
Abstract
Background:
Syphilis is a serious global public health challenge. Despite prior progress in syphilis control, incidence has been increasing in recent years. Syphilis is a common coinfection among people living with HIV (PLHIV). In Panama, few data describe syphilis prevalence among PLHIV. We describe syphilis antibody and high-titer (⩾1:8) active syphilis prevalence and associated factors among individuals who attended an antiretroviral clinic.
Methods:
A cross-sectional study was undertaken during February–March 2022 and September–October 2022 for adults (⩾18 year) assigned male and female at birth, respectively. Participants provided peripheral blood samples and self-administered a questionnaire. Samples were screened using immunochromatography; antibody-positive samples were tested using rapid plasma regain to 1:512 dilutions. Logistic regression was used to identify factors associated with syphilis antibody and high-titer active syphilis.
Results:
In all, 378 participants gave blood samples; 377 individuals participated in the questionnaire (216 self-reported male sex [males], 158 female [females], and three intersex individuals). Median age was 36 years (interquartile range: 28–45 years). Overall, syphilis antibody prevalence was 32.3% (122/378) (males, 50.7% [108/2013]; females, 5.7% [9/158]; intersex individuals, 100.0% (3/3)], p < 0.01. High-titer active syphilis was found among 24.6% (n = 30) of samples with positive antibody test (males 27.8% [n = 30], females 0.0% [0/9], intersex individuals 0.0% [0/3]). Antibody positivity was associated in the multivariable model with males (50.7%, AOR = 24.6, 95%CI: 1.57–384.53). High-titer active syphilis was associated with younger participant age (18–30 years, 13.2%, OR = 4.82, 95%CI: 1.17–19.83); 31–40 years, 7.8%, OR = 4.24, 95%CI: 1.04–17.21 versus 3.2% >40 years), homosexual identity (16.0% OR = 34.2, 95%CI: 4.50–259.27 versus 0.6% among heterosexual identity); in the multivariable model, associated with sexual identity (bisexual 19.1%, AOR = 10.89, 95%CI: 1.00–119.06) compared to heterosexual identity (0.6%) and weakly associated with concurrency (⩾1 ongoing sexual relationships, 15.9%, AOR = 3.09, 95%CI: 0.94–10.14).
Conclusion:
This study found very high prevalence of syphilis antibodies and high-titer syphilis among PLHIV in Panama. Those most affected are males, younger in age, those who practice concurrent sexual relationships, and those who reported homosexual and bisexual identity. Targeted interventions should include repetitive testing and treatment, especially among individuals who may be at increased infection risk.
Plain language summary
Syphilis is a significant health challenge worldwide. On a global scale, yearly syphilis incidence is increasing, including in Panama. However, there are no current data to explain syphilis prevalence and who is most affected among people living with HIV in Panama. In order to understand syphilis in Panama and create targeted interventions among specific groups of people, it is important to describe how many people are infected, and who is most affected by this infection. Therefore, we conducted a study among 378 people living with HIV at a treatment clinic in Panama City, Panama. Blood samples and demographic data were collected. In all, syphilis antibodies were found in 32.3% of individuals (50.7% of those who self-report as males, 5.7% as females, and 100% of those who self-report as intersex. Of those with positive antibody tests, 24.6% of individuals also had active syphilis. Only individuals who identify as male had active syphilis. Our findings show high syphilis prevalence among people with HIV in Panama City, particularly among males, those who are younger, those who report sexual identity as homosexual or bisexual, and those with ongoing sexual relationships with more than one individual. Targeted interventions are needed among people living with HIV, especially among the groups most affected. These interventions could include testing more often for syphilis and providing timely treatment, especially among individuals who may be at increased risk of infection.
