk of 1.41, encompassing 1521 and 1533 municipalities in Espírito Santo, Minas Gerais, São Paulo, Rio de Janeiro, Paraná, Goiás, and Mato Grosso do Sul, respectively. Secondary clusters were found in the North and Northeast states. It is also crucial to note that most identified clusters were situated in the Northeastern states (Period 1 = 7 clusters; Period 2 = 6 clusters) (Figure 3(b) and Table 2).
Spatiotemporal scan analysis of mortality from infectious and parasitic diseases in Brazil, 2000–2019.
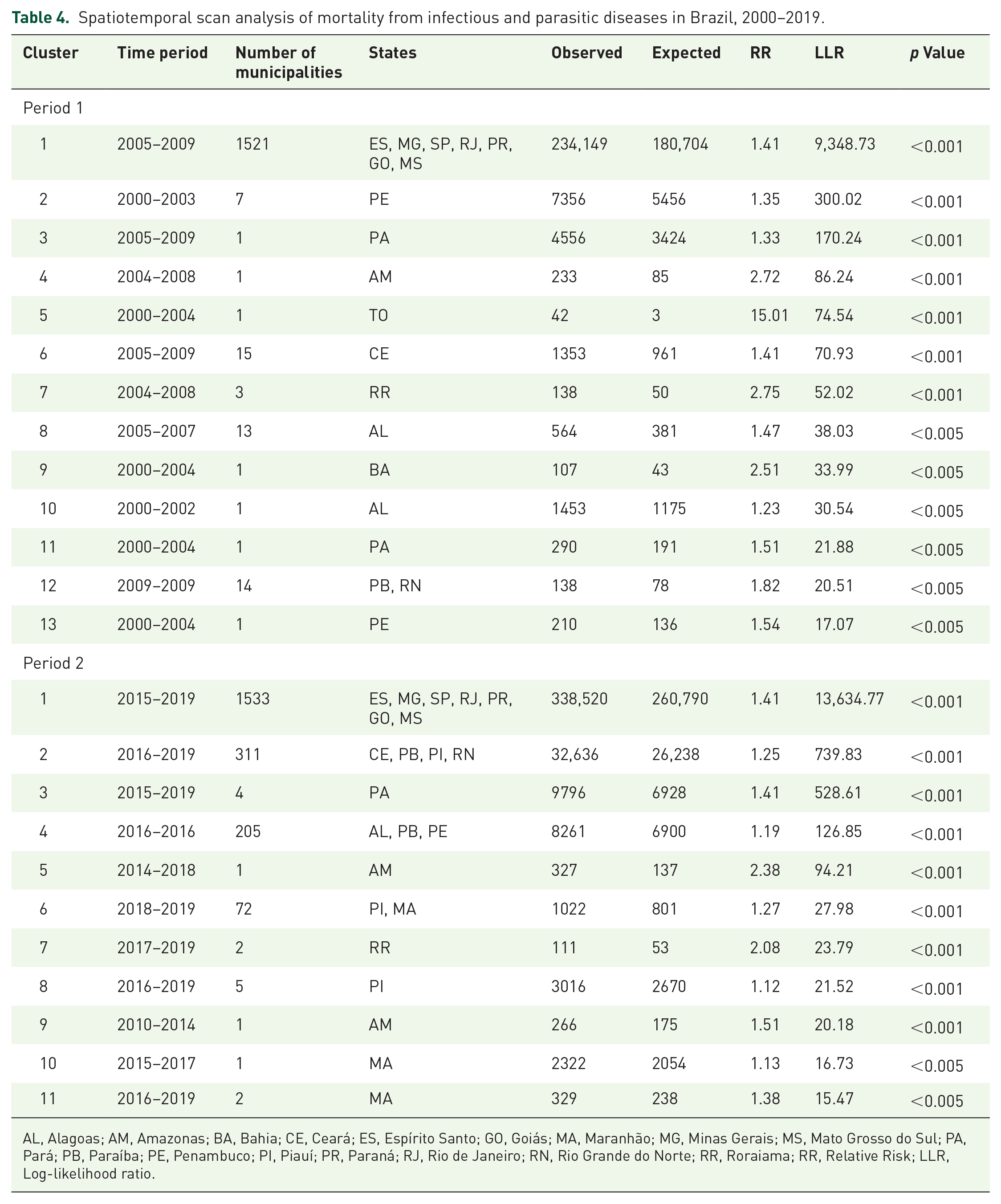
AL, Alagoas; AM, Amazonas; BA, Bahia; CE, Ceará; ES, Espírito Santo; GO, Goiás; MA, Maranhão; MG, Minas Gerais; MS, Mato Grosso do Sul; PA, Pará; PB, Paraíba; PE, Penambuco; PI, Piauí; PR, Paraná; RJ, Rio de Janeiro; RN, Rio Grande do Norte; RR, Roraiama; RR, Relative Risk; LLR, Log-likelihood ratio.
