
Abstract
Background:
The risk of infection following cesarean delivery is 5–20 times higher than that following normal delivery, contributing to 10% of pregnancy-related mortality. In 2019, Mbarara Regional Referral Hospital (MRRH) performed cesarean section for 40% of deliveries, surpassing the WHO’s recommended 15%–20%. The availability and provision of effective prophylactic antibiotics are crucial in preventing surgical site infections (SSIs).
Objectives:
To determine the prevalence and predictors of SSIs among mothers after cesarean section, length of hospital stay, and antibiotic use at MRRH.
Design:
This was an observational retrospective study conducted in the maternity ward of the MRRH.
Methods:
Data on the diagnosis of SSI, length of hospital stay, and antibiotic use were extracted and entered into EpiData software version 3.1 and analyzed using STATA version 15. We conducted logistic regression analysis to identify factors independently associated with SSIs. We also compared the length of hospital stay.
Results:
The prevalence of post-cesarean SSIs was 7.9% (95% CI: 6.3%–9.9%). Mothers aged 25 years and younger were less likely to develop SSIs (adjusted odds ratio (aOR): 0.53, 95% CI: 0.30–0.93; p = 0.027). Those with more than six pregnancies were more likely to develop SSIs (aOR: 3.4; 95% CI: 1.35–8.58; p = 0.009). The median length of stay was 8 days for mothers who developed an SSI (interquartile range (IQR): 5, 16) and 3 (IQR: 3, 4) days for those who did not (p < 0.001). Prophylactic antibiotics were prescribed to 83.4% of the women (95% CI: 80.7–85.8). Ampicillin (88.2%) was the most prescribed prophylactic antibiotic, and metronidazole was the most prescribed postoperatively (97.8%) and at discharge (77.6%).
Conclusion:
The current prevalence of post-cesarean SSIs is higher in Uganda than in developed countries. Older age and having had more than six pregnancies are independent predictors of SSIs, and post-cesarean SSI significantly prolonged hospital stay.
Introduction
Surgical site infections (SSIs) develop within 30 days of surgery or 1 year of implant placement and appear to be related to the surgery. 1 They affect up to 66% of patients after surgery and occur up to nine times more frequently in developing countries than in developed countries. 2 SSIs contribute to 14%–25% of all hospital acquired infections. 3 SSIs are of great concern to healthcare practitioners because they increase morbidity, mortality, and financial burden on the patient and necessitate cost-effective management within the healthcare system. 4
Cesarean section is a life-saving procedure; however, in settings lacking facilities to manage complications, it poses a risk of disability, and even death. 5 Mothers who deliver via cesarean section have a 2- to 20-fold higher risk of infection than those who deliver via spontaneous vaginal delivery. 6 Obstetric infection is the second most common cause of maternal mortality, followed by postpartum hemorrhage, and it increases the risk of prolonged hospital stay and patient costs.7,8 At the Mbarara Regional Referral Hospital (MRRH), there are more than 11,000 deliveries annually. 9 Out of 2151 deliveries, 865 (40%) were by cesarean section between January 1 and March 31, 2019, which is greater than the 15%–20% recommended by the WHO. Therefore, it is important to determine the prevalence and predictors of SSIs.
Factors associated with the prevalence of SSIs among mothers after cesarean section include age, parity, obesity, preexisting remote body site infection, contaminated or dirty wounds, colonization with microorganisms, and diabetes mellitus.6–8 Cesarean delivery is an independent risk factor for postpartum infection. 9 Rational prophylactic antibiotic use reduces the risk of postoperative infections, lowers costs, and saves nursing time following cesarean delivery.10,11 Single prophylactic antibiotic use is as effective as multiple antibiotic use. 10
The incidence of SSIs after surgery varies from place to place, with less than 3.0% in Germany and France; 16.9% in Rio de Janeiro, Brazil; and 26.0% in Mwanza, Tanzania. 11 SSI surveillance and providing feedback to the surgical team have been shown to reduce the prevalence of SSIs and the cost incurred. 12
In Uganda, data on SSI in the Obstetrics and Gynecological ward are still scarce; its prevalence and associated length of stay among mothers after cesarean section are not known. Research on the incidence of SSI in the surgical ward at MRRH in 2017 revealed a postoperative incidence density of 15.9% compared with an incidence of 16.4% in 2014. 1 This demonstrated insignificant reduction in the rate of SSIs at the MRRH surgery ward. This study aimed to determine the prevalence and predictors of SSIs, as well as the length of stay among mothers after cesarean section in the Obstetrics and Gynecology wards of MRRH.
