
Abstract
Introduction:
The incidence of infective endocarditis (IE) in pregnancy is rare and has been increasing during the opioid epidemic. IE in pregnancy is associated with high rates of maternal and fetal morbidity and mortality. Multidisciplinary endocarditis teams for management of IE have been shown to reduce in-hospital and 1-year mortality. We present a single-center experience managing IE in pregnancy utilizing a multidisciplinary endocarditis team.
Methods:
Patients diagnosed with IE while pregnant or within 30 days post-partum were identified. All patients discussed at the institution’s weekly multidisciplinary endocarditis meeting were included. Demographic and clinical data and outcome-related variables were retrospectively reviewed and recorded.
Results:
Between 1 October 2020 and 1 June 2021 6 pregnant or 30-day post-partum patients with IE were identified. All patients had co-morbid injection drug use; Staphylococcus aureus was the etiologic pathogen in all patients. All patients had embolic complications and 5 required ICU admission and mechanical ventilatory support. Four patients underwent valve replacement. There were no patient-directed discharges. All patients survived to hospital discharge and 90-days after diagnosis. Four pregnancies resulted in delivery at an average gestational age of 32.4 weeks with 3 requiring NICU admissions and prolonged lengths of stay. All patients were seen by addiction medicine and 5 were started on medication-assisted treatment for opioid use disorder.
Discussion:
In a small retrospective cases series, coordination of care by a multidisciplinary endocarditis team led to a high-rate of surgical intervention with no patient-directed discharges and no in-hospital or 90-day mortality.
Conclusion:
Multidisciplinary endocarditis teams are a low-risk intervention that may improve outcomes in pregnant patients with IE.
Introduction
Infectious endocarditis in pregnancy can present challenging management dilemmas. While the reported incidence is rare (0.006%), there has been an uptrend in endocarditis complicating pregnancies with the current opioid epidemic.1 –3 The cardiovascular physiology adaptations to pregnancy confer a substantial risk of hemodynamic collapse with acute valve failure secondary to endocarditis. Maternal mortality reports have ranged from 10% to 33% with recent studies demonstrating improving outcomes, likely due to early recognition and prompt initiation of treatment.1,3,4 Fetal mortality from maternal endocarditis in the United States may be as high as 14.6%. 3 In addition, more than half of deliveries complicated by endocarditis are pre-term with an average gestational age of 32.4 weeks, with further morbidity associated with prematurity. 5 While maternal outcomes from cardiac surgery are reportedly similar to non-pregnant women, current literature on management is limited to case series and retrospective reviews and data on neonatal outcomes have not been characterized.3,6,7 Discussions regarding indications and timing of valve surgery are particularly complex given poor fetal outcomes with cardiopulmonary bypass.6,7 Consequently, delivering effective care often requires coordination among several specialties. Multidisciplinary endocarditis teams for management of infective endocarditis have been shown to reduce in-hospital and 1-year mortality.8,9 However, the impact of this approach on the pregnant/peripartum population has not been previously studied. We present a 1-year single-center experience managing IE in pregnancy utilizing a multidisciplinary endocarditis team.
Methods
Patient cases
Ethical approval was obtained from the University of Pittsburgh. Institutional Rreview Board (IRB #20090137). Patient consent was not required as the study was exempted by the IRB. Consecutive patients diagnosed with infectious endocarditis while pregnant or within 30-days post-partum and whose cases were discussed at the institution’s weekly multidisciplinary endocarditis meeting were enrolled. Patient management plans were finalized by the endocarditis team, comprised of faculty from the departments of cardiac surgery, cardiology, infectious diseases, neurology, psychiatry and addiction medicine with ad hoc contributions from obstetrics and gynecology. Patient data were retrospectively reviewed by a study investigator not involved in the patients’ care. Demographic, clinical and outcomes related variables were recorded.