Introduction
Syphilis infection, caused by the bacterium Treponema pallidum and human immunodeficiency virus (HIV), continues to be significant public health challenge globally. Overall prevalence of syphilis has risen worldwide over the past 30 years, 1 with the most significant increase in low- and middle-income countries. In Panama, syphilis prevalence has steadily increased among all populations since 2015. 2 Syphilis is a common coinfection among people living with HIV, especially among males.3,4 Individuals with recent HIV diagnoses are at an elevated risk of acquiring syphilis due to overlapping risk behaviors, such as engaging in unprotected sexual activity. 5 Additionally, in the age of Preexposure prophylaxis and Undetectable = Untransmissible, chances of HIV transmission have decreased. However, an increased risk of transmission of other sexually transmitted infections (STIs), such as syphilis, has been found.6,7
The immunocompromized status of people living with HIV can influence the clinical course of syphilis, leading to atypical presentations and diagnostic challenges. 7 As a result, prompt and accurate diagnosis becomes imperative for appropriate management. Conversely, syphilis infection can exacerbate HIV transmission and disease progression. 7 The disruption of mucosal barriers during primary infection may increase the risk of HIV transmission during sexual contact. 7 Additionally, inflammatory responses induced by syphilis may enhance viral replication and viral shedding, further complicating HIV management and control. Among people living with HIV, syphilis may present differently than among people not living with HIV. For example, among those living with HIV, primary syphilis may present as multiple chancres, more extensive and deeper chancres, and anal chancres may be more common; secondary syphilis may include persistent chancres.8–11 Some patients with coinfection may present with atypical and aggressive manifestations, including a higher risk of early neurosyphilis, although the clinical and prognostic significance remains unknown.10,11
In Latin America and the Caribbean region, the World Health Organization reports an overall regional syphilis prevalence of 1.3% among all populations. 2 However, key populations [gay men, other men who have sex with men (MSM), and transwomen] are most affected. 2 In Panama, few syphilis prevalence data have been published. One exception is a 2012 study which found a syphilis prevalence of 16.0–31.6% among MSM and transgender women in three cities in Panama. 12 National surveillance shows syphilis prevalence in Panama (>18%) is higher than most countries in the region; there has been an increase in the prevalence of syphilis among transgender women sex workers. 2 In 2022, there were a total of 2597 cases of syphilis reported to the Ministry of Health; the incidence has been increasing in the last 10 years. Similarly, congenital syphilis prevalence has risen from 83 reported cases in 2015 to 221 cases in 2022. 13
In 2022, Panama had an estimated 29,000 people living with HIV (1.0% prevalence among all adults 15–49 years, 5.9% among MSM and 14.7% among transgender people), and male to female ratio was 2.7:1. 14 In the largest urban antiretroviral (ART) clinic in 2022, 6047 individuals attended (4503 males and 1544 females), and 448 were new patients. This clinic undertakes annual VDRL testing and provides treatment for active syphilis of all individuals who attend the clinic (oral communication, public Antiretroviral Clinic, Panama City, Panama).
As with the epidemic worldwide, Panama was able to control new syphilis cases for decades. However, there remains a notable gap in understanding the current increase in prevalence. Furthermore, despite the potential clinical ramifications of HIV-syphilis coinfection, there is a need to explain who is at greatest risk for syphilis, especially active infection.
The present research aims to address this knowledge gap by describing syphilis antibody and active syphilis prevalence and risk factors for infection among people living with HIV in a large ART clinic in Panama City. The findings will contribute to the literature on the prevalence and risk factors to recommend targeted interventions to mitigate the impact of syphilis among people living with HIV.
Methods
Recruitment targeted adults (⩾18 years) living with HIV who attend the ART Clinic who had specific binary sex (based on medical records) during the following months: February and March 2022 for participants assigned male at birth – AMAB (e.g. cis-gender men, transgender women, and intersex people assigned male at birth) and between September and October 2022 for participants assigned female at birth – AFAB (e.g. cis-gender women, transgender men, and intersex people assigned female at birth). However, participants who did not neatly fall within this binary sex (e.g. intersex and transgender) attended the recruitment based on the participant’s sex assigned at birth. In analyses, we report sex and gender based on the self-reported items collected at the time of recruitment rather than the sex implied by their time of recruitment.
Study procedures and sample collection
All potential participants were approached during their regularly scheduled clinical appointments. The study team visited the clinic on Mondays to Wednesdays and approached all participants for inclusion.