Methods
We reported our study according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement checklist for observational studies (version 4.0).
Study setting, design, period, and population
A retrospective observational study was conducted in the maternity ward of the MRRH between April 1 and May 31, 2020, using the patient records from January 1 to March 31, 2019. Of the women who underwent cesarean section during the study period, 865 of them were eligible for selection. Information on the diagnosis of SSI, length of stay, and antibiotics used by the patients were extracted from the patient charts.
Sample size and sampling procedure
Using the Epi Info™ software, developed by Centers for Disease Control and Prevention in Atlanta, Georgia, in the United States, we calculated a sample size of 842 using a prevalence of 16.4% from a previous study at the MRRH 1 and a two-sided margin error of 2.5%. After adding 5% for illegible or incomplete files, 884 patient files were considered for eligibility and enrollment. Thus, we included 849 patient charts with complete information from the 865 patient files available for consideration. Sixteen files were excluded because of incomplete information. The sample size was sufficient to estimate the prevalence of SSI in women after cesarean section at MRRH.
Sampling technique
During the study period, a consecutive sampling method involving all the patient charts of women who underwent cesarean section sampling at the MRRH was used. Patients diagnosed with preoperative infectious disease, patients with urinary or respiratory tract infections, patients already taking antibiotics, and patients who underwent surgery at another hospital and were later hospitalized at MRRH were excluded from the study.
Study outcomes
Primary outcome
The primary outcome was a documented diagnosis of SSI in patient charts by an obstetrician, senior house officer (SHO), or medical officer (MO). SSI included all wound infections, necrotizing fasciitis, and endometritis that were linked to or occurred at the same time as the cesarean section, even if there was no evidence of bacteria. 13 Wound infections manifested as erythema, discharge, and incision induration. We formulated a data collection sheet to extract the relevant data.
Secondary endpoints
The length of hospital stay was measured as the number of days between hospital admission and discharge. Treatment charts were also used to extract data on antibiotic use, specifically prophylaxis, post-cesarean delivery, and discharge. The drug name, dose, route of administration, frequency, and duration were recorded.
Variables of the study
The dependent variable was SSI as documented in the patient chart. The secondary endpoint, length of hospital stay, was defined as the number of days from admission to discharge from the hospital.
In this study, the independent variables for predicting SSIs were the patient sociodemographic characteristics (e.g., age, marital status, religion, parity), clinical characteristics (e.g., parity, gestational age), surgery-related factors (e.g., type of cesarean, operator), and antibiotic-related factors (e.g., prophylactic antibiotic use, post-antibiotic use, name of antibiotic, indication of antibiotic use, duration of prophylaxis or treatment, and adequacy of the antibiotic dose).
Data collection tool and procedure
Two nurses with Bachelor’s degrees in nursing and three trained midwife nurses collected data by reviewing the records of 849 patients using a pretested checklist. The checklist consisted of sections on sociodemographic data, clinical characteristics, post-cesarean SSI diagnosis, and antibiotic use. We directly obtained demographic data from the patients and extracted data on prescribed antibiotics from their hospital files. The recorded variables included the diagnosis of SSI by the obstetrician, SHO, or MO as documented in the patient files; sex; age in years; marital status; dates of admission; and dates of discharge. The importance of admission time to the time of discharge helped determine the length of stay. We collected data on commonly prescribed antibiotics by recording the name of the prescribed antibiotic from the patient chart or file along with its dose, frequency, and duration. These included prophylactic antibiotics, post-cesarean antibiotics, and antibiotics administered upon discharge.
Data quality control
We pretested the data checklist using 10% of a similar population at the MRRH to ensure completeness and appropriateness. Midwives trained as research assistants collected data under the supervision of the principal investigator. The data were checked daily for completeness and consistency. We double-entered the data, stored it on a password-protected computer to prevent data manipulation, maintained quality and patient confidentiality, and regularly backed the data up to prevent loss. We maintained the data quality by double-entering the results and securing them with a lock and key.