Multidisciplinary endocarditis team
The multidisciplinary endocarditis team at the University of Pittsburgh Medical Center’s (UPMC) Presbyterian and Montefiore hospitals was initially created in September 2019. In September 2020 an infectious diseases consult service, known as the endovascular infections team (EVI), dedicated specifically to caring for patients with endocarditis and cardiac device infections was created. Primary members of the multidisciplinary endocarditis team after September 2020 included faculty from the division of infectious diseases, cardiology and addiction medicine as well as the departments of cardiac surgery, neurology and psychiatry. This group met virtually for an hour once per week on Tuesday afternoons. In addition to providing antimicrobial recommendations, the EVI service also coordinated care between the other specialties. The EVI team ensured that cardiac surgery and addiction medicine were consulted in all cases of injection drug use related endocarditis and emailed all team members as well as patients’ primary teams with the list of patients to be presented ~24 hours before the multidisciplinary endocarditis team meeting. The faculty member on service for the EVI team moderated the discussion during the meeting and helped to achieve a consensus plan from the involved providers. The multidisciplinary team made recommendations about the type and duration of antimicrobial therapy, whether such therapy could be given in the outpatient setting, the role and timing of valve surgery, the role of anticoagulation, the need for additional echocardiographic or neurologic imaging, the role and type of medication for opioid use disorder, disposition from the hospital if patients lacked a stable housing situation as well as type and interval of required specialty follow-up. At the conclusion of the meeting, an advanced practice provider working with the EVI service would document a brief note including the team’s recommendations in the patient’s electronic medical record.
Pregnant patients with endocarditis were admitted to Magee Women’s Hospital at UPMC. Notably, this hospital is a separate physical building ~0.5 miles from the Presbyterian and Montefiore Hospitals where the multidisciplinary endocarditis team is based. Magee Women’s Hospital has separate infectious diseases and cardiology consult services as well as a separate echocardiography lab. In addition, Magee Women’s Hospital does not have a cardiac surgeon and the cardiac surgeons from Presbyterian and Montefiore Hospitals do not have privileges at Magee. Consulting obstetricians are available at Presbyterian and Montefiore hospitals. When a pregnant patient was found to have endocarditis, the cardiologist at Magee interpreting the echocardiogram contacted the EVI attending physician who would then add this patient to the list of patients to be discussed by the multidisciplinary endocarditis team. The EVI attending physician then notified the endocarditis team’s primary cardiac surgeon of the patient so that they could review the patient’s electronic medical record prior to the team meeting. The patient’s primary obstetrician was also invited to attend the multidisciplinary endocarditis team meeting. When discussing a pregnant patient, the multidisciplinary endocarditis team also provided guidance about timing of delivery and whether patients should be transferred from Magee Women’s Hospital to Presbyterian/Montefiore Hospital, in addition to the group’s typical recommendations (described above).
Definitions
Duration of bacteremia was defined by the number of days that elapsed between the first positive blood culture and two consecutive negative blood cultures, or a single negative blood culture if only one was obtained. Valve surgery indications were defined in accordance with American Heart Association recommendations. 10
Results
Demographics
Between 1 October 2020 and 1 May 2021 6 pregnant or 30-day post-partum patients with infectious endocarditis were identified. The average patient age was 29.3 years (median: 28 years, range: 26–37 years; Table 1). The average gestational age at presentation was 22.6 weeks (median: 26 weeks, range: 6–34 weeks) including 2 patients who presented in labor. No patients presented post-partum. All patients had co-morbid injection drug use and carried a mental health disorder diagnosis. Two patients had prior endocarditis, and 1 had a bicuspid aortic valve which served as additional endocarditis risk factors. Five patients presented to Magee Women’s Hospital initially and 1 patient presented to Presbyterian/Montefiore Hospitals. Four of 5 patients initially admitted to Magee were transferred to Presbyterian/Montefiore, including 3 who were immediately post-partum or post-miscarriage and subsequently underwent valve surgery.
Demographic data for pregnant patients with infectious endocarditis managed by the multidisciplinary endocarditis team at the University of Pittsburgh Medical Center.

HIV, human immunodeficiency virus.
Methicillin-susceptible Staphylococcal aureus (MSSA) was the etiologic pathogen in all patients (Table 2). Five patients had right-sided endocarditis. Three patients had isolated tricuspid disease and 1 had pulmonic involvement. One patient had both mitral and tricuspid valve vegetations and one patient had isolated mitral valve endocarditis. Five patients had septic pulmonary emboli on chest computerized tomography. Three patients had radiographic evidence of cerebral emboli, including two who presented clinically with stroke, one of whom suffered an intracranial hemorrhage. Five patients required intensive care unit admission and required mechanical ventilatory support. The average duration of bacteremia was 5.8 days (median: 5.5 days, range: 2–12 days). Three patients underwent uncomplicated transesophageal echocardiography as part of their diagnostic evaluation.
