
Abstract
Background:
Isolated native tricuspid valve infective endocarditis remains a challenging disease to treat given the large number of patients with substance use disorder. There is limited data on the optimal treatment strategy and the impact of a multidisciplinary endocarditis program on outcomes for this population.
Objectives:
To assess the clinical outcomes associated with management of native tricuspid valve infective endocarditis by a multidisciplinary team.
Design:
Single-center, retrospective cohort study.
Methods:
Patient cases were identified from the registry of the institutional multidisciplinary endocarditis team. Patients with left-sided endocarditis, multivalvular endocarditis, prosthetic tricuspid valves and cardiac implantable electronic devices were excluded.
Results:
Between September 7th, 2021 and February 1st, 2024 72 consecutive patients with isolated native tricuspid valve infective endocarditis were identified. Sixty-six (91.7%) patients were managed medically. Five patients underwent percutaneous mechanical aspiration of tricuspid valve vegetations and one patient underwent tricuspid valve replacement during the index hospitalization. In-hospital mortality was 1.4% and 90-day mortality was 2.8%. Nineteen (26.4%) patients discharged before medically advised and 25% were re-admitted within 30 days. Ten (13.9%) patients underwent elective tricuspid valve replacements after outpatient follow-up.
Conclusion:
Among 72 patients with isolated native tricuspid valve infective endocarditis managed by a multidisciplinary endocarditis program over a 2.5-year period, in-hospital, 90-day mortality and 1-year mortality were very low despite low rates of percutaneous mechanical aspiration and tricuspid valve surgery. Multidisciplinary follow-up can lead to elective tricuspid valve surgery in a delayed fashion.
Background
Right-sided infective endocarditis (RSIE) comprises 5%–10% of all infectious endocarditis (IE) in adults.1–6 The tricuspid valve is involved in 90% of all RSIE and isolated tricuspid valve infective endocarditis (TVIE) is predominantly associated with injection drug use (IDU) and cardiac implantable electronic devices (CIED).3–8 Many individuals in this population have co-morbid hepatitis C and/or HIV. 7 Other risk factors for isolated TVIE include congenital heart disease and central venous catheters.1–3,9–12
Patients with isolated TVIE have a more favorable prognosis with fever complications relative to left-sided IE. In-hospital mortality of TVIE is 5%–10% and previous data suggests that 80% of RSIE resolves with antibiotic therapy.2–4,6,12–14 This may be accounted for by the lack of systemic embolic complications, the ability of the cardiovascular system to tolerate significant tricuspid regurgitation, and the younger age of patients who use drugs (PWUDs).3,13,15 However, patients with TVIE remain at risk for serious complications including septic pulmonary emboli, hemoptysis, acute renal failure, and chronic right-sided heart failure. 10
Despite the high-reported rates of successful medical treatment of TVIE, the American Heart Association (AHA) still endorses several indications for cardiac surgery in this population. The 2015 AHA endocarditis guideline provides class IIa recommendations for valve surgery in patients with right sided infective endocarditis and: right heart failure secondary to severe tricuspid regurgitation with poor response to medical therapy, sustained infection caused by difficult-to-treat organisms, or lack of response to appropriate antimicrobial therapy, and tricuspid valve vegetations that are ⩾2.0 cm in diameter with recurrent pulmonary embolism despite antimicrobial therapy. 16 Unfortunately, there are no prosthetic valves that are specifically designed and approved by the Food and Drug Administration for surgical implantation in the tricuspid position. Additionally, without appropriate treatment of an underlying substance use disorder (SUD) many PWUDs who undergo tricuspid valve replacement will remain at risk for recurrent prosthetic TVIE, which is associated with increased morbidity. 17 Percutaneous mechanical aspiration (PMA) or vegetation removal has been utilized as an alternative or bridge to valve surgery in patients who may be considered high-risk for re-infection of a newly implanted prosthetic valve but have a clinical indication for procedural intervention to control infection or lower embolic risk. 18 However, recent data have suggested that PMA may have similar outcomes to medical treatment for TVIE. 19
In 2021, the University of Kentucky developed a multidisciplinary endocarditis program and adopted a standardized approach to patients with native TVIE that emphasized antibiotic therapy and addiction medicine consults as the primary treatment interventions. 20 Patients were then followed in a multidisciplinary fashion with delayed surgical intervention when their SUD was in remission and hemodynamic indications arose. Here, we report the demographics, management outcomes, and follow-up of patients from a single center diagnosed with definite isolated native tricuspid valve endocarditis and treated using this multidisciplinary and algorithmic approach (Figure 1).