Data management and analysis
Data were coded, entered, checked, and cleaned using EpiData software (version 3.1), developed in Mukilteo, the United States, and exported to STATA version 15 for analysis. Descriptive statistics were computed to determine the percentage of mothers with SSIs after cesarean. We used the Mann–Whitney U test to compare the length of hospital stay between the groups. Frequencies and proportions were used to describe the antibiotic name, route of administration, dose, frequency of administration, and duration of administration. We used univariate and multivariate regression analyses to identify the factors associated with SSIs and account for the potential confounding effect of these infections. Factors that showed p values ⩽0.20 in the bivariate model were included in the multivariate logistic regression model. We determined the level of significance at 95%, and p-values less than 0.05 denoted statistical significance.
Results
General characteristics of the mothers after cesarean section at MRRH
Overall, 865 of 2151 deliveries involved cesarean section at the MRRH between January 1 and December 31, 2019. This study included 849 mothers who provided complete information (Figure 1).
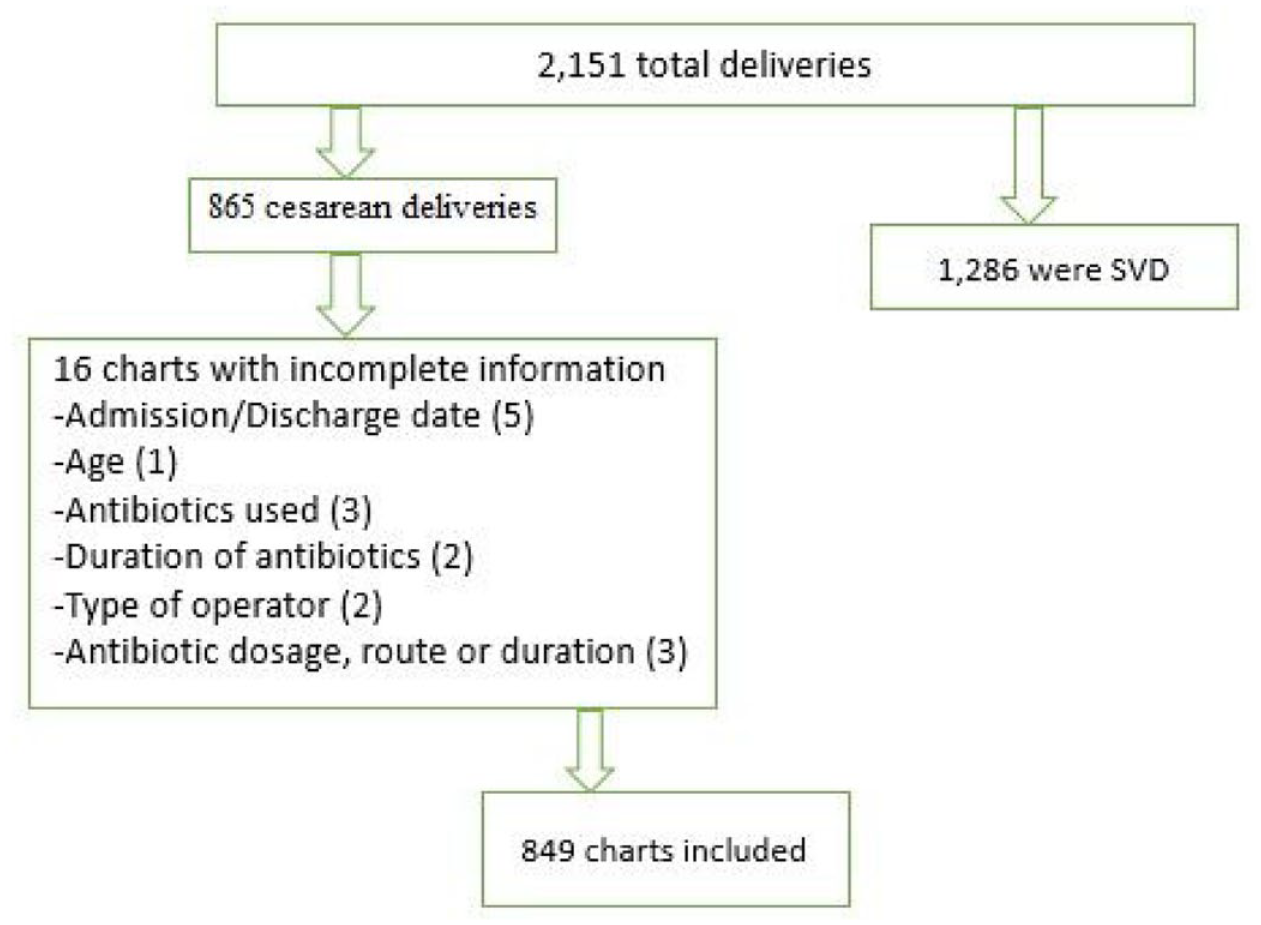
A flowchart showing the inclusion and exclusion of patient medication charts.