Discussion
To our knowledge, this is the first study to evaluate mortality due to IPDs over a 20-year series in Brazil. We observed a significant uptick in mortality rates from IPDs during the study period, with an increasing temporal trend across all regions. Notably, preventable and treatable diseases such as acute respiratory infections, HIV, TB, intestinal infections and parasites, Chagas disease, viral hepatitis, and schistosomiasis were among the leading causes of death. Regions with substantial social vulnerability, particularly the Northeast and North, experienced the highest rates of increase. These findings paint a concerning picture where IPDs continue to pose a serious public health challenge and are a prominent cause of mortality across vast regions of Brazil.
Brazil’s socioeconomic progress and improved living conditions have significantly altered health standards, indicative of an epidemiological transition. 26 This transition, particularly in developing countries, is characterized by heightened life expectancy and a proportionate decline in infectious disease morbidity and mortality. 27 However, low- and middle-income regions grapple with a dynamic and complex reality, contending with the enduring prevalence of IPDs against a backdrop of pronounced social inequality.3,4
The rise in IPD mortality rates identified in our study echoes the ongoing epidemiological situation in Brazil. Despite considerable advancements in disease control through expanded sanitation, housing improvements, and public health measures—including universal vaccination, timely diagnosis and treatment, and primary healthcare access28,29—several persistent factors hinder the full reduction of IPD mortality.
Brazil’s complexity is marked by varied geographic, socioeconomic, and cultural traits, and it stands as one of the most unequal nations globally. Such disparity leads to significant socioeconomic gaps. In many areas, individuals endure substandard living conditions, including unhealthy, overcrowded housing, insufficient basic sanitation, and restricted healthcare access.30,31 These conditions foster environments susceptible to IPDs, contributing to the escalating mortality rates from these diseases in the country.
It is critical to emphasize that advancements in controlling IPDs in Brazil have been uneven. While some diseases, such as those preventable by vaccines and diarrhea in children, have seen significant reductions in morbidity and mortality, others have only achieved partial control, like HIV and TB, or have not seen similar progress, such as respiratory infections in adults and the elderly. 5 This corroborates our findings, where the leading causes of IPD-related deaths included acute respiratory infections, septicemia, HIV, and TB. Furthermore, certain intestinal infections, parasites, and NTDs like Chagas disease and schistosomiasis continue to be prevalent.
The high mortality from respiratory infections may be attributed to several factors, including increased life expectancy leading to a larger elderly population more vulnerable to these infections, coupled with inadequate vaccination coverage. 32 Additionally, regional air pollution and climatic conditions conducive to the spread of respiratory pathogens, 33 the overuse of antibiotics with subsequent bacterial resistance, 34 and healthcare system strains during infection outbreaks 35 all contribute to this issue. These infections are also a common cause of sepsis, 36 which could be linked to the significant proportion of septicemia-related deaths identified in our study.
Furthermore, addressing TB and HIV, and their complex interplay, remains a formidable challenge for Brazil. 37 The nation continues to report high rates of TB and TB-HIV co-infections, 38 with increasing co-infection rates posing substantial barriers to reducing morbidity and mortality from these diseases. 37 HIV not only increases the number of TB cases but is also a primary factor in the rising mortality of co-infected patients.37,38 Additionally, disparities in access to timely diagnosis and treatment, along with the heightened vulnerability of specific demographic groups like those living in extreme poverty, the homeless, and drug users, further challenge morbidity and mortality reduction efforts in Brazil.37,39
Our findings align with prior research that has observed elevated mortality rates from NTDs such as Chagas disease and schistosomiasis in Brazil.9,12 The chronic nature of Chagas disease contributes to high mortality, and even with reduced transmission, mortality rates diminish slowly.9,40 For schistosomiasis, factors like population migration, the widespread presence of intermediate hosts, and poor sanitary conditions in socioeconomically vulnerable areas contribute to its persistence and the rise of new outbreaks, subsequently increasing mortality rates. 9
Understanding epidemiological distribution is crucial for the prevention and control of IPDs. 11 Our gender-based analysis revealed more deaths among men, yet the most significant growth in mortality rates was among women. Typically, men engage in behaviors that exacerbate these diseases and often delay seeking healthcare until later stages, negatively impacting their survival. 40 Meanwhile, the rising participation of women in traditionally male-dominated occupations may have increased their exposure to infectious agents, contributing to the rise in IPD morbidity and mortality among women. 13
In terms of age demographics, there was a declining trend in IPD mortality rates among younger populations, while a higher and increasing mortality rate was observed in the elderly. The reduction in younger age groups, especially in children, can be linked to successful control measures for historically prevalent diseases in Brazil, including immunization-preventable diseases and gastrointestinal infections like measles, diarrhea, rotavirus, and cholera.5,28,29 Such success is attributed to widespread vaccination, the dissemination of oral rehydration therapy, and increased access to clean water.5,29 Conversely, the substantial mortality and its rise among those over 60 years can be partly ascribed to increased life expectancy and the growing elderly demographic. Aging is associated with immune senescence, which heightens susceptibility to infections and the likelihood of severe complications. 41
The dynamics of mortality in Brazil exhibit significant heterogeneity, shaped by regional and social development disparities. These disparities are deeply rooted in the social, economic, political, and cultural fabric, giving rise to varied mortality landscapes.26,42 Prior research has also pointed to regionalization and heterogeneity concerning various IPDs across the nation.6,12,13 Our findings underscore the pronounced spatial variation in IPD-associated mortality among different Brazilian regions.