Treatment pathway for patients with isolated native tricuspid valve endocarditis managed by the University of Kentucky multidisciplinary endocarditis team.
Patients and methods
Team protocol
In September 2021 University of Kentucky Healthcare (UK) created a multidisciplinary endocarditis team (MDET) and cardiovascular infectious diseases (CVID) consult service. The MDET is comprised of providers from infectious diseases, cardiac surgery, cardiology, addiction medicine, neurosurgery, neurology, physical medicine and rehabilitation, palliative care, and ethics. The group developed an internal protocol for medical treatment (Supplemental Figure 1) and formally meets weekly to discuss all inpatients with IE and document its recommendations in the electronic medical record. Cases for the conference are identified primarily by the infectious diseases consult service with collaboration with the cardiac surgery service. Frequent communication between MDET providers and clinical primary teams also occurs outside of scheduled meeting times. Decisions regarding PMA and valve replacement are made at the weekly conference. At our institution, PMA is generally considered only in patients with bacteremia lasting ⩾7 days, while on maximum medical therapy and provided all other foci of infection have been addressed. The CVID consult service is an interdisciplinary team housed in the division of infectious diseases and comprised of an attending physician, advanced practice provider, nurse navigator, pharmacist, and social worker. The CVID service consults on all inpatients with IE and follows them throughout their hospitalization and transition to outpatient. The CVID team coordinates the weekly MDET meetings and works with other specialties to coordinate follow-up and outpatient testing. 20
All patients, particularly those on intravenous or complex oral antibiotic regimens, are scheduled in the infectious diseases (ID) clinic within 2 weeks of discharge and to reduce the number of required follow-up appointments the ID clinic can prescribe medication for opioid use disorder (MOUD). The endocarditis nurse navigator performs a check-in phone call with all patients or their support systems within 48 h of discharge and interfaces closely with staff from other specialties to ensure that all teams relevant to the patients’ care needs are updated and involved in the clinical decision-making for the visit. Additionally, the divisions of cardiothoracic surgery and ID created a combined clinic where patients with TVIE see providers from both specialties in the same visit. 20 The CVID consult team meets weekly to review all patients who have been discharged and are scheduled for follow-up outpatient appointments that week. Our program’s practice is to have all patients with moderate or greater tricuspid valve regurgitation followed in the multidisciplinary clinic. Surgery is offered when the patients develop symptomatic right heart failure or progressive right ventricular dilation on transthoracic echocardiogram and when an individual’s SUD and social situation have stabilized.
Patient identification
Beginning in September 2021, a registry was created in the hospital’s electronic medical record of all of the patients presented at the weekly MDET conference. Institutional review board approval was obtained from the University of Kentucky and the requirement for informed consent was waived by the institutional review board, due to the retrospective nature of the work. The investigators subsequently established a database to collect each patient’s demographics, comorbidities, diagnostics, treatments, and outcomes data. A total of 414 patients were recorded in this database from September 2021 to February 2024. Only patients who met modified Duke criteria for definite native TVIE were included in this study. 21 Patients with left-sided IE (117), prosthetic valves (68), cardiac devices (11), and multivalvular IE (40) were excluded. An additional 106 patients who were presented at the MDET conference but met Duke criteria for possible or rejected IE were excluded (Figure 2). For patients who were not seen in follow-up additional chart review was taken to evaluate whether they were seen at other surrounding institutions to confirm their status at 90-days and 1-year post discharge (if available). There was no control group for this single-center, retrospective cohort study. The reporting of this study conformed to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 22

Study enrollment flowchart.
Definitions of terms
IDU was defined as active or recent IDU within 30-days of admission. SUD was defined as patients with IDU, individuals who endorsed non-intravenous drug use or were receiving MOUD. Hepatitis C infection was defined by the presence of detectable viral load by polymerase chain reaction testing during the index hospitalization.
Persistent bacteremia was defined as blood cultures that were positive for ⩾72 h after the initial positive culture. Heart failure secondary to IE was defined as new-onset or acute worsening of symptomatic heart failure during the index hospitalization as outlined by the New York Heart Association heart failure classification system during the index hospitalization. Acute renal failure was defined as patients initiated on renal replacement therapy during the index hospitalization.
Admissions for reinfection were defined as a new hospitalization within 30 days of discharge for IE. Duration of intravenous antibiotic therapy was defined as starting on the day of blood culture clearance.