Table 1 summarizes the general characteristics of the 849 participants studied. The median age of the mothers was 25 years (interquartile range (IQR): 21, 29). Most were married (595, 70.1%) and had between one and four pregnancies (719, 84.7%). Most women underwent surgery on emergency terms (785, 92.5%), mainly by SHOs (711, 84.0%). The median length of hospital stay was 3 days (IQR: 3–4) (Table 1).
Sociodemographic characteristics of mothers who underwent cesarean section at MRRH in 2019.
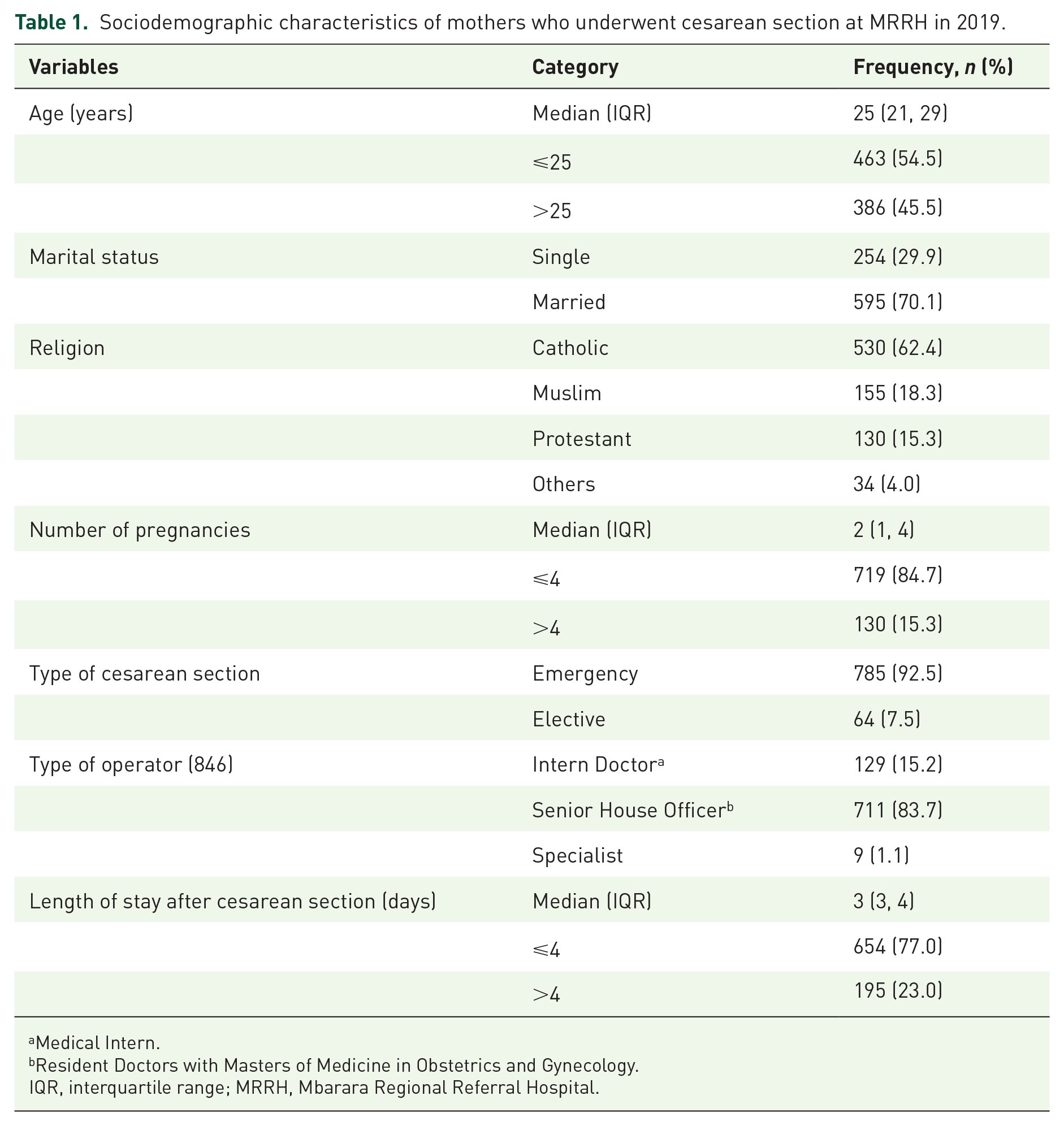
Medical Intern.