The minimum sample size was calculated based on the primary outcome of interest of expected genital chlamydia prevalence (not reported here) of 19% among those AMAB and 10% among AFAB, assuming 3000 patients AMAB patients and 1200 patients AFAB attend the clinic bi-annually and using a 95% confidence interval. In all, 76% of AMAB attendees and 82% of AFAB attendees were approached and gave written, informed consent to participate.
Data were obtained for sociodemographics, STI history, and sexual behavior using a self-administered questionnaire on a tablet computer using Kobo Toolbox (Harvard Humanitarian Initiative, CA, USA). Study personnel were available and aided in filling out the questionnaire if the participant was unable to do so.
A peripheral blood sample was collected, stored in EDTA tubes, and transported within 4 hours to the Department of Research and Biological Surveillance-3 laboratory at the Gorgas Memorial Institute for Health Studies.
Measures
Laboratory assessment of syphilis
Testing was undertaken in all samples using rapid syphilis antibody tests (Syphilis anti-TP Test, Abbott Diagnostics Korea Inc, Republic of Korea), with active syphilis testing using nontreponemal assay (Rapid Plasma Reagin Test, Rapid Labs Ltd, UK) with assay titration to 1:512 for all antibody-positive samples, to assure samples did not have prozone phenomenon. Treponemal seroreactivity was defined as positivity to the treponemal assay, whereas high-titer syphilis was defined as the dual positivity to treponemal and nontreponemal assay positivity at ⩾1:8.
Within 24 h of submitting their blood sample, participants with high-titer active syphilis who were not already in a syphilis treatment program (n = 12 were already in a treatment program) were contacted by the study team and asked to return within the following 3 days to the ART clinic for treatment, according to national guidelines. 15 ART clinic physicians made treatment decisions on a case-by-case basis with benzathine penicillin: (a) participants with no known previous VDRL or RPR reactive results, independent of current RPR findings and (b) those with past VDRL or RPR results but insufficient decrease were treated for late-stage syphilis. As per local clinical guidelines, four participants required lumbar puncture (LP) for further testing (VDRL, as used by the clinic) due to clinical criteria (high titer on RPR). Of those four who had LP, two had up-to-date LP results and decreasing titers. LP was ordered for the other two participants; these results were non-reactive.
Questionnaire demographic measures
These variables included self-reported sex [self-reported male sex (males), self-reported female sex (females), self-reported intersex (intersex individuals)]. Note that intersex variation may include a wide range of phenotypic presentations that may or may not be visibly perceptible and, therefore, may or may not impact the sex assigned at birth. In Panama, birth records currently use exclusively binary sex (male or female). 16 For these reasons, we use self-reported sex. Other variables included are gender identity (men, women, another gender), gender modality (cis-gender, transgender or another modality), sexual identity (homosexual, heterosexual, bisexual, another identity), concurrency in last three partners (reported to have had ongoing sexual relationships with ⩾1 of the current and previous three sexual partners) and years since HIV diagnosis (years living with HIV).
Statistical methods
Questionnaire responses were uploaded into the Kobo Toolbox cloud, imported, and analyzed in Stata V18.0 (StataCorp, College Station, TX, USA). The X2 test was used to evaluate the difference in syphilis antibody and high-titer active syphilis prevalence between sociodemographic and behavioral variables. Kruskal Wallis Test was used to evaluate associative trends among variables. Individuals who participated in the questionnaire or blood samples were included in demographic tables. Missing variable values were excluded from analyses; three individuals declined to give blood samples but participated in the questionnaire, and four individuals gave blood samples but did not participate in the questionnaire. Logistical regression (using participant data of those who partook in blood samples and the questionnaire) was used to calculate odds ratio (OR) and 95% confidence interval (CI). Variables associated with each syphilis outcome, at p < 0.2, were included in the initial multivariable model adjusting for participant sex. The model first included sociodemographic (distal) variables, then behavioral (proximal) variables. In the final model, variables independently associated with outcomes at p < 0.05 were reported.