Description of endocarditis and modality of medical therapy for pregnant patients with endocarditis.
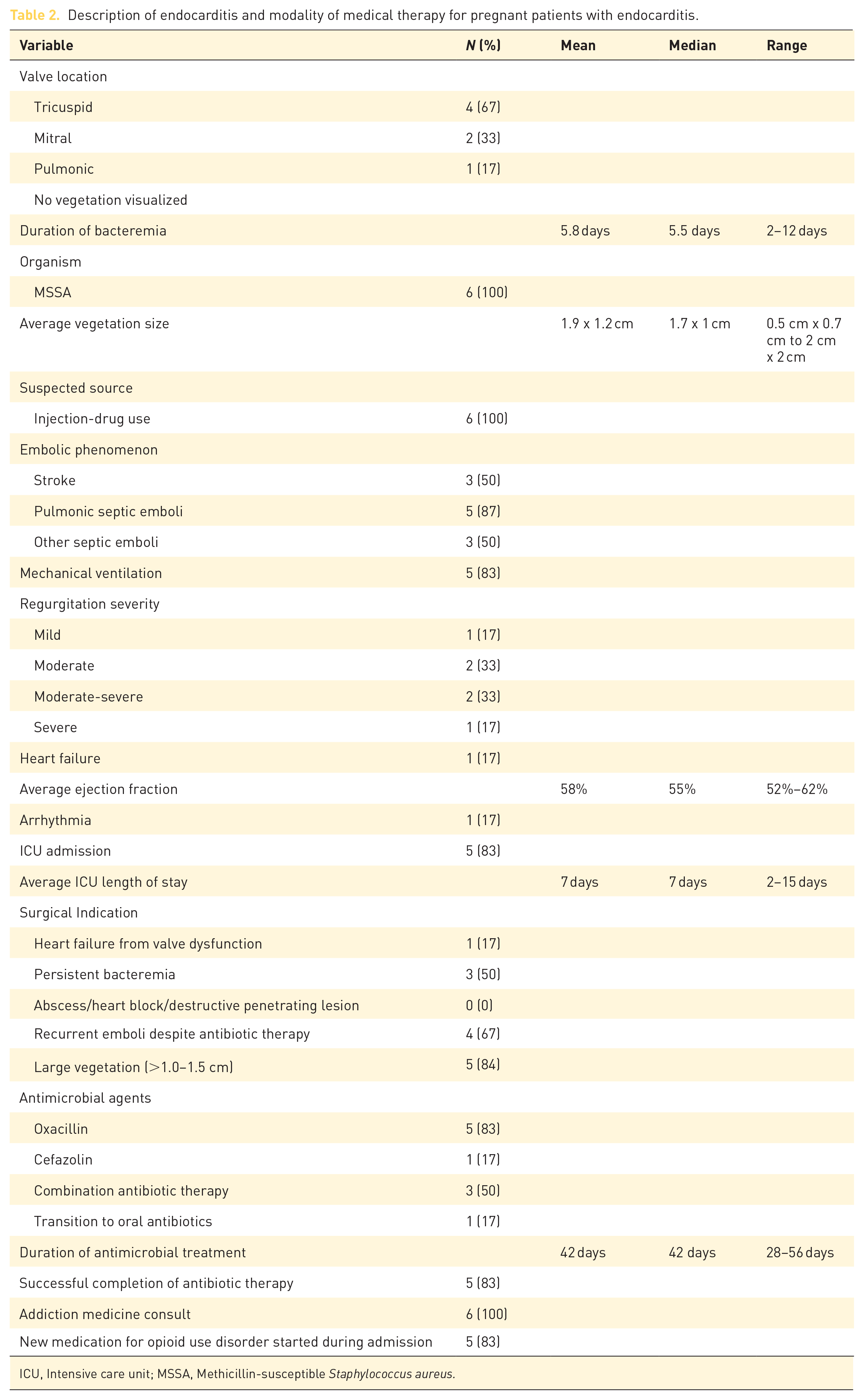
ICU, Intensive care unit; MSSA, Methicillin-susceptible Staphylococcus aureus.