Resident Doctors with Masters of Medicine in Obstetrics and Gynecology.
IQR, interquartile range; MRRH, Mbarara Regional Referral Hospital.
Prevalence of SSIs
Sixty-seven out of 849 mothers had a chart diagnosis of deep or superficial SSIs, translating into a prevalence of 7.9% (95% CI: 6.3–9.9), as shown in Figure 2.

Occurrence of SSIs in mothers after cesarean section at the MRRH in Uganda.
Factors associated with SSIs
Univariate analysis showed that only the number of pregnancies was significantly associated with SSIs (p = 0.049). Factors with p-values of ⩽ 0.25 were used for the multivariate logistic regression, which showed that mothers aged 25 years or younger were less likely to develop SSIs (adjusted odds ratio (aOR): 0.53, 95% CI: 0.30–0.93; p = 0.027). The mothers with more than six pregnancies were also more likely to develop SSIs (aOR: 3.4; 95% CI: 1.35–8.58; p = 0.009) than those with six or fewer pregnancies. The results are presented in Table 2.
Univariate and multivariate analysis for predictors of SSIs (N = 849).
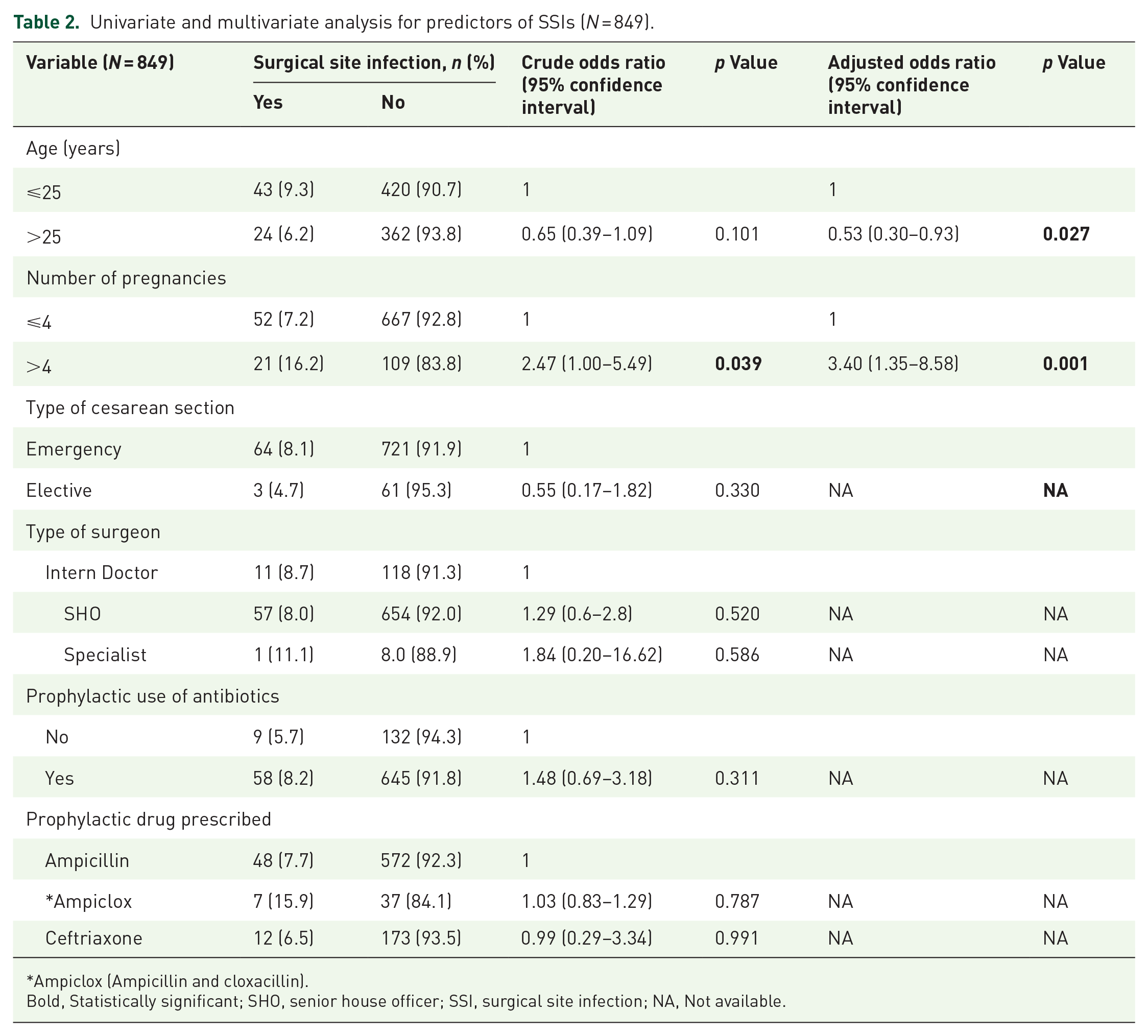
Ampiclox (Ampicillin and cloxacillin).
Bold, Statistically significant; SHO, senior house officer; SSI, surgical site infection; NA, Not available.
Length of hospital stay
The median length of hospital stay for all participants was 4.3 days. The median number of days spent in the hospital by mothers who developed SSIs after cesarean section was 8 (5, 16) days, compared with 3 (3, 4) days for those who did not. The Mann–Whitney U test showed that this median difference in the length of hospital stay was statistically significant (p < 0.001) (Figure 3).

Lengths of hospital stay of mothers with and without SSIs after cesarean section at MRRH, Uganda.
Prophylactic antibiotic use among mothers after cesarean section at MRRH
Antibiotics were used for prophylaxis by 83.4% (95% CI: 80.7–85.8) of the mothers who had undergone cesarean section at MRRH in 2019. All drugs were administered intravenously. The most commonly administered antibiotic was ampicillin (88.2%), followed by ampiclox (6.3%) and ceftriaxone (5.5%) (Table 3).
Prophylactic antibiotic use among mothers after cesarean section at MRRH.
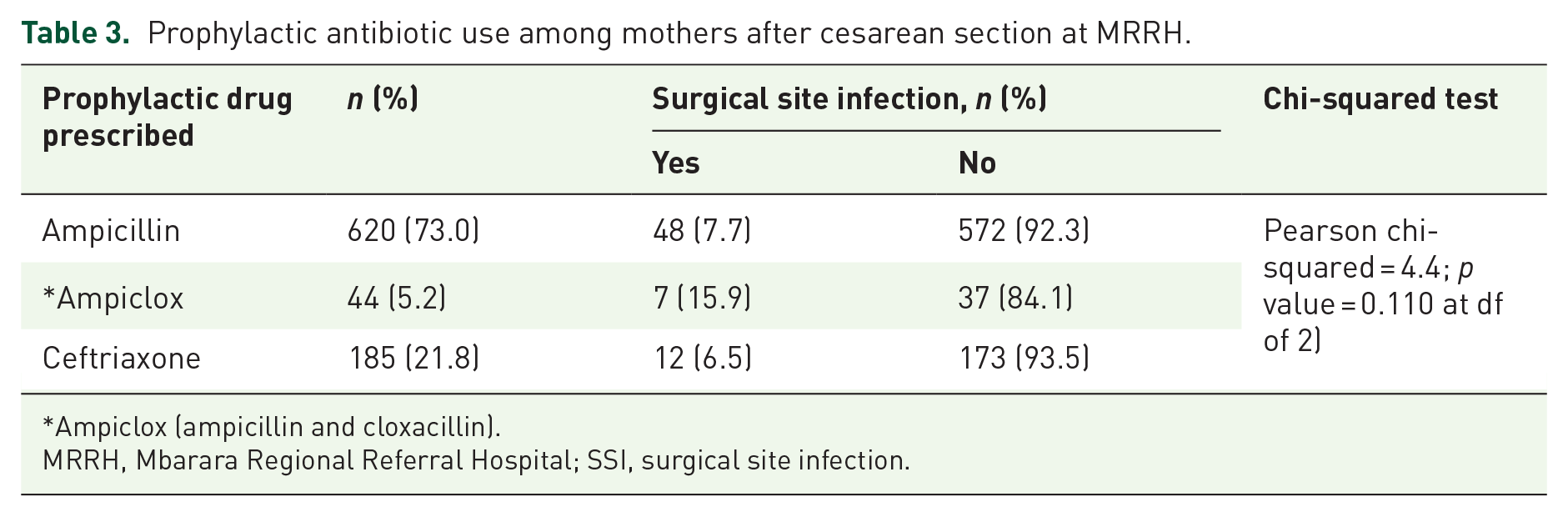
Ampiclox (ampicillin and cloxacillin).
MRRH, Mbarara Regional Referral Hospital; SSI, surgical site infection.
Post-cesarean antibiotic use and antibiotics on discharge
Intravenous metronidazole was the most commonly prescribed antibiotic after surgery (97.8%), followed by ceftriaxone (94.6%), ampicillin-cloxacillin (6.2), and other antibiotics (including flucamox, cefotaxime, ampicillin, ampicillin, and cefixime) (Figure 4).