Results
Study population
Between September 7th, 2021, and February 1st, 2024, 72 patients were identified with definite isolated native TVIE. The median age of patients was 34 years (25th–75th Interquartile range (IQR) 12.3 years) and 47.2% (34) were female (Table 1). Approximately 90% (64) of patients identified as white and 87.5% (63) endorsed a history of IDU within 30-days of admission. Seventy (97.2%) patients had a diagnosis of SUD. The most common pathogen was Staphylococcus aureus, which was identified in 60 (83.3%) patients. Over 40% (29) of patients had a prior admission for TVIE and 13.9% (10) had documented preexisting tricuspid regurgitation. For the 29 patients with a history of TVIE, 16 had ongoing IDU at the time of readmission, 10 left their previous hospitalizations before medically advised, two had suspected odontogenic sources of infection, and one patient was administratively discharged by the hospital during their previous admission. Fifty percent (36) of patients had active hepatitis C infection and 33% (24) had evidence of dental disease. There were three patients who were pregnant at the time of diagnosis.
Characteristics of patients with isolated, definite native tricuspid valve endocarditis treated by a multidisciplinary endocarditis team.
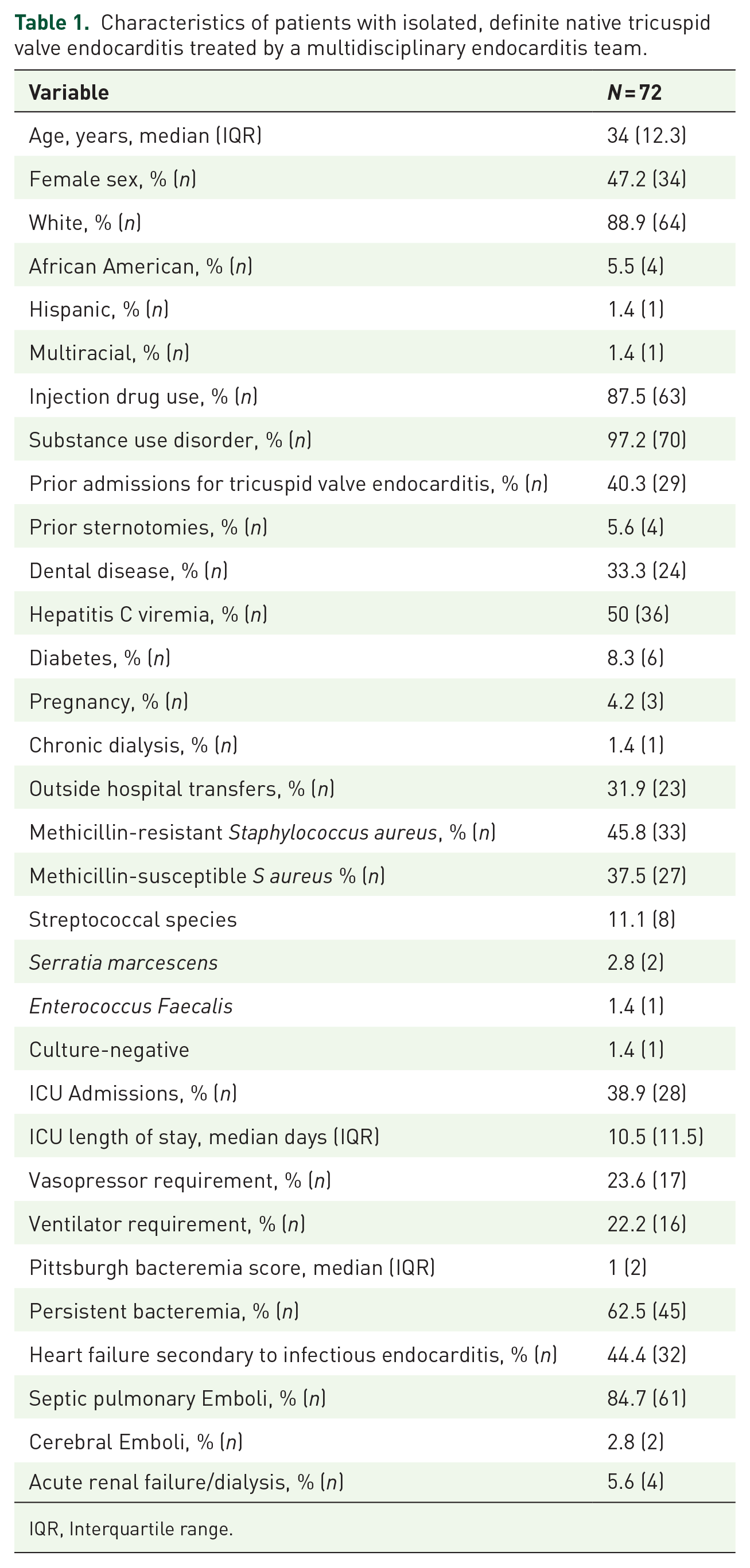
IQR, Interquartile range.