The spatial analysis techniques employed in this study revealed high-risk mortality zones for IPDs, notably in the Southeastern states. Our spatio-temporal scan pinpointed a primary high-risk death cluster encompassing much of the Southeast and parts of Paraná (South), Goiás, and Mato Grosso do Sul (Central-West). Secondary clusters were identified in the Northern and Northeastern states. These findings are in agreement with previous studies that located higher death concentrations from certain IPDs in the Southeast12,43 and Northeast.12,13
Remarkably, the Southeast, despite being a developed region, suffers from acute socioeconomic inequalities. Rapid and often haphazard urbanization has led to the proliferation of impoverished communities on the outskirts of major cities, where residents grapple with substandard living conditions, overcrowding, inadequate sanitation, irregular water supply, and garbage collection,31,44 compounded by limited healthcare access. 44 The region’s high population density further facilitates the swift transmission of various infectious agents. 7
Conversely, the Northeastern region faces a high mortality risk from NTDs like Chagas disease and schistosomiasis, exacerbated by marked social inequities. With the lowest human development indices and the highest social vulnerability, 30 many inhabitants, especially in remote rural locales, endure challenges in accessing healthcare. Living in extreme poverty, without basic sanitation or clean water, 45 these communities are persistently vulnerable to infection and death from these diseases.
Socio-environmental determinants are pivotal in shaping the health outcomes of populations, particularly concerning the mortality risk from infectious and parasitic diseases. An understanding of the natural history and transmission dynamics of these diseases is crucial to grasp their community impact. 6 Yet, our study uncovers a troubling trend in Brazil, where IPDs have been a major mortality cause over the past two decades, with rising mortality rates across all regions. This constitutes a severe public health issue demanding prompt and strategic intervention. Notably, the COVID-19 pandemic has negatively influenced the prevention and control of many such diseases in Brazil, potentially exacerbating morbidity and mortality in the coming years and intensifying the public health challenge.14–16
Our study is not without limitations. The reliance on secondary data could lead to underreporting or exaggeration of the analyzed variables’ values. Additionally, the ecological nature of the study means that the group-level findings may not accurately represent individual-level realities. Despite these limitations, our findings provide valuable insights into the spatio-temporal trends of IPD mortality in Brazil. They can underpin the formulation of targeted public policies and interventions aimed at disease control and mortality reduction, particularly in higher-risk areas.
Conclusion
Our research indicates that mortality due to IPDs is a critical public health issue in Brazil. Notable diseases contributing to mortality include acute respiratory infections, septicemia, HIV, TB, and NTDs such as Chagas disease and schistosomiasis. A concerning increasing trend in IPD mortality across all Brazilian regions was particularly pronounced in the Northeast. It is noteworthy that the most significant increases in mortality were among women and the elderly. Through spatial analysis and spatiotemporal scanning, we identified a heterogeneous distribution of IPD mortality, with the Southeast and Northeast regions being the most prominent areas of risk.
Given these alarming trends, there is an imperative for the swift enactment of comprehensive intersectoral public policies that span Brazil’s entire territory, tailoring strategies to regional needs. These policies should ensure enhanced resource allocation and strategic focus on preventing and controlling these diseases, concentrating efforts on the most critical areas to substantially reduce mortality rates, with particular attention to the regions most afflicted.