Antibiotics prescribed after cesarean section at MRRH, Uganda.
Oral metronidazole was the most commonly prescribed antibiotic upon discharge, with a prescription frequency of 77.6%. It was followed by cefixime (39.5%), ampiclox (19.9%), flucamox (flucloxacillin and amoxicillin; 13.5%), and others (5.1%) (Figure 5).

Antibiotics prescribed at discharge for mothers after cesarean section at the MRRH, Uganda.
Discussion
The prevalence of SSIs was 7.9% in the study. This surpassed the prevalence reported in two Tanzanian hospitals, which was less than 3%.12,14 This disparity may be attributed to differences in socioeconomic status and health delivery systems. 15 The availability and provision of effective surgical prophylactic antibiotics, as well as the overall quality of surgical and obstetric services, may differ across facilities and countries. 16
Our results are in agreement with those of a multi-country study across sub-Saharan African countries including Burundi, the Democratic Republic of the Congo, Sierra Leone, and Ethiopia, which found the prevalence of post-cesarean SSIs to be between 7.3% and 9.4%.7,8,17
However, the current prevalence is lower than those reported by other studies from low and middle income countries: 15% in Ethiopia, 18 19.4% in Tanzania, 12 and 14.4% in the Jordanian University Hospital. 19 Differences in study settings and participants may explain this variation. The lower prevalence rate could also be due to differences in SSI definition, distribution of risk factors among the studied populations, study time, study location, sample size, socioeconomic status, and healthcare delivery system, which varies from place to place. 18 The incidence may also have differed due to the postoperative hospital stay, antibiotic prophylaxis, and aseptic techniques. 14 Closed-incision negative-pressure wound therapy (ciNPWT) has been introduced as a prophylactic intervention to reduce cesarean section wound complications but with inconclusive evidence. 20
Regarding factors independently associated with SSIs, our study showed that women aged 25 years and younger were approximately 47% less likely to develop SSI than those older than 25 years. This finding is in agreement with that of a study by Zejnullahu et al. that showed that the likelihood of developing SSIs was higher among women older than 35 years. 19 Other studies have also reported that increased age is independently associated with SSIs.21,22 Patient immunity may decline with age, which increases the risk of SSI. 19 Our results showed that mothers with six or more pregnancies were 3.4 times more likely to have SSIs than those with fewer than six pregnancies. This finding aligns with those of a previous study. 22