Ethical procedures
The research was approved by the Gorgas Memorial Institutional Bioethics Board [628/CBI/ICGES/19 (original approval), 347/CVI/ICGES/22 (amendment approval to include individuals AFAB)]. All participants were 18 years and older and gave written informed consent to participate.
Results
Study population
Participant inclusion is found in Figure 1; of the male participants, 95.3% (205) reported identifying as cis-gender men; 4.6% (n = 10) were transgender or of another gender modality (Table 1). Of the female participants, 99.4% (156) reported identifying cis-gender women, 0.6% (n = 1) of transgender or another gender modality. Of the three individuals who self-reported as intersex individuals, 100% reported to identify as men.
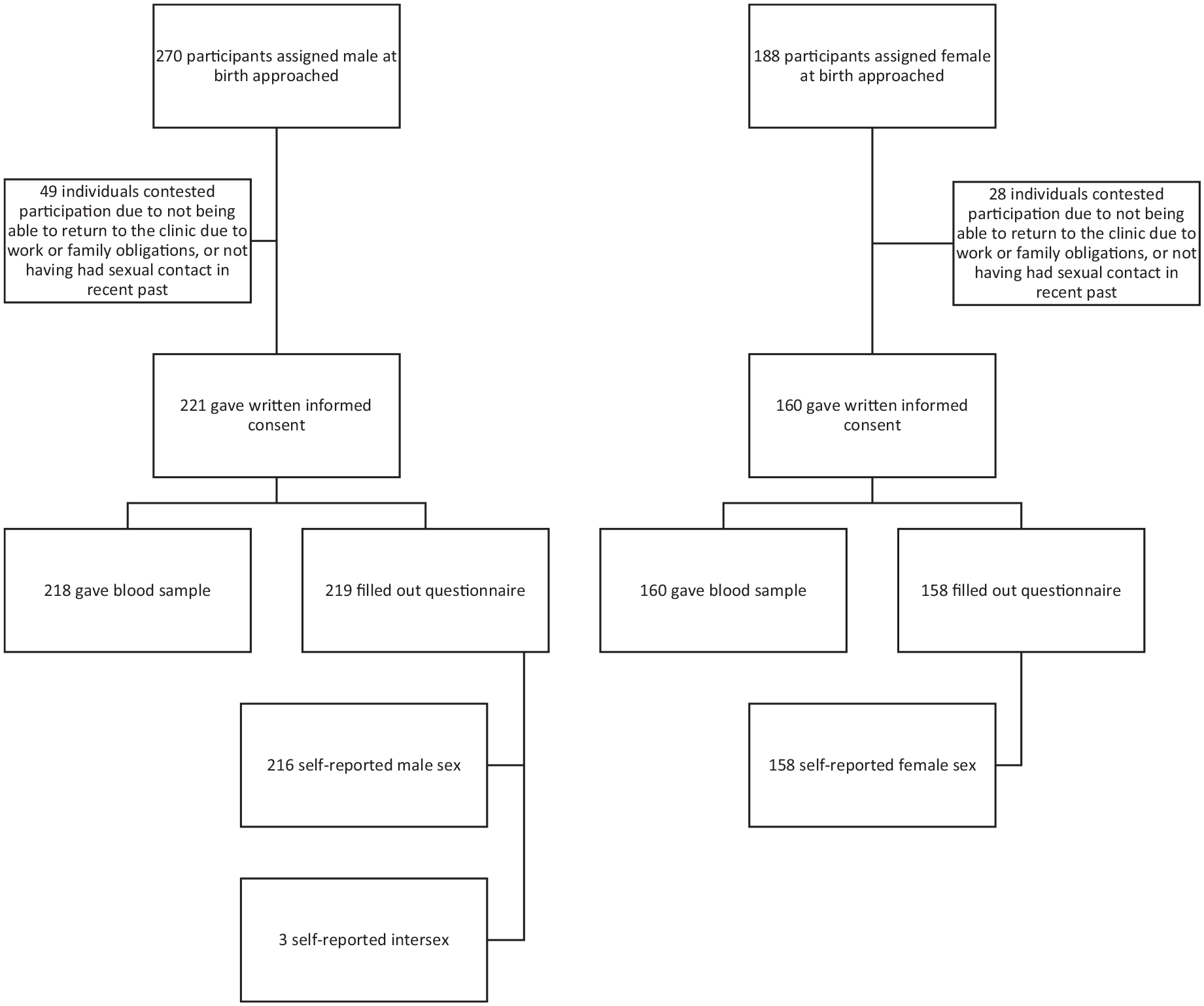
Flowchart of participant inclusion at large ART clinic in Panama, 2022.