Complicating factors
Almost 1/3 (23) of patients were transferred from referring hospitals (Table 1) and 38.9% (28) of patients were admitted to the ICU at some point during their admission with a median stay of 10.5 days (IQR: 11.5 days). Rates of vasopressor and ventilator requirement were similar at 23.6% (17) and 22.2% (16), respectively. The median Pitt Bacteremia Score was 1 (IQR: 2). Forty-five patients (62.5%) had persistent bacteremia of ⩾72 hours duration and 44.4% (32) presented with new-onset or worsening symptomatic heart failure. Septic pulmonary emboli were identified in 84.7% (61) of patients and 5.6% (4) developed acute renal failure requiring renal replacement therapy.
In-hospital management
The CVID team was consulted in 98.6% (71) of cases at a median of 1 day after admission and addiction medicine was consulted for 86.1% (62; Table 2). Cardiac surgery was formally consulted in 65.3% (47) of cases and 51.4% (37) had 1 or more indications for surgery per the 2015 AHA guidelines. Seventeen patients had severe tricuspid regurgitation, eight patients had symptoms of right-heart failure, seven patients had vegetations ⩾20 mm, four patients had recurrent septic pulmonary emboli, and one patient had bacteremia lasting ⩾7 days. Sixty-six patients (91.7%) were managed with antibiotics alone. The median duration of intravenous antibiotic therapy was 28 days. Thirty-seven patients (51.4%) were transitioned to oral antibiotics to complete their treatment regimen and the median duration of oral antibiotic therapy was 14 days. Five (6.9%) patients underwent PMA of a tricuspid valve vegetation. Among patients who received PMA, all five presented with Staphylococcus aureus bacteremia of a median duration of 10 days. Two patients receiving PMA developed transient hypotension postprocedure requiring initiation of vasopressors and admission to the ICU. Discrete vegetation sizes were not available for all five patients. One (1.4%) patient underwent tricuspid valve replacement during the index hospitalization for an overall procedural intervention rate of 8.3%. The patient who underwent valve surgery presented with S. aureus TVIE and evidence of cerebral emboli in the setting of a patent foramen ovale (PFO) with symptomatic right-to-left shunt. They underwent bioprosthetic tricuspid valve replacement and surgical PFO closure. Four patients underwent transcatheter closure of a PFO during their hospitalization.
In-hospital management strategies for patients with isolated, definite native tricuspid valve endocarditis treated by a multidisciplinary endocarditis team.

Clinical outcomes
There was 1 in-hospital death for a mortality rate of 1.4%. The patient who passed away during their index admission had two previous admission for TVIE and discharged before medically advised in both instances. Their index hospitalization was complicated by refractory septic shock, multiorgan failure, cachexia, and bowl ischemia. Consequently, the multidisciplinary team did not believe the patient would survive an operation and the family transitioned the patient to comfort measures. There was one additional death between discharge and 90-days postdischarge for a 90-day mortality of 2.8% (Table 3). The patient who died within 90-days of discharge developed S. mitis TVIE while undergoing chemotherapy for refractory B-cell acute lymphoblastic leukemia. The patient passed away from complications of their leukemia. All patients who underwent PMA, valve replacement surgery, and PFO closure survived to discharge.
Postdischarge outcomes and follow-up of patients with isolated, definite native tricuspid valve endocarditis treated by a multidisciplinary endocarditis team.

Nineteen patients were discharged before medically advised. Median length of stay was 18.5 days (IQR: 16.5 days). There were 18 (25%) re-admissions at 30-days and 9 (50%) of these were in patients who previously left before medically advised. Five patients were re-admitted for complications of treatment or progression of disease, three patients were re-admitted for reasons not related to IE, and one patient was admitted with a new bloodstream infection. Follow-up was greatest with ID at 63.9%, followed by cardiac surgery at 36.1%, and cardiology and 26.4%. Only 12.5% of patients followed up with addiction medicine at the authors institution, although 66.7% were discharged on MOUD initiated during the index hospitalization.