The median length of the participants was 4.3 days. The median number of days spent in the hospital by mothers who developed SSIs after cesarean section was 8 days, compared with the median of 3 days for those who did not. This was comparable with the report of a study in Mwanza, Tanzania, which reported that patients with post-cesarean SSIs had a longer length of hospital stay—12.7 days compared with 4.0 days. 14 Similarly, another study in India reported longer hospital stays for patients with SSIs and revealed that it was an important independent predictor of SSIs.23,24 In contrast, the prolongation of hospital stay may be due to SSIs. 24 As they require medication and review by healthcare workers before discharge, patients with SSIs stay in the hospital longer. The longer hospital stay of patients with SSIs increases the bed occupancy rate, morbidity, and mortality, and more than 1.4 million people suffer from complications of infections acquired in the hospital. 23
Prophylactic antibiotic use was observed in 83.4% of mothers who underwent surgery at the MRRH. The most commonly administered prophylactic antibiotic was intravenous ampicillin (88.2%). Ampicillin is recommended for surgical prophylaxis by the Uganda Clinical Guidelines (2016), which may explain its widespread use. This finding is similar to that of a study conducted in Ethiopia, which found that 92% of mothers received prophylactic antibiotics, most of whom received intravenous ampicillin. 17 These results differ from those of an Ethiopian study in which 84% received ceftriaxone, 25 a South Sudan study in which 95% received cefuroxime, 25 and a South Sudan study in which 95% received cefuroxime. 6 Different antibiotic policies and prescription choices may have contributed to these differences.
Most doctors prescribe these drugs in combination, but intravenous metronidazole and ceftriaxone are the most commonly used post-cesarean antibiotics. These findings are consistent with the report of a Tanzanian study in which the majority of patients received metronidazole and ceftriaxone. 26 In 2019, a systematic review examined preoperative and postoperative antibiotic use in sub-Saharan African countries and concluded that 100% of patients received ceftriaxone. 27 The results differ from those of a study in Ethiopia that reported that 70% of mothers received ampicillin after cesarean delivery 17 and another in Kosovo where 77.5% received cefazolin and ampicillin-cloxacillin postoperatively; however, the decision was guided by the hospital protocol, which explains the difference. 19 However, the Uganda Clinical Guidelines (2016) do not recommend routine postoperative antibiotic administration for most surgeries, because it wastes limited resources, causes unnecessary side effects for the patient, and can lead to antimicrobial resistance. However, the Uganda Clinical Guidelines recommend a course of antibiotics during procedures involving contaminated and dirty or infected wounds.