Management
Four patients underwent post-partum valve replacement as part of their endocarditis treatment at an average of 17.8 days (median: 16.5 days, range: 15–21 days) after admission (Table 3). Prior to surgery two patients delivered spontaneously at 34 weeks and 39 weeks, 4 days. One patient underwent emergency C-section at 28 weeks and 1 miscarried at 10 week, 5 days. Indications for surgery in patients undergoing valve replacement included recurrent emboli in all 4 individuals, 3 of whom had vegetations > 1.0 cm. One patient also had persistent bacteremia for 7 days. One patient underwent an isolated tricuspid valve replacement, 1 received a tricuspid valve replacement with patent foramen ovale closure, 1 underwent isolated mitral valve replacement and 1 underwent both tricuspid and mitral valve replacements. All 4 had extensive valve destruction at the time of surgery that precluded valve repair. Timing of surgery in patients with cerebral emboli was determined by the multidisciplinary endocarditis team with input from cardiac surgery, neurology, and neurosurgery. Of the 2 patients who were managed medically, both had persistent bacteremia > 7 days, large vegetations > 1.0 cm and 1 had accompanying heart failure secondary to severe valve dysfunction. Since both patients had desired pregnancies surgery was not performed antenatally due to the potential fetal impact of cardiopulmonary bypass.
Mortality, surgical and post-operative outcomes for pregnant patients with endocarditis managed by the multidisciplinary endocarditis team.

CIED, cardiac implantable electronic device; PFO, patent foramen ovale.
After initial empiric antibiotic therapy all patients were narrowed to targeted antimicrobial treatment with an anti-staphylococcal beta-lactam. Three were treated with combination beta-lactam therapy until blood culture clearance.11,12
Maternal outcomes
All 6 patients survived until hospital discharge and were alive at 90-days after diagnosis. Four patients remained in the hospital to complete intravenous antibiotic therapy, including 3 who underwent valve replacement. One patient was discharged after ~4 weeks of intravenous oxacillin on oral antibiotics for an additional 2 weeks. 13 One was transferred to another institution closer to her home after clinical stabilization. In all, 5 of 6 patients were discharged on medication for opioid use disorder. Four patients followed-up with cardiac surgery, 2 with infectious diseases and 2 with an obstetrician (Table 4). Only one patient was discharged with a form of contraception. Two patients developed recurrent endocarditis with different micro-organisms in the setting of relapsed injection drug use ~4 and 7 months post-operatively. One of these patients underwent redo mitral valve replacement and developed endocarditis again 4 months after the second operation secondary to ongoing injection drug use.
Fetal/neonatal outcomes
Four pregnancies resulted in delivery at an average gestational age of 32.4 weeks (median 31 weeks, range 28–39 weeks; Table 5). There was one miscarriage at 10 weeks, 5 days and one patient was lost to follow-up with an unknown pregnancy outcome. Three deliveries were spontaneous vaginal deliveries and 1 was an emergent c-section secondary to fetal bradycardia. Average available birthweight for 3 babies was 1816 g (median 1083 g, range 1050 – 3316 g) with APGAR scores at 1 and 5-minutes averaging 2.3 and 5.7, respectively (median 1, 7, range (1,2–5,7, Table 6). Three babies required neonatal ICU admission with an average length of stay of 44.3 days (median: 46 days, range: 17–70 days). Two infants met clinical criteria for neonatal respiratory distress syndrome and 2 suffered Grades 1–2 intraventricular hemorrhages. One baby met diagnostic criteria for neonatal abstinence syndrome. Two mothers were unable to breastfeed secondary to their ongoing medical issues. A third mother’s child resided with family members > 60 miles from UPMC Presbyterian/Montefiore and consequently was unable to breastfeed. A fourth delivered an infant after discharge from UPMC and the authors could not ascertain whether or not she chose to breastfeed. Despite prematurity and long-term antenatal antibiotic exposure, no infants developed necrotizing enterocolitis.
Post-discharge outcomes, including rates of follow-up, relapsed injection drug use and recurrent endocarditis for pregnant patients with endocarditis managed by the multidisciplinary endocarditis team.