During the study period, an additional 10 patients received elective tricuspid valve replacements after outpatient follow-up, including one who previously underwent PMA. Five patients received a bioprosthetic valve at a median of 242 days postdischarge, and an additional five patients received a mechanical valve at a median of 331 days.
One-year follow-up data were available for 60 patients. There were five total deaths from any cause in that period (Supplemental Figure 2). The 12 remaining patients are all currently alive but have yet to reach 1-year follow-up. Of the three late deaths, one patient presented to a referring hospital with a new bloodstream infection, sepsis, and disseminated intravascular coagulation and passed away at the other facility, one patient passed away from a suspected opioid overdose, and one passed away suddenly at home and autopsy was declined by the family.
Discussion
In this single-center retrospective series, we report 72 patients with isolated native TVIE managed by a multidisciplinary endocarditis program with very low rates of in-hospital and 90-day mortality. Our study is unique in three notable ways. First, it is the first to report exclusively on the outcomes of patients with TVIE managed in a multidisciplinary fashion. Second, over 90% were managed medically in the acute setting, with only one tricuspid valve replacement and five PMAs performed during the index hospitalization despite 51% of patients having indications for valve surgery. Finally, it also includes longitudinal data about the rates of delayed elective valve surgery in this population.
As expected, patients were young, but medically complex, with high-rates of co-morbid SUD, IDU, Hepatitis C, and 40% had a previous diagnosis of TVIE. There has been substantial debate about the optimal treatment strategy for patients with IDU-related TVIE. The AHA, Society of Thoracic Surgeons and European Society of Cardiology have all recommended this population be treated by multidisciplinary teams.18,23 However, each of these societies continues to provide recommendations for valve surgery during the index hospitalization in specific situations. Additionally, there is virtually no data or guidance about the appropriate indications for PMA in TVIE. Our multidisciplinary approach heavily favored initial medical management with antibiotic therapy and addiction medicine consultation. Over 90% of patients were treated medically and more than 85% received addiction medicine consultation. Despite nearly 40% of patients requiring intensive care unit admissions and approximately one quarter receiving vasopressor support and/or mechanical ventilation, in-hospital, and 90-day mortality outcomes were excellent with this approach. One driver of mortality in this population is overdose after discharge. Two-thirds of patients were initiated on MOUD prior to discharge, which may have contributed to the very low 90-day and 1-year mortality in this vulnerable population. The majority of patients with SUD who were not discharged on MOUD were offered, but declined treatment.
Only a small number of procedural interventions were needed during the index hospitalization, but these outcomes were also encouraging. Although cardiac surgery was formally consulted in 65% of cases, their team attended all of the weekly MDET meetings and provided input as needed. PMA was pursued only in patients who had persistent bacteremia for ⩾7 days on maximal antibiotic therapy and provided that other foci of infection were addressed. Patients with vegetations >2 cm who were clinically stable with clear blood cultures were not referred for PMA. Our CVID service initiates patients with persistent S. aureus bacteremia on combination antimicrobial therapy within 72 h based on an internal protocol and aggressively searches for other possible sites of infection which we hypothesize limits the number of patients meeting our criteria for PMA.24–27 The role and efficacy of combination antibiotic therapy was not specifically analyzed in this study, but this is the subject of ongoing research by our multidisciplinary team. Approximately half of patients were also transitioned to oral antibiotics to complete treatment of their TVIE. The practice of successful treatment of IE with partial oral antibiotic therapy was previously reported by our group. 28
A subgroup of four patients also underwent percutaneous PFO closure during the index hospitalization. We have previously reported on three cases of patients receiving this procedure.29,30 In these four instances, the patients had recent IDU and were found to have isolated TVIE with PFO and either evidence of systemic emboli or hypoxemia from right-to-left shunt. All patients had transesophageal echocardiograms to rule out evidence of left-sided IE. Two patients subsequently underwent tricuspid valve replacement in a delayed fashion after clinical stabilization and treatment of their SUD. In both of those cases, the closure device was removed intraoperatively, and the PFO was surgically closed. One patient has moderate tricuspid regurgitation and is being followed outpatient to monitor for indications for valve surgery. One patient died at >90 days after discharge after admission to another hospital with bacteremia caused by a new organism. None of the four patients developed relapsed infection with their original pathogen. There is not sufficient data to advocate for this approach in all patients with TVIE and PFO. Providers could consider percutaneous PFO closure as a salvage intervention in patients with TVIE and significant shunt or evidence of systemic emboli in the absence of left-sided IE with the ultimate goal of delayed surgical valve replacement and PFO closure.