Participant characteristics among participants living with HIV who attend the ART clinic at a large public hospital in Panama City, 2022.

Of those who have had sex with a female, male, or transgender person (question dependent).
HIV, human immunodeficiency virus; OR, odds ratio; STI, sexually transmitted infection.
STI symptoms and syphilis testing
In all, 45.0% (168/373) of participants reported STI symptoms in the past month [28.6% (61/213)] of male participants, 68.2% [107/157] of female participants and 0.0% [0/3] of intersex participants, p < 0.01. Of all participants, 67.8% (253/373) thought they had or were not sure if they had an STI other than HIV; 39.2% (147/375) of participants reported a syphilis test in the past 6 months. Male participants, 44.9% (96/214) and intersex participants, 66.7% (2/3), were more likely to have had a syphilis test in the past 6 months than female participants, 31.0% (49/158), p = 0.02. Of those who were tested in the past 6 months and tested positive [36.2% (42/116)] for syphilis, 85.4% (35/41) received treatment.
Syphilis prevalence
Syphilis antibodies were found among 32.3% (122/378) of participants tested. There were statistically significant differences (p < 0.01) among participants when segregating by participant self-reported sex: syphilis antibodies were found among 50.7% (108/213) of males, 5.7% (9/158) of female participants and 100.0% (3/3) of intersex individuals (p < 0.01) (Table 2). High-titer active syphilis (⩾1:8) was found among 24.6% (n = 30) of all participants who had positive antibody tests. Among males with a positive antibody test, 27.8% (n = 30) had high-titer active syphilis; among female participants, 0% (0/9) had high-titer active syphilis; among intersex individuals, 0.0% (0/3) had high-titer active syphilis. Titer distribution was 30.3% (37/122) non-reactive, 10.7% (13/122) 1:1, 21.3% (26/122) 1:2, 13.1% (16/122) 1:4, 13.9% (17/122) 1:8, 4.9% (6/122) 1:16, 3.3% (4/122) 1:32, 0.8% (1/122) 1:64, 1.6% (2/122) 1:128.
Prevalence of syphilis antibody and active syphilis, by participant characteristics among participants living with HIV who attend the ART Clinic at a large public hospital in Panama City, 2022.

Of those who have had sex with a female, male or trans person (question dependent).
ART, antiretroviral; HIV, human immunodeficiency virus; OR, odds ratio; STI, sexually transmitted infection.
All participants were evaluated for treatment by clinical providers based on previous syphilis test positivity and titer level; this was deemed appropriate for 25 male and 0 female participants.
Factors related to antibody positivity
In bivariable analyses, syphilis antibody positivity was associated with gender identity (men (50.0%, OR = 13.36, 95%CI: 6.83–26.13) compared to women (7.0%)), and those who reported to be of another gender (62.5%, OR = 22.27, 95% CI: 4.69–105.67) (Table 3). Antibody positivity was also associated with gender modality (transgender or another gender modality (63.6%, OR = 3.89, 95% CI: 1.12–13.56) compared to cis-gender (31.0%)), and sexual identity (homosexual identity [55.5% (OR = 10.62, 95% CI: 5.84–19.29) and bisexual (59.5%, OR = 12.54, 95% CI: 5.76–27.30) or another identity, 55.5%, OR = 4.26, 95% CI: 1.53–11.87) compared to heterosexual (10.5%), and with those who reported to ever had sex with someone of the same sex (57.2%), compared to only having had sex with someone of the opposite sex (9.1%, OR = 13.38, 95% CI: 7.56–23.67).
Factors associated with syphilis antibody and active syphilis positivity among participants living with HIV who attend the ART Clinic at a large public hospital in Panama City, 2022.