Obstetric outcomes for pregnant patients with endocarditis managed by the multidisciplinary endocarditis team.

IUFD, Intrauterine fetal demise.
Fetal outcomes for babies born to mothers with infectious endocarditis whose care was managed by the multidisciplinary endocarditis team.

Discussion
In this case series we present the 1-year experience with management of infective endocarditis in pregnancy by a single center multidisciplinary team. Results are notable for an absence of maternal deaths at 90-days follow-up. This may reflect a more widespread historical trend in mortality as diagnostic capability and access to treatment for endocarditis has improved over time. While the observed mortality was low, morbidity was impacted by substantial rates of pulmonary septic emboli, stroke, ICU admission, and long lengths of stay.
The epidemiologic results of our study largely reflect the national trend of IE in pregnancy, with all cases attributable to injection drug use. Despite increased rates of OUD screening and availability of treatment, data suggests that large percentages of hospitalized pregnant patients do not receive medication for opioid use disorder.14,15 In our study, all patients were evaluated by addiction medicine and 5 were discharged on medication for opioid use disorder. We still observed a high rate of relapse and recurrent endocarditis, which is reflective of the disease course when complicated by substance use disorders. However, at the time of this study no patients had died from overdose, which may be related to the protective effects of medication for opioid use disorder. In addition, only 1 patient was discharged with contraception. It is unclear from our study how many patients were offered contraception. However, given the challenges managing endocarditis and cardiac valvular diseases in pregnancy multidisciplinary endocarditis teams may want to consider performing more detailed assessment of patients’ interest in contraception prior to hospital discharge. 4
With respect to fetal outcomes, the series had adverse outcomes in all pregnancies, including 1 intrauterine demise. We also observed a high preterm delivery rate, with average gestational age at live birth of 32 weeks, similar to reported literature. 5 This led to further neonatal complications with half of the neonates requiring ICU admissions and prolonged lengths of stay. There were substantial rates of low fetal birth weight, low APGAR scores, respiratory distress syndrome, and intraventricular hemorrhage. These fetal complications have been associated with adverse neurodevelopmental outcomes as well as higher disability rates in children; however, the long-term pediatric outcomes related to maternal endocarditis have not been studied.16,17
Access to valve surgery historically has been challenging for both pregnant patients and patients who inject drugs. However, a highlight of this series was the high rate of surgical intervention which occurred in 4 patients. The use of cardiopulmonary bypass and cardiac surgery in pregnancy is still quite controversial, and data on rates of surgical intervention are limited. 3 As discussed above, cardiac surgery was not available at Magee Women’s Hospital and the presence of the multidisciplinary endocarditis team facilitated hospital transfers and provided access to surgical opinions that would not otherwise have been readily available. Notably, all surgically managed patients in our series underwent valve surgery after delivery or miscarriage. With regards to antimicrobial treatment, 5 patients completed the recommended courses of antibiotic therapy. As a result of the multidisciplinary endocarditis team, pregnant patient with endocarditis received access to input from infectious diseases specialists with expertise in endocarditis. Consequently, 3 patients were treated with combination beta-lactam therapy, a novel approach that has been shown to decrease time to blood culture clearance and is associated with low-mortality in patients with MSSA endocarditis.11,12 Historically patients with injection drug use and/or pregnancy have high rates of patient-directed discharges and failure of antibiotic completion.18,19 Encouragingly, there were no patient-directed discharges after involvement of the multidisciplinary endocarditis team.
While this is a small case series assessing the impact of multidisciplinary teams in caring for pregnant or post-partum patients with endocarditis, it extends existing evidence demonstrating the benefits of these teams on patient outcomes. While more robust clinical trials are needed, given the challenges conducting intervention research in both pregnant patients and individuals with endocarditis it may be difficult to obtain high quality data. In the interim, multidisciplinary endocarditis teams are a low-risk intervention that may improve outcomes in this population (Table 7).
Potential benefits of a multidisciplinary endocarditis team on the care of pregnant patients with endocarditis.

Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical board approval was obtained from the institutional review board at the University of Pittsburgh (IRB #20090137). Patient consent was not required as the study was exempted by the IRB.