Limitations of the study
The limitations of this study include its retrospective design, as some information was not in the files, and some SSIs developed after 30 days. Some important information was missing from the medical charts of the patients, such as information on comorbidities, body mass index, time of administration of prophylactic and post-cesarean antibiotics, and surgery-related factors (e.g., type of surgical drains used, operation duration, and type of anesthetic used). Information on the classification and management of SSIs was lacking. However, the estimation of prevalence at a 2.5% margin of error is an important strength.
Conclusion
The study concluded that the incidence of SSIs among mothers after cesarean section was higher than that in developed countries but within the range reported by studies conducted in Sub-Saharan Africa. Independent predictors of SSIs were increasing age and more than six pregnancies. Mothers with post-cesarean SSIs had significantly longer median hospital stays than those without SSIs. Ampicillin was the most commonly prescribed prophylactic antibiotic, whereas metronidazole was the most commonly prescribed after surgery and on discharge. We suggest creating and implementing protocols to reduce the number of SSIs that occur after cesarean section. These protocols should include new methods of dressing wounds, such as ciNPWT and prophylactic wound vacuum therapy. These should be considered preventative measures to lower the number of cesarean section wound complications in high-risk mothers, such as those who are older or have had more than six pregnancies. We recommend good wound surveillance and infection control for all mothers who deliver via cesarean section. Post-cesarean antibiotics should only be used when indicated, such as for contaminated, dirty, or infected wounds, or other risk factors. A large-scale prospective cohort study should be conducted to better understand the prevalence and interventions after 30 days of treatment.
Footnotes
Appendix
Acknowledgements
The authors would like to acknowledge the MRRH for making data available. The authors thank the midwives who participated in the data collection and their appreciation goes to Dr. Francis Bajjunirwe, who assisted with the conceptualization of the research idea.