Bolded ORs are significant at p ⩽ 0.05.
Not included due to collinearity with sex.
ART, antiretroviral; HIV, human immunodeficiency virus; OR, odds ratio; STI, sexually transmitted infection.
In multivariable analyses, syphilis antibody positivity was associated with males (50.7%, OR = 24.6, 95%CI: 1.57–384.53) compared to females (5.7%), as well as having had a syphilis test in the past 6 months (47.9%, OR = 3.65, 95%CI: 1.43–9.35) compared to no test (22.0%).
In multivariable analyses, gender identity was not found to be associated with syphilis antibody positivity.
Factors associated with high-titer active syphilis positivity
High-titer active syphilis was associated in bivariable analyses with males (14.1%, OR = 11.75, 95% CI: 3.40–40.60) compared to female participants (0.0%) (Table 3). Recent (<1 year) HIV diagnosis was associated with active syphilis 15.9%, OR = 2.41, 95% CI: 1.01–5.74), compared to those who had their diagnosis >5 years prior (7.2%), gender modality [transgender individuals (36.4%, OR = 7.36, 95% CI: 2.02–26.79) compared to cis-gender (7.2%)], reported anal sex in last 3 months (15.6%, OR = 4.69, 95%CI: 2.10–10/56) compared to no anal sex (3.8%) and reported oral sex in last 3 months (12.2%, OR = 2.97, 95% CI: 1.32–6.66), compared to no oral sex (4.5%).
In the multivariable model, high-titer active syphilis was found to be associated with younger age (18–30 years 13.2%, OR = 4.82, 95% CI: 1.17–19.83) and (31–40 years, 7.8%, OR = 4.24, 95% CI: 1.04–17.21) compared to older than 40 years 3.6%. Active syphilis was found to be weakly associated with reported concurrent sexual relationships (15.9%, OR = 3.09, 95% CI: 0.94–10.14) compared to no concurrency (6.9%), and sexual identity (bisexual 19.1%, AOR = 10.89, 95% CI: 1.00–119.06) compared to heterosexual identity (0.6%).
In independent multivariable analyses, gender identity was not found to be associated with active syphilis positivity.
Discussion
We conducted the first syphilis prevalence study among people living with HIV in Panama. We found a very high prevalence of syphilis antibodies and active syphilis among this population, especially among male participants, younger individuals, those with more recent HIV infection, individuals of transgender and other gender modalities, and homosexual and bisexual identities. Additionally, sexual behaviors were found to be important, as syphilis was associated with participants who reported to engage in anal sex and have concurrent sexual relationships. While male participants were more likely to have a syphilis test in the past 6 months. Still, less than half reported a test within the timeframe. Our findings indicate the importance of more consistent syphilis testing in initial and follow-up visits and follow-up testing among individuals at greatest risk for infection.
Antibody positivity and high-titer active syphilis prevalence were found to be associated with key populations, including individuals of transgender or another gender modality and homosexual and bisexual identities. These key populations have been found to have higher STI prevalence in general in Panama, 12 in Latin America, and worldwide.2,17,18 The reasons for the prevalence disparity may be due to condomless anal sex, dense sexual networks, as well a lack of opportune testing and treatment.12,18 Moreover, women may be screened at higher rates than men due to healthcare-seeking behavior and prenatal visits. 19
High-titer active syphilis was additionally associated with younger individuals and those with more recent HIV diagnoses. Furthermore, our research findings highlight that younger individuals living with HIV are at a heightened risk of syphilis infection. This observation corroborates with global trends in the early 2000s that demonstrate a higher prevalence of syphilis among young adults than older. 20 More recently, older males have also had increasing prevalence. New HIV infections are also greater among young adult populations in Panama. 21 Behavioral factors, such as condomless sex and concurrent sexual relationships, are most likely driving new syphilis as well as new HIV infections in this population.22,23 Furthermore, research has shown a 32% increase in syphilis prevalence post-COVID-19 pandemic in Spain. 24 This pattern is most likely to have occurred in Panama as well among people living with HIV, as medical and especially HIV care appointments were greatly affected by pandemic closures. 25
Concurrent sexual relationships were identified in unadjusted analyses as a risk factor for syphilis infection.26,27 Our findings also indicate that these concurrent sexual encounters increase association with syphilis infection and further underscore the importance of understanding and addressing the impact of sexual networks and concurrent partnerships on the transmission dynamics of STIs.28,29 Furthermore, although participants were probed about concurrent partnerships, it has been found that short pauses between partners are important in decreasing the transmission of STIs. 30 Therefore, a proper sexual network study is needed among key populations in Panama to understand the complexities of concurrent relationships with STI outcomes to create potential interventions for this population.