Our multidisciplinary team continued to follow patients in the outpatient setting, both in individual specialty clinics and in a collaborative ID/cardiac surgery clinic. Almost 2/3 of patients were seen for ID follow-up with lower rates of follow-up with cardiac surgery and cardiology. Addiction medicine follow-up was recorded for patients who followed specifically with providers at the authors’ institution. Approximately 1/3 of patients reside in counties in rural Eastern Kentucky, that are a 2–4-h drive from our institution. Consequently, many patients were scheduled for follow-up with local providers for ease of access, but we could not reliably record whether or not these appointments were attended. Several patients also received their MOUD concurrently in ID clinic. As a result, the rate of addiction medicine follow-up care is likely significantly higher than the 12.5% reported here. Thirty-day readmission rates were relatively high at 25%, although 50% of these occurred in patients who left before medically advised. The social factors, particularly in patients with SUD, that contributed to follow-up challenges may also contribute to the higher rates of re-admission.
Ten patients, approximately 14% of the study population, ultimately underwent delayed, elective tricuspid valve replacements using our protocolized process for follow-up of patients with moderate or greater tricuspid regurgitation. This finding highlights that a multidisciplinary program can longitudinally follow patients with native TVIE and offer access to surgery after the index hospitalization in more favorable circumstances once both their infection has been cured and their SUD treatment optimized.
Limitations
Our study is limited by its retrospective nature, the lack of a control group, and that it was conducted at a single center. Nearly 1/3 of patients were transferred from outside hospitals, and we do not have data on the number of patients that were referred to our institution but not accepted. It is possible that sicker patients were not accepted for transfer because they were not felt to be salvageable, thereby skewing our patient population toward more stable patients. Additionally, we did not record 90-day rates of relapsed infection or re-admission which may lead to an underestimation of postdischarge complications. Patients with prosthetic tricuspid valves and CIEDs were excluded as the management strategies are more complex for this population and this exclusion likely impacted the mortality outcomes compared to other published literature.
Conclusion
Isolated native TVIE remains a challenging disease to treat, in part due to the high rates of co-morbid substance use, as well as the lack of high-quality data to help guide clinical decision-making. Given the illness acuity and challenges with follow-up, it is unlikely that randomized controlled trial data will be available for this population in the near future. Our study findings suggest that, with a dedicated multidisciplinary endocarditis program using structured follow-up algorithms, patients can be effectively medically treated for native TVIE with low rates of in-hospital and 90-day mortality, high rates of addiction medicine consultation and a moderate number of delayed elective tricuspid valve replacements. Despite the presence of a collaborative team, there were still substantial rates of patient-directed discharges, re-admissions, and patients not seen in follow-up. Additional patient resources, such as housing and transportation support as well as rural outreach programs may help to improve these outcomes. More data are needed regarding the optimal implementation of these resources and construction of a multidisciplinary endocarditis program especially programs serving rural and under-resourced populations.
Supplemental Material
sj-doc-3-tai-10.1177_20499361241280690 – Supplemental material for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study
Supplemental material, sj-doc-3-tai-10.1177_20499361241280690 for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study by Bennett Collis, Talal Alnabelsi, Evan Hall, Chloe Cao, Meredith Johnson, John Gurley, Luke Strnad, Hassan Reda, Tessa London, Erinn Ogburn, Michael Sekela, Bobbi Jo Stoner and Sami El-Dalati in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-docx-1-tai-10.1177_20499361241280690 – Supplemental material for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study
Supplemental material, sj-docx-1-tai-10.1177_20499361241280690 for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study by Bennett Collis, Talal Alnabelsi, Evan Hall, Chloe Cao, Meredith Johnson, John Gurley, Luke Strnad, Hassan Reda, Tessa London, Erinn Ogburn, Michael Sekela, Bobbi Jo Stoner and Sami El-Dalati in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-tiff-2-tai-10.1177_20499361241280690 – Supplemental material for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study
Supplemental material, sj-tiff-2-tai-10.1177_20499361241280690 for Management of isolated native tricuspid valve infective endocarditis by a multidisciplinary program: a single-center retrospective cohort study by Bennett Collis, Talal Alnabelsi, Evan Hall, Chloe Cao, Meredith Johnson, John Gurley, Luke Strnad, Hassan Reda, Tessa London, Erinn Ogburn, Michael Sekela, Bobbi Jo Stoner and Sami El-Dalati in Therapeutic Advances in Infectious Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.