The implications of these findings are critical for targeted syphilis control interventions. First, testing intervals could be decreased among those living with HIV who attend ART clinics. Secondly, targeted testing could be increased among specific populations with greater syphilis prevalence; this has been found to lead to a decrease in secondary syphilis among MSM in Australia. 31 Testing may be provider-initiated, and newer methods such as self-testing32,33 and electronic medical record computer prompts may increase the total number of people tested. 32 Syphilis testing and treatment may have an impact on HIV prevalence as well; testing and treatment of syphilis have been found in mathematical models to possibly decrease new HIV infections by up to 48%. 34 However, these testing strategies are not a silver bullet for syphilis control; political will is needed to undertake a multifaceted approach. The medical system, medical professionals, and professional and civil societies would need to be called upon to work together. 32
Our study included a decent sample size, we could use self-applied electronic questionnaires to mitigate reporting bias, and a good percentage of individuals who were approached agreed to participate. However, the study also had some limitations. First, the cross-sectional nature of the research design restricts our ability to establish causality between the identified risk factors and syphilis infection. Furthermore, although the study occurred during the same year, those assigned male and female at birth were not sampled simultaneously due to funding limitations. However, across Panama, no remarkable changes in testing and treatment were made that could cause significant differences between sexes. Second, despite our approach to mitigate bias in a sexual behavior survey by using a self-administered questionnaire, the questions may still be subject to reporting bias. Third, the study was conducted at one ART clinic in Panama. Therefore, the results may not be representative of those of other clinics across the country. Fourth, the HIV male: female ratio in Panama is 2.7:1; in our study, we included a ratio of 1.4:1. Fifth, the syphilis anti-TP test reported high sensitivity (99.3%) and specificity (99.5%, versus TPHA); this test is unable to differentiate sexually transmitted syphilis from endemic treponematosis infections. However, yaws has not been reported in Panama since before 1978, 35 and pinta was last reported in a study in the 1980s,36,37 although endemic treponematosis may have remained underreported in Panama and across the region. Lastly, our study did not collect information from patient charts on CD4+ cell counts, viral load, ART duration of use or regimens. Future studies should include these variables from patient charts to best correlate with syphilis outcomes.
Our study demonstrates very high prevalence of syphilis antibodies and high-titer active syphilis among people living with HIV who attend the ART clinic in Panama City, especially among those who identify as male, are younger, report homosexual and bisexual sexual identity, and to some extent, those involved in concurrent sexual relationships. These findings highlight the urgent need for targeted syphilis control interventions to reduce syphilis transmission among these vulnerable populations, as well as potentially to other populations such as pregnant women, and to decrease the potential for long-lasting complications caused by syphilis infection. By addressing these factors, Panama could take significant strides in improving the health of those living with HIV, especially those at greatest risk for syphilis infection. Future longitudinal studies and more extensive, cross-country studies are warranted to corroborate these findings and enhance our understanding of the complex interplay between risk factors and syphilis infection dynamics among people living with HIV.
Footnotes
Acknowledgements
We are grateful to all participants who took part in the study. We would also like to thank the staff at the ART clinic, especially Dr. Lilibeth Canales, nurses Venus Reyes and Zuleyka Ureña, and phlebotomist Ariadne Guevara, for their unwavering support, even when the clinic was very busy.
Correction (June 2022):
Since the original online publication, this article has been updated to correct second author’s name as Félix Díaz Fernández.